Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics




Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design
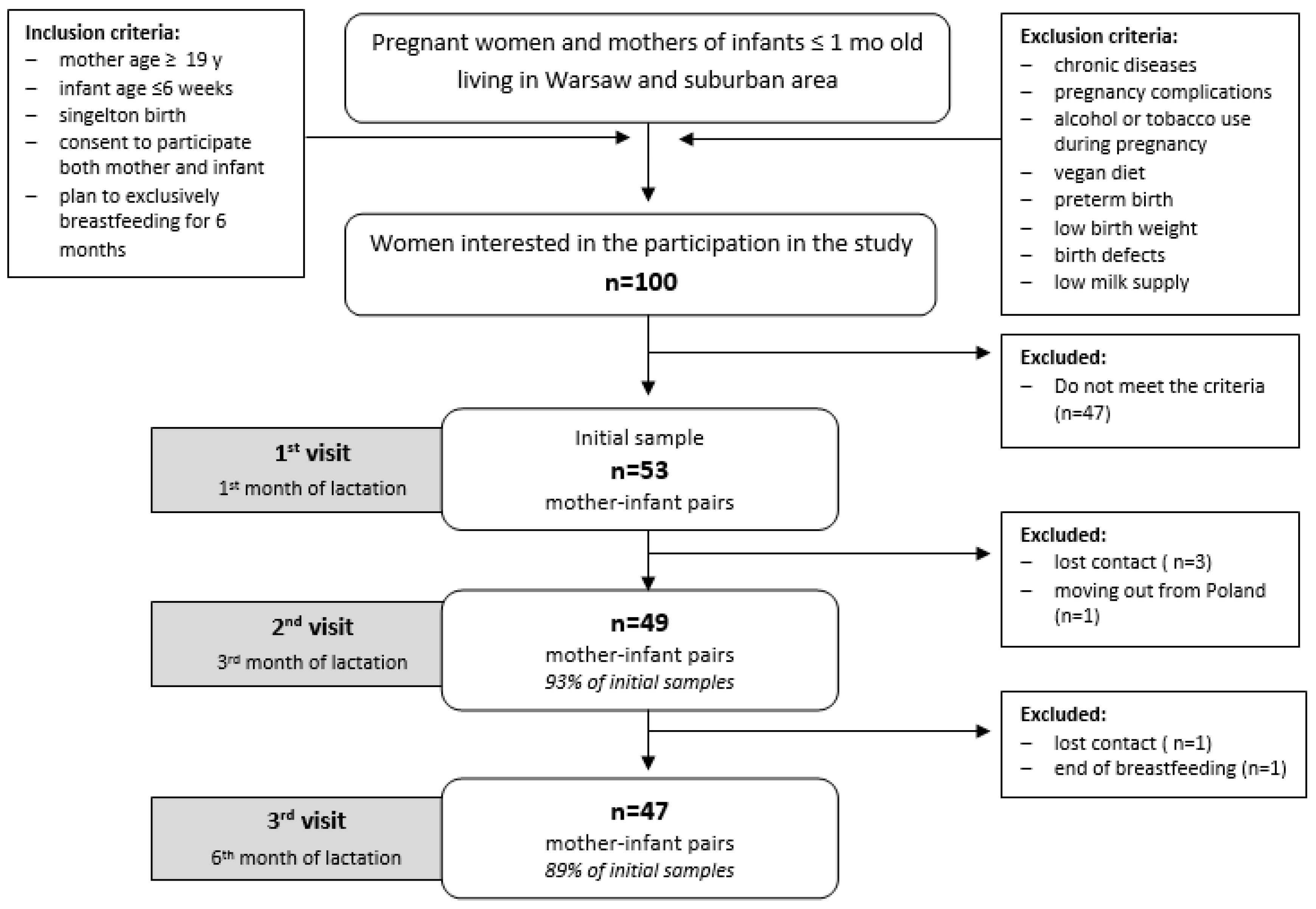
2.3. Study Participants
2.4. Breastmilk Collection
2.5. Breastmilk Composition Analysis
2.6. Breastmilk Carotenoid Analysis
2.7. Dietary Intake Analysis
2.8. Anthropometric Measurements
2.9. Statistical Analysis
3. Results
3.1. Breastmilk Composition and Carotenoid Concentration
3.2. Dietary Intake
3.3. Associations between Carotenoid Concentrations, Dietary Intake and Maternal Characteristics
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization/United Nations Children’s Fund. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Eidelman, A.I.; Schanler, R.J.; Johnston, M.; Landers, S.; Noble, L.; Szucs, K.; Viehmann, L. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Lopez-Alarcon, M.G.; Garza, C. Nutrient Adequacy of Exclusive Breastfeeding for the Term Infant During the First 6 Months of Life; World Health Organization: Geneva, Switzerland, 2001; Available online: http://www.who.int/nutrition/publications/infantfeeding/nut_adequacy_of_exc_bfeeding_eng.pdf/ (accessed on 20 November 2018).
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Zielińska, M.A.; Wesołowska, A.; Pawlus, B.; Hamułka, J. Health Effects of Carotenoids during Pregnancy and Lactation. Nutrients 2017, 9, 838. [Google Scholar] [CrossRef] [PubMed]
- Tsopmo, A. Phytochemicals in human milk and their potential antioxidative protection. Antioxidants 2018, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Mitoulas, L.R.; Kent, J.C.; Cox, D.B.; Owens, R.; Sherriff, J.L.; Hartmann, P.E. Variation in fat, lactose and protein in human milk over 24 h and throughout the first year of lactation. Br. J. Nutr. 2002, 88, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.C.; Mitoulas, L.R.; Cregan, M.D.; Ramsay, D.T.; Doherty, D.A. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics 2006, 117, e387. [Google Scholar] [CrossRef]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef]
- Napierala, M.; Mazela, J.; Merritt, T.A.; Florek, E. Tobacco smoking and breastfeeding: Effect on the lactation process, breast milk composition and infant development. A critical review. Environ. Res. 2016, 151, 321–338. [Google Scholar] [CrossRef]
- Grote, V.; Verduci, E.; Scaglioni, S.; Vecchi, F.; Contarini, G.; Giovannini, M.; Koletzko, B.; Agostoni, C.; European Childhood Obesity Project. Breast milk composition and infant nutrient intakes during the first 12 months of life. Eur. J. Clin. Nutr. 2016, 70, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Bzikowska-Jura, A.; Czerwonogrodzka-Senczyna, A.; Olędzka, G.; Szostak-Węgierek, D.; Weker, H.; Wesołowska, A. Maternal Nutrition and Body Composition During Breastfeeding: Association with Human Milk Composition. Nutrients 2018, 10, 1379. [Google Scholar] [CrossRef] [PubMed]
- Barrera, C.; Valenzuela, R.; Chamorro, R.; Bascuñán, K.; Sandoval, J.; Sabag, N.; Valenzuela, F.; Valencia, M.P.; Puigrredon, C.; Valenzuela, A. The Impact of Maternal Diet during Pregnancy and Lactation on the Fatty Acid Composition of Erythrocytes and Breast Milk of Chilean Women. Nutrients 2018, 10, 839. [Google Scholar] [CrossRef] [PubMed]
- Henjum, S.; Lilleengen, A.M.; Aakre, I.; Dudareva, A.; Gjengedal, E.L.F.; Meltzer, H.M.; Brantsæter, A.L. Suboptimal Iodine Concentration in Breastmilk and Inadequate Iodine Intake among Lactating Women in Norway. Nutrients 2017, 9, 643. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. B vitamins in breast milk: Relative importance of maternal status and intake, and effects on infant status and function. Adv. Nutr. 2012, 3, 362–369. [Google Scholar] [CrossRef]
- Aumeistere, L.; Ciproviča, I.; Zavadska, D.; Bavrins, K.; Borisova, A. Zinc Content in Breast Milk and Its Association with Maternal Diet. Nutrients 2018, 10, 1438. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Campos-Giménez, E.; Redeuil, K.M.; Lévèques, A.; Actis-Goretta, L.; Vinyes-Pares, G.; Zhang, Y.; Wang, P.; Thakkar, S.K. Concentrations of Carotenoids and Tocopherols in Breast Milk from Urban Chinese Mothers and Their Associations with Maternal Characteristics: A Cross-Sectional Study. Nutrients 2017, 9, 1229. [Google Scholar] [CrossRef] [PubMed]
- Ambati, R.R.; Phang, S.M.; Ravi, S.; Aswathanarayana, R.G. Astaxanthin: Sources, extraction, stability, biological activities and its commercial applications—A review. Mar. Drugs 2014, 12, 128–152. [Google Scholar] [CrossRef]
- Saini, R.K.; Nile, S.H.; Park, S.W. Carotenoids from fruits and vegetables: Chemistry, analysis, occurrence, bioavailability and biological activities. Food Res. Int. 2015, 76, 735–750. [Google Scholar] [CrossRef]
- US Department of Agriculture, Agricultural Research Service, Nutrient Data Laboratory. USDA National Nutrient Database for Standard Reference, Legacy. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 20 September 2018).
- Fiedor, J.; Burda, K. Potential role of carotenoids as antioxidants in human health and disease. Nutrients 2014, 6, 466–488. [Google Scholar] [CrossRef]
- Johnson, E.J. Role of lutein and zeaxanthin in visual and cognitive function throughout the lifespan. Nutr. Rev. 2014, 72, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Eggersdorfer, M.; Wyss, A. Carotenoids in human nutrition and health. Arch. Biochem. Biophys. 2018, 652, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Giordano, E.; Quadro, L. Lutein, zeaxanthin and mammalian development: Metabolism, functions and implications for health. Arch. Biochem. Biophys. 2018, 647, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Cena, H.; Castellazzi, A.M.; Pietri, A.; Roggi, C.; Turconi, G. Lutein concentration in human milk during early lactation and its relationship with dietary lutein intake. Public Health Nutr. 2009, 12, 1878–1884. [Google Scholar] [CrossRef]
- Canfield, L.M.; Clandinin, M.T.; Davies, D.P.; Fernandez, M.C.; Jackson, J.; Hawkes, J.; Goldman, W.J.; Pramuk, K.; Reyes, H.; Sablan, B.; et al. Multinational study of major breast milk carotenoids of healthy mothers. Eur. J. Nutr. 2003, 42, 133–141. [Google Scholar]
- Jackson, J.G.; Zimmer, J.P. Lutein and zeaxanthin in human milk independently and significantly differ among women from Japan, Mexico, and the United Kingdom. Nutr. Res. 2007, 27, 449–453. [Google Scholar] [CrossRef]
- Lipkie, T.E.; Morrow, A.L.; Jouni, Z.E.; McMahon, R.J.; Ferruzzi, M.G. Longitudinal survey of carotenoids in human milk from urban cohorts in China, Mexico, and the USA. PLoS ONE 2015, 10, e0127729. [Google Scholar] [CrossRef]
- Schweigert, F.J.; Bathe, K.; Chen, F.; Büscher, U.; Dudenhausen, J.W. Effect of the stage of lactation in humans on carotenoid levels in milk, blood plasma and plasma lipoprotein fractions. Eur. J. Nutr. 2004, 43, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, B.S.; Chan, G.; Hoffman, R.O.; Sharifzadeh, M.; Ermakov, I.V.; Gellermann, W.; Bernstein, P.S. Interrelationships between maternal carotenoid status and newborn infant macular pigment optical density and carotenoid status. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5568–5578. [Google Scholar] [CrossRef]
- Xu, X.; Zhao, X.; Berde, Y.; Low, Y.; Kuchan, M. Milk and Plasma Lutein and Zeaxanthin Concentrations in Chinese Breast-Feeding Mother-Infant Dyads with Healthy Maternal Fruit and Vegetable Intake. J. Am. Coll. Nutr. 2018, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wądołowska, L.; Niedźwiedzka, E. Food Frequency Questionnaire FFQ-6. Available online: www.uwm.edu.pl/edu/lidiawadolowska (accessed on 4 November 2018). (In Polish).
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Juczyński, Z.; Ogińska-Bulik, N. PSS-10–Perceived Stress Scale; Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2009. (In Polish) [Google Scholar]
- Matczak, A.; Jaworowska, A.; Ciechanowicz, A.; Fecenec, D.; Stańczak, J.; Zalewska, E. DSR—Children Development Scale DSR; Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2007. (In Polish) [Google Scholar]
- Giuliano, A.R.; Neilson, E.M.; Yap, H.H.; Baier, M.; Canfield, L.M. Methods of nutritional biochemistry quantitation of and inter/intra-individual variability in major carotenoids of mature human milk. J. Nutr. Biochem. 1994, 5, 551–556. [Google Scholar] [CrossRef]
- Jackson, J.G.; Lien, E.L.; White, S.J.; Bruns, N.J.; Kuhlman, C.F. Major carotenoids in mature human milk: Longitudinal and diurnal patterns. J. Nutr. Biochem. 1998, 9, 2–7. [Google Scholar] [CrossRef]
- Macias, C.; Schweigert, F.J. Changes in the concentration of carotenoids, vitamin A, alpha-tocopherol and total lipids in human milk throughout early lactation. Ann. Nutr. Metab. 2001, 45, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Szponar, L.; Wolnicka, K.; Rychlik, E. Album of Photographs of Food Products and Dishes; National Food and Nutrition Institute: Warsaw, Poland, 2000. (In Polish) [Google Scholar]
- Kunachowicz, H.; Nadolna, I.; Przygoda, B.; Iwanow, K. (Eds.) Food Composition Tables; PZWL: Warsaw, Poland, 2017. (In Polish) [Google Scholar]
- ISAK. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2001; Available online: http://www.ceap.br/material/MAT17032011184632.pdf (accessed on 18 November 2018).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of WHO Consultation, WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Xavier, A.A.O.; Díaz-Salido, E.; Arenilla-Vélez, I.; Aguayo-Maldonado, J.; Garrido-Fernández, J.; Fontecha, J.; Sánchez-García, A.; Pérez-Gálvez, A. Carotenoid Content in Human Colostrum is Associated to Preterm/Full-Term Birth Condition. Nutrients 2018, 10, 1654. [Google Scholar] [CrossRef] [PubMed]
- Song, B.J.; Jouni, Z.E.; Ferruzzi, M.G. Assessment of phytochemical content in human milk during different stages of lactation. Nutrition 2013, 29, 195–202. [Google Scholar] [CrossRef]
- Bohn, T.; Desmarchelier, C.; Dragsted, L.O.; Nielsen, C.S.; Stahl, W.; Rühl, R.; Keijer, J.; Borel, P. Host-related factors explaining interindividual variability of carotenoid bioavailability and tissue concentrations in humans. Mol. Nutr. Food Res. 2017, 61, 1600685. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Prime, D.K.; Hepworth, A.R.; Lai, C.T.; Trengove, N.J.; Hartmann, P.E. Investigation of short-term variations in term breast milk composition during repeated breast expression sessions. J. Hum. Lact. 2013, 29, 196–204. [Google Scholar] [CrossRef]
- De Azeredo, V.B.; Trugo, N.M. Retinol, carotenoids, and tocopherols in the milk of lactating adolescents and relationships with plasma concentrations. Nutrition 2008, 24, 133–139. [Google Scholar] [CrossRef]
- Meneses, F.; Trugo, N.M.F. Retinol, β-carotene, and lutein + zeaxanthin in the milk of Brazilian nursing women: Associations with plasma concentrations and influences of maternal characteristics. Nutr. Res. 2005, 25, 443–451. [Google Scholar] [CrossRef]
- Strobel, M.; Tinz, J.; Biesalski, H.K. The importance of beta-carotene as a source of vitamin A with special regard to pregnant and breastfeeding women. Eur. J. Nutr. 2007, 46, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.; Lyden, E.; Furtado, J.; Van Ormer, M.; White, K.; Overby, N.; Anderson-Berry, A. Serum Lycopene Concentrations and Associations with Clinical Outcomes in a Cohort of Maternal-Infant Dyads. Nutrients 2018, 10, 204. [Google Scholar] [CrossRef] [PubMed]
- Litonjua, A.A.; Rifas-Shiman, S.L.; Ly, N.P.; Tantisira, K.G.; Rich-Edwards, J.W.; Camargo, C.A., Jr.; Weiss, S.T.; Gillman, M.W.; Gold, D.R. Maternal antioxidant intake in pregnancy and wheezing illnesses in children at 2 y of age. Am. J. Clin. Nutr. 2006, 84, 903–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamułka, J.; Sulich, A.; Zielińska, M.; Wawrzyniak, A. Assessment of carotenoid intake in a selected group of pregnant women. Probl. Hig. Epidemiol. 2015, 96, 763–768. [Google Scholar]
- Mathews, F.; Yudkin, P.; Smith, R.F.; Neil, A. Nutrient intakes during pregnancy: The influence of smoking status and age. J. Epidemiol. Community Health 2000, 54, 17–23. [Google Scholar] [CrossRef]
- Scaife, A.R.; McNeill, G.; Campbell, D.M.; Martindale, S.; Devereux, G.; Seaton, A. Maternal intake of antioxidant vitamins in pregnancy in relation to maternal and fetal plasma levels at delivery. Br. J. Nutr. 2006, 95, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Watson, P.E.; McDonald, B.W. Seasonal variation of nutrient intake in pregnancy: Effects on infant measures and possible influence on diseases related to season of birth. Eur. J. Clin. Nutr. 2007, 61, 1271–1280. [Google Scholar] [CrossRef]
- Miyake, Y.; Sasaki, S.; Tanaka, K.; Hirota, Y. Consumption of vegetables, fruit, and antioxidants during pregnancy and wheeze and eczema in infants. Allergy 2010, 65, 758–765. [Google Scholar] [CrossRef]
- Johnson, E.J.; Maras, J.E.; Rasmussen, H.M.; Tucker, K.L. Intake of lutein and zeaxanthin differ with age, sex, and ethnicity. J. Am. Diet. Assoc. 2010, 110, 1357–1362. [Google Scholar] [CrossRef]
- Allore, T.; Lemieux, S.; Vohl, M.C.; Couture, P.; Lamarche, B.; Couillard, C. Correlates of the difference in plasma carotenoid concentrations between men and women. Br. J. Nutr. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sherry, C.L.; Oliver, J.S.; Renzi, L.M.; Marriage, B.J. Lutein supplementation increases breast milk and plasma lutein concentrations in lactating women and infant plasma concentrations but does not affect other carotenoids. J. Nutr. 2014, 144, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Lietz, G.; Mulokozi, G.; Henry, J.C.; Tomkins, A.M. Xanthophyll and hydrocarbon carotenoid patterns differ in plasma and breast milk of women supplemented with red palm oil during pregnancy and lactation. J. Nutr. 2006, 136, 1821–1827. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, J.; Noda, K.; Uchikawa, T.; Maruyama, I.; Shimomura, H.; Miyahara, M. Effect of maternal Chlorella supplementation on carotenoid concentration in breast milk at early lactation. Int. J. Food Sci. Nutr. 2014, 65, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Haftel, L.; Berkovich, Z.; Reifen, R. Elevated milk β-carotene and lycopene after carrot and tomato paste supplementation. Nutrition 2015, 31, 443–445. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B. Human Milk Lipids. Ann. Nutr. Metab. 2016, 69, 28–40. [Google Scholar] [CrossRef]
- Widomska, J.; Subczynski, W.K. Why has nature chosen lutein and zeaxanthin to protect the retina? J. Clin. Exp. Ophthalmol. 2014, 5, 326. [Google Scholar] [CrossRef]
- Wang, L.; Gaziano, J.M.; Norkus, E.P.; Buring, J.E.; Sesso, H.D. Associations of plasma carotenoids with risk factors and biomarkers related to cardiovascular disease in middle-aged and older women. Am. J. Clin. Nutr. 2008, 88, 747–754. [Google Scholar] [CrossRef]
- Johnson, E.J.; Hammond, B.R.; Yeum, K.J.; Qin, J.; Wang, X.D.; Castaneda, C.; Snodderly, D.M.; Russell, R.M. Relation among serum and tissue concentrations of lutein and zeaxanthin and macular pigment density. Am. J. Clin. Nutr. 2000, 71, 1555–1562. [Google Scholar] [CrossRef] [Green Version]
- Knight, B.A.; Shields, B.M.; Brook, A.; Hill, A.; Bhat, D.S.; Hattersley, A.T.; Yajnik, C.S. Lower Circulating B12 Is Associated with Higher Obesity and Insulin Resistance during Pregnancy in a Non-Diabetic White British Population. PLoS ONE 2015, 10, e0135268. [Google Scholar] [CrossRef]
- Maffoni, S.; De Giuseppe, R.; Stanford, F.C.; Cena, H. Folate status in women of childbearing age with obesity: A review. Nutr. Res. Rev. 2017, 30, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Keaney, J.F., Jr.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J.; et al. Obesity and systemic oxidative stress: Clinical correlates of oxidative stress in the Framingham Study. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Visit | Assessment | ||||
|---|---|---|---|---|---|
| Breastmilk | Nutritional | Anthropometric | Psychological | ||
| 1st (1st month) | Mother | - macronutrients - carotenoids - fatty acid profile | - Food Frequency Questionnaire FFQ-6 1 [34] - dietary supplement use | - pre-pregnancy, 14 Hbd 2, 27 Hbd body mass - current body mass | - EPDS 3 [35] - PSS-10 4 [36,37] |
| Infant | - | - breastfeeding frequency - dietary supplement use | - birth parameters - body mass - body length - head circumference | - | |
| 2nd (3rd month) | Mother | - macronutrients - carotenoids - fatty acid profile | - 3-day dietary record - carotenoid intake - dietary supplement use | - current body mass | - EPDS 3 [35] - PSS-10 4 [36,37] |
| Infant | - | - breastfeeding frequency - dietary supplement use | - body mass - body length - head circumference | - | |
| 3rd (6th month) | Mother | - macronutrients - carotenoids - fatty acid profile | - 3-day dietary record - carotenoid intake - dietary supplement use | - current body mass | - EPDS 3 [35] - PSS-10 4 [36,37] |
| Infant | - | - breastfeeding frequency - dietary supplement use - introduced to other foods or drinks | - body mass - body length - head circumference | - DSR 5 Scale [38]. | |
| Nutrient (Unit) | Breastmilk Composition Mean Value (95% CI 1) Min–Max | p-Value 2 | ||
|---|---|---|---|---|
| First Month (n = 53) | Third Month (n = 49) | Sixth Month (n = 47) | ||
| Energy (kcal/100 mL) | 69.5 (67.5–71.6) 57.0–89.7 | 68.2 (65.3–71.0) 49.3–95.5 | 68.4 (66.5–70.4) 53.7–90.3 | 0.777 |
| Total fat (g/100 mL) | 3.8 (3.6–4.1) 2.2–6.0 | 3.8 (3.5–4.1) 1.7–6.9 | 3.9 (3.7–4.1) 2.2–6.4 | 0.595 |
| β-carotene (nmol/L) | 33.2 (33.0–33.5) 31.9–36.3 | 33.1 (32.9–33.3) 31.8–35.9 | 33.3 (33.1–33.6) 32.3–35.4 | 0.436 |
| Lycopene (nmol/L) | 112.2 (106.1–118.3) 77.2–169.0 | 111.2 (105.0–117.3) 75.4–176.9 | 110.1 (103.9–116.3) 78.3–176.7 | 0.457 |
| Lutein + zeaxanthin (nmol/L) | 33.0 (26.3–39.7) 2.7–123.2 | 33.0 (24.1–41.8) 3.2–139.9 | 37.1 (26.5–47.8) 1.8–169.0 | 0.640 |
| Nutrient (Unit) | Dietary Intake Mean Value ± SD 1 or (95% CI 2) Min–Max | p-Value 3 | |
|---|---|---|---|
| Third Month (n = 49) | Sixth Month (n = 47) | ||
| Energy (kcal/day) | 2193.7 ± 631.17 1186.5–3914.0 | 2046.2 ± 502.9 1051.4–3317.3 | 0.083 |
| Total fat (g/day) | 84.3 ± 28.5 37.2–185.6 | 76.4 ± 26.1 18.9–135.7 | 0.085 |
| Vitamin E, dietary (mg α-tocopherol Equivalent/day) | 12.6 ± 5.9 4.3–32.7 | 11.4 ± 5.1 4.7–24.5 | 0.258 |
| Vitamin E, dietary & supplements (mg α-tocopherol Equivalent/day) | 21.5 ± 13.9 4.3–57.7 | 13.1 ± 6.7 4.7–27.5 | 0.000 |
| Vitamin A, dietary (µg Retinol Equivalent/day) | 1289.5 ± 591.4 226.4–2447.3 | 1030.1 ± 500.0 213.1–2745.2 | 0.010 |
| Vitamin A, dietary & supplements (µg Retinol Equivalent/day) | 1295.0 ± 588.3 226.4–2447.3 | 1030.1 ± 500.0 213.1–2745.2 | 0.009 |
| β-carotene (µg/day) | 4480.8 (3575.0–5386.7) 319.6–16461.0 | 3441.9 (5037.5–9474.1) 716.2–9552.9 | 0.232 |
| Lycopene (µg/day) | 7897.3 (5465.2–10329.5) 477.2–30472.7 | 7255.8 (5037.5–9474.1) 339.2 – 38852.9 | 0.422 |
| Lutein + zeaxanthin (µg/day) | 2945.2 (1910.8–3979.6) 263.7–16678.9 | 3739.3 (2834.9–4643.7) 128.9–12207.3 | 0.054 |
| Variables | Breastmilk β-carotene r Coefficient (p-Value) | Breastmilk Lycopene r Coefficient (p-Value) | Breastmilk Lutein + Zeaxanthin r Coefficient (p-Value) | |||
|---|---|---|---|---|---|---|
| Third Month (n = 49) | Sixth Month (n = 47) | Third Month (n = 49) | Sixth Month (n = 47) | Third Month (n = 49) | Sixth Month (n = 47) | |
| Maternal characteristic | ||||||
| Maternal age (years) 1 | 0.015 | −0.197 | −0.136 | 0.113 | −0.048 | −0.009 |
| Maternal education 2 | 0.022 | −0.091 | 0.026 | 0.046 | −0.029 | −0.020 |
| Mode of delivery 2 | −0.009 | −0.001 | −0.094 | −0.050 | −0.175 | −0.115 |
| Number of children 2 | 0.079 | 0.061 | −0.003 | 0.105 | 0.057 | 0.037 |
| BMI at third or sixth month (kg/m2) 1 | −0.248 * | −0.337 * | −0.286 * | −0.119 | −0.355* | −0.205 |
| Maternal dietary intake | ||||||
| Carotenoid intake (µg) 1,3 | 0.442 *** | 0.532 *** | 0.374 ** | 0.338 * | 0.711 *** | 0.726 *** |
| Energy intake (kcal/day) 1 | 0.041 | 0.182 | −0.097 | −0.005 | −0.078 | 0.169 |
| Fat intake (g/day) 1 | 0.049 | 0.302 * | −0.197 | −0.155 | −0.105 | 0.167 |
| Vitamin E intake (mg/day) 1 | 0.270 | 0.062 | 0.082 | 0.013 | 0.123 | −0.069 |
| Vitamin A intake (µg/day) 1 | 0.008 | 0.136 | 0.175 | 0.241 | −0.027 | −0.001 |
| Breastmilk composition | ||||||
| Breastmilk fat (g/100 mL) 1 | 0.235 | 0.167 | 0.274 | 0.064 | 0.399 * | 0.237 |
| Model | Dietary Intake | Breastmilk Carotenoids at Third Month of Lactation | Breastmilk Carotenoids at Sixth Month of Lactation | ||||
|---|---|---|---|---|---|---|---|
| β-carotene (n = 49) | Lycopene (n = 49) | Lutein + Zeaxanthin (n = 49) | β-carotene (n = 47) | Lycopene (n = 47) | Lutein + Zeaxanthin (n = 47) | ||
| 1 | β (95% CI) p-value | 0.342 (0.066–0.618) 0.016 | 0.364 (0.087–0.640) 0.011 | 0.711 (0.504–0.917) 0.000 | 0.397 (0.121–0.672) 0.016 | 0.364 (0.084–0.643) 0.012 | 0.779 (0.591–0.967) 0.000 |
| Model parameters | R2 = 0.10 | R2 = 0.11 | R2 = 0.49 | R2 = 0.14 | R2 = 0.11 | R2 = 0.60 | |
| 2 | β (95% CI) p-value | 0.325 (0.054–0.596) 0.020 | 0.369 (0.088–0.650) 0.011 | 0.680 (0.468–0.891) 0.000 | 0.391 (0.116–0.665) 0.006 | 0.379 (0.092–0.665) 0.011 | 0.785 (0.593–0.977) 0.000 |
| Model parameters | R2 = 0.14 0.013 | R2 = 0.10 0.039 | R2 = 0.50 0.000 | R2 = 0.07 0.037 | R2 = 0.10 0.037 | R2 = 0.60 0.000 | |
| 3 | β (95% CI) p-value | 0.325 (0.054–0.596) 0.020 | 0.369 (0.088–0.650) 0.011 | 0.680 (0.468–0.891) 0.000 | 0.391 (0.116–0.665) 0.006 | 0.379 (0.092–0.665) 0.011 | 0.785 (0.593–0.977) 0.000 |
| Model parameters | R2 = 0.06 0.238 | R2 = 0.11 0.126 | R2 = 0.62 0.000 | R2 = 0.29 0.005 | R2 = 0.07 0.191 | R2 = 0.62 0.000 | |
| 4 | β (95% CI) p-value | 0.407 (0.094–0.721) 0.012 | 0.415 (0.104–0.726) 0.010 | 0.730 (0.516–0.943) 0.000 | 0.428 (0.180–0.676) 0.001 | 0.401 (0.089–0.713) 0.013 | 0.644 (0.448–0.840) 0.000 |
| Model parameters | R2 = 0.04 0.337 | R2 = 0.06 0.262 | R2 = 0.51 0.000 | R2 = 0.35 0.003 | R2 = 0.03 0.351 | R2 = 0.68 0.000 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zielinska, M.A.; Hamulka, J.; Wesolowska, A. Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics. Nutrients 2019, 11, 193. https://doi.org/10.3390/nu11010193
Zielinska MA, Hamulka J, Wesolowska A. Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics. Nutrients. 2019; 11(1):193. https://doi.org/10.3390/nu11010193
Chicago/Turabian StyleZielinska, Monika A., Jadwiga Hamulka, and Aleksandra Wesolowska. 2019. "Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics" Nutrients 11, no. 1: 193. https://doi.org/10.3390/nu11010193
APA StyleZielinska, M. A., Hamulka, J., & Wesolowska, A. (2019). Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics. Nutrients, 11(1), 193. https://doi.org/10.3390/nu11010193