Marketing Strategy, Serving Size, and Nutrition Information of Popular Children’s Food Packages in Taiwan



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Coding Procedure and Coded Content
2.3. Nutritional Information and HNM Strategies
2.4. Interrater Reliability and Data Analysis
3. Results
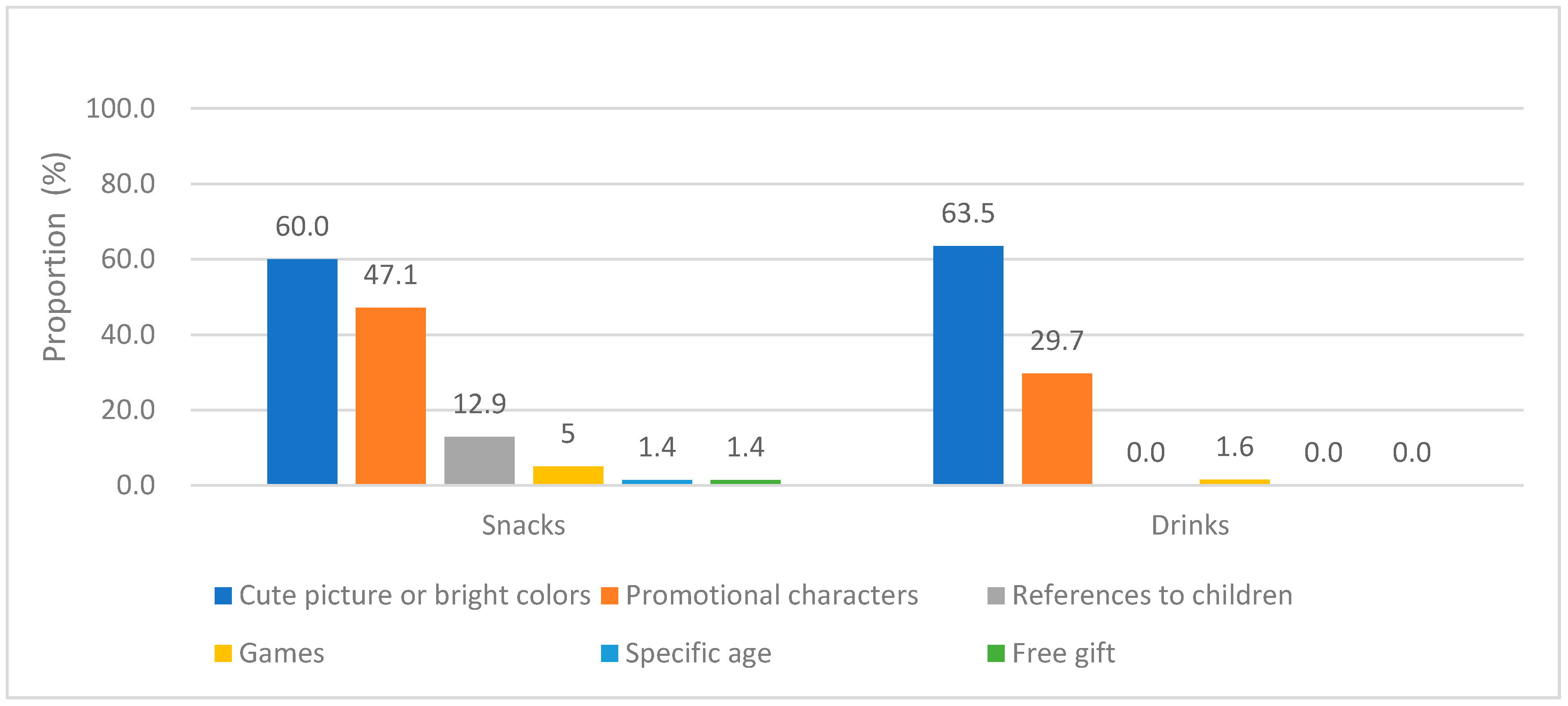
3.1. Marketing Strategy Distribution of Snacks and Drinks
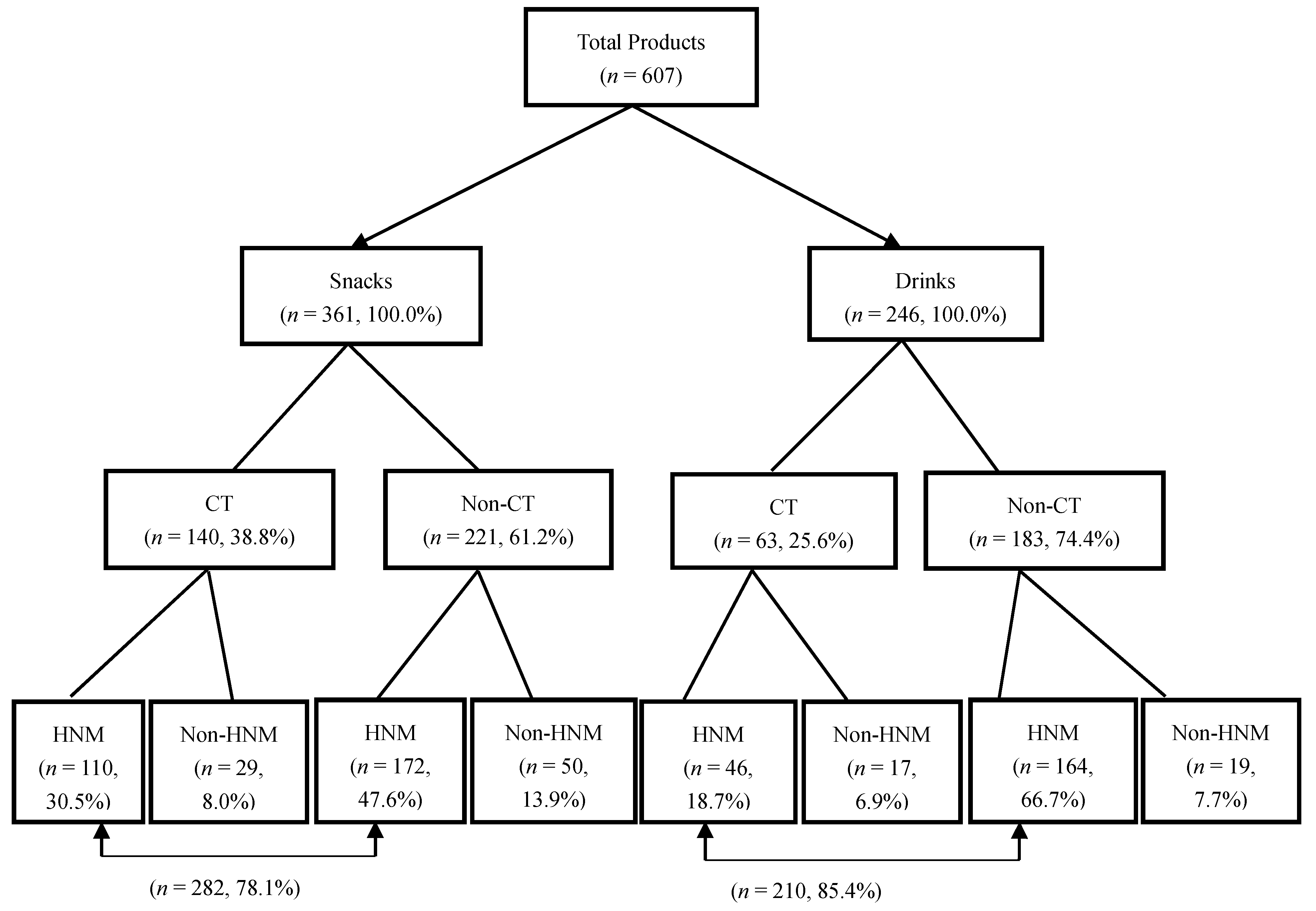
3.2. CT and HNM
3.3. Serving Sizes and Nutritional Information of Products
3.4. HNM Versus Nutritional Quality
3.5. Nutritional Quality of Products with Low Fat or Sugar-related Claims
4. Discussion
4.1. Marketing Strategy of Snacks and Drinks
4.2. Serving Size, Calorie, and Nutrition Information
4.3. Nutrition Quality versus Marketing Strategy
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5·24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Hu, F.B. Sugar Sweetened Beverages, Obesity, Type 2 Diabetes and Cardiovascular Disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Akil, L.; Ahmad, H.A. Relationships between Obesity and Cardiovascular Diseases in Four Southern States and Colorado. J. Health Care Poor U 2011, 22, 61–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health and Welfare. Obesity Prevention of White Paper. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=1405&pid=8920 (accessed on 20 October 2018).
- World Health Organization. Set of Recommendations on the Marketing of Foods and Non-Alcoholic Beverages to Children. Available online: https://www.who.int/dietphysicalactivity/publications/recsmarketing/en/ (accessed on 20 October 2018).
- Rodrigues, V.; Rayner, M.; Fernandes, A.; de Oliveira, R.; Proença, R.; Fiates, G. Nutritional quality of packaged foods targeted at children in Brazil: Which ones should be eligible to bear nutrient claims? Int. J. Obes. 2017, 41, 71. [Google Scholar] [CrossRef]
- Elliott, C. Packaging health: Examining “better-for-you” foods targeted at children. Can. Public Pol. 2012, 38, 265–281. [Google Scholar] [CrossRef]
- Duffey, K.J.; Popkin, B.M. Causes of increased energy intake among children in the US, 1977–2010. Am. J. Prev. Med. 2013, 44, e1–e8. [Google Scholar] [CrossRef]
- Looney, S.M.; Raynor, H.A. Impact of portion size and energy density on snack intake in preschool-aged children. J. Am. Diet. Assoc. 2011, 111, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Ledikwe, J.H.; Ello-Martin, J.A.; Rolls, B.J. Portion sizes and the obesity epidemic. J. Nutr. 2005, 135, 905–909. [Google Scholar] [CrossRef]
- Livingstone, M.B.E.; Pourshahidi, L.K. Portion Size and Obesity. Adv. Nutr. 2014, 5, 829–834. [Google Scholar] [CrossRef] [Green Version]
- Young, L.R.; Nestle, M. The contribution of expanding portion sizes to the US obesity epidemic. Am. J. Public Health 2002, 92, 246–249. [Google Scholar] [CrossRef]
- Colby, S.E.; Johnson, L.; Scheett, A.; Hoverson, B. Nutrition marketing on food labels. J. Nutr. Educ. Behav. 2010, 42, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Dixon, H.; Scully, M.; Wakefield, M.; Kelly, B.; Chapman, K.; Donovan, R. Parent’s responses to nutrient claims and sports celebrity endorsements on energy-dense and nutrient-poor foods: An experimental study. Public Health Nutr. 2011, 14, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F. Meals and snacking, diet quality and energy balance. Physiol. Behav. 2014, 134, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; van der Horst, K.; Jacquier, E.; Eldridge, A.L. Snacking Among US Children: Patterns Differ by Time of Day. J. Nutr. Educ. Behav. 2016, 48, 369–375.e361. [Google Scholar] [CrossRef] [PubMed]
- Piernas, C.; Popkin, B.M. Trends in snacking among US children. Health Aff. 2010, 29, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Kliemann, N.; Kraemer, M.; Scapin, T.; Rodrigues, V.; Fernandes, A.; Bernardo, G.; Uggioni, P.; Proença, R. Serving size and nutrition labelling: Implications for nutrition information and nutrition claims on packaged foods. Nutrients 2018, 10, 891. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Food and Drug Administration. Regulations on Nutrition Labeling for Prepackaged Food Products. Available online: https://www.fda.gov.tw/en/lawContent.aspx?cid=16&id=1633 (accessed on 1 September 2014).
- Orlet Fisher, J.; Rolls, B.J.; Birch, L.L. Children’s bite size and intake of an entree are greater with large portions than with age-appropriate or self-selected portions. Am. J. Clin. Nutr. 2003, 77, 1164–1170. [Google Scholar] [CrossRef]
- Brown, H.M.; Rollo, M.E.; de Vlieger, N.M.; Collins, C.E.; Bucher, T. Influence of the nutrition and health information presented on food labels on portion size consumed: A systematic review. Nutr. Rev. 2018. [Google Scholar] [CrossRef]
- Lyu, L.-C.; Yang, Y.-C.; Yu, H.-W. A long-term follow-up study of sugar sweetened beverages, snacks and desserts, and refined sugar consumption among preschoolers aged 2 to 5 in Taiwan. Taiwan J. Public Health 2013, 32, 346. [Google Scholar] [CrossRef]
- Lythgoe, A.; Roberts, C.; Madden, A.M.; Rennie, K.L. Marketing foods to children: A comparison of nutrient content between children’s and non-children’s products. Public Health Nutr. 2013, 16, 2221–2230. [Google Scholar] [CrossRef]
- World Health Organization. Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Taiwan Food and Drug Administration. Regulations Governing Advertising and Promotion of Unsuitable Food for Children’s Long-term Consumption. Available online: https://www.fda.gov.tw/tc/lawContent.aspx?cid=62&pn=19&id=2909 (accessed on 20 October 2018).
- World Health Organization. Draft Guidelines on Saturated Fatty Acid and Trans-Fatty Acid Intake for Adults and Children. Available online: https://extranet.who.int/dataform/upload/surveys/666752/files/Draft%20WHO%20SFA-TFA%20guidelines_04052018%20Public%20Consultation(1).pdf (accessed on 20 October 2018).
- Elliott, C.D. Sweet and salty: Nutritional content and analysis of baby and toddler foods. J. Public Health 2010, 33, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Lapierre, M.A.; Brown, A.M.; Houtzer, H.V.; Thomas, T.J. Child-directed and nutrition-focused marketing cues on food packaging: Links to nutritional content. Public Health Nutr. 2017, 20, 765–773. [Google Scholar] [CrossRef]
- Canadian Food Inspection Agency. Food Labelling for Industry: Composition and Quality Claims. Available online: http://www.inspection.gc.ca/food/labelling/food-labelling-for-industry/composition-and-quality-claims/eng/1391025998183/1391026062752?chap=3#s11c3 (accessed on 20 October 2018).
- Codex Alimentarius Commission. Guidelines for Use of Nutrition and Health Claims (CAC-GL 23-1997). 1997. Available online: http://www.fao.org/ag/humannutrition/32444-09f5545b8abe9a0c3baf01a4502ac36e4.pdf (accessed on 20 October 2018).
- Administration, T.F.A.D. Regulation on Nutrition Labeling for Prepackaged Food Products. Available online: https://gpmnetfda.blob.core.windows.net/filestorage/332dbdd3-4551-11e5-bef6-0015837488fe/PolicyBulletin2File/44e06b2e-6d3e-48f6-96dc-17c8a78f0f46.pdf (accessed on 20 October 2018).
- Taiwan Ministry of Health and Welfare. Health Food Control Act. Available online: https://consumer.fda.gov.tw/Law/Detail.aspx?nodeID=518&lawid=167 (accessed on 20 October 2018).
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Chacon, V.; Letona, P.; Barnoya, J. Child-oriented marketing techniques in snack food packages in Guatemala. BMC Public Health 2013, 13, 967. [Google Scholar] [CrossRef]
- Rodrigues, V.M.; Rayner, M.; Fernandes, A.C.; de Oliveira, R.C.; da Costa Proença, R.P.; Fiates, G.M.R. Comparison of the nutritional content of products, with and without nutrient claims, targeted at children in Brazil. Br. J. Nutr. 2016, 115, 2047–2056. [Google Scholar] [CrossRef]
- Cairns, G.; Angus, K.; Hastings, G.; Caraher, M. Systematic reviews of the evidence on the nature, extent and effects of food marketing to children. A retrospective summary. Appetite 2013, 62, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kliemann, N.; Veiros, M.B.; Gonzalez-Chica, D.A.; Proenca, R.P.D.C. Serving size on nutrition labeling for processed foods sold in Brazil: Relationship to energy value. Rev. De Nutr. 2016, 29, 741–750. [Google Scholar] [CrossRef] [Green Version]
- Walker, K.Z.; Woods, J.L.; Rickard, C.A.; Wong, C.K. Product variety in Australian snacks and drinks: How can the consumer make a healthy choice? Public Health Nutr. 2008, 11, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Maillot, M.; Darmon, N. Should nutrient profiles be based on 100 g, 100 kcal or serving size? Eur. J. Clin. Nutr. 2009, 63, 898. [Google Scholar] [CrossRef]
- Chan, J.Y.M.; Scourboutakos, M.J.; L’Abbé, M.R. Unregulated serving sizes on the Canadian nutrition facts table—An invitation for manufacturer manipulations. BMC Public Health 2017, 17, 418. [Google Scholar] [CrossRef]
- United States Department of Agriculture. 10 Tips: MyPlate Snack Tips for Parents. Available online: https://www.choosemyplate.gov/ten-tips-snack-tips-for-parents (accessed on 20 October 2018).
- Fisher, J.O.; Kral, T.V. Super-size me: Portion size effects on young children’s eating. Physiol. Behav. 2008, 94, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Change4Life. Me Size Meals. Available online: http://change4lifewales.org.uk/families/mesize/?lang=en (accessed on 20 October 2018).
- Safefood. Parents Urged to Give Children Child-Sized Portions, Not Adult Ones. Available online: https://www.safefood.eu/News/2016/Parents-urged-to-give-children-child-sized-portion.aspx (accessed on 20 October 2018).
- Ferrage, A.; R Fries, L.; Godinot, N.; Labbe, D.; Martin, N. Fairness-Based Tasks for Assessing Children’s Perceptions of Food Quantities and Associations with Portion Selection. Nutrients 2018, 10, 453. [Google Scholar] [CrossRef] [PubMed]
- Devi, A.; Eyles, H.; Rayner, M.; Mhurchu, C.N.; Swinburn, B.; Lonsdale-Cooper, E.; Vandevijvere, S. Nutritional quality, labelling and promotion of breakfast cereals on the New Zealand market. Appetite 2014, 81, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Elliott, C. Assessing ‘fun foods’: Nutritional content and analysis of supermarket foods targeted at children. Obes. Rev. 2008, 9, 368–377. [Google Scholar] [CrossRef]
- Koo, Y.-C.; Chang, J.-S.; Chen, Y.C. Food claims and nutrition facts of commercial infant foods. PLoS ONE 2018, 13, e0191982. [Google Scholar] [CrossRef] [PubMed]
- Seburg, E.M.; Kunin-Batson, A.; Senso, M.M.; Crain, A.L.; Langer, S.L.; Sherwood, N.E. Concern about child weight among parents of children at-risk for obesity. Health Behav. Policy Rev. 2014, 1, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Young, B.M.; de Bruin, A.; Eagle, L. Attitudes of parents toward advertising to children in the UK, Sweden and New Zealand. J. Mark. Mansag. 2003, 19, 475–490. [Google Scholar] [CrossRef]
- Bernstein, J.T.; Franco-Arellano, B.; Schermel, A.; Labonté, M.-È.; L’Abbé, M.R. Healthfulness and nutritional composition of Canadian prepackaged foods with and without sugar claims. Appl. Physiol. Nutr. Metab. 2017, 42, 1217–1224. [Google Scholar] [CrossRef] [Green Version]
- Food Standards Australia and New Zealand. Food Labelling Issues: Quantitative Research with Consumers. Evaluation Report Series No. 4. Available online: http://foodstandards.gov.au/publications/documents/Part_1_with%20App_A.pdf (accessed on 20 October 2018).
- Chien, T.-Y.; Chien, Y.-W.; Chang, J.-S.; Chen, Y.C. Influence of mothers’ nutrition knowledge and attitudes on their purchase intention for infant cereal with no added sugar claim. Nutrients 2018, 10, 435. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Coding Content | Coding Standards |
|---|---|
| General | Product name |
| Information | Brand name |
| Product classification | Snacks or drinks |
| Product category | Cookies, bread, ready-to-eat cereal, pudding/jelly, fruit/vegetable juice, flavored milk, fermented milk, soymilk/rice milk, milk tea |
| Child-targeted strategy | Cute picture or bright colors, promotional characters, references to children, games, specified age ranges or free gifts |
| Nutrition facts | Calorie, carbohydrate, protein, total fat, saturated fat (SFA), sugar, and sodium content |
| Nutritional quality | High fat 1, high SFA 2, high sugar 3, high sodium 4 |
| Health and nutrition marketing strategy | Health symbol, composition claim, nutrition claims, health claim, product names symbolizing the healthiness |
| Health symbol | Fresh fruits or vegetables picture, a natural scenery |
| Composition claim | No added coloring agent, no added preservative, no added flavoring agent, no artificial sweeteners, non GMO (Genetically modified organism) food, not fried, milk content above 50%, no added food additive, organic food, gluten-free, nature source, fresh yeast, no coffee cream, whole grain, no allergens, non-hydrogenation, additives from plants, contains plant oil, no added glutamate flavoring, contains fresh milk, contains health oligosaccharides, modified starch free, contains nuts, contains vegetables, contains fruits, no food additives, nature fruit and vegetable juice, plant milk, no added sugar, no added salt |
| Nutrition claims | No trans-fat, no cholesterol, no fat, low fat, sugar free, contains probiotics and/or prebiotic, contains dietary fiber, contains calcium, contains several vitamins, contains iron, contains oligosaccharides, contains protein or amino acid, low sodium, contains vitamin C, contains vitamin E, contains variety mineral, reduced/low calories, reduced sugar, contains vitamin B1, contains vitamin B2, contains folate, contains ω-3, contains vitamin A, contains vitamin D |
| Health claims | Good for digestion and absorption, good for constitution, good for health, good for enteric flora, nutritionally balanced, good for growth, improve constipation, vitality, good for iron absorption, good for teeth and bone |
| Product names symbolizing the healthiness | Nature, health, nutrition, energetic |
| Sugar-related claims | Sugar free, reduced sugar, no added sugar and no added artificial sweeteners |
| Fat-related claims | Fat free, low fat, no cholesterol, no trans-fat, not fried |
| Snacks | Drinks | |||||
|---|---|---|---|---|---|---|
| Total | CT | Non-CT | Total | CT | Non-CT | |
| HNM strategy 2 | 361 (100.0) | 140 (100.0) | 221 (100.0) | 246 (100.0) | 63 (100.0) | 183 (100.0) |
| Health symbol | 167 (46.3) | 58 (41.4) | 109 (49.3) | 158 (64.2) | 32 (50.8) | 126 (68.9) |
| Composition claim | 163 (45.2) | 69 (49.3) | 94 (42.5) | 94 (38.2) | 21 (33.3) | 73 (39.9) |
| Nutrition claim | 71 (19.7) | 42 (30.0) | 29 (13.1) | 83 (33.7) | 16 (25.4) | 67 (36.6) |
| Health claim | 8 (2.2) | 8 (5.7) | 0 (0.0) | 22 (8.9) | 5 (7.9) | 17 (9.3) |
| Product names symbolizing the healthiness | 14 (3.9) | 5 (3.6) | 9 (4.1) | 8 (3.3) | 1 (1.6) | 7 (3.8) |
| N | Serving Size Range | Serving Size (g or mL) 2 | Calories (kcal) 2 | Calories Density 2 | Serving Size vs. Calories (r) 3 | |
|---|---|---|---|---|---|---|
| Snacks | ||||||
| Cookies | 176 | 4.0–88.0 | 26.0 (14.8) a | 131.7 (71.1) a | 4.99 (0.49) c | 0.97 ** |
| Bread | 80 | 11.0–180.0 | 101.0 (33.0) c | 319.0 (163.1) b | 3.43 (1.00) b | 0.87 ** |
| Ready-to-eat cereal | 68 | 20.0–50.0 | 35.0 (15.0) b | 132.8 (48.6) a | 3.82 (0.26) b | 0.97 ** |
| Pudding/jelly | 37 | 19.3–190.0 | 130.0 (65.0) c | 112.4 (57.0) a | 1.00 (0.37) a | 0.36 * |
| Drinks | ||||||
| Fruit/vegetable juice | 66 | 125.0–650.0 | 250.0 (100.0) b | 107.5 (54.3) a | 0.43 (0.09) a | 0.79 ** |
| Flavored milk | 60 | 125.0–440.0 | 285.0 (114.5) bc | 177.6 (68.8) c | 0.64 (0.09) b | 0.87 ** |
| Fermented milk | 44 | 100.0–359.0 | 213.0 (113.4) a | 132.6 (82.2) ab | 0.65 (0.16) b | 0.87 ** |
| Soymilk/rice milk | 41 | 190.0–450.0 | 250.0 (187.5) bc | 133.3 (81.9) b | 0.52 (0.18) c | 0.78 ** |
| Milk tea | 35 | 236.5–400.0 | 315.3 (132.5) c | 156.0 (66.5) bc | 0.53 (0.19) c | 0.60 ** |
| N (%) | Serving Size | Calorie (kcal) | Carbohydrate (g) | Protein (g) | Fat (g) | Saturated Fat (g) | Sugar (g) | Sodium (mg) | |
|---|---|---|---|---|---|---|---|---|---|
| Median (IQR) | |||||||||
| Cookies | |||||||||
| CT 2 | 85 (48.3) | 26.0 (16.0) | 131.3 (83.1) | 18.6 (8.5) | 1.6 (1.1) | 5.9 (6.0) | 3.0 (3.2) | 5.4 (7.1) | 50.0 (131.4) |
| Non-CT | 91 (51.7) | 25.4 (13.4) | 131.8 (66.5) | 16.5 (8.0) | 1.8 (1.5) | 5.8 (3.1) | 2.9 (1.6) | 4.7 (7.4) | 78.0 (88.3) |
| p-value | 0.362 | 0.993 | 0.004 * | 0.279 | 0.601 | 0.537 | 0.086 | 0.483 | |
| Bread | |||||||||
| CT 2 | 6 (7.5) | 55.0 (48.8) | 192.2 (157.5) | 31.4 (28.7) | 4.1 (4.0) | 4.2 (4.9) | 1.5 (1.3) | 10.1 (11.6) | 87.1 (58.5) |
| Non-CT | 74 (92.5) | 102.0 (30.0) | 347.1 (152.8) | 49.6 (16.0) | 8.3 (3.5) | 12.9 (13.3) | 5.0 (5.8) | 15.1 (9.9) | 289.4 (184.0) |
| p-value | 0.001 * | 0.001 * | 0.004 * | 0.002 * | 0.009 * | 0.003 * | 0.132 | <0.001 ** | |
| Ready-to-eat cereal | |||||||||
| CT 2 | 39 (57.4) | 30.0 (15.0) | 116.0 (54.3) | 22.4 (13.3) | 2.0 (1.0) | 0.9 (1.9) | 0.3 (0.4) | 8.8 (4.8) | 90.0 (81.0) |
| Non-CT | 29 (42.6) | 37.5 (14.0) | 140.8 (50.8) | 30.0 (10.2) | 3.4 (2.1) | 1.9 (2.5) | 0.5 (0.6) | 8.0 (4.1) | 49.0 (105.8) |
| p-value | 0.001 * | 0.002 * | 0.014 * | <0.001 ** | 0.014 * | 0.269 | 0.170 | 0.076 | |
| Pudding/jelly | |||||||||
| CT 2 | 10 (27.0) | 100.0 (34.5) | 103.5 (77.1) | 16.9 (13.7) | 1.1 (2.3) | 1.5 (3.5) | 1.1 (2.6) | 16.0 (20.1) | 50.0 (66.2) |
| Non-CT | 27 (73.0) | 150.0 (55.0) | 114.5 (50.9) | 26.5 (8.9) | 0.2 (4.0) | 0.3 (2.6) | 0.0 (0.8) | 22.3 (8.3) | 68.9 (58.4) |
| p-value | 0.002 * | 0.274 | 0.058 | 0.386 | 0.874 | 0.825 | 0.128 | 0.161 | |
| Fruit/vegetable juice | |||||||||
| CT 2 | 15 (22.7) | 200.0 (75.0) | 88.0 (40.5) | 21.0 (10.6) | 0.4 (1.0) | 0.0 (0.0) | 0.0 (0.0) | 20.0 (8.9) | 27.5 (24.9) |
| Non-CT | 51 (77.3) | 250.0 (105.0) | 112.5 (57.5) | 28.1 (16.0) | 0.0 (0.6) | 0.0 (0.0) | 0.0 (0.0) | 25.8 (13.4) | 47.5 (42.0) |
| p-value | <0.001 ** | 0.004 * | 0.003 * | 0.033 * | 0.340 | 1.000 | 0.005 * | 0.010 * | |
| Flavored milk | |||||||||
| CT 2 | 22 (36.7) | 247.5 (100.0) | 170.9 (66.1) | 23.5 (11.6) | 5.2 (2.7) | 5.0 (1.9) | 3.0 (1.5) | 21.5 (10.7) | 85.0 (62.5) |
| Non-CT | 38 (63.3) | 290.0 (100.3) | 184.7 (80.4) | 27.5 (14.1) | 5.6 (2.4) | 5.3 (3.2) | 3.1 (2.1) | 21.6 (15.0) | 117.4 (81.7) |
| p-value | 0.055 | 0.200 | 0.369 | 0.078 | 0.125 | 0.425 | 0.662 | 0.104 | |
| Fermented milk | |||||||||
| CT 2 | 11 (25.0) | 170.0 (140.0) | 108.8 (68.6) | 25.2 (15.0) | 2.2 (2.8) | 0.0 (0.0) | 0.0 (0.0) | 23.8 (15.5) | 42.5 (38.2) |
| Non-CT | 33 (75.0) | 242.9 (85.7) | 140.0 (69.4) | 25.9 (13.4) | 6.2 (5.7) | 1.2 (3.2) | 0.8 (2.5) | 20.7 (13.7) | 103.0 (92.5) |
| p-value | 0.052 | 0.104 | 0.946 | 0.009 * | 0.017 * | 0.019 * | 0.440 | 0.029 * | |
| Soymilk/rice milk | |||||||||
| CT 2 | 9 (22.0) | 200.0 (50.0) | 115.0 (35.2) | 19.0 (9.3) | 5.0 (1.4) | 3.2 (0.4) | 0.8 (0.1) | 15.4 (9.9) | 66.0 (77.5) |
| Non-CT | 32 (78.0) | 270.0 (153.8) | 143.6 (99.9) | 16.6 (20.6) | 7.4 (7.2) | 5.1 (3.7) | 1.0 (0.8) | 11.1 (18.3) | 29.8 (61.9) |
| p-value | 0.002 * | 0.083 | 0.987 | 0.032 * | 0.007 * | 0.070 | 0.625 | 0.119 | |
| Milk tea | |||||||||
| CT 2 | 6 (17.1) | 357.5 (114.3) | 170.9 (36.8) | 28.2 (8.3) | 5.1 (3.2) | 5.3 (2.5) | 3.9 (1.6) | 26.5 (5.2) | 81.1 (37.5) |
| Non-CT | 29 (82.9) | 312.5 (141.3) | 148.4 (74.3) | 27.8 (8.6) | 2.0 (3.2) | 3.7 (4.3) | 3.0 (3.0) | 23.3 (9.6) | 79.8 (42.0) |
| p-value | 0.658 | 0.246 | 0.662 | 0.062 | 0.430 | 0.776 | 0.314 | 0.710 |
| N (%) | CT | Non-CT | |||
|---|---|---|---|---|---|
| HNM | Non-HNM | HNM | Non-HNM | ||
| Total (Snacks) | 110 (100.0) | 29 (100.0) | 172 (100.0) | 50 (100.0) | |
| High fat 2 | 195 (54.0) | 48 (43.6) | 20 (69.0) | 91 (53.2) | 36 (72.0) |
| High SFA 3 | 215 (59.6) | 52 (47.3) | 23 (79.3) | 102 (59.3) | 38 (76.0) |
| High sugar 4 | 287 (79.5) | 91 (82.7) | 20 (69.0) | 135 (78.5) | 41 (82.0) |
| High sodium 5 | 76 (21.1) | 10 (9.0) | 6 (20.7) | 44 (25.7) | 16 (32.0) |
| Total (Drinks) | 46 (100.0) | 17 (100.0) | 164 (100.0) | 19 (100.0) | |
| High fat 2 | 30 (15.9) | 5 (10.9) | 3 (17.6) | 29 (17.7) | 2 (10.5) |
| High SFA 3 | 96 (39.0) | 13 (28.3) | 10 (58.8) | 61 (37.2) | 12 (63.2) |
| High sugar 4 | 240 (97.6) | 46 (100.0) | 17 (100.0) | 158 (96.3) | 19 (100.0) |
| High sodium 5 | 6 (2.4) | 0 (0.0) | 0 (0.0) | 5 (3.0) | 1 (5.9) |
| Total | High Sugar 2 | High Fat 3 | High SFA 4 | |
|---|---|---|---|---|
| Low sugar related claim | 72 (100.0) | 66 (91.7) | 7 (9.7) | 8 (11.1) |
| Sugar free | 4 (100.0) | 0 (0.0) | 2 (50.0) | 1 (25.0) |
| Reduced sugar | 3 (100.0) | 3 (100.0) | 1 (33.3) | 0 (0.0) |
| No added sugar | 24 (100.0) | 23 (95.8) | 3 (12.5) | 7 (29.2) |
| No added artificial sweeteners | 42 (100.0) | 41 (97.6) | 2 (4.8) | 1 (2.4) |
| Low fat related claim | 84 (100.0) | 72 (85.7) | 13 (15.5) | 12 (14.3) |
| Fat free | 9 (100.0) | 9 (100.0) | 0 (0.0) | 0 (0.0) |
| Low fat | 8 (100.0) | 7 (87.5) | 0 (0.0) | 1 (12.5) |
| No cholesterol | 10 (100.0) | 6 (60.0) | 4 (40.0) | 0 (0.0) |
| No trans fat | 46 (100.0) | 41 (89.1) | 2 (4.3) | 2 (4.3) |
| Not fried | 19 (100.0) | 14 (73.7) | 7 (36.8) | 9 (47.4) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.C.; Chien, Y.-W.; Yang, H.-T.; Chen, Y.C. Marketing Strategy, Serving Size, and Nutrition Information of Popular Children’s Food Packages in Taiwan. Nutrients 2019, 11, 174. https://doi.org/10.3390/nu11010174
Chen MC, Chien Y-W, Yang H-T, Chen YC. Marketing Strategy, Serving Size, and Nutrition Information of Popular Children’s Food Packages in Taiwan. Nutrients. 2019; 11(1):174. https://doi.org/10.3390/nu11010174
Chicago/Turabian StyleChen, Mei Chun, Yi-Wen Chien, Hui-Ting Yang, and Yi Chun Chen. 2019. "Marketing Strategy, Serving Size, and Nutrition Information of Popular Children’s Food Packages in Taiwan" Nutrients 11, no. 1: 174. https://doi.org/10.3390/nu11010174
APA StyleChen, M. C., Chien, Y. -W., Yang, H. -T., & Chen, Y. C. (2019). Marketing Strategy, Serving Size, and Nutrition Information of Popular Children’s Food Packages in Taiwan. Nutrients, 11(1), 174. https://doi.org/10.3390/nu11010174