The Effect of Vitamin D Supplementation on its Metabolism and the Vitamin D Metabolite Ratio



Abstract
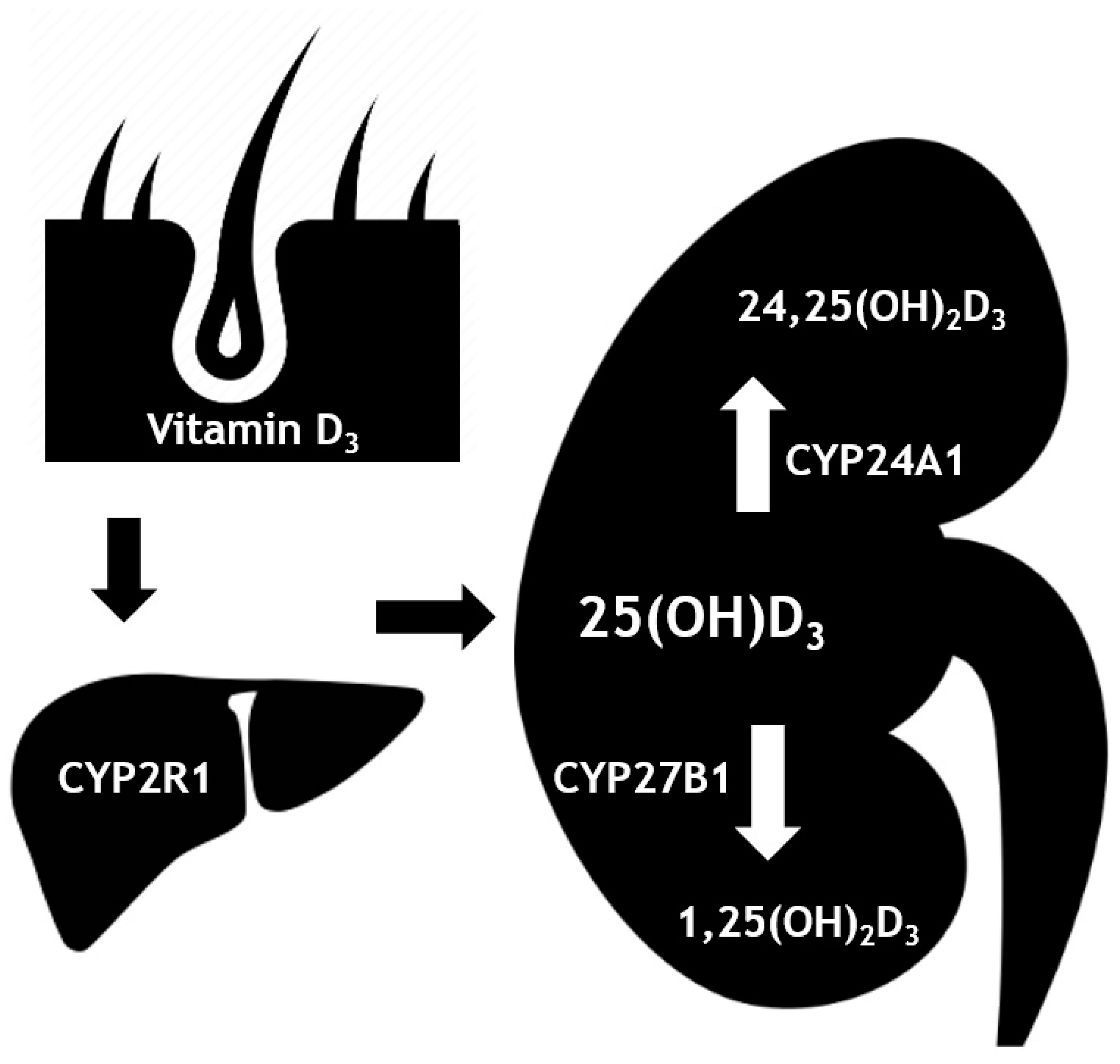
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Measurements
2.3. Statistical Analysis
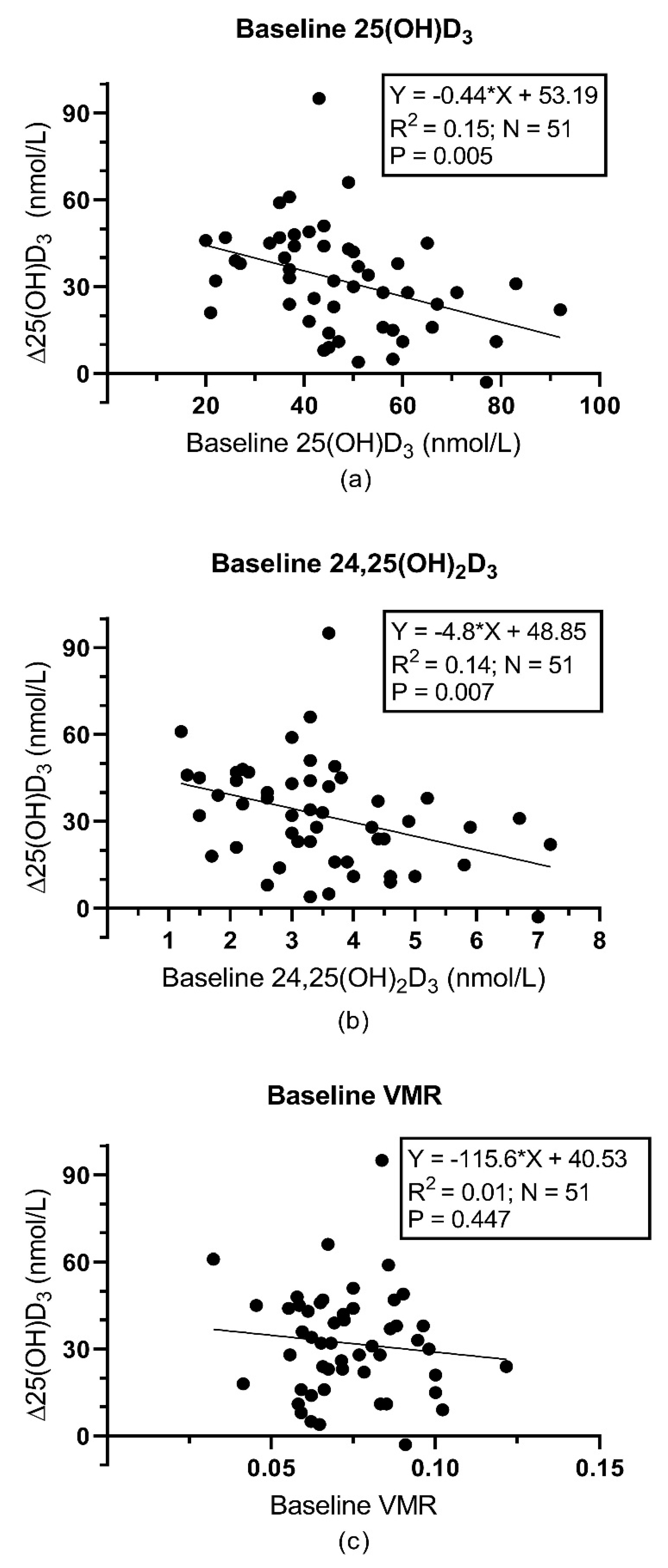
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Baseline Parameters | Δ25(OH)D3 | Δ1,25(OH)2D | Δ24,25(OH)2D3 | |
|---|---|---|---|---|
| 25(OH)D3 | r | −0.508 | −0.277 | −0.657 |
| p-value | 0.013 | 0.201 | 0.001 | |
| Adjusted p-value | 0.104 | 1.000 | 0.008 | |
| 1,25(OH)2D | r | −0.350 | −0.171 | −0.430 |
| p-value | 0.102 | 0.435 | 0.040 | |
| Adjusted p-value | 0.816 | 1.000 | 0.320 | |
| 24,25(OH)2D3 | r | −0.490 | −0.129 | −0.597 |
| p-value | 0.018 | 0.559 | 0.003 | |
| Adjusted p-value | 0.440 | 1.000 | 0.096 | |
| VMR | r | −0.064 | 0.137 | −0.516 |
| p-value | 0.773 | 0.534 | 0.012 | |
| Adjusted p-value | 1.000 | 1.000 | 0.096 | |
| Calculated free 25(OH)D3 * | r | −0.451 | −0.363 | −0.399 |
| p-value | 0.031 | 0.089 | 0.059 | |
| Adjusted p-value | 0.248 | 0.712 | 0.472 | |
| Calculated bioavailable 25(OH)D3 * | r | −0.451 | −0.363 | −0.404 |
| p-value | 0.031 | 0.089 | 0.056 | |
| Adjusted p-value | 0.248 | 0.712 | 0.448 | |
| 1,25(OH)2D/25(OH)D3 * | r | 0.122 | 0.272 | 0.218 |
| p-value | 0.578 | 0.209 | 0.318 | |
| Adjusted p-value | 1.000 | 1.000 | 1.000 | |
| 1,25(OH)2D /24,25(OH)2D3 * | r | 0.126 | 0.136 | 0.211 |
| p-value | 0.565 | 0.536 | 0.333 | |
| Adjusted p-value | 1.000 | 1.000 | 1.000 | |
References
- Bergwitz, C.; Jüppner, H. Regulation of Phosphate Homeostasis by PTH, Vitamin D, and FGF23. Annu. Rev. Med. 2010, 61, 91–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuckey, R.C.; Cheng, C.Y.S.; Slominski, A.T. The Serum Vitamin D Metabolome: What We Know and What is Still to Discover. J. Steroid Biochem. Mol. Biol. 2019, 186, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and immune function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Strugnell, S.A.; DeLuca, H.F. Current Understanding of the Molecular Actions of Vitamin D. Physiol. Rev. 1998, 78, 1193–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirks, N.; Ackermans, M.; Lips, P.; de Jongh, R.; Vervloet, M.; de Jonge, R.; Heijboer, A. The When, What & How of Measuring Vitamin D Metabolism in Clinical Medicine. Nutrients 2018, 10, 482. [Google Scholar] [Green Version]
- Aloia, J.; Fazzari, M.; Shieh, A.; Dhaliwal, R.; Mikhail, M.; Hoofnagle, A.N.; Ragolia, L. The vitamin D metabolite ratio (VMR) as a predictor of functional biomarkers of bone health. Clin. Endocrinol. (Oxf.) 2017, 86, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, C.; Katz, R.; de Boer, I.H.; Kestenbaum, B.R.; Chonchol, M.; Shlipak, M.G.; Sarnak, M.J.; Hoofnagle, A.N.; Rifkin, D.E.; Garimella, P.S.; et al. The 24,25 to 25-hydroxyvitamin D Ratio and Fracture Risk in Older Adults: The Cardiovascular Health Study. Bone 2018, 107, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D.; Hanwell, H.E.; Schnabl, K.; Yazdanpanah, M.; Kimball, S.; Fu, L.; Sidhom, G.; Rousseau, D.; Cole, D.E.C.; Vieth, R. The Ratio of Serum 24,25-dihydroxyvitamin D3 to 25-hydroxyvitamin D3 is Predictive of 25-hydroxyvitamin D3 Response to Vitamin D3 Supplementation. J. Steroid Biochem. Mol. Biol. 2011, 126, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Hayes, A.; Galvin, K.; Merkel, J.; Jones, G.; Kaufmann, M.; Hoofnagle, A.N.; Carter, G.D.; Durazo-Arvizu, R.A.; Sempos, C.T. Significance of Serum 24,25-Dihydroxyvitamin D in the Assessment of Vitamin D Status: A Double-edged Sword? Clin. Chem. 2015, 61, 636–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binkley, N.; Borchardt, G.; Siglinsky, E.; Krueger, D. Does Vitamin D Metabolite Measurement Help Predict 25(OH)D Change Following Vitamin D Supplementation? Endocr. Pract. 2017, 23, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Saleh, L.; Tang, J.; Gawinecka, J.; Boesch, L.; Fraser, W.D.; von Eckardstein, A.; Nowak, A. Impact of a Single Oral Dose of 100,000 IU Vitamin D3 on Profiles of Serum 25(OH)D3 and its Metabolites 24,25(OH)2D3, 3-epi-25(OH)D3, and 1,25(OH)2D3 in Adults with Vitamin D Insufficiency. Clin. Chem. Lab. Med. 2017, 55, 1912–1921. [Google Scholar] [CrossRef] [PubMed]
- Mazahery, H.; von Hurst, P. Factors Affecting 25-Hydroxyvitamin D Concentration in Response to Vitamin D Supplementation. Nutrients 2015, 7, 5111–5142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilz, S.; Gaksch, M.; Kienreich, K.; Grübler, M.; Verheyen, N.; Fahrleitner-Pammer, A.; Treiber, G.; Drechsler, C.; Hartaigh, B.Ó.; Obermayer-Pietsch, B.; et al. Effects of Vitamin D on Blood Pressure and Cardiovascular Risk Factors. Hypertension 2015, 65, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Dirks, N.F.; Ackermans, M.T.; de Jonge, R.; Heijboer, A.C. Reference Values for 24,25-dihydroxyvitamin D and the 25-hydroxyvitamin D/24,25-dihydroxyvitamin D Ratio. Clin. Chem. Lab. Med. 2019, 25, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Powe, C.E.; Ricciardi, C.; Berg, A.H.; Erdenesanaa, D.; Collerone, G.; Ankers, E.; Wenger, J.; Karumanchi, S.A.; Thadhani, R.; Bhan, I. Vitamin D-binding protein modifies the vitamin D-bone mineral density relationship. J. Bone Miner. Res. 2011, 26, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.C.Y.; Jackson, S.; Walsh, N.P.; Greeves, J.; Fraser, W.D. Bioanalytical Facility team The Dynamic Relationships Between the Active and Catabolic Vitamin D Metabolites, their ratios, and Associations with PTH. Sci. Rep. 2019, 9, 6974. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Zittermann, A.; Trummer, C.; Theiler-Schwetz, V.; Lerchbaum, E.; Keppel, M.H.; Grübler, M.R.; März, W.; Pandis, M. Vitamin D testing and treatment: A narrative review of current evidence. Endocr. Connect. 2019, 8, R27–R43. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Sempos, C.T.; Heijboer, A.C.; Bikle, D.D.; Bollerslev, J.; Bouillon, R.; Brannon, P.M.; DeLuca, H.F.; Jones, G.; Munns, C.F.; Bilezikian, J.P.; et al. Vitamin D assays and the definition of hypovitaminosis D: Results from the First International Conference on Controversies in Vitamin D. Br. J. Clin. Pharmacol. 2018, 84, 2194–2207. [Google Scholar] [CrossRef] [PubMed]
- Tsuprykov, O.; Chen, X.; Hocher, C.-F.; Skoblo, R.; Yin, L.; Hocher, B. Why should we measure free 25(OH) vitamin D? J. Steroid Biochem. Mol. Biol. 2018, 180, 87–104. [Google Scholar] [CrossRef] [PubMed]


| Parameter | All (n = 106) | Placebo (n = 54) | Vitamin D (n = 52) | p-value |
|---|---|---|---|---|
| Age (years) | 62.0 (51.3–68.7) | 64.8 (50.8–70.2) | 59.6 (52.4–66.6) | 0.318 |
| Body mass index (kg/m2) | 30.0 ± 5.4 | 29.7 ± 5.9 | 30.3 ± 4.9 | 0.562 |
| Gender (% female) | 57 | 57 | 56 | 0.865 |
| 24,25(OH)2D3 (nmol/L) | 3.5 ± 1.6 | 3.4 ± 1.5 | 3.6 ± 1.5 | 0.419 |
| 25(OH)D3 (nmol/L) | 48 ± 18 | 46 ± 19 | 49 ± 18 | 0.401 |
| VMR ((nmol/L)/(nmol/L)) | 0.073 ± 0.017 | 0.072 ± 0.018 | 0.073 ± 0.017 | 0.768 |
| PTH (pmol/L) | 5.5 (4.1–6.7) | 5.5 (4.0–6.7) | 5.3 (4.1–6.7) | 0.779 |
| 1,25(OH)2D (pmol/L) | 126 ± 53 | 118 ± 52 | 133 ± 52 | 0.142 |
| Serum phosphate (mmol/L) | 0.94 ± 0.17 | 0.96 ± 0.17 | 0.92 ± 0.16 | 0.282 |
| Serum calcium (mmol/L) | 2.26 (2.21–2.33) | 2.26 (2.21–2.34) | 2.26 (2.20–2.33) | 0.773 |
| eGFR (mL/min/1.73m2) | 72 ± 17 | 69 ± 16 | 74 ± 18 | 0.152 |
| 24h urinary calcium excretion (mmol/24h) | 3.30 (1.90–5.00) | 2.95 (1.83–4.78) | 3.70 (2.10–6.30) | 0.222 |
| Calculated free 25(OH)D3 (pmol/L) | 15 (9–21) | 12 (8–21) | 17 (11–20) | 0.153 |
| Vitamin D binding protein (µg/mL) | 247.1 ± 109.5 | 254.8 ± 110.6 | 239.3 ± 109.0 | 0.772 |
| Calculated bioavailable 25(OH)D3 (nmol/L) | 5.9 (3.9–8.2) | 5.2 (3.2–8.5) | 6.6 (4.1–8.0) | 0.149 |
| 1,25(OH)2D /25(OH)D3 ((nmol/L)/(nmol/L)) | 0.0023 (0.0019–0.0036) | 0.0027 (0.0018–0.0039) | 0.0028 (0.0021–0.0035) | 0.753 |
| 1,25(OH)2D /24,25(OH)2D3 ((nmol/L)/(nmol/L)) | 0.036 (0.025–0.05) | 0.036 (0.024–0.051) | 0.035 (0.026–0.050) | 0.893 |
| Parameter | Group | Baseline | Follow-up | Treatment Effect (95% CI) | p-value |
|---|---|---|---|---|---|
| 25(OH)D3 (nmol/L) | Placebo, n=54 | 46 ± 19 | 45 ± 20 | 32 (26 to 39) | <0.001 |
| Vitamin D, n=52 | 49 ± 18 | 79 ± 19 | |||
| 1,25(OH)2D (pmol/L) | Placebo, n=52 | 118 ± 52 | 114 ± 39 | 26 (9 to 42) | 0.003 |
| Vitamin D, n=52 | 133 ± 52 | 150 ± 63 | |||
| 24,25(OH)2D3 (nmol/L) | Placebo, n=54 | 3.4 ± 1.5 | 3.3 ± 1.8 | 3.3 (2.7 to 3.9) | <0.001 |
| Vitamin D, n=52 | 3.6 ± 1.6 | 6.8 ± 1.7 | |||
| VMR | Placebo, n=54 | 0.072 ± 0.018 | 0.071 ± 0.017 | 0.015 (0.010 to 0.020) | <0.001 |
| Vitamin D, n=52 | 0.073 ± 0.017 | 0.087 ± 0.018 | |||
| Calculated free 25(OH)D3 (pmol/L)* | Placebo, n=53 | 12 (8–21) | 12 (8–18) | 12 (6 to 18) | <0.001 |
| Vitamin D, n=51 | 17 (11–20) | 21 (17–31) | |||
| Calculated bioavailable 25(OH)D3 (nmol/L) * | Placebo, n=53 | 5.22 (3.15–8.51) | 4.99 (2.95–6.83) | 4.66 (2.63 to 6.68) | <0.001 |
| Vitamin D, n=51 | 6.60 (4.10–8.02) | 8.69 (6.58–12.51) | |||
| 1,25(OH)2D/ 25(OH)D3 * | Placebo, n=52 | 0.0027 (0.0018–0.0039) | 0.0026 (0.0019–0.0036) | −0.0010 (−0.0013 to −0.0006) | <0.001 |
| Vitamin D, n=52 | 0.0028 (0.0021–0.0035) | 0.0019 (0.0014–0.0026) | |||
| 1,25(OH)2D /24,25(OH)2D3 * | Placebo, n=52 | 0.036 (0.024–0.051) | 0.037 (0.026–0.052) | −0.020 (−0.026 to −-0.015) | <0.001 |
| Vitamin D, n=52 | 0.035 (0.026–0.050) | 0.022 (0.016–0.028) |
| Baseline Parameters | Δ25(OH)D3 | Δ1,25(OH)2D | Δ24,25(OH)2D3 | |
|---|---|---|---|---|
| 25(OH)D3 | r | −0.388 | −0.142 | −0.562 |
| p-value | 0.005 | 0.322 | <0.001 | |
| Adjusted p-value | 0.056 | 1.000 | <0.001 | |
| 1,25(OH)2D | r | −0.287 | −0.260 | −0.272 |
| p-value | 0.041 | 0.065 | 0.053 | |
| Adjusted p-value | 0.328 | 0.520 | 0.424 | |
| 24,25(OH)2D3 | r | −0.374 | −0.122 | −0.476 |
| p-value | 0.007 | 0.392 | <0.001 | |
| Adjusted p-value | 0.056 | 1.000 | 0.003 | |
| VMR | r | −0.109 | −0.027 | −0.015 |
| p-value | 0.448 | 0.850 | 0.916 | |
| Adjusted p-value | 1.000 | 1.000 | 1.000 | |
| Calculated free 25(OH)D3 * | r | −0.373 | −0.281 | −0.382 |
| p-value | 0.007 | 0.046 | 0.006 | |
| Adjusted p-value | 0.056 | 0.368 | 0.048 | |
| Calculated bioavailable 25(OH)D3 * | r | −0.375 | −0.280 | −0.393 |
| p-value | 0.007 | 0.047 | 0.004 | |
| Adjusted p-value | 0.056 | 0.376 | 0.032 | |
| 1,25(OH)2D/25(OH)D3 * | r | −0.004 | −0.058 | 0.176 |
| p-value | 0.980 | 0.687 | 0.216 | |
| Adjusted p-value | 1.000 | 1.000 | 1.000 | |
| 1,25(OH)2D /24,25(OH)2D3 * | r | 0.053 | −0.028 | 0.181 |
| p-value | 0.711 | 0.843 | 0.204 | |
| Adjusted p-value | 1.000 | 1.000 | 1.000 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francic, V.; Ursem, S.R.; Dirks, N.F.; Keppel, M.H.; Theiler-Schwetz, V.; Trummer, C.; Pandis, M.; Borzan, V.; Grübler, M.R.; Verheyen, N.D.; et al. The Effect of Vitamin D Supplementation on its Metabolism and the Vitamin D Metabolite Ratio. Nutrients 2019, 11, 2539. https://doi.org/10.3390/nu11102539
Francic V, Ursem SR, Dirks NF, Keppel MH, Theiler-Schwetz V, Trummer C, Pandis M, Borzan V, Grübler MR, Verheyen ND, et al. The Effect of Vitamin D Supplementation on its Metabolism and the Vitamin D Metabolite Ratio. Nutrients. 2019; 11(10):2539. https://doi.org/10.3390/nu11102539
Chicago/Turabian StyleFrancic, Vito, Stan R. Ursem, Niek F. Dirks, Martin H. Keppel, Verena Theiler-Schwetz, Christian Trummer, Marlene Pandis, Valentin Borzan, Martin R. Grübler, Nicolas D. Verheyen, and et al. 2019. "The Effect of Vitamin D Supplementation on its Metabolism and the Vitamin D Metabolite Ratio" Nutrients 11, no. 10: 2539. https://doi.org/10.3390/nu11102539
APA StyleFrancic, V., Ursem, S. R., Dirks, N. F., Keppel, M. H., Theiler-Schwetz, V., Trummer, C., Pandis, M., Borzan, V., Grübler, M. R., Verheyen, N. D., März, W., Tomaschitz, A., Pilz, S., Heijboer, A. C., & Obermayer-Pietsch, B. (2019). The Effect of Vitamin D Supplementation on its Metabolism and the Vitamin D Metabolite Ratio. Nutrients, 11(10), 2539. https://doi.org/10.3390/nu11102539