Tocotrienol-Rich Vitamin E from Palm Oil (Tocovid) and Its Effects in Diabetes and Diabetic Nephropathy: A Pilot Phase II Clinical Trial

Abstract
:1. Introduction
2. Materials and Methods
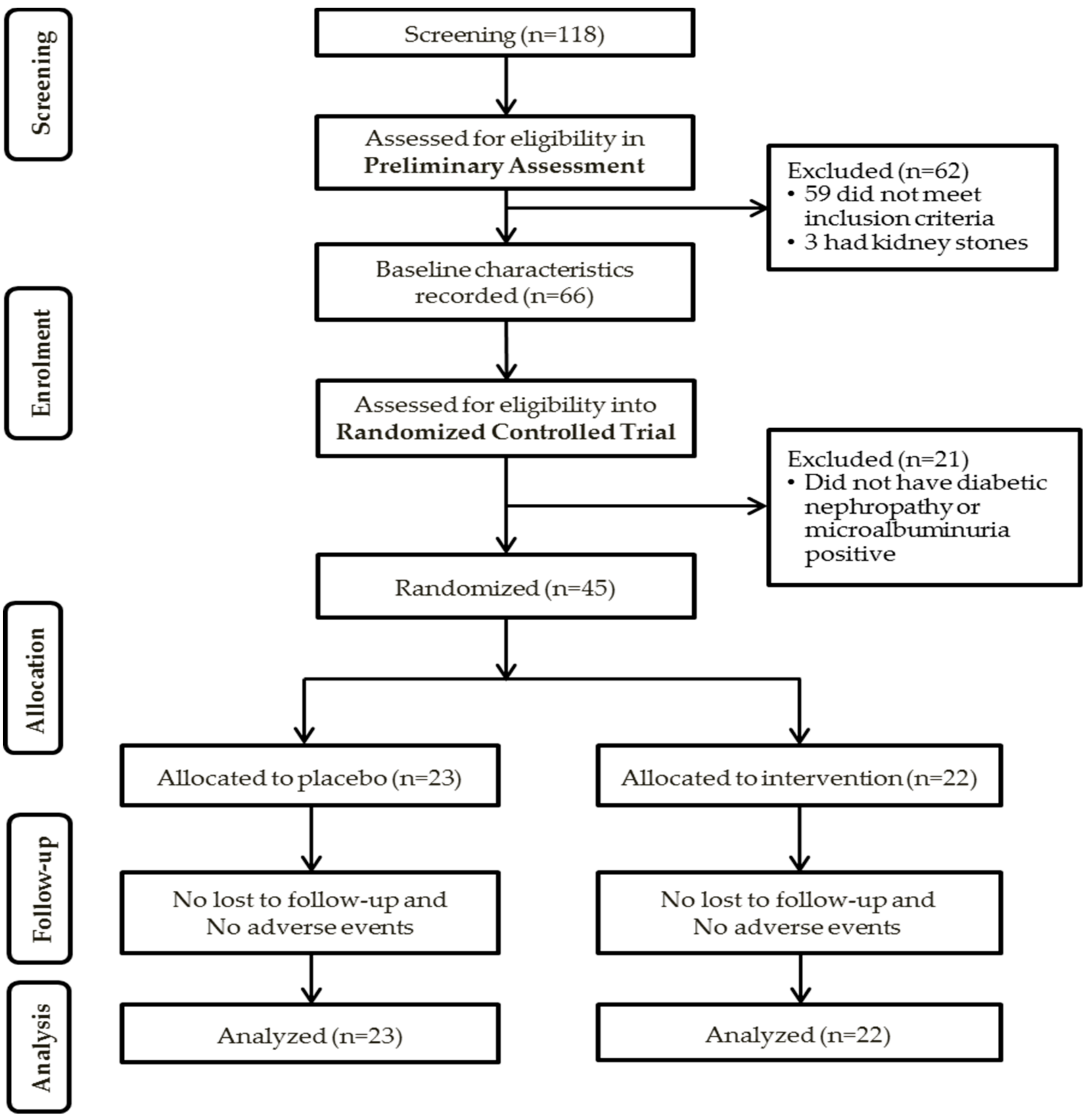
2.1. Participants and Study Enrolment
2.2. Preliminary Assessment
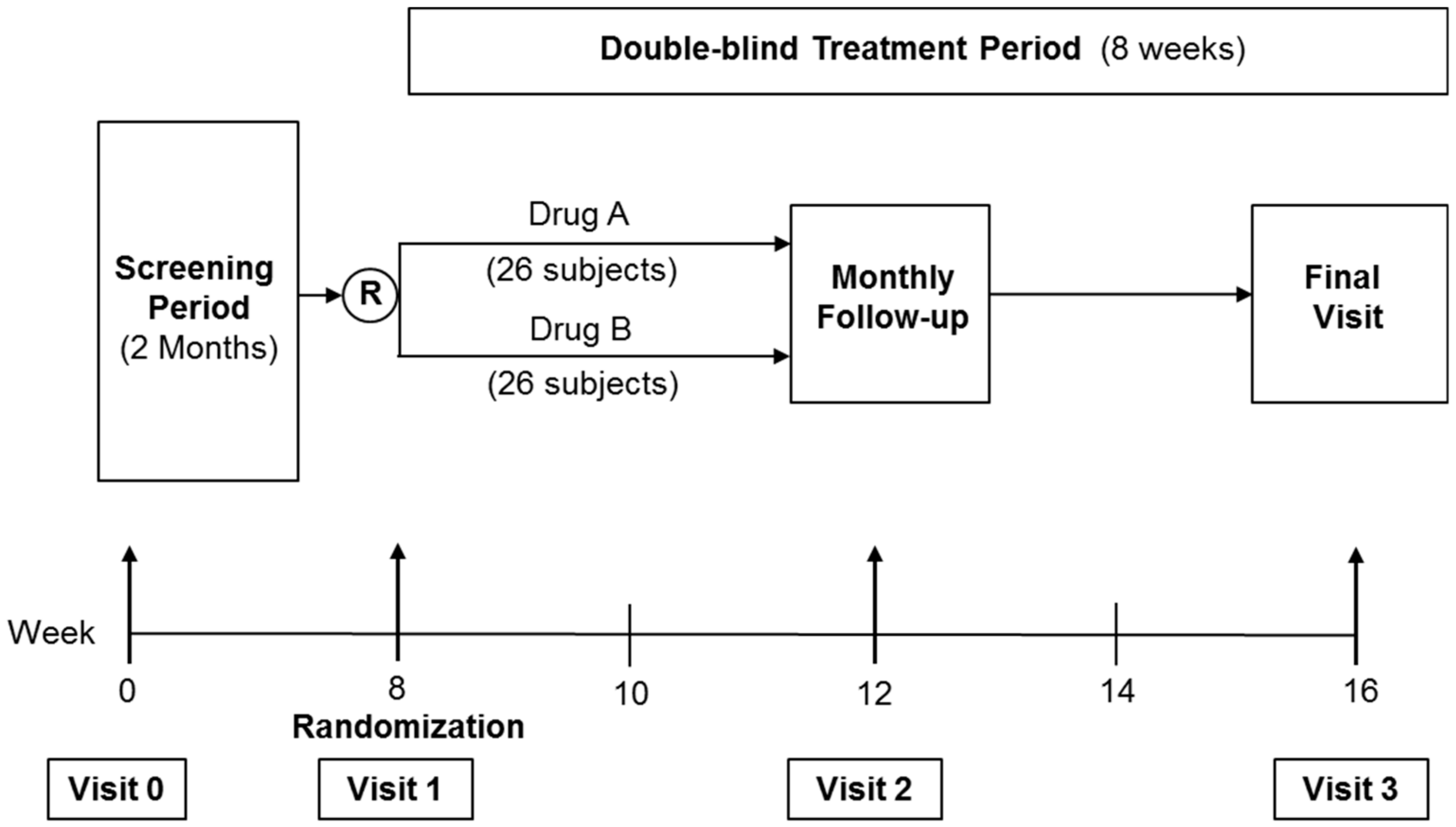
2.3. Randomized Controlled Trial (RCT)
2.4. Sample Size
2.5. Randomization
2.6. Follow-Up Visits
2.7. Assessment of Outcomes
2.8. HbA1c
2.9. BUSE Creatinine, Lipid Profile, and Liver Function Test
2.10. AGE, sRAGE, Nε-CML, and Cystatin C
2.11. UACR
2.12. Statistical Analysis
3. Results
3.1. Preliminary Assessment
3.1.1. Correlations with UACR Grades
3.1.2. Correlations with Serum Creatinine and eGFR
3.1.3. Correlations with Nε-CML
3.1.4. Univariate and Multivariate Analysis
3.2. Randomized Controlled Trial
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016; ISBN 9789241565257. [Google Scholar]
- Bolignano, D.; Cernaro, V.; Gembillo, G.; Baggetta, R.; Buemi, M.; D’Arrigo, G. Antioxidant agents for delaying diabetic kidney disease progression: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0178699. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.J.; Foley, R.N.; Chavers, B.; Gilbertson, D.; Herzog, C.; Ishani, A.; Johansen, K.; Kasiske, B.L.; Kutner, N.; Liu, J.; et al. US Renal Data System 2013 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. Am. J. Kidney Dis. 2014, 63, A4. [Google Scholar] [CrossRef] [PubMed]
- Weyer, C.; Bogardus, C.; Mott, D.M.; Pratley, R.E. The natural history of insulin secretory dysfunction and insulin resistance in the pathogenesis of type 2 diabetes mellitus. J. Clin. Investig. 1999, 104, 787–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etgen, T.; Chonchol, M.; Forstl, H.; Sander, D. Chronic Kidney Disease and Cognitive Impairment: A Systematic Review and Meta-Analysis. Am. J. Nephrol. 2012, 35, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Perlman, R.; Finkelstein, F.; Liu, L.; Roys, E.; Kiser, M.; Eisele, G. Quality of life in chronic kidney disease (CKD): A cross-sectional analysis in the Renal Research Institute-CKD study. Am. J. Kidney Dis. 2005, 45, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Chin, H.; Song, Y.; Lee, J.; Lee, S.; Kim, K.; Na, K. Moderately decreased renal function negatively affects the health-related quality of life among the elderly Korean population: A population-based study. Nephrol. Dial. Transplant. 2008, 23, 2810–2817. [Google Scholar] [CrossRef] [PubMed]
- Khatami, P.G.; Soleimani, A.; Sharifi, N.; Aghadavod, E.; Asemi, Z. The effects of high-dose vitamin E supplementation on biomarkers of kidney injury, inflammation, and oxidative stress in patients with diabetic nephropathy: A randomized, double-blind, placebo-controlled trial. J. Clin. Lipidol. 2016, 10, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Peh, H.Y.; Tan, W.S.; Liao, W.; Wong, W.S. Vitamin E therapy beyond cancer: Tocopherol versus tocotrienol. Pharmacol. Ther. 2016, 162, 152–169. [Google Scholar] [CrossRef] [PubMed]
- Lonn, E.; Yusuf, S.; Hoogwerf, B.; Pogue, J.; Yi, Q.; Zinman, B.; Bosch, J.; Dagenais, G.; Mann, J.F.; Gerstein, H.C.; et al. Effects of vitamin E on cardiovascular and microvascular outcomes in high-risk patients with diabetes: Results of the HOPE study and MICRO-HOPE substudy. Diabetes Care 2002, 25, 1919–1927. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.; Ahsan, H.; Khan, M.R.; Siddiqui, W.A. Protective effects of tocotrienols against lipid-induced nephropathy in experimental type-2 diabetic rats by modulation in TGF-beta expression. Toxicol. Appl. Pharmacol. 2013, 273, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Kuhad, A.; Chopra, K. Attenuation of diabetic nephropathy by tocotrienol: Involvement of NFkB signaling pathway. Life Sci. 2009, 84, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.S.; Ton, S.H.; Tan, J.B.L.; Abdul Kadir, K. The Ameliorative Effects of a Tocotrienol-Rich Fraction on the AGE-RAGE Axis and Hypertension in High-Fat-Diet-Fed Rats with Metabolic Syndrome. Nutrients 2017, 9, 984. [Google Scholar] [CrossRef] [PubMed]
- Nowotny, K.; Jung, T.; Hohn, A.; Weber, D.; Grune, T. Advanced glycation end products and oxidative stress in type 2 diabetes mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, S.I.; Nakamura, N.; Matsui, T. Glycation and cardiovascular disease in diabetes: A perspective on the concept of metabolic memory. J. Diabetes 2017, 9, 141–148. [Google Scholar] [CrossRef] [PubMed]
- UK Prospective Diabetes Study (UKPDS). Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- The Diabetes Control and Complications Trial Research Group (DCCT). The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; DCCT/EDIC Research Group. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study at 30 Years: Overview. Diabetes Care 2014, 37, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. N. Engl. J. Med. 2008, 359, 1577–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aso, Y.; Inukai, T.; Tayama, K.; Takemura, Y. Serum concentrations of advanced glycation endproducts are associated with the development of atherosclerosis as well as diabetic microangiopathy in patients with type 2 diabetes. Acta Diabetol. 2000, 37, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Ono, Y.; Aoki, S.; Ohnishi, K.; Yasuda, T.; Kawano, K.; Tsukada, Y. Increased serum levels of advanced glycation end-products and diabetic complications. Diabetes Res. Clin. Pract. 1998, 41, 131–137. [Google Scholar] [CrossRef]
- Genuth, S.; Sun, W.; Cleary, P.; Sell, D.R.; Dahms, W.; Malone, J.; Sivitz, W.; Monnier, V.M.; DCCT Skin Collagen Ancillary Study Group. Glycation and carboxymethyllysine levels in skin collagen predict the risk of future 10-year progression of diabetic retinopathy and nephropathy in the diabetes control and complications trial and epidemiology of diabetes interventions and complications participants with type 1 diabetes. Diabetes 2005, 54, 3103–3111. [Google Scholar] [PubMed]
- Lee, E.J.; Park, J.H. Receptor for Advanced Glycation Endproducts (RAGE), Its Ligands, and Soluble RAGE: Potential Biomarkers for Diagnosis and Therapeutic Targets for Human Renal Diseases. Genomics Inform. 2013, 11, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Kajikawa, M.; Nakashima, A.; Fujimura, N.; Maruhashi, T.; Iwamoto, Y.; Iwamoto, A.; Matsumoto, T.; Oda, N.; Hidaka, T.; Kihara, Y.; et al. Ratio of serum levels of AGEs to soluble form of RAGE is a predictor of endothelial function. Diabetes Care 2015, 38, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Campion, C.G.; Sanchez-Ferras, O.; Batchu, S.N. Potential Role of Serum and Urinary Biomarkers in Diagnosis and Prognosis of Diabetic Nephropathy. Can. J. Kidney Health Dis. 2017, 4, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Wan Nazaimoon, W.M.; Sakinah, O.; Gapor, A.; Khalid, B.A.K. Effects of palm olein tocopherol and tocotrienol on lipid peroxidation, lipid profiles and glycemic control in non-insulin diabetes mellitus patients. Nutr. Res. 1996, 16, 1901–1911. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; WHO Technical Report Series 894; World Health Organ: Geneva, Switzerland, 2000; pp. 1–253. [Google Scholar]
- Wagner, Z.; Wittmann, I.; Mazak, I.; Schinzel, R.; Heidland, A. Nϵ-(carboxymethyl)lysine levels in patients with type 2 diabetes: Role of renal function. Am. J. Kidney Dis. 2001, 38, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Kubo, K. Relationship between Blood levels of CML and pentosidine and the severity of Microangiopathy in Type 2 diabetes. Endocr. J. 2004, 51, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Coughlan, M.T.; Patel, S.K.; Jerums, G.; Penfold, S.A.; Nguyen, T.V.; Sourris, K.C.; Panagiotopoulos, S.; Srivastava, P.M.; Cooper, M.E.; Burrell, L.M.; et al. Advanced glycation urinary protein-bound biomarkers and severity of diabetic nephropathy in man. Am. J. Nephrol. 2011, 34, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Boesten, D.M.P.H.J.; Elie, A.G.I.M.; Drittij-Reijnders, M.J.; den Hartog, G.J.M.; Bast, A. Effect of Nε-carboxymethyllysine on oxidative stress and the glutathione system in beta cells. Toxicol. Rep. 2014, 1, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Requena, J.; Jenkins, A.; Lyons, T.; Baynes, J.; Thorpe, S. The Advanced Glycation End Product, NGraphic-(Carboxymethyl)lysine, Is a Product of both Lipid Peroxidation and Glycoxidation Reactions. J. Biol. Chem. 1996, 271, 9982–9986. [Google Scholar] [CrossRef] [PubMed]
- Duckworth, W.; Abraira, C.; Moritz, T.; Reda, D.; Emanuele, N.; Reaven, P.D. Glucose Control and Vascular Complications in Veterans with Type 2 Diabetes. N. Engl. J. Med. 2009, 360, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Margolis, K.L.; O’Connor, P.J.; Morgan, T.M.; Buse, J.B.; Cohen, R.M.; Cushman, W.C.; Cutler, J.A.; Evans, G.W.; Gerstein, H.C.; Grimm, R.H., Jr.; et al. Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: The ACCORD randomized trial. Diabetes Care 2014, 37, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- ADVANCE Collaborative Group; Patel, A.; MacMahon, S.; Chalmers, J.; Neal, B.; Billot, L.; Woodward, M.; Marre, M.; Cooper, M.; Glasziou, P.; et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2008, 358, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- UK Prospective Diabetes Study (UKPDS). VIII. Study design, progress and performance. Diabetologia 1991, 34, 877–890. [Google Scholar]



{kind=link}
{kind=link}
| Baseline Characteristics | Participants (N = 66) |
|---|---|
| Gender, n (%) | |
| Male | 48 (72.7) |
| Female | 18 (27.3) |
| Race, n (%) | |
| Malay | 34 (51.5) |
| Chinese | 14 (21.2) |
| Indian | 18 (27.3) |
| Age (years) * | 61.6 ± 9.5 |
| Duration of DM (years) * | 18.5 ± 8.9 |
| HbA1c (%) * | 8.9 ± 1.7 |
| SBP (mmHg) * | 136.7 ± 15.3 |
| DBP (mmHg) * | 77.2 ± 9.1 |
| BMI (kg/m2) * | 29 ± 4.8 |
| UACR Grade (mg/mmol) | N (%) | AGE (µg/mL) | sRAGE (pg/mL) | Nε-CML *,† (ng/mL) | Cystatin C (ng/mL) |
|---|---|---|---|---|---|
| 0–29 | 29 (43.9) | 61.4 ± 95.8 | 956.5 ± 467.8 | 1.46 ± 0.36 | 2235.1 ± 956.7 |
| 30–149 | 29 (43.9) | 159.3 ± 191.6 | 1131.9 ± 395.4 | 2.85 ± 0.36 | 1933.2 ± 906.8 |
| 150–299 | 5 (7.6) | 90.9 ± 65.3 | 1301.9 ± 643.8 | 1.92 ± 0.90 | 1767.7 ± 1114.9 |
| ≥300 | 3 (4.5) | 12.7 ± 9.9 | 1020.6 ± 443.4 | 3.41 ± 1.10 | 2043.8 ± 928.2 |
| UACR Grade (mg/mmol) | N (%) | HbA1c (%) | SBP (mmHg) | DBP (mmHg) | Age (years) | Duration of Diabetes (years) |
|---|---|---|---|---|---|---|
| 0–29 | 29 (43.9) | 8.7 ± 1.6 | 136 ± 11 | 76 ± 8 | 62.5 ± 7.8 | 17.8 ± 9.4 |
| 30–149 | 29 (43.9) | 8.9 ± 1.9 | 136 ± 18 | 79 ± 10 | 61.7 ± 10.4 | 18.8 ± 8.6 |
| 150–299 | 5 (7.6) | 10.2 ± 2.2 | 140 ± 23 | 75 ± 8 | 54.6 ± 14.8 | 20 ± 11.2 |
| ≥300 | 3 (4.5) | 8.9 ± 0.4 | 143 ± 8 | 81 ± 10 | 62.3 ± 2.1 | 20.3 ± 5.7 |
| Baseline Parameters | Serum Creatinine (mmHg) | eGFR (mL/min/1.73 m2) | ||
|---|---|---|---|---|
| Correlation, r | p-Value | Correlation, r | p-Value | |
| AGE (µg/mL) | 0.140 | 0.287 | −0.145 | 0.269 |
| sRAGE (pg/mL) | −0.199 | 0.121 | 0.185 | 0.151 |
| Nε-CML (ng/mL) | 0.31 | 0.015 * | −0.30 | 0.032 * |
| Cystatin C (ng/mL) | −0.238 | 0.061 | 0.164 | 0.199 |
| HbA1c (%) † | 0.116 | 0.369 | −0.049 | 0.704 |
| SBP (mmHg) ‡ | 0.182 | 0.153 | −0.126 | 0.325 |
| DBP (mmHg) ‡ | 0.086 | 0.504 | −0.017 | 0.893 |
| Baseline Parameters | Nε-CML (ng/mL) | |
|---|---|---|
| Correlation, r | p-Value | |
| HbA1c (%) | −0.08 | 0.522 |
| Age (years) | −0.20 | 0.107 |
| Duration of diabetes (years) | 0.06 | 0.625 |
| AGE (µg/mL) ‡ | 0.500 | 0.000 * |
| sRAGE (pg/mL) ‡ | −0.094 | 0.476 |
| Cystatin C (ng/mL) ‡ | −0.180 | 0.169 |
| Baseline Parameters | Simple Logistic Regression | Multiple Logistic Regression a | ||||
|---|---|---|---|---|---|---|
| B | Crude OR (95% CI) | p-Value | B | Adjusted OR ‡ (95% CI) | p-Value | |
| HbA1c (%) | 0.132 | 1.141 (0.852, 1.527) | 0.377 | |||
| SBP (mmHg) | 0.006 | 0.730 (0.974, 1.039) | 0.730 | |||
| DBP (mmHg) | 0.033 | 1.033 (0.978, 1.092) | 0.246 * | |||
| AGE (µg/mL) | 0.004 | 1.004 (1.000, 1.009) | 0.049 * | |||
| sRAGE (pg/mL) | 0.001 | 1.001 (1.000, 1.002) | 0.099 * | |||
| Nε-CML (ng/mL) | 0.357 | 1.429 (1.106, 1.845) | 0.006 * | 0.389 | 1.476 (1.112, 1.996) | 0.008 ** |
| Cystatin C (ng/mL) | 0.000 | 1.000 (0.999, 1.000) | 0.143 * | |||
| General Characteristics | Placebo Group (N = 23) | Tocovid Group (N = 22) | p-Value |
|---|---|---|---|
| Gender | 0.586 | ||
| Male (%) | 15 (65.2) | 16 (72.7) | |
| Female (%) | 8 (34.8) | 6 (27.30 | |
| Race | 0.895 | ||
| Malay (%) | 14 (60.9) | 12 (54.5) | |
| Chinese (%) | 5 (21.7) | 6 (27.3) | |
| Indian (%) | 4 (17.4) | 4 (18.2) | |
| Age (years) | 63.3 ± 10.42 | 59.9 ± 10.24 | 0.283 |
| Duration of DM (years) | 17.9 ± 7.65 | 18.2 ± 10 | 0.893 |
| HbA1c (%) | 8.7 ± 1.5 | 9.0 ± 2 | 0.611 |
| SBP (mmHg) | 138.8 ± 15 | 136.2 ± 18.4 | 0.601 |
| DBP (mmHg) | 78.5 ± 9.4 | 77.0 ± 10.2 | 0.617 |
| Weight (kg) | 78.3 ± 12.8 | 78.2 ± 16.5 | 0.983 |
| BMI (kg/m2) | 29.3 ± 4.7 | 29.4 ± 5.4 | 0.978 |
| Renal Parameters: | |||
| UACR (mg/mmol) | 128.7 ± 164.7 | 66.4 ± 61.8 | 0.101 |
| Serum Creatinine (umol/L) | 125.5 ± 56.6 | 120.2 ± 57.9 | 0.761 |
| eGFR (mL/min/1.73 m²) | 57.5 ± 25.1 | 63.1 ± 24.1 | 0.445 |
| Biomarkers: | |||
| AGE (µg/mL) | 112.2 ± 149.5 | 136.1 ± 188.4 | 0.646 |
| sRAGE (pg/mL) | 1060.9 ± 438.8 | 1099.9 ± 408 | 0.759 |
| Nε-CML (ng/mL) | 2.4 ± 2.2 | 2.7 ± 2.5 | 0.695 |
| Cystatin C (ng/mL) | 1947.5 ± 1078 | 1941.3 ± 837 | 0.983 |
| Safety Tests: | |||
| Urea (mmol/L) | 8.4 ± 4.7 | 6.3 ± 3.5 | 0.095 |
| Total chol (mmol/L) | 4.2 ± 0.9 | 4.6 ± 0.9 | 0.192 |
| HDL (mmol/L) | 1.1 ± 0.3 | 1.2 ± 0.2 | 0.728 |
| AST (UI/L) | 19.2 ± 6.9 | 25.4 ± 9.1 | 0.013 * |
| ALT (UI/L) | 19.3 ± 11 | 29 ± 15.7 | 0.020 * |
| Analytes | Placebo Group | Tocovid Group | Mean Difference | p-Value † |
|---|---|---|---|---|
| HbA1c (%) | 8.61 ± 0.17 | 8.45 ± 0.17 | −0.16 ± 0.24 | 0.518 |
| SBP (mmHg) | 137.09 ± 2.81 | 130.48 ± 2.88 | −6.62 ± 4.03 | 0.108 |
| DBP (mmHg) | 77.61 ± 1.78 | 77.91 ± 1.82 | 0.297 ± 2.57 | 0.909 |
| Weight (kg) | 78.22 ± 0.84 | 79.47 ± 0.86 | 1.24 ± 1.20 | 0.308 |
| Renal parameters: | ||||
| UACR (mg/mmol) | 66.93 ± 8.93 | 85.43 ± 9.14 | 18.45 ± 12.97 | 0.161 |
| Sr Creatinine (μmol/L) | 131.04 ± 2.92 | 119.76 ± 2.92 | −11.28 ± 4.31 | * 0.014 ‡ |
| eGFR (mL/min/1.73 m²) | 74.89 ± 11.51 | 63.57 ± 11.77 | −11.31 ± 16.51 | 0.497 |
| Serum biomarkers: | ||||
| AGE (µg/mL) | 83.66 ± 27.20 | 89.82 ± 27.20 | 6.16 ± 38.50 | 0.874 |
| sRAGE (pg/mL) | 1088.32 ± 111.65 | 1246.36 ± 114.16 | 158.05 ± 159.77 | 0.328 |
| Nε-CML (ng/mL) | 2.56 ± 0.48 | 2.59 ± 0.49 | 0.28 ± 0.69 | 0.967 |
| Cystatin C (ng/mL) | 2172.45 ± 181.56 | 2031.99 ± 185.64 | −140.46 ± 259.66 | 0.591 |
| Safety tests: | ||||
| Urea (mmol/L) | 7.33 ± 0.37 | 7.26 ± 0.38 | −0.07 ± 0.54 | 0.896 |
| Total chol (mmol/L) | 4.52 ± 0.12 | 4.67 ± 0.12 | 0.15 ± 0.17 | 0.384 |
| HDL (mmol/L) | 1.17 ± 0.03 | 1.18 ± 0.03 | 0.01 ± 0.04 | 0.772 |
| AST (IU/L) | 21.21 ± 0.91 | 19.41 ± 0.93 | −1.80 ± 1.35 | 0.190 |
| ALT (IU/L) | 26.45 ± 1.67 | 22.17 ± 1.71 | −4.28 ± 2.46 | 0.089 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, S.M.Q.; Chiew, Y.; Ahmad, B.; Kadir, K.A. Tocotrienol-Rich Vitamin E from Palm Oil (Tocovid) and Its Effects in Diabetes and Diabetic Nephropathy: A Pilot Phase II Clinical Trial. Nutrients 2018, 10, 1315. https://doi.org/10.3390/nu10091315
Tan SMQ, Chiew Y, Ahmad B, Kadir KA. Tocotrienol-Rich Vitamin E from Palm Oil (Tocovid) and Its Effects in Diabetes and Diabetic Nephropathy: A Pilot Phase II Clinical Trial. Nutrients. 2018; 10(9):1315. https://doi.org/10.3390/nu10091315
Chicago/Turabian StyleTan, Suzanne May Quinn, Yilynn Chiew, Badariah Ahmad, and Khalid Abdul Kadir. 2018. "Tocotrienol-Rich Vitamin E from Palm Oil (Tocovid) and Its Effects in Diabetes and Diabetic Nephropathy: A Pilot Phase II Clinical Trial" Nutrients 10, no. 9: 1315. https://doi.org/10.3390/nu10091315
APA StyleTan, S. M. Q., Chiew, Y., Ahmad, B., & Kadir, K. A. (2018). Tocotrienol-Rich Vitamin E from Palm Oil (Tocovid) and Its Effects in Diabetes and Diabetic Nephropathy: A Pilot Phase II Clinical Trial. Nutrients, 10(9), 1315. https://doi.org/10.3390/nu10091315