Breakfast in Denmark. Prevalence of Consumption, Intake of Foods, Nutrients and Dietary Quality. A Study from the International Breakfast Research Initiative

Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Intake of Energy, Nutrients, and Foods
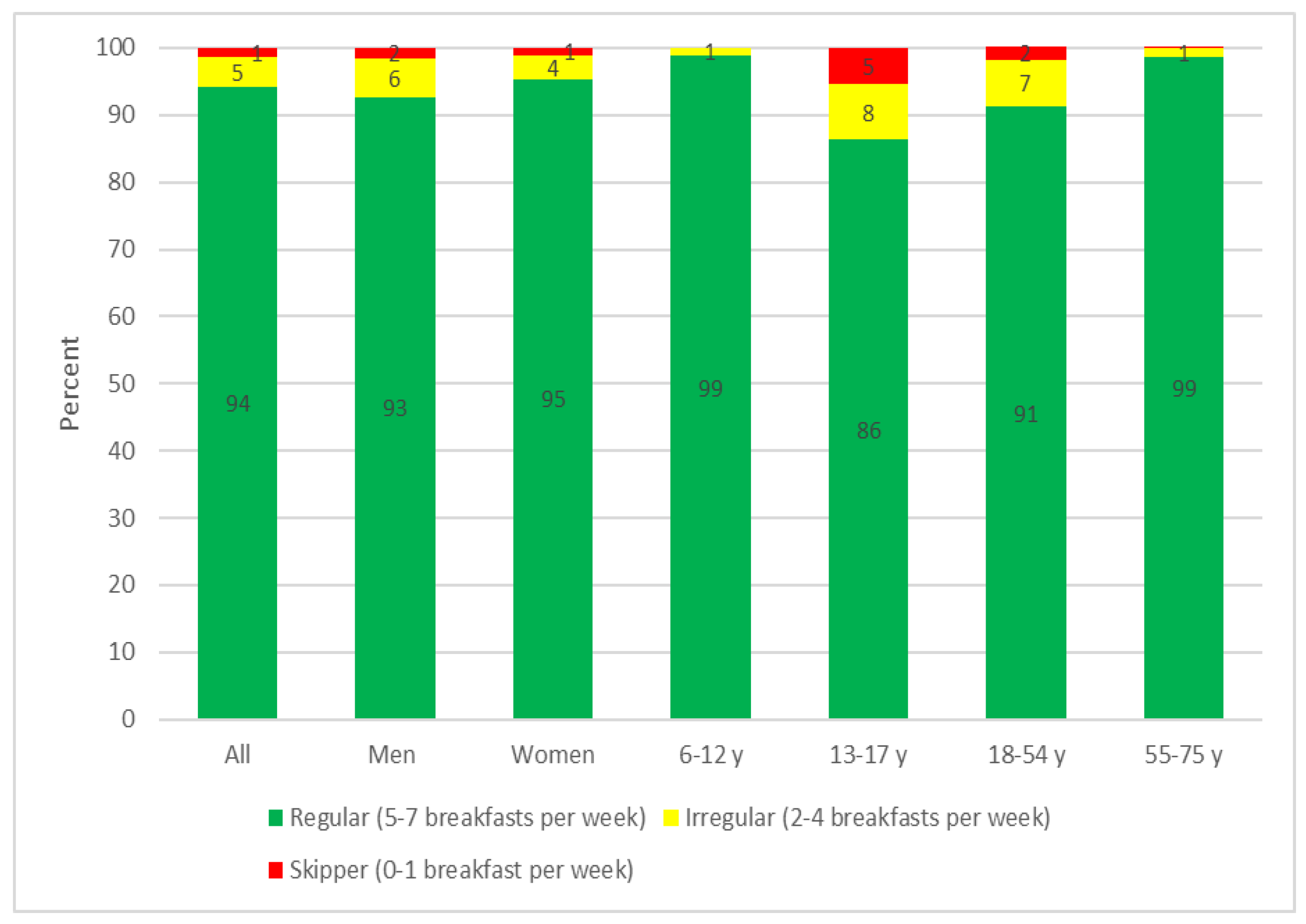
2.3. The Regularity of Breakfast Consumption
- 5–7 breakfasts per week: Regular consumer
- 2–4 breakfasts per week: Irregular consumer
- Breakfast 0–1 day per week: Skipper
2.4. Calculation of Dietary Quality of the Diet by the NRF 9.3 Index
2.5. Statistical Analysis
3. Results
3.1. The Regularity of Breakfast Consumption
3.2. Daily and Breakfast Intake of Energy, Nutrients and Foods
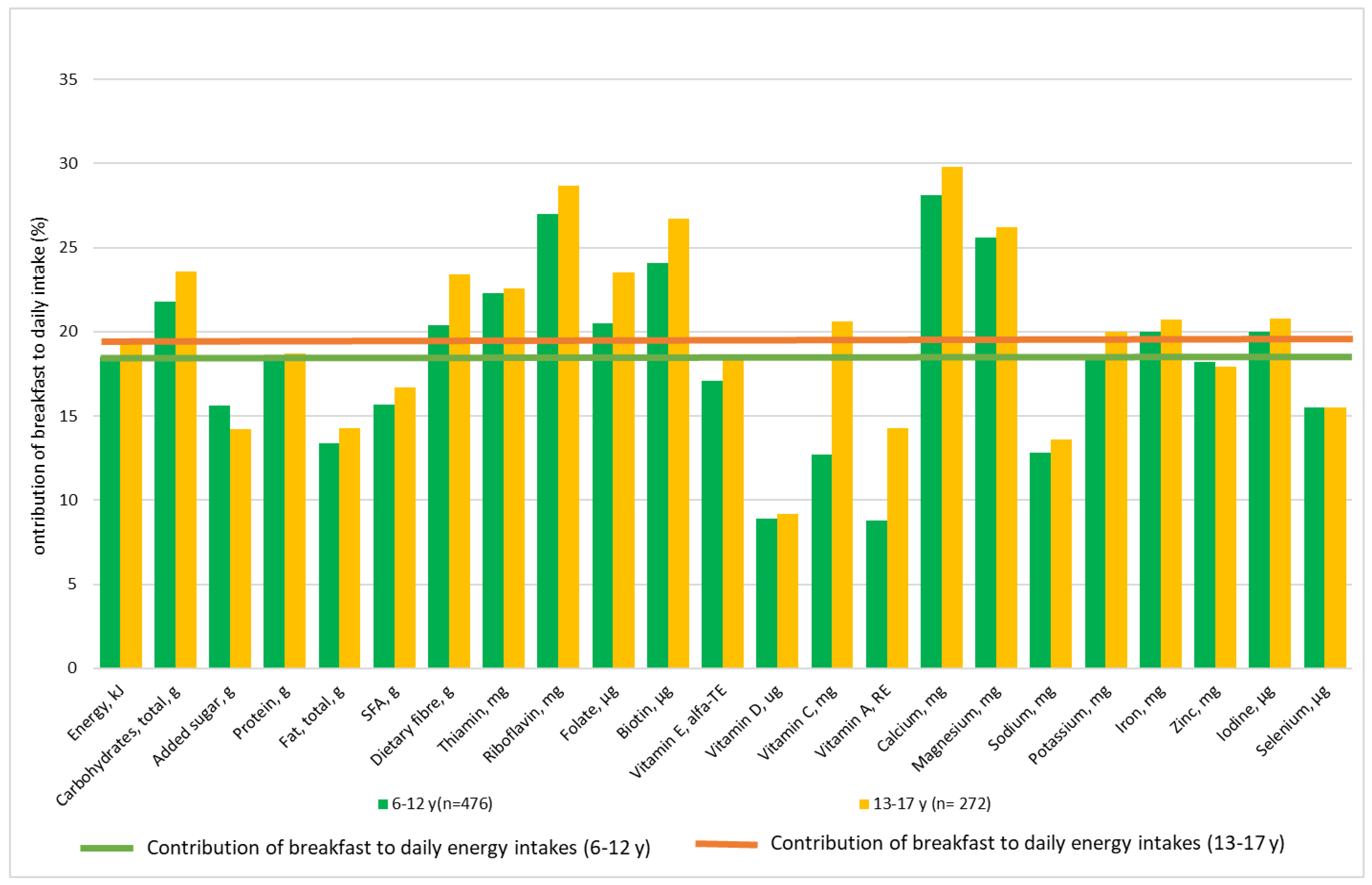
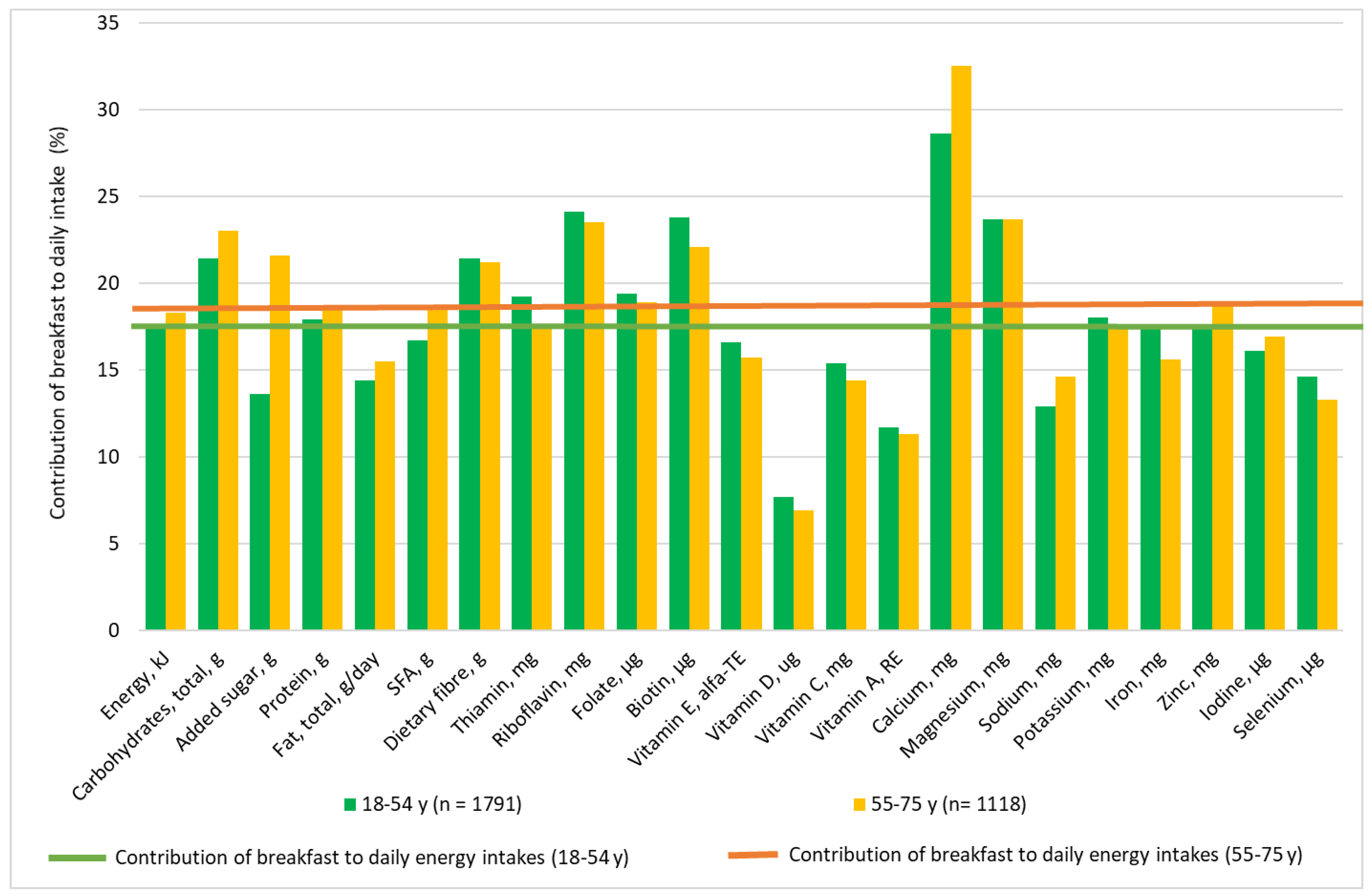
3.3. The Contribution of Breakfast to Daily Energy and Nutrient Intakes
3.4. Energy, Nutrients and Food Intakes at Breakfast by Tertiles of Daily Dietary Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Dye, L. The Importance of Breakfast in Europe. A Review of National Policies and Health Campaigns; European Breakfast Cereal Association, 2017; Available online: http://www.breakfastisbest.eu/docs/102017/BIB_Report_Executive_Summary_Importance_of_Breakfast_in_Europe_2017.pdf (accessed on 1 April 2018).
- De la Hunty, A.; Gibson, S.; Ashwell, M. Does regular breakfast cereal consumption help children and adolescents stay slimmer? A systematic review and meta-analysis. Obesity Facts 2013, 6, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Nordic Nutrition Recommendations 2004. Integrating Nutrition and Physical Activity, 4th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2004. [Google Scholar]
- Nordic Nutrition Recommendations 2012. Integrating Nutrition and Physical Activity, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- Danish Veterinary and Food Administration. Available online: http://altomkost.dk/tips/til-maaltiderne/morgenmad/ (accessed on 28 May 2018).
- Danish Whole Grain Partnership. Available online: www.fuldkorn.dk/english (accessed on 28 May 2018).
- Mejborn, H.; Ygil, K.H.; Fagt, S.; Trolle, E.; Korup, K.; Christensen, T. Danskernes Fuldkørnsindtag 2011–2013 (Intake of Whole Grain in Denmark—in Danish); National Food Institute: 2014. Available online: https://www.food.dtu.dk/-/media/Institutter/Foedevareinstituttet/Publikationer/Pub-2014/Danskernes_fuldkornsindtag_2011-2013.ashx (accessed on 1 June 2018).
- Fagt, S.; Groth, M.V.; Andersen, N.L. Danskernes Kostvaner 1995. Mad og Måltider (In Danish with an English Summary); 2000:06; Fødevaredirektoratet: København, Demark, 2000. [Google Scholar]
- Christensen, L.M.; Kørup, K.; Trolle, E.; Matthiessen, J.; Fagt, S. Børn og Unges Måltidsvaner 2005–2008 (In Danish with an English Summary); DTU Fødevareinstituttet: København, Demark, 2012; Available online: http://orbit.dtu.dk/files/54035355/rapport_m_ltidsvaner2005_2008_4_19_r_jan.pdf (accessed on 28 May 2018).
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [CrossRef] [PubMed]
- Priebe, M.G.; McMonagle, J.R. Effects of ready-to-eat-cereals on key nutritional and health outcomes: A. systematic review. PLoS ONE 2016, 11, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Cahill, L.E.; Chiuve, S.E.; Mekary, R.A.; Jensen, M.K.; Flint, A.J.; Hu, F.B.; Rimm, E.B. Prospective study of breakfast eating and incident coronary heart disease in a cohort of male US health professionals. Circulation 2013, 128, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Uemura, M.; Yatsuya, H.; Hilawe, E.H.; Li, Y.; Wang, C.; Chiang, C.; Otsuka, R.; Toyoshima, H.; Tamakoshi, K.; Aoyama, A. Breakfast skipping is positively associated with incidence of type 2 diabetes mellitus: Evidence from the aichi workers cohort study. J. Epidemiol. 2015, 25, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Mekary, R.A.; Giovannucci, E.; Willett, W.C.; van Dam, R.M.; Hu, F.B. Eating patterns and type 2 diabetes risk in men: Breakfast omission, eating frequency, and snacking. Am, J. Clin Nutr. 2012, 95, 1182–1189. [Google Scholar] [CrossRef] [PubMed]
- Mekary, R.A.; Giovannucci, E.; Cahill, L.; Willett, W.C.; van Dam, R.M.; Hu, F.B. Eating patterns and type 2 diabetes risk in older women: Breakfast consumption and eating frequency. Am. J. Clin. Nutr. 2013, 98, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Ruszczynski, M. Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in Europe. Crit. Rev. Food Sci. Nutr. 2010, 50, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Hoyland, A.; Dye, L.; Lawton, C.L. A systematic review of the effect of breakfast on the cognitive performance of children and adolescents. Nutr. Res. Rev. 2009, 22, 220–243. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K.; American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; et al. Meal timing and frequency: Implications for cardiovascular disease prevention: A Scientific Statement from the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [PubMed]
- Dhurandbar, E.J.; Dawson, J.; Alcorn, A.; Larsen, L.H.; Thomas, E.A.; Cardel, M.; Bourland, A.C.; Astrup, A.; St-Onge, M.-P.; Hill, J.O.; et al. The effectiveness of breakfast recommendations on weight loss: A randomized controlled trial. Am. J. Clin. 2014, 100, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.I.; Severin, M.; Holmberg, T.; Eriksen, L.; Toftager, M.; Zachariassen, A.; Ekholm, O.; Tolstrup, J.S.; Grønbaek, M.; Curtis, T. KRAM-Undersøgelsen i tal og Billeder (In Danish); National Institute of Public Health, University of Southern Denmark: Copenhagen, Demark, 2009. [Google Scholar]
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.; Torsheim, T.; Augustson, L.; Mathison, F.; Aleman-Diaz, A.; Molcho, M.; Weber, M.; et al. Growing up unequal: Gender and socioeconomic differences in young people’s health and well-being. In Health Behavior in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey; WHO Regional Office for Europe: Copenhagen, Demark, 2016; Available online: http://www.euro.who.int/en/publications/abstracts/growing-up-unequal.-hbsc-2016-study-20132014-survey (accessed on 20 March 2018).
- COOP. Danskernes Madvaner 2016; Roland, T., Poulsen, D., Steenberg, M., Obelitz, M., Falk, J., Eds.; Coop Analyse: Albertslund, Demark, 2016; Available online: https://om.coop.dk/Upload/om.coop.dk/Publikationer/analyser/Danskernes%20Madvaner%202016_Coop%20Analyse.pdf (accessed on 30 March 2018).
- Gibney, M.J.; Barr, S.I.; Bellisle, F.; Drewnowski, A.; Fagt, S.; Livingstone, B.; Masset, G.; Varela-Moreiras, G.; Moreno, L.; Smith, J.; et al. Breakfast in human nutrition: The International Breakfast Research Initiative. Nutrients 2018, 10, 559. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.N.; Christensen, T.; Matthiessen, J.; Knudsen, V.K.; Rosenlund-Sørensen, M.; Biltoft-Jensen, A.; Hinsch, H.J.; Ygil, K.H.; Kørup, K.; Saxholt, E.; et al. Danskernes Kostvaner 2011–2013. Høvedresultater (In Danish with an English Summary); DTU Fødevareinstituttet: Cøbenhavn, Demark, 2015; Available online: http://www.food.dtu.dk/Publikationer/Ernaering-og-kostvaner/De_nationale_kostundersoegelser (accessed on 20 March 2018).
- Biltoft-Jensen, A.P.; Matthiessen, J.; Rasmussen, L.B.; Fagt, S.; Groth, M.V.; Hels, O. Validation of the Danish 7-day pre-coded food diary among adults: Energy intake v. energy expenditure and recording length. Br. J. Nutr. 2009, 102, 1838–1846. [Google Scholar] [CrossRef] [PubMed]
- Danish Food Data. Available online: www.frida.fooddata.dk (accessed on 26 October 2016).
- Drewnowski, A. The Nutrient Rich Foods Index helps to identify healthy, affordable foods. Am. J. Clin. Nutr. 2010, 91, 1095S–1101S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulgoni, V.L., III; Keast, D.R.; Drewnowski, A. Development and validation of the Nutrient-Rich Foods Index: A tool to measure nutritional quality of foods. J. Nutr. 2009, 139, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Regulation (eu) no 1169/2011 of the European parliament and of the council of 25 october 2011. Off. J. Eur. Union 2011, 1169/2011, 18–63. [Google Scholar]
- Guideline: Sugar Intake for Adults and Children; World Health Organisation: Geneva, Switzerland, 2015; Available online: http://apps.who.int/iris/bitstream/handle/10665/149782/9789241549028_eng.pdf;jsessionid=44345FBF70B58A25B4BB48DF36D3D5F2?sequence=1 (accessed on 1 February 2018).
- European Food Safety Authority. Scientific opinion on dietary reference values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 1462. [Google Scholar]
- Groth, M.V.; Fagt, S.; Brøndsted, L. Social determinants of dietary habits in Denmark. Eur. J. Clin. Nutr. 2001, 55, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groth, M.V.; Sørensen, M.R.; Matthiessen, J.; Fagt, S.; Landvad, N.; Knudsen, V.K. Disparities in dietary habits and physical activity in Denmark and trends from 1995 to 2008. Scand. J. Public Health 2014, 42, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Barr, S.I.; DiFrancesco, L.; Fulgoni, V.L., 3rd. Breakfast consumption is positively associated with nutrient adequacy in Canadian children and adolescents. Br. J. Nutr. 2014, 112, 1373–1383. [Google Scholar] [CrossRef] [Green Version]
- Tsalis, G.; Hummelshøj, I.; Lahteenmaki, L. Undersøgelse af Forbrugernes Holdning til Produkter, der er Tilsat D-Vitamin af Sundhedsmaessige Årsager (Study of Attitudes towards Products Fortified woth Vitamin D for Health Reasons—In Danish); Aarhus University, Business and Social Sciences MAPP-Centre for Research and Customer Relations in the Food Sector: Aarhus, Demark, 2015; Available online: https://pure.au.dk/ws/files/93733978/DCArapport_d_vitamin_net.pdf (accessed on 1 June 2018).
- Bech-Larsen, T.; Grunert, K.G.; Poulsen, J.B. The Acceptance of Functional Foods in Denmark, Finland and the United States; Working paper no 73; The Aarhus School of Business: Aarhus, Demark, 2001; Available online: https://pure.au.dk/ws/files/32301883/0003055.pdf (accessed on 1 June 2018).
- Groth, M.V.; Fagt, S. Danskernes Kostvaner. Måltidsvaner, Holdninger, Sociale Forskelle og Sammenhaeng med Anden Livsstil. (In Danish with English summary); Fodevaredirektoratet: København, Demark, 2003; Available online: http://www.food.dtu.dk/Publikationer/Ernaering-og-kostvaner/De_nationale_køstundersoegelser (accessed on 25 July 2018).
- Groth, M.V.; Fagt, S.; Stockmarr, A.; Matthiessen, J.; Biltoft-Jensen, A. Dimensions of socioeconomic position related to body mass index and obesity among Danish women and men. Scand. J. Public Health 2009, 37, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Groth, M.V.; Christensen, L.M.; Knudsen, V.K.; Sørensen, M.R.; Fagt, S.; Ege, M.; Matthiessen, J. Sociale Forskelle. Børns Kostvaner, Fysiske Aktivitet og Overvaegt & Voksnes Kostvaner; DTU Fødevareinstituttet: København, Demark, 2013; Available online: http://www.food.dtu.dk/Publikationer/Ernaering-og-kostvaner/De_nationale_kostundersoegelser (accessed on 25 July 2018).
- Knudsen, V.K.; Fagt, S.; Trolle, E.; Matthiessen, J.; Groth, M.V.; Biltoft-Jensen, A.; Sørensen, M.R.; Pedersen, A.N. Evaluation of dietary intake in Danish adults by means of an index based on food-based dietary guidelines. Food Nutr. Res. 2012, 56. Available online: https://www.tandfonline.com/doi/abs/10.3402/fnr.v56i0.17129 (accessed on 25 July 2018). [CrossRef] [PubMed] [Green Version]
- Fagt, S.; Biltoft-Jensen, A.; Matthiessen; Groth, M.V.; Christensen, T.; Trolle, E. Danskernes Kostvaner 1995–2006. Status og Udvikling med Henblik på Frugt og Grønt Samt Sukker; DTU Fødevareinstituttet: København, Demark, 2008; Available online: http://www.food.dtu.dk/Publikationer/Ernaering-og-kostvaner/De_nationale_kostundersoegelser (accessed on 25 July 2018).
- Christensen, A.I.; Ekholm, O.; Gray, L.; Glumer, C.; Juel, K.W. What is wrong with non-respondents? Alcohol-, drug- and smoking-related mortality and morbidity in a 12-year follow-up study of respondents and non-respondents in the Danish Health and Morbidity Survey. Addiction 2015, 110, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Tolonen, H.; Laatikainen, T.; Helakorpi, S.; Talala, K.; Martelin, T.; Prattala, R. Marital status, educational level and household income explain part of the excess mortality of survey non-respondents. Eur. J. Epidemiol. 2010, 25, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.B.; Matthiessen, J.; Biltoft-Jensen, A.P.; Tetens, I. Characteristics of misreporters of dietary intake and physical activity. Public Health Nutr. 2007, 10, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 h recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101, S73–S85. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Nutrient | NRV 1 | MRV 2 |
|---|---|---|
| Protein (g) | 50 | - |
| Dietary fibre (g) | 25 | - |
| Vitamin A (ug) | 800 | - |
| Vitamin C (mg) | 80 | - |
| Vitamin D (ug) | 5 | - |
| Calcium (mg) | 800 | - |
| Iron (mg) | 14 | - |
| Potassium (mg) | 2000 | - |
| Magnesium (mg) | 375 | - |
| Saturated fat (E% fat) | - | 10 |
| Added sugar (E% fat) | - | 10 |
| Sodium (g) | - | 6 |
| Age Group | All (6–75 years) n = 3657 | Children (6–12 years) n = 476 | Adolescents (13–17 years) n = 272 | Younger Adults (18–54 years) n = 1791 | Older Adults (55–75 years) n = 1118 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | p * | p ** | |||||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Breakfast Intake | Daily Intakes | |
| Energy (kJ) | 1736 | 806 | 9645 | 3066 | 1599 | 564 | 8655 | 1934 | 1759 | 820 | 9042 | 3365 | 1754 | 844 | 10029 | 3267 | 1761 | 824 | 9599 | 2932 | 0.0012 | <0.0001 |
| Carbohydrates (g) | 59 | 28 | 266 | 87 | 59 | 22 | 269 | 62 | 64 | 31 | 273 | 104 | 58 | 28 | 273 | 91 | 58 | 28 | 251 | 82 | <0.0001 | <0.0001 |
| Carbohydrates (E%) | 56 | 12 | 47 | 6 | 60 | 8 | 51 | 5 | 60 | 11 | 50 | 6 | 55 | 12 | 47 | 6 | 54 | 12 | 45 | 6 | <0.0001 | <0.0001 |
| Added sugars (g) | 8 | 9 | 51 | 38 | 9 | 7 | 56 | 28 | 9 | 8 | 62 | 42 | 7 | 8 | 53 | 41 | 9 | 11 | 42 | 32 | <0.0001 | <0.0001 |
| Added sugars (E%) | 8 | 9 | 9 | 5 | 9 | 6 | 11 | 5 | 8 | 7 | 11 | 6 | 7 | 8 | 9 | 6 | 9 | 10 | 8 | 4 | <0.0001 | <0.0001 |
| Proteins (g) | 16 | 8 | 87 | 29 | 14 | 6 | 74 | 20 | 15 | 8 | 81 | 30 | 16 | 8 | 91 | 31 | 16 | 8 | 87 | 27 | <0.0001 | <0.0001 |
| Proteins (E%) | 16 | 5 | 16 | 3 | 15 | 3 | 15 | 2 | 15 | 5 | 16 | 3 | 16 | 6 | 16 | 3 | 16 | 5 | 17 | 3 | <0.0001 | <0.0001 |
| Fat (g) | 14 | 10 | 94 | 37 | 11 | 6 | 81 | 22 | 12 | 8 | 85 | 36 | 14 | 10 | 99 | 39 | 15 | 10 | 95 | 36 | <0.0001 | <0.0001 |
| Fat (E%) | 28 | 11 | 37 | 6 | 25 | 9 | 34 | 4 | 25 | 10 | 34 | 5 | 29 | 11 | 37 | 6 | 30 | 11 | 38 | 6 | <0.0001 | <0.0001 |
| SFA (g) | 7 | 5 | 38 | 16 | 5 | 3 | 33 | 10 | 6 | 4 | 34 | 16 | 7 | 5 | 3 | 17 | 7 | 5 | 38 | 16 | <0.0001 | <0.0001 |
| SFA (E%) | 13 | 6 | 15 | 3 | 12 | 5 | 14 | 2 | 12 | 6 | 14 | 3 | 13 | 6 | 15 | 3 | 14 | 7 | 15 | 3 | <0.0001 | <0.0001 |
| Dietary fibre (g) | 5 | 3 | 22 | 8 | 4 | 2 | 20 | 6 | 4 | 3 | 19 | 8 | 5 | 4 | 23 | 8 | 5 | 3 | 23 | 8 | <0.0001 | <0.0001 |
| Age Group | All (6–75 years) n = 3657 | Children (6–12 years) n = 476 | Adolescents (13–17 years) n = 272 | Younger Adults (18–54 years) n = 1791 | Older Adults (55–75 years) n = 1118 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | Breakfast Intake | Daily Intake | p * | p ** | |||||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Breakfast Intake | Daily Intake | |
| Thiamin (mg) | 0.3 | 0.1 | 1.4 | 0.5 | 0.3 | 0.1 | 1.3 | 0.4 | 0.3 | 0.2 | 1.3 | 0.5 | 0.3 | 0.2 | 1.4 | 0.5 | 0.2 | 0.1 | 1.4 | 0.5 | <0.0001 | 0.4550 |
| Riboflavin (mg) | 0.4 | 0.2 | 1.8 | 0.7 | 0.4 | 0.2 | 1.6 | 0.5 | 0.5 | 0.3 | 1.7 | 0.7 | 0.4 | 0.2 | 1.8 | 0.7 | 0.4 | 0.2 | 1.8 | 0.6 | <0.0001 | 0.1042 |
| Niacin (NE) | 5.1 | 2.5 | 33.0 | 11.7 | 3.4 | 1.5 | 23.8 | 6.9 | 4.0 | 2.0 | 27.2 | 10.6 | 5.3 | 2.6 | 34.9 | 12.1 | 5.8 | 2.4 | 35.2 | 10.6 | <0.0001 | <0.0001 |
| B6 (mg) | 0.2 | 0.1 | 1.6 | 0.5 | 0.2 | 0.1 | 1.3 | 0.4 | 0.2 | 0.1 | 1.4 | 0.5 | 0.2 | 0.1 | 1.7 | 0.6 | 0.2 | 0.1 | 1.6 | 0.5 | <0.0001 | <0.0001 |
| Folate (ug) | 67 | 36 | 340 | 129 | 59 | 25 | 288 | 86 | 67 | 35 | 286 | 109 | 69 | 40 | 355 | 133 | 67 | 34 | 351 | 132 | 0.0570 | <0.0001 |
| B12 (mg) | 1.0 | 0.8 | 6.6 | 3.7 | 0.9 | 0.6 | 5.4 | 2.4 | 1.0 | 0.9 | 5.3 | 2.8 | 1.0 | 0.8 | 6.6 | 3.7 | 1.0 | 0.8 | 7.4 | 4.2 | 0.1320 | <0.0001 |
| Biotin (mg) | 9 | 6 | 36 | 15 | 8 | 5 | 34 | 11 | 9 | 7 | 32 | 15 | 9 | 6 | 38 | 17 | 8 | 6 | 35 | 146 | <0.0001 | <0.0001 |
| Vit E (alfa-TE) | 1.5 | 1.4 | 8.9 | 4.0 | 1.3 | 1.2 | 7.6 | 2.6 | 1.3 | 1.3 | 7.2 | 3.4 | 1.5 | 1.5 | 9.3 | 4.3 | 1.4 | 1.4 | 9.1 | 4.0 | 0.0001 | <0.0001 |
| Vit D (ug) | 0.3 | 0.9 | 4.4 | 4.2 | 0.2 | 0.2 | 2.7 | 2.1 | 0.3 | 0.3 | 2.9 | 2.7 | 0.4 | 0.5 | 4.4 | 3.9 | 0.4 | 1.5 | 5.7 | 5.1 | 0.0020 | <0.0001 |
| Vitamin C (mg) | 17 | 20 | 112 | 57 | 13 | 15 | 103 | 52 | 19 | 23 | 94 | 51 | 18 | 20 | 114 | 58 | 17 | 21 | 117 | 58 | 0.0010 | <0.0001 |
| Vit A (RE) | 148 | 236 | 1299 | 967 | 105 | 145 | 1189 | 706 | 139 | 211 | 973 | 737 | 155 | 244 | 1330 | 992 | 156 | 259 | 1376 | 1051 | 0.0030 | <0.0001 |
| Calcium (mg) | 331 | 183 | 1113 | 413 | 295 | 141 | 1052 | 346 | 322 | 209 | 1081 | 441 | 332 | 186 | 1161 | 426 | 348 | 185 | 1071 | 403 | 0.0004 | <0.0001 |
| Iron (mg) | 1.9 | 1.1 | 11.2 | 3.7 | 1.9 | 0.9 | 9.5 | 2.4 | 2.0 | 1.2 | 9.8 | 3.7 | 2.0 | 1.1 | 11.7 | 3.8 | 1.8 | 1.0 | 11.5 | 3.6 | <0.0001 | <0.0001 |
| Zinc (mg) | 2.2 | 1.1 | 12.0 | 4.2 | 1.8 | 0.9 | 10.1 | 2.8 | 2.0 | 1.2 | 11.2 | 4.4 | 2.2 | 1.2 | 12.6 | 4.4 | 2.3 | 1.2 | 12.1 | 3.9 | <0.0001 | <0.0001 |
| Sodium (mg) | 501 | 324 | 3726 | 127 | 413 | 206 | 3216 | 838 | 481 | 251 | 3534 | 1272 | 508 | 355 | 3941 | 1368 | 532 | 324 | 3646 | 1198 | <0.0001 | <0.0001 |
| Iodine (ug) | 42 | 26 | 247 | 142 | 47 | 24 | 233 | 119 | 49 | 32 | 235 | 128 | 42 | 26 | 259 | 157 | 40 | 24 | 236 | 129 | <0.0001 | 0.0197 |
| Potassium (mg) | 619 | 280 | 3436 | 1097 | 504 | 212 | 2750 | 784 | 575 | 307 | 2875 | 1066 | 638 | 289 | 3556 | 1099 | 647 | 272 | 3673 | 1053 | <0.0001 | <0.0001 |
| Magnesium (mg) | 89 | 52 | 370 | 118 | 77 | 46 | 300 | 83 | 82 | 63 | 314 | 121 | 93 | 53 | 391 | 123 | 90 | 48 | 380 | 1072 | <0.0001 | <0.0001 |
| Selenium (ug) | 7.4 | 4.4 | 51.5 | 20.0 | 6.5 | 3.1 | 41.5 | 13.3 | 6.9 | 3.6 | 44.7 | 18.1 | 7.8 | 5.0 | 53.5 | 21.2 | 7.2 | 4.1 | 54.1 | 19.1 | <0.0001 | <0.0001 |
| Age Group | Children/Adolescents 6–17 years (n = 748) | Adults 18–75 years (n = 2909) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Dietary Quality T1 | Medium Dietary Quality T2 | High Dietary Quality T3 | Low Dietary Quality T1 | Medium Dietary Quality T2 | High Dietary Quality T3 | |||||||||||||
| Mean | SD | Mean | SD | Mean | SD | p * | p ** | p *** | Mean | SD | Mean | SD | Mean | SD | p * | p ** | p *** | |
| NRF 9.3 | 538 | 66 | 644 | 20 | 729 | 41 | 571 | 66 | 685 | 30 | 774 | 95 | ||||||
| Energy (kJ) | 1720 | 750 | 1632 | 628 | 1620 | 630 | <0.0001 | <0.0001 | <0.0001 | 1861 a | 1021 | 1727 a | 741 | 1682 b | 701 | <0.0001 | <0.0001 | 0.0007 |
| Carbohydrates (g) | 60 b | 27 | 60 b | 25 | 62 a | 27 | <0.0001 | 0.0008 | 0.0003 | 56 c | 30 | 57 b | 26 | 61 a | 28 | <0.0001 | <0.0001 | <0.0001 |
| Carbohydrates (%E) | 58 c | 11 | 60 b | 9 | 63 a | 8 | <0.0001 | <0.0001 | <0.0001 | 51 c | 14 | 54 b | 11 | 58 a | 11 | <0.0001 | <0.0001 | <0.0001 |
| Added sugars (g) | 11 a | 9 | 9 b | 7 | 7 c | 7 | <0.0001 | <0.0001 | <0.0001 | 10 a | 11 | 7 b | 8 | 7 a,b | 8 | <0.0001 | 0.0049 | 0.0203 |
| Added sugars (%E) | 11 a | 8 | 9 b | 6 | 7 c | 5 | <0.0001 | <0.0001 | <0.0001 | 10 a | 12 | 7 b | 7 | 7 b | 7 | <0.0001 | <.0001 | <0.0001 |
| Proteins (g) | 14 b | 7 | 14 b | 6 | 15 a | 7 | <0.0001 | <0.0001 | <0.0001 | 16 c | 10 | 16 b | 8 | 16 a | 7 | <0.0001 | <0.0001 | <0.0001 |
| Proteins (%E) | 14 b | 4 | 14 b | 3 | 16 a | 4 | <0.0001 | <0.0001 | <0.0001 | 15 c | 7 | 16 b | 4 | 17 a | 5 | <0.0001 | <0.0001 | <0.0001 |
| Fat (g) | 13 a | 8 | 11 b | 6 | 9 c | 5 | <0.0001 | <0.0001 | <0.0001 | 18 a | 13 | 14 b | 8 | 11 a | 7 | <0.0001 | <0.0001 | <0.0001 |
| Fat (%E) | 28 a | 10 | 25 b | 9 | 21 c | 7 | <0.0001 | <0.0001 | <0.0001 | 34 a | 12 | 29 b | 10 | 25 c | 9 | <0.0001 | <0.0001 | <0.0001 |
| SFA (g) | 7 a | 4 | 5 b | 3 | 4 c | 2 | <0.0001 | <0.0001 | <0.0001 | 9 a | 7 | 7 b | 4 | 5 c | 3 | <0.0001 | <0.0001 | <0.0001 |
| SFA (%E) | 14 a | 6 | 12 b | 5 | 9 c | 4 | <0.0001 | <0.0001 | <0.0001 | 17 a | 7 | 14 b | 6 | 10 c | 5 | <0.0001 | <0.0001 | <0.0001 |
| Dietary fibre (g) | 4 c | 2 | 4 b | 2 | 5 a | 3 | <0.0001 | <0.0001 | <0.0001 | 4 c | 2 | 5 b | 3 | 6 a | 3 | <0.0001 | <0.0001 | <0.0001 |
| Age Group | Children/Adolescents 6–17 years (n = 748) | Adults 18–75 years (n = 2909) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Dietary Quality T1 | Medium Dietary Quality T2 | High Dietary Quality T3 | Low Dietary Quality T1 | Medium Dietary Quality T2 | High Dietary Quality T3 | |||||||||||||
| Mean | SD | Mean | SD | Mean | SD | p * | p ** | p *** | Mean | SD | Mean | SD | Mean | SD | p * | p ** | p *** | |
| Thiamin (mg) | 0.27 c | 0.13 | 0.28 b | 0.13 | 0.32 a | 0.16 | <0.0001 | <0.0001 | <0.0001 | 0.23 c | 0.14 | 0.26 b | 0.14 | 0.29 a | 0.14 | <0.0001 | <0.0001 | <0.0001 |
| Riboflavin (mg) | 0.44 a | 0.25 | 0.44 b | 0.22 | 0.49 a | 0.23 | <0.0001 | <0.0001 | <0.0001 | 0.40 c | 0.26 | 0.43 b | 0.22 | 0.45 a | 0.21 | <0.0001 | <0.0001 | <0.0001 |
| Niacin (NE) | 3.5 b | 1.8 | 3.4 a | 1.5 | 4.0 a | 1.7 | <0.0001 | <0.0001 | <0.0001 | 5.4 c | 2.9 | 5.6 b | 2.4 | 5.6 a | 2.2 | <0.0001 | <0.0001 | <0.0001 |
| B6 (mg) | 0.20 b | 0.11 | 0.21 a | 0.10 | 0.25 a | 0.10 | <0.0001 | <0.0001 | <0.0001 | 0.19 c | 0.12 | 0.23 b | 0.13 | 0.25 a | 0.13 | <0.0001 | <0.0001 | <0.0001 |
| Folate (ug) | 61.5 b | 32.6 | 60.6 a | 27.2 | 63.9 a | 27.3 | <0.0001 | 0.0036 | 0.0008 | 63.3 c | 37.1 | 68.5 b | 35.8 | 72.2 a | 39.9 | <0.0001 | <0.0001 | <0.0001 |
| B12 (mg) | 0.91 b | 0.76 | 0.89 a | 0.67 | 1.08 a | 0.66 | <0.0001 | <0.0001 | <0.0001 | 1.01 b | 0.97 | 1.03 a | 0.75 | 1.01 a | 0.64 | <0.0001 | <0.0001 | <0.0001 |
| Biotin (mg) | 6.5 c | 4.4 | 7.6 b | 4.7 | 10.6 a | 6.7 | <0.0001 | <0.0001 | <0.0001 | 7.0 c | 5.6 | 8.4 b | 5.6 | 10.1 a | 6.5 | <0.0001 | <0.0001 | <0.0001 |
| Vit E (alfa-TE) | 1.59 a | 1.66 | 1.26 b | 1.19 | 1.08 c | 0.79 | <0.0001 | 0.0058 | 0.0320 | 1.44 b | 1.33 | 1.40 c | 1.30 | 1.65 a | 1.70 | <0.0001 | <0.0001 | <0.0001 |
| Vit D (ug) | 0.28 a | 0.27 | 0.23 a,b | 0.16 | 0.25 b | 0.19 | <0.0001 | 0.1986 | 0.1432 | 0.34 b | 0.38 | 0.33 b | 0.78 | 0.41 a | 1.54 | <0.0001 | 0.0592 | 0.1035 |
| Vitamin C (mg) | 15.2 b | 21.7 | 14.9 a,b | 17.0 | 16.0 a | 15.7 | <0.0001 | 0.0253 | 0.0041 | 13.0 c | 17.0 | 17.7 b | 20.0 | 21.4 a | 23.5 | <0.0001 | <0.0001 | <0.0001 |
| Vit A (RE) | 136 | 197 | 113 | 151 | 102 | 166 | <0.0001 | 0.0100 | 0.0070 | 201 a | 296 | 154 b | 220 | 112 c | 217 | <0.0001 | <0.0001 | <0.0001 |
| Calcium (mg) | 284 c | 182 | 293 b | 152 | 339 a | 169 | <0.0001 | <0.0001 | <0.0001 | 313 c | 211 | 344 b | 178 | 358 a | 161 | <0.0001 | <0.0001 | <0.0001 |
| Iron (mg) | 1.76 c | 0.86 | 1.88 b | 0.94 | 2.19 a | 1.16 | <0.0001 | <0.0001 | <0.0001 | 1.74 c | 1.04 | 1.89 b | 1.00 | 2.18 a | 1.17 | <0.0001 | <0.0001 | <0.0001 |
| Zinc (mg) | 1.70 c | 0.92 | 1.80 b | 0.88 | 2.18 a | 1.12 | <0.0001 | <0.0001 | <0.0001 | 2.07 c | 1.29 | 2.25 b | 1.11 | 2.39 a | 1.08 | <0.0001 | <0.0001 | <0.0001 |
| Sodium (mg) | 500 a | 255 | 427 b | 203 | 386 b | 201 | <0.0001 | <0.0001 | 0.0010 | 616 a | 421 | 528 a | 313 | 409 b | 239 | <0.0001 | <0.0001 | <0.0001 |
| Iodine (ug) | 46.2 b | 29.3 | 45.7 b | 24.7 | 50.6 a | 25.7 | <0.0001 | 0.0005 | 0.0001 | 38.1 c | 27.8 | 41.4 b | 24.4 | 43.7 a | 22.3 | <0.0001 | <0.0001 | <0.0001 |
| Potassium (mg) | 482 c | 271 | 507 b | 217 | 600 a | 253 | <0.0001 | <0.0001 | <0.0001 | 556 c | 262 | 644 b | 270 | 726 a | 289 | <0.0001 | <0.0001 | <0.0001 |
| Magnesium (mg) | 63.4 c | 37.9 | 74.4 b | 44.5 | 99.0 a | 64.9 | <0.0001 | <0.0001 | <0.0001 | 74.0 c | 39.8 | 90.1 b | 47.2 | 110.7 a | 57.4 | <0.0001 | <0.0001 | <0.0001 |
| Selenium (ug) | 6.54 b | 3.72 | 6.24 b | 2.90 | 7.10 a | 3.21 | <0.0001 | <0.0001 | <0.0001 | 7.49 c | 5.37 | 7.54 b | 4.21 | 7.74 a | 4.37 | <0.0001 | <0.0001 | <0.0001 |
| Age Group | Children/Adolescents 6–17 years (n = 748) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Dietary Quality T1 | Medium Dietary Quality T2 | High Dietary QualityT3 | ||||||||||
| % Consumers (n) | Mean | SD | % Consumers (n) | Mean | SD | % Consumers (n) | Mean | SD | p * | p ** | p*** | |
| Breakfast cereals incl. oats & muesli (g) | 58 (143) | 22 b | 19 | 73 (183) | 20 b | 24 | 82 (204) | 37 a | 33 | <0.0001 | <0.0001 | <0.0001 |
| Porridge (oats, rice etc.) (g) | 10 (25) | 68 | 67 | 13 (33) | 75 | 69 | 18 (42) | 84 | 75 | 0.4253 | 0.4238 | 0.3771 |
| Milk for breakfast cereals (g) | 36 (90) | 75 b | 48 | 50 (125) | 90 b | 62 | 58 (145) | 105 a | 65 | 0.0014 | 0.0010 | 0.0100 |
| Fermented dairy products (g) | 25 (63) | 84 a | 70 | 37 (92) | 72 b | 63 | 29 (72) | 63 b | 49 | 0.0722 | 0.1184 | 0.0869 |
| Non-whole grain wheat bread (g) | 80 (200) | 38 a | 31 | 68 (169) | 34 a | 27 | 60 (151) | 23 b | 20 | <0.0001 | <0.0001 | 0.0002 |
| Whole grain wheat bread (g) | 39 (98) | 28 | 23 | 46 (115) | 29 | 25 | 43 (108) | 27 | 23 | 0.7045 | 0.8552 | 0.9845 |
| Whole grain rye bread (g) | 16 (41) | 19 | 17 | 17 (42) | 16 | 16 | 24 (59) | 19 | 19 | 0.7540 | 0.6835 | 0.7101 |
| Pastry, cakes, biscuits (g) | 18 (44) | 17 | 18 | 13(33) | 13 | 11 | 12(29) | 12 | 7 | 0.5758 | 0.6673 | 0.9216 |
| Fats on bread (g) | 73 (183) | 7a | 6 | 73(182) | 6 a | 4 | 58(146) | 4 b | 4 | <0.0001 | <0.0001 | <0.0001 |
| Cold cuts, cheese, egg on bread (g) | 89 (222) | 22 | 20 | 86(214) | 17 | 14 | 81(202) | 16 | 15 | 0.0026 | 0.0326 | 0.2876 |
| Vegetables, rich in dietary fibre (g) | 1 (2) | 16 | 8 | 5(12) | 9 | 12 | 4(11) | 14 | 13 | 0.3371 | 0.4983 | 0.3407 |
| Vegetables, low in dietary fibre (g) | 3 (8) | 19 | 19 | 5(12) | 12 | 11 | 6(15) | 17 | 16 | 0.8888 | 0.9426 | 0.2989 |
| Fruits (g) | 22 (54) | 45 a | 88 | 35(87) | 33 a,b | 36 | 54(134) | 41b | 52 | 0.2760 | 0.1162 | 0.0787 |
| Beverages total (g) | 97 (242) | 226 b | 134 | 98 (245) | 199 b | 122 | 98 (246) | 219 a | 132 | 0.0560 | 0.0658 | 0.0190 |
| Coffee (g) | 4 (10) | 188 | 170 | 4 (10) | 110 | 80 | 5 (12) | 113 | 67 | 0.7356 | 0.7396 | 0.6723 |
| Tea (g) | 10 (26) | 99 a | 68 | 8 (21) | 81 b | 45 | 13 (33) | 78 b | 69 | 0.1310 | 0.1586 | 0.0819 |
| Water (g) | 38(93) | 106 | 81 | 45(111) | 109 | 103 | 48 (121) | 105 | 104 | 0.8085 | 0.6899 | 0.8720 |
| Milk (incl. milk with chocolate flavor/fruits) (g) | 71 (176) | 153 a,b | 125 | 74 (185) | 122 b | 101 | 74 (186) | 147 a | 101 | 0.0287 | 0.0263 | 0.0019 |
| Juice (g) | 41 (103) | 99 | 87 | 48 (119) | 83 | 81 | 46 (116) | 75 | 63 | 0.0914 | 0.1790 | 0.6084 |
| Cordial (g) | 8 (19) | 66 | 45 | 4 (11) | 53 | 22 | 2 (6) | 76 | 49 | 0.7231 | 0.7352 | 0.4738 |
| Cordial light (g) | 3 (8) | 80 | 84 | 3 (8) | 44 | 30 | 1 (3) | 57 | 49 | 0.3943 | 0.4086 | 0.1834 |
| Carbonated soft drinks sugar sweetened (g) | 6 (14) | 47 | 29 | 1 (2) | 32 | 15 | - | n/a | n/a | 0.7012 | 0.7326 | 0.5374 |
| Carbonated soft drinks sugar light (g) | 0 | n/a | n/a | − (1) | 29 | 0 | − (1) | 21 | n/a | <0.0001 | n/a | n/a |
| Beer (g) | 0 | n/a | n/a | 0 | n/a | n/a | 0 | n/a | n/a | n/a | n/a | n/a |
| Wine/spirits (g) | 0 | n/a | n/a | 0 | n/a | n/a | 0 | n/a | n/a | n/a | n/a | n/a |
| Age Group | Adults 18–75 years (n = 2909) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Dietary Quality T1 | Medium Dietary Quality T2 | High Dietary Quality T3 | ||||||||||
| % Consumers (n) | Mean | SD | % Consumers (n) | Mean | SD | % Consumers (n) | Mean | SD | p * | p ** | p *** | |
| Breakfast cereals incl. oats & muesli (g) | 38 (367) | 27 c | 23 | 57 (551) | 31 b | 25 | 71 (688) | 37 a | 29 | <0.0001 | <0.0001 | <0.0001 |
| Porridge (oats, rice etc.) (g) | 8 (75) | 81 | 67 | 11 (108) | 90 | 91 | 15 (145) | 98 | 94 | 0.6462 | 0.3394 | 0.4779 |
| Milk for breakfast cereals (g) | 22 (217) | 89 b | 50 | 32 (309) | 94 a,b | 51 | 40 (383) | 102 a | 53 | 0.0161 | 0.0009 | 0.0110 |
| Fermented dairy products (g) | 23 (220) | 96 b | 88 | 34 (331) | 100 b | 81 | 42 (406) | 115 a | 85 | 0.0019 | <0.0001 | <0.0001 |
| Non-whole grain wheat bread (g) | 73 (708) | 41a | 34 | 62 (600) | 27 b | 21 | 47 (459 | 20 c | 17 | <0.0001 | <0.0001 | <0.0001 |
| Whole grain wheat bread (g) | 35 (337) | 29 a,b | 22 | 45 (439) | 29 a,b | 22 | 46 (444) | 26b | 22 | 0.0003 | 0.0601 | 0.1251 |
| Whole grain rye bread (g) | 39 (373) | 23 | 18 | 50 (42) | 16 | 16 | 46 (59) | 19 | 19 | 0.0523 | 0.3660 | 0.6989 |
| Pastry, cakes, biscuits (g) | 14 (137) | 17 a | 16 | 11 (104) | 13 a,b | 10 | 9 (84) | 10 b | 9 | 0.0003 | 0.0042 | 0.0396 |
| Fats on bread (g) | 75 (728) | 11 a | 9 | 64 (620) | 7 b | 6 | 43 (419) | 5 c | 5 | <0.0001 | <0.0001 | <0.0001 |
| Cold cuts, cheese, egg on bread (g) | 86 (839) | 43 a | 37 | 88 (854) | 37 a,b | 32 | 82 (798) | 33 b | 32 | <0.0001 | 0.0039 | 0.0292 |
| Vegetables, rich in dietary fibre (g) | 3 (26) | 15 b | 14 | 5 (50) | 30 a | 54 | 6 (58) | 28 a | 42 | 0.1456 | 0.1462 | 0.0852 |
| Vegetables, low in dietary fibre (g) | 6 (58) | 18 | 27 | 7 (63) | 22 | 27 | 7 (65) | 21 | 21 | 0.3237 | 0.1755 | 0.4446 |
| Fruits (g) | 29 (284) | 40c | 41 | 49 (477) | 54 b | 57 | 66 (643) | 67a | 82 | <0.0001 | <0.0001 | <0.0001 |
| Beverages total (g) | 98 (954) | 439 c | 228 | 99 (960) | 475 b | 221 | 98 (963) | 497 a | 229 | <0.0001 | <0.0001 | <0.0001 |
| Coffee (g) | 70 (674) | 113c | 67 | 75 (723) | 291 a | 167 | 75 (724) | 264 b | 158 | <0.0001 | <0.0001 | <0.0001 |
| Tea (g) | 15 (141) | 175 | 144 | 22 (213) | 195 | 172 | 27 (260) | 201 | 169 | 0.4072 | 0.1432 | 0.2605 |
| Water (g) | 51 (498) | 170 c | 128 | 63 (611) | 196 b | 139 | 73 (712) | 224a | 149 | <0.0001 | <0.0001 | <0.0001 |
| Milk (incl. milk with chocolate flavor/fruits) (g) | 37 (256) | 140 | 120 | 37 (358) | 124 | 100 | 33 (322) | 118 | 95 | 0.0567 | 0.3336 | 0.5149 |
| Juice (g) | 29 (283) | 95 | 71 | 36 (348) | 98 | 73 | 36 (349) | 93 | 68 | 0.7467 | 0.9310 | 0.9168 |
| Cordial (g) | 5 (45) | 88 | 74 | 3 (31) | 68 | 49 | 2 (23) | 74 | 80 | 0.2370 | 0.2774 | 0.2553 |
| Cordial light (g) | 3(24) | 99 | 72 | 2 (21) | 80 | 63 | 1 (12) | 91 | 61 | 0.6213 | 0.6174 | 0.4768 |
| Carbonated soft drinks sugar sweetened (g) | 4 (40) | 128 a | 129 | 1 (13) | 47 b | 34 | 1 (5) | 77 a,b | 101 | 0.0037 | 0.0103 | 0.0237 |
| Carbonated soft drinks sugar light (g) | 2 (17) | 142 | 187 | 1 (11) | 55 | 27 | − (3) | 107 | 126 | 0.4415 | 0.6744 | 0.3888 |
| Beer (g) | − (2) | 79 | 44 | − (4) | 159 | 135 | 0 | n/a | n/a | 0.8205 | 0.4893 | 0.3807 |
| Wine/spirits (g) | 3 (30) | 17 | 22 | 3 (30) | 10 | 7 | 4 (42) | 7 | 4 | 0.0012 | 0.0022 | 0.0057 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fagt, S.; Matthiessen, J.; Thyregod, C.; Kørup, K.; Biltoft-Jensen, A. Breakfast in Denmark. Prevalence of Consumption, Intake of Foods, Nutrients and Dietary Quality. A Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1085. https://doi.org/10.3390/nu10081085
Fagt S, Matthiessen J, Thyregod C, Kørup K, Biltoft-Jensen A. Breakfast in Denmark. Prevalence of Consumption, Intake of Foods, Nutrients and Dietary Quality. A Study from the International Breakfast Research Initiative. Nutrients. 2018; 10(8):1085. https://doi.org/10.3390/nu10081085
Chicago/Turabian StyleFagt, Sisse, Jeppe Matthiessen, Camilla Thyregod, Karsten Kørup, and Anja Biltoft-Jensen. 2018. "Breakfast in Denmark. Prevalence of Consumption, Intake of Foods, Nutrients and Dietary Quality. A Study from the International Breakfast Research Initiative" Nutrients 10, no. 8: 1085. https://doi.org/10.3390/nu10081085
APA StyleFagt, S., Matthiessen, J., Thyregod, C., Kørup, K., & Biltoft-Jensen, A. (2018). Breakfast in Denmark. Prevalence of Consumption, Intake of Foods, Nutrients and Dietary Quality. A Study from the International Breakfast Research Initiative. Nutrients, 10(8), 1085. https://doi.org/10.3390/nu10081085