Energy Expenditure in Older People Hospitalized for an Acute Episode

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Setting
2.2. Control Population
2.3. Measurements
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Patient Characteristics
3.2. Energy Balance and Physical Activity Level
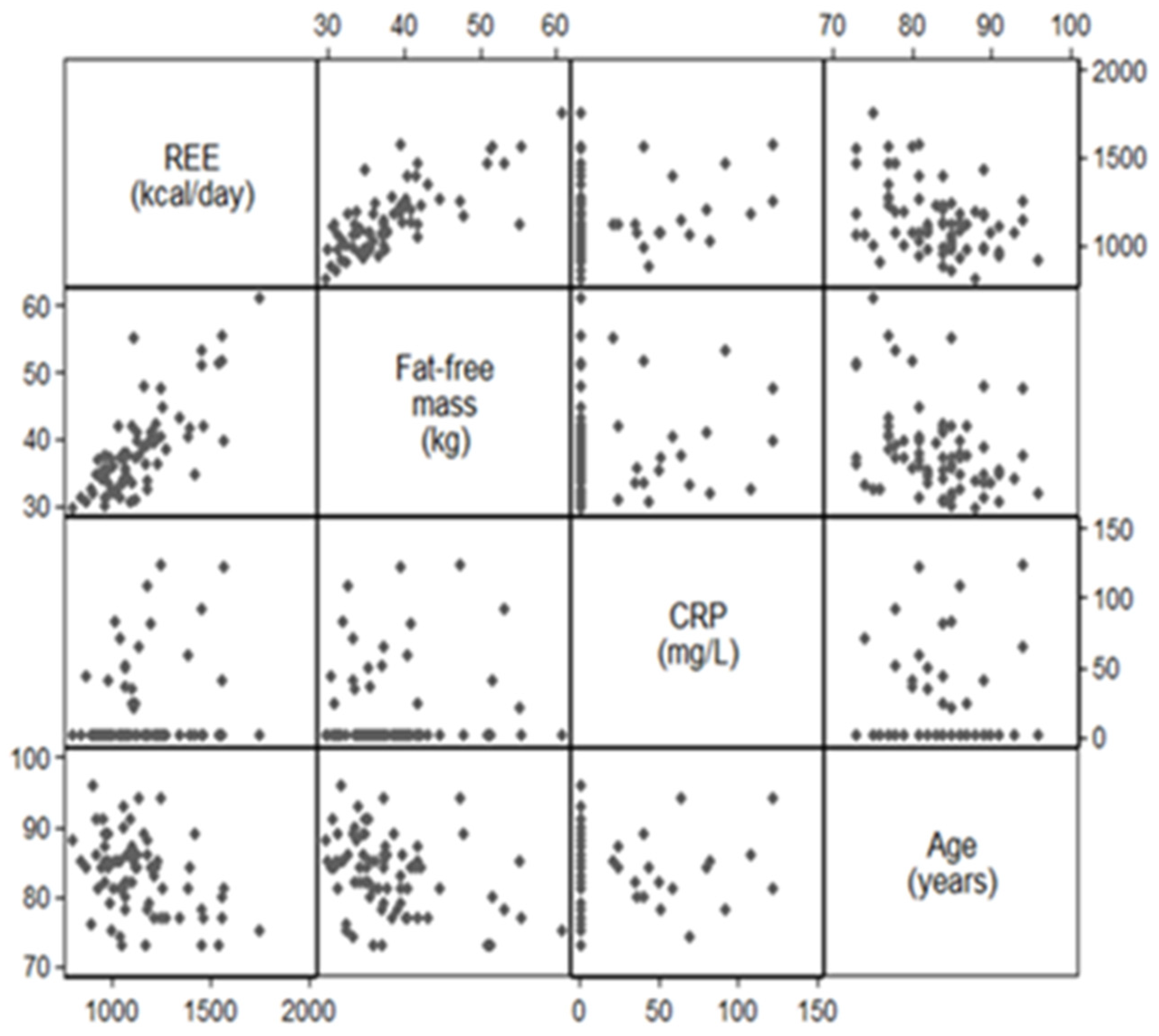
3.3. Associations between REE, Fat-Free Mass, and CRP
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A


Appendix B

References
- Violan, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.; Freitag, M.; Glynn, L.; Muth, C.; Valderas, J.M. Prevalence, determinants and patterns of multimorbidity in primary care: A systematic review of observational studies. PLoS ONE 2014, 9, e102149. [Google Scholar] [CrossRef] [PubMed]
- Inouye, S.K.; Zhang, Y.; Jones, R.N.; Shi, P.; Cupples, L.A.; Calderon, H.N.; Marcantonio, E.R. Risk factors for hospitalization among community-dwelling primary care older patients: Development and validation of a predictive model. Med. Care 2008, 46, 726–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corkins, M.R.; Guenter, P.; DiMaria-Ghalili, R.A.; Jensen, G.L.; Malone, A.; Miller, S.; Patel, V.; Plogsted, S.; Resnick, H.E. American Society for Parenteral and Enteral Nutrition Malnutrition diagnoses in hospitalized patients: United States, 2010. JPEN J. Parenter. Enter. Nutr. 2014, 38, 186–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allard, J.P.; Keller, H.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R.; Gramlich, L.; Payette, H.; Bernier, P.; Vesnaver, E.; Davidson, B.; et al. Malnutrition at Hospital Admission-Contributors and Effect on Length of Stay: A Prospective Cohort Study From the Canadian Malnutrition Task Force. JPEN J. Parenter. Enter. Nutr 2016, 40, 487–497. [Google Scholar] [CrossRef]
- Parker, E.A.; Feinberg, T.M.; Wappel, S.; Verceles, A.C. Considerations When Using Predictive Equations to Estimate Energy Needs Among Older, Hospitalized Patients: A Narrative Review. Curr. Nutr. Rep. 2017, 6, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Noreik, M.; Maurmann, M.; Meier, V.; Becker, I.; Röhrig, G.; Polidori, M.C.; Schulz, R.-J. Resting energy expenditure (REE) in an old-old population: Implications for metabolic stress. Exp. Gerontol. 2014, 59, 47–50. [Google Scholar] [CrossRef] [Green Version]
- Segadilha, N.L.A.L.; Rocha, E.E.M.; Tanaka, L.M.S.; Gomes, K.L.P.; Espinoza, R.E.A.; Peres, W.A.F. Energy Expenditure in Critically Ill Elderly Patients: Indirect Calorimetry vs Predictive Equations. JPEN J. Parenter. Enter. Nutr. 2017, 41, 776–784. [Google Scholar] [CrossRef]
- Dambach, B.; Sallé, A.; Marteau, C.; Mouzet, J.-B.; Ghali, A.; Favreau, A.-M.; Berrut, G.; Ritz, P. Energy requirements are not greater in elderly patients suffering from pressure ulcers. J. Am. Geriatr. Soc. 2005, 53, 478–482. [Google Scholar] [CrossRef]
- Gaillard, C.; Alix, E.; Sallé, A.; Berrut, G.; Ritz, P. Energy requirements in frail elderly people: A review of the literature. Clin. Nutr. 2007, 26, 16–24. [Google Scholar] [CrossRef]
- Obisesan, T.O.; Toth, M.J.; Poehlman, E.T. Prediction of resting energy needs in older men with heart failure. Eur. J. Clin. Nutr. 1997, 51, 678–681. [Google Scholar] [CrossRef]
- Vaisman, N.; Silverberg, D.S.; Wexler, D.; Niv, E.; Blum, M.; Keren, G.; Soroka, N.; Iaina, A. Correction of anemia in patients with congestive heart failure increases resting energy expenditure. Clin. Nutr. 2004, 23, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.L.S.; Chung, M.L.; Elia, M.; Hui, E.; Lum, C.M.; Luk, J.K.H.; Jones, M.G.; Woo, J. Total daily energy expenditure in wasted chronic obstructive pulmonary disease patients. Eur. J. Clin. Nutr. 2002, 56, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Leibel, R.L.; Rosenbaum, M.; Hirsch, J. Changes in energy expenditure resulting from altered body weight. N. Engl. J. Med. 1995, 332, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Elia, M.; Ritz, P.; Stubbs, R.J. Total energy expenditure in the elderly. Eur. J. Clin. Nutr. 2000, 54 (Suppl. 3), 92–103. [Google Scholar] [CrossRef]
- Boullata, J.; Williams, J.; Cottrell, F.; Hudson, L.; Compher, C. Accurate determination of energy needs in hospitalized patients. J. Am. Diet. Assoc. 2007, 107, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy, M.; Normand, S.; Pachiaudi, C.; Lacour, J.R.; Laville, M.; Kostka, T. Simultaneous validation of ten physical activity questionnaires in older men: A doubly labeled water study. J. Am. Geriatr. Soc. 2001, 49, 28–35. [Google Scholar] [CrossRef]
- Schoeller, D.A.; Ravussin, E.; Schutz, Y.; Acheson, K.J.; Baertschi, P.; Jéquier, E. Energy expenditure by doubly labeled water: Validation in humans and proposed calculation. Am. J. Physiol. 1986, 250, 823–830. [Google Scholar] [CrossRef]
- Kruizenga, H.M.; Hofsteenge, G.H.; Weijs, P.J.M. Predicting resting energy expenditure in underweight, normal weight, overweight, and obese adult hospital patients. Nutr. Metab. 2016, 13, 85. [Google Scholar] [CrossRef] [Green Version]
- Porter, J.; Nguo, K.; Gibson, S.; Huggins, C.E.; Collins, J.; Kellow, N.J.; Truby, H. Total energy expenditure in adults aged 65 years and over measured using doubly-labelled water: International data availability and opportunities for data sharing. Nutr. J. 2018, 17, 40. [Google Scholar] [CrossRef]
- Bonnefoy, M.; Cornu, C.; Normand, S.; Boutitie, F.; Bugnard, F.; Rahmani, A.; Lacour, J.R.; Laville, M. The effects of exercise and protein-energy supplements on body composition and muscle function in frail elderly individuals: A long-term controlled randomised study. Br. J. Nutr. 2003, 89, 731–739. [Google Scholar] [CrossRef]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Assessing the nutritional status of the elderly: The Mini Nutritional Assessment as part of the geriatric evaluation. Nutr. Rev. 1996, 54, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.-L. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Racette, S.B.; Schoeller, D.A.; Luke, A.H.; Shay, K.; Hnilicka, J.; Kushner, R.F. Relative dilution spaces of 2H- and 18O-labeled water in humans. Am. J. Physiol. 1994, 267, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Arock, M.; Desnault, H.; Viars, P.; Guillosson, J.J. Determination of total nitrogen in biological milieux by chemoluminescence: A comparison with the reference method. Ann. Biol. Clin. 1985, 43, 872–874. [Google Scholar]
- Ferrannini, E. The theoretical bases of indirect calorimetry: A review. Metab. Clin. Exp. 1988, 37, 287–301. [Google Scholar] [CrossRef]
- Harris, J.A.; Benedict, F.G. A Biometric Study of Basal Metabolism in Man; Carnegie Institution of Washington: Washington, DC, USA, 1919. [Google Scholar]
- Seale, J.L.; Conway, J.M.; Canary, J.J. Seven-day validation of doubly labeled water method using indirect room calorimetry. J. Appl. Physiol. 1993, 74, 402–409. [Google Scholar] [CrossRef]
- Weir, J.B.D.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef]
- Roberts, S.B.; Dallal, G.E. Energy requirements and aging. Public Health Nutr. 2005, 8, 1028–1036. [Google Scholar] [CrossRef] [Green Version]
- Geisler, C.; Braun, W.; Pourhassan, M.; Schweitzer, L.; Glüer, C.-C.; Bosy-Westphal, A.; Müller, M.J. Age-Dependent Changes in Resting Energy Expenditure (REE): Insights from Detailed Body Composition Analysis in Normal and Overweight Healthy Caucasians. Nutrients 2016, 8, 322. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.A.; Manini, T.M.; Paton, C.M.; Yamada, Y.; Everhart, J.E.; Cummings, S.; Mackey, D.C.; Newman, A.B.; Glynn, N.W.; Tylavsky, F.; et al. Longitudinal change in energy expenditure and effects on energy requirements of the elderly. Nutr. J. 2013, 12, 73. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, D.; Belmonte, D.; Deurenberg, P.; Wang, Z.; Krasnow, N.; Pi-Sunyer, F.X.; Heymsfield, S.B. Organ-tissue mass measurement allows modeling of REE and metabolically active tissue mass. Am. J. Physiol. 1998, 275, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition-A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruder, N.; Raynal, M.; Pellissier, D.; Courtinat, C.; François, G. Influence of body temperature, with or without sedation, on energy expenditure in severe head-injured patients. Crit. Care Med. 1998, 26, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Ratheiser, K.M.; Brillon, D.J.; Campbell, R.G.; Matthews, D.E. Epinephrine produces a prolonged elevation in metabolic rate in humans. Am. J. Clin. Nutr. 1998, 68, 1046–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrack, J.A.; Knuth, N.D.; Simonsick, E.M.; Ferrucci, L. “IDEAL” aging is associated with lower resting metabolic rate: The Baltimore Longitudinal Study of Aging. J. Am. Geriatr. Soc. 2014, 62, 667–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purcell, S.A.; Wallengren, O.; Baracos, V.E.; Lundholm, K.; Iresjö, B.-M.; Chu, Q.S.C.; Ghosh, S.S.; Prado, C.M. Determinants of change in resting energy expenditure in patients with stage III/IV colorectal cancer. Clin. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Utaka, S.; Avesani, C.M.; Draibe, S.A.; Kamimura, M.A.; Andreoni, S.; Cuppari, L. Inflammation is associated with increased energy expenditure in patients with chronic kidney disease. Am. J. Clin. Nutr. 2005, 82, 801–805. [Google Scholar] [CrossRef]
- Alix, E.; Berrut, G.; Boré, M.; Bouthier-Quintard, F.; Buia, J.M.; Chlala, A.; Cledat, Y.; d’Orsay, G.; Lavigne, C.; Levasseur, R.; et al. Energy requirements in hospitalized elderly people. J. Am. Geriatr. Soc. 2007, 55, 1085–1089. [Google Scholar] [CrossRef]
- Gardner, A.W.; Womack, C.J.; Sieminski, D.J.; Montgomery, P.S.; Killewich, L.A.; Fonong, T. Relationship between free-living daily physical activity and ambulatory measures in older claudicants. Angiology 1998, 49, 327–337. [Google Scholar] [CrossRef]
- Jallut, D.; Tappy, L.; Kohut, M.; Bloesch, D.; Munger, R.; Schutz, Y.; Chiolero, R.; Felber, J.P.; Livio, J.J.; Jéquier, E. Energy balance in elderly patients after surgery for a femoral neck fracture. JPEN J. Parenter. Enter. Nutr. 1990, 14, 563–568. [Google Scholar] [CrossRef]
- Sergi, G.; Coin, A.; Bussolotto, M.; Benincà, P.; Tomasi, G.; Pisent, C.; Peruzza, S.; Inelmen, E.M.; Enzi, G. Influence of fat-free mass and functional status on resting energy expenditure in underweight elders. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, J.M. Energy expenditure in hospitalized patients: Implications for nutritional support. Mayo Clin. Proc. 2006, 81, 809–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, C.O.; Cappola, A.R.; Varadhan, R.; Fried, L.P. Resting metabolic rate in old-old women with and without frailty: Variability and estimation of energy requirements. J. Am. Geriatr. Soc. 2012, 60, 1695–1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbri, E.; An, Y.; Schrack, J.A.; Gonzalez-Freire, M.; Zoli, M.; Simonsick, E.M.; Guralnik, J.M.; Boyd, C.M.; Studenski, S.A.; Ferrucci, L. Energy Metabolism and the Burden of Multimorbidity in Older Adults: Results From the Baltimore Longitudinal Study of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1297–1303. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Welsh, D.A.; Ravussin, E.; Welsch, M.A.; Cherry, K.E.; Myers, L.; Jazwinski, S.M. An elevation of resting metabolic rate with declining health in nonagenarians may be associated with decreased muscle mass and function in women and men, respectively. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 650–656. [Google Scholar] [CrossRef] [Green Version]
- Lammes, E.; Akner, G. Repeated assessment of energy and nutrient intake in 52 nursing home residents. J. Nutr. Health Aging 2006, 10, 222–230. [Google Scholar]
- Hall, K.S.; Morey, M.C.; Dutta, C.; Manini, T.M.; Weltman, A.L.; Nelson, M.E.; Morgan, A.L.; Senior, J.G.; Seyffarth, C.; Buchner, D.M. Activity-related energy expenditure in older adults: A call for more research. Med. Sci. Sports Exerc. 2014, 46, 2335–2340. [Google Scholar] [CrossRef] [Green Version]
- Rothenberg, E.M.; Bosaeus, I.G.; Westerterp, K.R.; Steen, B.C. Resting energy expenditure, activity energy expenditure and total energy expenditure at age 91–96 years. Br. J. Nutr. 2000, 84, 319–324. [Google Scholar] [CrossRef] [Green Version]
- Valiani, V.; Sourdet, S.; Schoeller, D.A.; Mackey, D.C.; Bauer, D.C.; Glynn, N.W.; Yamada, Y.; Harris, T.B.; Manini, T.M. Health, Aging and Body Composition Study Surveying predictors of late-life longitudinal change in daily activity energy expenditure. PLoS ONE 2017, 12, e0186289. [Google Scholar] [CrossRef] [Green Version]
- Manini, T.M.; Everhart, J.E.; Patel, K.V.; Schoeller, D.A.; Colbert, L.H.; Visser, M.; Tylavsky, F.; Bauer, D.C.; Goodpaster, B.H.; Harris, T.B. Daily activity energy expenditure and mortality among older adults. JAMA 2006, 296, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Purcell, S.A.; Elliott, S.A.; Walter, P.J.; Preston, T.; Cai, H.; Skipworth, R.J.E.; Sawyer, M.B.; Prado, C.M. Total energy expenditure in patients with colorectal cancer: Associations with body composition, physical activity, and energy recommendations. Am. J. Clin. Nutr. 2019, 110, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academies Press: Washington, DC, USA, 2005; ISBN 978-0-309-08525-0. [Google Scholar]
- Blanc, S.; Schoeller, D.A.; Bauer, D.; Danielson, M.E.; Tylavsky, F.; Simonsick, E.M.; Harris, T.B.; Kritchevsky, S.B.; Everhart, J.E. Energy requirements in the eighth decade of life. Am. J. Clin. Nutr. 2004, 79, 303–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SACN Dietary References Values for Energy. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/339317/SACN_Dietary_Reference_Values_for_Energy.pdf 2011 (accessed on 30 November 2019).
- Soysal, P.; Ates Bulut, E.; Yavuz, I.; Isik, A.T. Decreased Basal Metabolic Rate Can Be an Objective Marker for Sarcopenia and Frailty in Older Males. J. Am. Med. Dir. Assoc. 2019, 20, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Ceolin Alves, A.L.; Zuconi, C.P.; Correia, M.I. Energy Expenditure in Patients With Esophageal, Gastric, and Colorectal Cancer. JPEN J. Parenter. Enter. Nutr. 2016, 40, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Zhu, Y.; Kadel, D.; Pang, L.; Chen, G.; Chen, Z. The prognostic influence of body mass index, resting energy expenditure and fasting blood glucose on postoperative patients with esophageal cancer. BMC Gastroenterol. 2016, 16, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | All | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | n | Mean | SD | |
| Age (years) | 19 | 83.6 | 5.1 | 55 | 83.1 | 5.6 | 74 | 83.2 | 5.4 |
| Weight (kg) | 19 | 63.1 | 13.2 | 55 | 64.0 | 11.6 | 74 | 63.8 | 12.0 |
| BMI (kg/m²) | 19 | 24.1 | 3.7 | 55 | 27.0 | 4.3 | 74 | 26.3 | 4.4 |
| Fat-free mass (kg) | 19 | 39.0 | 7.7 | 55 | 37.9 | 6.2 | 74 | 38.1 | 6.6 |
| Fat-free mass (%) | 19 | 62.3 | 7.2 | 55 | 59.8 | 6.9 | 74 | 60.4 | 7.0 |
| Fat mass (kg) | 19 | 24.2 | 8.0 | 55 | 26.2 | 7.9 | 74 | 25.6 | 7.9 |
| Fat mass (%) | 19 | 37.7 | 7.2 | 55 | 40.2 | 6.9 | 74 | 39.6 | 7.0 |
| Albumin (g/L) | 16 | 29.0 | 5.0 | 51 | 40.9 | 2.4 | 67 | 38.0 | 6.0 |
| Prealbumin (g/L) | 19 | 0.2 | 0.1 | 50 | 0.3 | 0.0 | 69 | 0.2 | 0.1 |
| Baseline CRP (mg/L) | 19 | 61.6 | 32.3 | 55 | 0.5 | 0.0 | 74 | 16.2 | 31.3 |
| CRP at day 14 (mg/L) | 19 | 22.4 | 27.9 | - | - | - | 19 | 22.4 | 27.9 |
| Group A | Group B | All | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | n | Mean | SD | ||
| Age (years) | All | 19 | 83.6 | 5.1 | 55 | 83.1 | 5.6 | 74 | 83.2 | 5.4 |
| Women | 13 | 83.3 | 4.9 | 49 | 83.5 | 5.5 | 62 | 83.5 | 5.3 | |
| Men | 6 | 84.2 | 5.8 | 6 | 79.8 | 6.0 | 12 | 82.0 | 6.1 | |
| Weight (kg) | All | 19 | 63.1 | 13.2 | 55 | 64.0 | 11.6 | 74 | 63.8 | 12.0 |
| Women | 13 | 57.1 | 8.2 | 49 | 62.9 | 10.9 | 62 | 61.7 | 10.6 | |
| Men | 6 | 76.1 | 13.0 | 6 | 72.8 | 14.8 | 12 | 74.4 | 13.4 | |
| BMI (kg/m²) | All | 19 | 24.1 | 3.7 | 55 | 27.0 | 4.3 | 74 | 26.3 | 4.4 |
| Women | 13 | 23.3 | 3.6 | 49 | 27.1 | 4.3 | 62 | 26.3 | 4.4 | |
| Men | 6 | 26.0 | 3.6 | 6 | 26.6 | 5.3 | 12 | 26.3 | 4.3 | |
| Fat-free mass (kg) | All | 19 | 39.0 | 7.7 | 55 | 37.9 | 6.2 | 74 | 38.1 | 6.6 |
| Women | 13 | 34.7 | 3.3 | 49 | 36.5 | 4.2 | 62 | 36.1 | 4.1 | |
| Men | 6 | 48.2 | 6.1 | 6 | 49.1 | 8.6 | 12 | 48.7 | 7.2 | |
| Fat-free mass (%) | All | 19 | 62.3 | 7.2 | 55 | 59.8 | 6.9 | 74 | 60.4 | 7.0 |
| Women | 13 | 61.4 | 6.9 | 49 | 58.8 | 6.4 | 62 | 59.3 | 6.5 | |
| Men | 6 | 64.2 | 8.0 | 6 | 68.0 | 5.1 | 12 | 66.1 | 6.7 | |
| Fat mass (kg) | All | 19 | 24.2 | 8.0 | 55 | 26.2 | 7.9 | 74 | 25.6 | 7.9 |
| Women | 13 | 22.4 | 7.1 | 49 | 26.5 | 7.9 | 62 | 25.6 | 7.8 | |
| Men | 6 | 27.9 | 9.2 | 6 | 23.6 | 7.9 | 12 | 25.8 | 8.5 | |
| Fat mass (%) | All | 19 | 37.7 | 7.2 | 55 | 40.2 | 6.9 | 74 | 39.6 | 7.0 |
| Women | 13 | 38.6 | 6.9 | 49 | 41.2 | 6.4 | 62 | 40.7 | 6.5 | |
| Men | 6 | 35.8 | 8.0 | 6 | 32.0 | 5.1 | 12 | 33.9 | 6.7 | |
| Group A | Group B | All | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | n | Mean | SD | n | Mean | SD | |
| Energy intake (kcal/d) 1 | 19 | 1420 | 280 | 0 | 19 | 1420 | 280 | ||
| REE (kcal/day) | 19 | 1184 | 215 | 55 | 1125 | 193 | 74 | 1140 | 199 |
| REE (kcal/kg FMM/d) | 19 | 31 | 4 | 55 | 29 | 3 | 74 | 30 | 3 |
| TEE (kcal/d) | 19 | 1497 | 209 | 0 | 19 | 1497 | 209 | ||
| Physical Activity Level 2 | 19 | 1.3 | 0.2 | 0 | 19 | 1.3 | 0.2 | ||
| Covariates | Regression Coefficient (95% CI) | p-Value |
|---|---|---|
| Fat-free mass (per 5 kg increment) | 103.74 (69.37; 138.10) | <0.001 |
| C-reactive protein (per 20 unit increment) | 20.23 (−2.93; 43.38) | 0.086 |
| Age (per five-year increment) | −30.50 (−57.99; −3.00) | 0.030 |
| Sex (women vs. men) | 16.60 (−100.79; 133.99) | 0.779 |
| Resting energy expenditure (men vs. women) | 1108.04 (995.42; 1220.67) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonnefoy, M.; Gilbert, T.; Normand, S.; Jauffret, M.; Roy, P.; Morio, B.; Cornu, C.; Roche, S.; Laville, M. Energy Expenditure in Older People Hospitalized for an Acute Episode. Nutrients 2019, 11, 2946. https://doi.org/10.3390/nu11122946
Bonnefoy M, Gilbert T, Normand S, Jauffret M, Roy P, Morio B, Cornu C, Roche S, Laville M. Energy Expenditure in Older People Hospitalized for an Acute Episode. Nutrients. 2019; 11(12):2946. https://doi.org/10.3390/nu11122946
Chicago/Turabian StyleBonnefoy, Marc, Thomas Gilbert, Sylvie Normand, Marc Jauffret, Pascal Roy, Béatrice Morio, Catherine Cornu, Sylvain Roche, and Martine Laville. 2019. "Energy Expenditure in Older People Hospitalized for an Acute Episode" Nutrients 11, no. 12: 2946. https://doi.org/10.3390/nu11122946
APA StyleBonnefoy, M., Gilbert, T., Normand, S., Jauffret, M., Roy, P., Morio, B., Cornu, C., Roche, S., & Laville, M. (2019). Energy Expenditure in Older People Hospitalized for an Acute Episode. Nutrients, 11(12), 2946. https://doi.org/10.3390/nu11122946