Comparison of Clinical Outcomes in Surgical Patients Subjected to CIPA Nutrition Screening and Treatment versus Standard Care

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
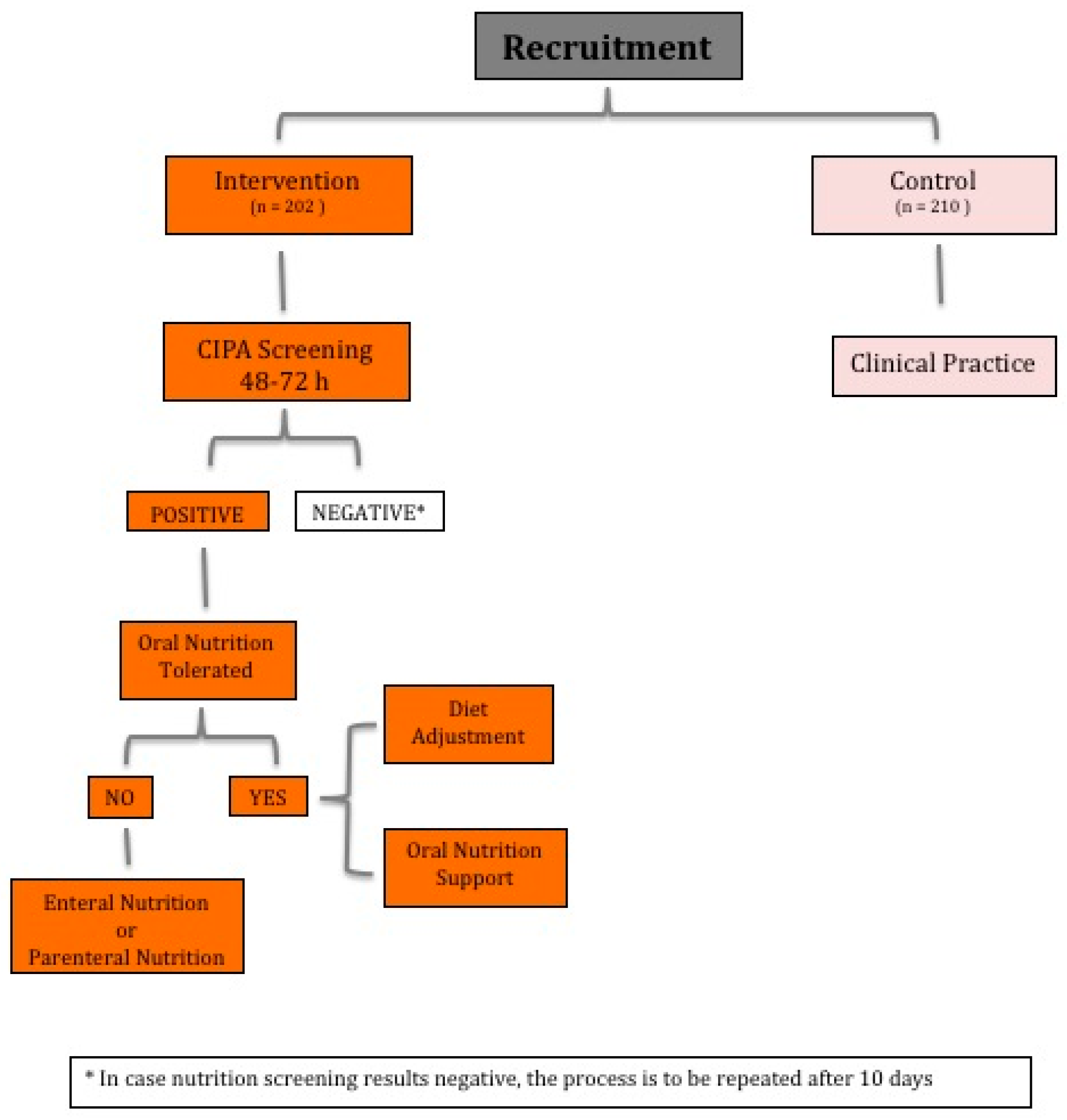
2.2. Trial Design
2.3. Interventions
2.4. Clinical Outcomes
2.5. Statistical Analysis
3. Results
3.1. Nutrition Treatment
3.2. Mean Length of Stay
3.3. Other Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; Waitzberg, D.L.; Bischoff, S.C.; Singer, P. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef]
- Sandrucci, S.; Beets, G.; Braga, M.; Dejong, K.; Demartines, N. Perioperative nutrition and enhanced recovery after surgery in gastrointestinal cancer patients. A position paper by the ESSO task force in collaboration with the ERAS society (ERAS coalition). Eur. J. Surg. Oncol. 2018, 44, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Corish, C.A.; Kennedy, N.P. Review article Protein ± energy undernutrition in hospital in-patients. Br. J. Nutr. 2000, 83, 575. [Google Scholar] [CrossRef] [PubMed]
- Pikul, J.; Sharpe, M.; Lowndes, R.; Ghent, C. Degree of preoperative malnutrition is predictive of postoperative morbidity and mortality in liver transplant recipients. Transplantation 1994, 57, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Neeman, E.; Sharon, E.; Ben-Eliyahu, S. Exploiting the critical perioperative period to improve long-term cancer outcomes. Nat. Rev. Clin. Oncol. 2015, 12, 213–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ljungqvist, O. ERAS—enhanced recovery after surgery: Moving evidence-based perioperative care to practice. J. Parenter. Enter. Nutr. 2014, 38, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Reginster, J.-Y.; Cabrerizo, S.; Bruyère, O.; Kanis, J.; Martinez, J.; Zulet, M. Nutritional status and nutritional treatment are related to outcomes and mortality in older adults with hip fracture. Nutrients 2018, 10, 555. [Google Scholar] [CrossRef]
- Elia, M.; Normand, C.; Norman, K.; Laviano, A. A systematic review of the cost and cost effectiveness of using standard oral nutritional supplements in the hospital setting. Clin. Nutr. 2016, 35, 370–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philipson, T.J.; Snider, J.T.; Lakdawalla, D.N.; Stryckman, B.; Goldman, D.P. Impact of oral nutritional supplementation on hospital outcomes. Am. J. Manag. Care 2013, 19, 121–128. [Google Scholar] [CrossRef]
- Sanz París, A.; García, J.M.; Gómez-Candela, C.; Burgos, R.; Martín, Á.; Matía, P. Malnutrition prevalence in hospitalized elderly diabetic patients. Nutr. Hosp. 2013, 28, 592–599. [Google Scholar] [CrossRef]
- Deutz, N.E.; Matheson, E.M.; Matarese, L.E.; Luo, M.; Baggs, G.E.; Nelson, J.L.; Hegazi, R.A.; Tappenden, K.A.; Ziegler, T.R. Readmission and mortality in malnourished, older, hospitalized adults treated with a specialized oral nutritional supplement: A randomized clinical trial. Clin. Nutr. 2016, 35, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Beattie, A.H.; Prach, A.T.; Baxter, J.P.; Pennington, C.R. A randomised controlled trial evaluating the use of enteral nutritional supplements postoperatively in malnourished surgical patients. Gut 2000, 46, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscaritoli, M.; Krznarić, Z.; Singer, P.; Barazzoni, R.; Cederholm, T.; Golay, A.; Van Gossum, A.; Kennedy, N.; Kreymann, G.; Laviano, A.; et al. Effectiveness and efficacy of nutritional therapy: A systematic review following Cochrane methodology. Clin. Nutr. 2017, 36, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Van Bokhorst-de van der Schueren, M.A.E.; Guaitoli, P.R.; Jansma, E.P.; de Vet, H.C.W. Nutrition screening tools: Does one size fit all? A systematic review of screening tools for the hospital setting. Clin. Nutr. 2014, 33, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Schindler, K.; Pernicka, E.; Laviano, A.; Howard, P.; Schütz, T.; Bauer, P.; Grecu, I.; Jonkers, C.; Kondrup, J.; Ljungqvist, O.; et al. How nutritional risk is assessed and managed in European hospitals: A survey of 21,007 patients findings from the 2007–2008 cross-sectional nutritionDay survey. Clin. Nutr. 2010, 29, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Mora-Mendoza, A.; Suárez-Llanos, J.P.; Delgado-Brito, I.; Pereyra-García-Castro, F.; López-Travieso, R.; Perez-Delgado, N.; Garcia-Núñez, M.; Benitez-Brito, N.; Palacio-Abizanda, E. Optimisation of nutritional screening tool CIPA: Are two parameters of protein really necessary? Nutr. Hosp. 2018, 35, 914–919. [Google Scholar] [CrossRef]
- Suarez-Llanos, J.P.; Benitez-Brito, N.; Oliva-García, J.G.; Pereyra-García-Castro, F.; López-Frías, M.A.; García-Hernández, A.; Díaz-Sirgo, B.; Llorente-Gómez-de Segura, I. Introducing a mixed nutritional screening tool (CIPA) in a tertiary hospital. Nutr. Hosp. 2014, 29, 1149–1153. [Google Scholar] [CrossRef]
- Suárez-Llanos, J.P.; Mora-Mendoza, A.; Benítez-Brito, N.; Pérez-Méndez, L.; Pereyra-García-Castro, F.; Oliva-García, J.G.; Palacio-Abizanda, J.E. Validity of the new nutrition screening tool Control of Food Intake, Protein, and Anthropometry (CIPA) in nonsurgical inpatients. Arch. Med. Sci. 2018, 14, 1020–1024. [Google Scholar] [CrossRef] [PubMed]
- Benitez Brito, N.; Suárez Llanos, J.P.; Fuentes Ferrer, M.; Oliva Garcia, J.G.; Delgado Brito, I.; Pereyra-García Castro, F.; Caracena Castellanos, N.; Acevedo Rodriguez, C.X.; Palacio Abizanda, E. Relationship between mid-upper arm circumference and body mass index in inpatients. PLoS ONE 2016, 11, 1–10. [Google Scholar] [CrossRef]
- Benitez Brito, N.; Mora Mendoza, A.; Suarez Llanos, J.P.; Delgado Brito, I.; Perez Mendez, L.; Herrera Rodriguez, E.; Oliva Garcia, J.G.; Pereyra García-Castro, F. Concordance in the results of control intake performance of 72 h by different health professionals in a tertiary hospital. Nutr. Hosp. 2015, 32, 2895–2899. [Google Scholar] [CrossRef]
- Suárez-Llanos, J.P.; Benítez-Brito, N.; Vallejo-Torres, L.; Delgado-Brito, I.; Rosat-Rodrigo, A.; Hernández-Carballo, C.; Ramallo-Fariña, Y.; Pereyra-García-Castro, F.; Carlos-Romero, J.; Felipe-Pérez, N.; et al. Clinical and cost-effectiveness analysis of early detection of patients at nutrition risk during their hospital stay through the new screening method CIPA: A study protocol. BMC Health Serv. Res. 2017, 292. [Google Scholar] [CrossRef]
- Suárez-Llanos, J.P.; Vallejo-Torres, L.; García-Bello, M.Á.; Hernández-Carballo, C.; Calderón-ledezma, E.M.; Rosat-Rodrigo, A.; Delgado-Brito, I.; Pereyra-García-Castro, F.; Benitez-Brito, N.; Felipe-Pérez, N.; et al. Cost-effectiveness of the hospital nutrition screening tool CIPA. Arch. Med. Sci. 2018, 1–9. [Google Scholar] [CrossRef]
- Kruizenga, H.M.; Tulder, M.W.; Seidell, J.C.; Thijs, A.; Ader, H.J.; Van Bokhorst-de van der Schueren, M.A. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients (Structured abstract). Am. J. Clin. Nutr. 2005, 82, 1082–1089. [Google Scholar] [CrossRef]
- Trentino, K.M.; Swain, S.G.; Burrows, S.A.; Sprivulis, P.C.; Daly, F.F.S. Measuring the incidence of hospital-acquired complications and their effect on length of stay using CHADx. Med. J. Aust. 2013, 199, 543–547. [Google Scholar] [CrossRef] [PubMed]
- González Madroño, A.; Mancha, A.; Rodríguez, F.J.; De Ulibarri, J.I.; Culebras, J. The use of biochemical and immunological parameters in nutritional screening and assessment. Nutr. Hosp. 2011, 26, 594–601. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C. The systemic inflammation-based Glasgow prognostic score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Torres Torres, B.; Ballesteros-Pomar, M.; García Calvo, S.; Castro Lozano, M.; de la Fuente Salvador, B.; Izaola Jáuregui, O.; López Gómez, J.; Gómez Hoyos, E.; Vaquero Puertas, C.; de Luis Román, D. Clinical and economic implications of disease-related malnutrition in a surgical service. Nutr. Hosp. 2018, 35, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.; Lavinhas, C.; Fernandes, L.; Camilo, M.; Ravasco, P. Nutritional risk and status of surgical patients; the relevance of nutrition training of medical students. Nutr. Hosp. 2012, 27, 1086–1091. [Google Scholar] [CrossRef]
- Shpata, V.; Prendushi, X.; Kreka, M.; Kola, I.; Kurti, F.; Ohri, I. Malnutrition at the Time of Surgery Affects Negatively the Clinical Outcome of Critically Ill Patients with Gastrointestinal Cancer. Med. Arch. 2014, 68, 263. [Google Scholar] [CrossRef]


{kind=link}
| Category | Control Group (n = 210) | CIPA Group (n = 202) | p |
|---|---|---|---|
| Age at admission | 61.4 ± 15.0 | 62.5 ± 14.4 | 0.43 |
| Age ≥ 65 years | 93 (44%) | 95 (47%) | 0.576 |
| Sex female | 88 (42%) | 107 (53%) | 0.025 |
| Urgent admission | 138 (66%) | 103 (51%) | 0.002 |
| Surgical pathology | 0.065 | ||
| Infectious | 89 (42%) | 71 (35%) | 0.132 |
| Neoplastic | 49 (23%) | 70 (35%) | 0.011 |
| Inflammatory | 19 (9%) | 13 (6%) | 0.322 |
| Obstructive | 20 (9%) | 12 (6%) | 0.174 |
| Others | 33 (16%) | 36 (18%) | 0.567 |
| Surgery team | <0.001 | ||
| Colorectal | 69 (33%) | 23 (11%) | <0.0001 |
| Gastroesophageal | 58 (28%) | 76 (38%) | 0.033 |
| Hepatobiliary-pancreatic | 52 (25%) | 81 (40%) | 0.001 |
| Endocrine | 30 (14%) | 22 (11%) | 0.29 |
| Charlson index | 3.0 ± 2.5 | 3.7 ± 2.7 | 0.004 |
| EQ-5D-5L score | 0.7 ± 0.35 | 0.58 ± 0.38 | <0.001 |
| Surgical Group | Control Median (percentiles 25–75) | Intervention Median (percentiles 25–75) |
|---|---|---|
| Colorectal | 6 (5–9) | 8 (5–12) |
| Gastroesophageal | 7 (6–10) | 7 (6–9) |
| Hepatobiliary-pancreatic | 13 (8–20) | 9 (7–14) |
| Endocrine | 6 (4–9) | 7 (6–9) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suárez-Llanos, J.P.; Rosat-Rodrigo, A.; García-Niebla, J.; Vallejo-Torres, L.; Delgado-Brito, I.; García-Bello, M.A.; Pereyra-García-Castro, F.; Barrera-Gómez, M.A. Comparison of Clinical Outcomes in Surgical Patients Subjected to CIPA Nutrition Screening and Treatment versus Standard Care. Nutrients 2019, 11, 889. https://doi.org/10.3390/nu11040889
Suárez-Llanos JP, Rosat-Rodrigo A, García-Niebla J, Vallejo-Torres L, Delgado-Brito I, García-Bello MA, Pereyra-García-Castro F, Barrera-Gómez MA. Comparison of Clinical Outcomes in Surgical Patients Subjected to CIPA Nutrition Screening and Treatment versus Standard Care. Nutrients. 2019; 11(4):889. https://doi.org/10.3390/nu11040889
Chicago/Turabian StyleSuárez-Llanos, José Pablo, Adriá Rosat-Rodrigo, Jennifer García-Niebla, Laura Vallejo-Torres, Irina Delgado-Brito, Miguel A. García-Bello, Francisca Pereyra-García-Castro, and Manuel A. Barrera-Gómez. 2019. "Comparison of Clinical Outcomes in Surgical Patients Subjected to CIPA Nutrition Screening and Treatment versus Standard Care" Nutrients 11, no. 4: 889. https://doi.org/10.3390/nu11040889
APA StyleSuárez-Llanos, J. P., Rosat-Rodrigo, A., García-Niebla, J., Vallejo-Torres, L., Delgado-Brito, I., García-Bello, M. A., Pereyra-García-Castro, F., & Barrera-Gómez, M. A. (2019). Comparison of Clinical Outcomes in Surgical Patients Subjected to CIPA Nutrition Screening and Treatment versus Standard Care. Nutrients, 11(4), 889. https://doi.org/10.3390/nu11040889