Adherence to the Healthy Eating Index-2015 across Generations Is Associated with Birth Outcomes and Weight Status at Age 5 in the Lifeways Cross-Generation Cohort Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethics
2.3. Dietary Intake Assessment
2.4. HEI-2015 Scoring
2.5. Offspring Outcomes Assessment
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Parental HEI Scores and Nutrient Intakes
3.3. Parental HEI Scores and Offspring Outcomes
3.4. Grandparental HEI Scores and Offspring Outcomes
3.5. Associations between Parental HEI Scores and Grandparental HEI Scores
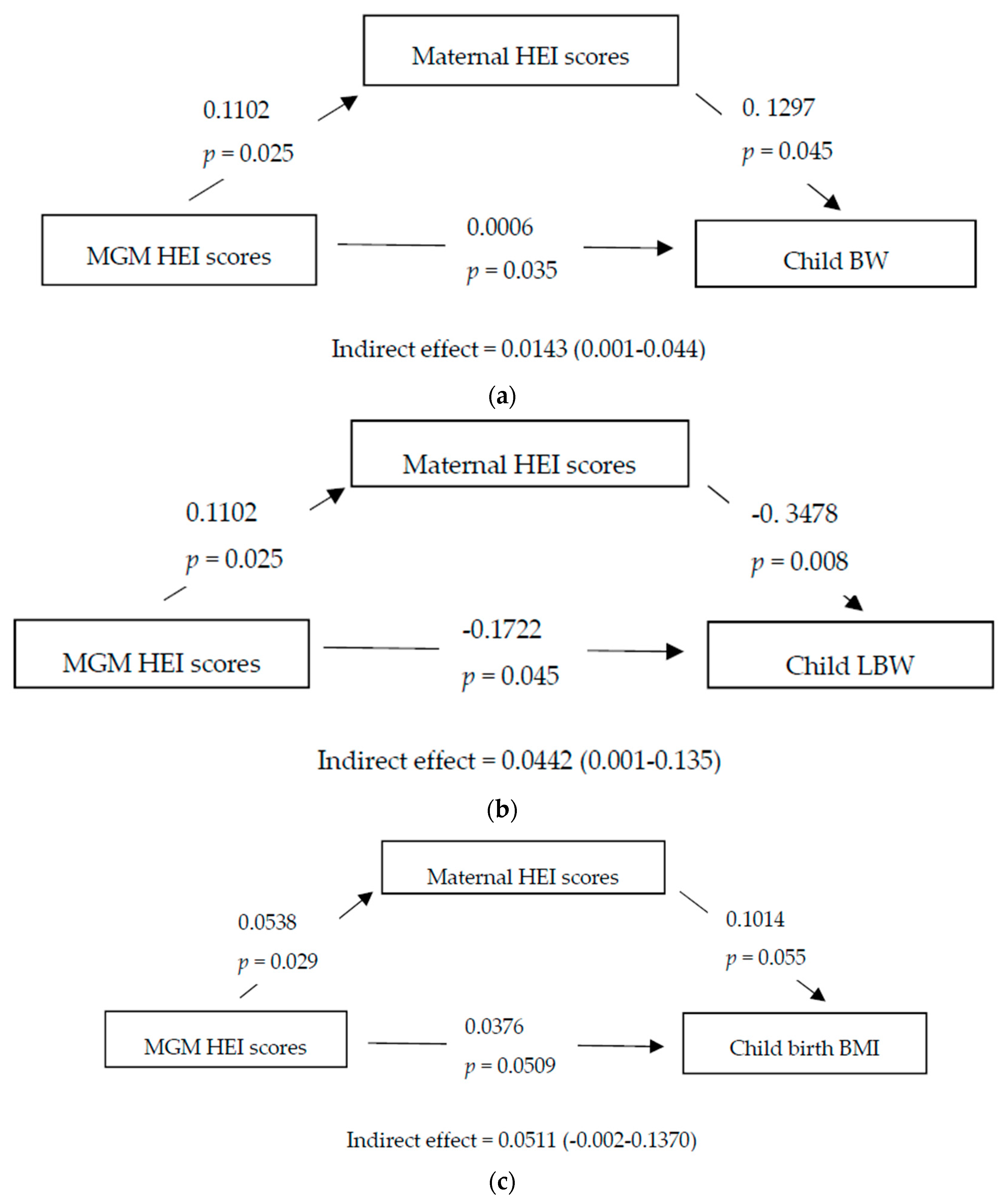
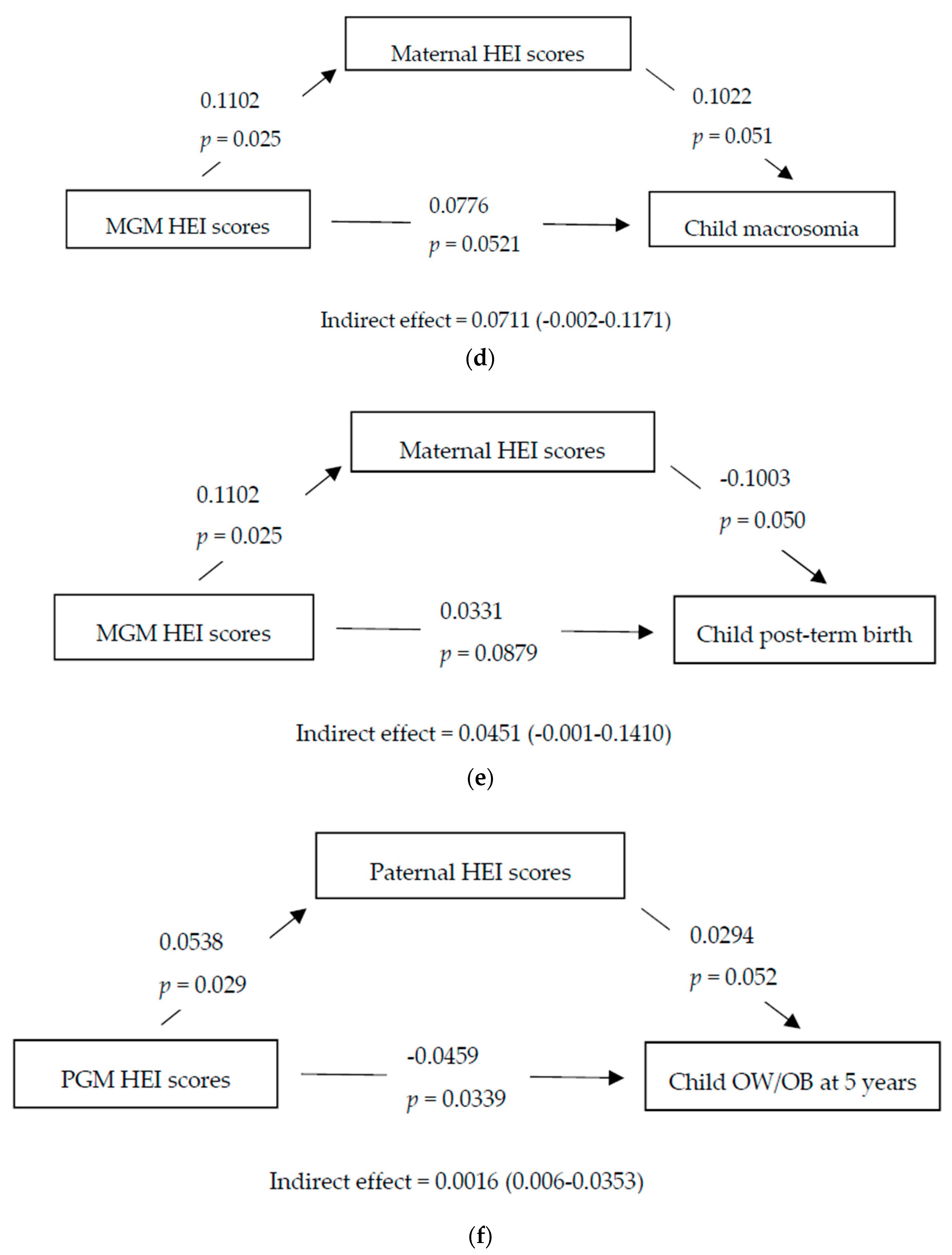
3.6. Mediation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blumfield, M. Update on the role of maternal diet in pregnancy and the programming of infant body composition. Nutr. Bull. 2015, 40, 286–290. [Google Scholar] [CrossRef]
- Abu-Saad, K.; Fraser, D. Maternal nutrition and birth outcomes. Epidemiol. Rev. 2010, 32, 5–25. [Google Scholar] [CrossRef]
- Barker, D.J. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mochizuki, K.; Hariya, N.; Honma, K.; Goda, T. Relationship between epigenetic regulation, dietary habits, and the developmental origins of health and disease theory. Congenit. Anom. 2017, 57, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Murrin, C.; Sweeney, M.R.; Heavey, P.; Kelleher, C.C. Familial intergenerational and maternal aggregation patterns in nutrient intakes in the Lifeways Cross Generation Cohort Study. Public Health Nutr. 2013, 16, 1476–1486. [Google Scholar] [CrossRef] [PubMed]
- Waterland, R.A.; Travisano, M.; Tahiliani, K.G.; Rached, M.T.; Mirza, S. Methyl donor supplementation prevents transgenerational amplification of obesity. Int. J. Obes. 2008, 32, 1373–1379. [Google Scholar] [CrossRef] [Green Version]
- Pembrey, M.; Saffery, R.; Bygren, L.O. Human transgenerational responses to early-life experience: potential impact on development, health and biomedical research. J. Med. Genet. 2014, 51, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Maslova, E.; Rytter, D.; Bech, B.H.; Henriksen, T.B.; Rasmussen, M.A.; Olsen, S.F.; Halldorsson, T.I. Maternal protein intake during pregnancy and offspring overweight 20 y later. Am. J. Clin. Nutr. 2014, 100, 1139–1148. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.-W.; Aris, I.M.; Bernard, J.Y.; Tint, M.-T.; Colega, M.; Gluckman, P.D.; Tan, K.H.; Shek, L.P.; Chong, Y.-S.; Yap, F.; et al. Associations of maternal macronutrient intake during pregnancy with infant BMI peak characteristics and childhood BMI. Am. J. Clin. Nutr. 2017, 105, 705–713. [Google Scholar] [CrossRef]
- Blumfield, M.L.; Hure, A.J.; MacDonald-Wicks, L.K.; Smith, R.; Simpson, S.J.; Giles, W.B.; Raubenheimer, D.; Collins, C.E. Dietary balance during pregnancy is associated with fetal adiposity and fat distribution. Am. J. Clin. Nutr. 2012, 96, 1032–1041. [Google Scholar] [CrossRef] [Green Version]
- Murrin, C.; Shrivastava, A.; Kelleher, C.C. Lifeways Cross-generation Cohort Study Steering Group. Maternal macronutrient intake during pregnancy and 5 years postpartum and associations with child weight status aged five. Eur. J. Clin. Nutr. 2013, 67, 670–679. [Google Scholar] [CrossRef]
- Maslova, E.; Halldorsson, T.I.; Astrup, A.; Olsen, S.F. Dietary protein-to-carbohydrate ratio and added sugar as determinants of excessive gestational weight gain: A prospective cohort study. BMJ Open 2015, 5, e005839. [Google Scholar] [CrossRef]
- Shapiro, A.L.; Kaar, J.L.; Crume, T.L.; Starling, A.P.; Siega-Riz, A.M.; Ringham, B.M.; Glueck, D.H.; Norris, J.M.; Barbour, L.A.; Friedman, J.E.; et al. Maternal diet quality in pregnancy and neonatal adiposity: The Healthy Start Study. Int. J. Obes. 2016, 40, 1056–1062. [Google Scholar] [CrossRef] [Green Version]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary quality during pregnancy varies by maternal characteristics in Project Viva: A US cohort. J. Am. Diet Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef]
- Poon, A.K.; Yeung, E.; Boghossian, N.; Albert, P.S.; Zhang, C. Maternal dietary patterns during third trimester in association with birthweight characteristics and early infant growth. Scientifica 2013, 2013, 786409. [Google Scholar] [CrossRef]
- Rodríguez-Bernal, C.L.; Rebagliato, M.; Iñiguez, C.; Vioque, J.; Navarrete-Muñoz, E.M.; Murcia, M.; Bolumar, F.; Marco, A.; Ballester, F. Diet quality in early pregnancy and its effects on fetal growth outcomes: the Infancia y Medio Ambiente (Childhood and Environment) Mother and Child Cohort Study in Spain. Am. J. Clin. Nutr. 2010, 91, 1659–1666. [Google Scholar] [CrossRef] [Green Version]
- Saunders, L.; Guldner, L.; Costet, N.; Kadhel, P.; Rouget, F.; Monfort, C.; Thomé, J.P.; Multigner, L.; Cordier, S. Effect of a Mediterranean diet during pregnancy on fetal growth and preterm delivery: results from a French Caribbean mother–child cohort study (TIMOUN). Paediatr. Perinat. Epidemiol. 2014, 28, 235–244. [Google Scholar] [CrossRef]
- Chatzi, L.; Mendez, M.; Garcia, R.; Roumeliotaki, T.; Ibarluzea, J.; Tardon, A.; Amiano, P.; Lertxundi, A.; Iñiguez, C.; Vioque, J.; et al. Mediterranean diet adherence during pregnancy and fetal growth: INMA (Spain) and RHEA (Greece) mother-child cohort studies. Br. J. Nutr. 2012, 107, 135–145. [Google Scholar] [CrossRef]
- Martin, C.L.; Sotres-Alvarez, D.; Siega-Riz, A.M. Maternal Dietary Patterns during the Second Trimester Are Associated with Preterm Birth. J. Nutr. 2015, 145, 1857–1864. [Google Scholar] [CrossRef]
- Overview and Background of the Healthy Eating Index. Available online: https://epi.grants.cancer.gov/hei/ (accessed on 11 February 2018).
- Reedy, J.; Lerman, J.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- Chia, A.R.; Tint, M.T.; Han, C.Y.; Chen, L.-W.; Colega, M.; Aris, I.M.; Chua, M.C.; Tan, K.H.; Yap, F.; Shek, L.P.; et al. Adherence to a healthy eating index for pregnant women is associated with lower neonatal adiposity in a multiethnic Asian cohort: The Growing Up in Singapore Towards healthy Outcomes (GUSTO) Study. Am. J. Clin. Nutr. 2018, 107, 71–79. [Google Scholar] [CrossRef]
- Tsigga, M.; Filis, V.; Hatzopoulou, K.; Kotzamanidis, C.; Grammatikopoulou, M.G. Healthy Eating Index during pregnancy according to pre-gravid and gravid weight status. Public Health Nutr. 2011, 14, 290–296. [Google Scholar] [CrossRef]
- Moran, L.J.; Sui, Z.; Cramp, C.S.; Dodd, J.M. A decrease in diet quality occurs during pregnancy in overweight and obese women which is maintained post-partum. Int. J. Obes. 2013, 37, 704–711. [Google Scholar] [CrossRef]
- Vollmer, R.L.; Adamsons, K.; Gorin, A.; Foster, J.S.; Mobley, A.R. Investigating the Relationship of Body Mass Index, Diet Quality, and Physical Activity Level between Fathers and Their Preschool-Aged Children. J. Acad. Nutr. Diet 2015, 115, 919–926. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Wang, Y. Parent-child dietary intake resemblance in the United States: Evidence from a large representative survey. Soc. Sci. Med. 2009, 68, 2137–2144. [Google Scholar] [CrossRef]
- O’Mahony, D.; Fallon, U.B.; Hannon, F.; Kloeckner, K.; Avalos, G.; Murphy, A.W.; Kelleher, C.C.; Lifeways Cross Generation Cohort Study Steering Group. The Lifeways Cross-Generation Study: design, recruitment and data management considerations. Ir. Med. J. 2007, 100, 3–6. [Google Scholar]
- Kelleher, C.C.; Viljoen, K.; Khalil, H.; Somerville, R.; O’Brien, J.; Shrivastava, A.; Murrin, C.; Lifeways Cross-Generation Cohort Study Steering Group. Longitudinal follow-up of the relationship between dietary intake and growth and development in the Lifeways cross-generation cohort study 2001–2013. Proc. Nutr. Soc. 2014, 73, 118–131. [Google Scholar] [CrossRef]
- Food Standards Agency. Mc Cance and Widdowson’s The Composition of Foods; Royal Society of Chemistry: London, UK, 2002.
- Department of Agriculture. 2015–2020 Dietary Guidelines for Americans 8th Edition. 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines (accessed on 11 February 2019).
- Kirkpatrick, S.I.; Reedy, J.; Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Wilson, M.M.; Lerman, J.L.; Tooze, J.A. Applications of the Healthy Eating Index for Surveillance, Epidemiology, and Intervention Research: Considerations and Caveats. J. Acad. Nutr. Diet. 2018, 118, 1603–1621. [Google Scholar] [CrossRef]
- Araujo Júnior, E.; Peixoto, A.B.; Zamarian, A.C.P.; Elito Júnior, J.; Tonni, G. Macrosomia. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 38, 83–96. [Google Scholar] [CrossRef]
- Galal, M.; Symonds, I.; Murray, H.; Petraglia, F.; Smith, R. Postterm pregnancy. Facts Views Vis. Obgyn 2012, 4, 175–187. [Google Scholar]
- United Nations Children’s Fund and World Health Organization. Low Birthweight: Country, Regional and Global Estimates; Unicef: New York, NY, USA, 2004.
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Fallon, U.B.; Murphy, A.W.; Majawit, E.; O’Riordan, C.; Bury, G.; O’Mahony, D.; Kelleher, C.C.; Lifeways Cross Generation Cohort Study Steering Group. Primary care utilisation rates in pre-school children. Ir. Med. J. 2007, 100, 23–27. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Gesteiro, E.; Rodríguez Bernal, B.; Bastida, S.; Sánchez-Muniz, F.J. Maternal diets with low healthy eating index or Mediterranean diet adherence scores are associated with high cord-blood insulin levels and insulin resistance markers at birth. Eur. J. Clin. Nutr. 2012, 66, 1008–1015. [Google Scholar] [CrossRef]
- Dhana, K.; Haines, J.; Liu, G.; Zhang, C.; Wang, X.; Field, A.E.; Chavarro, J.E.; Sun, Q. Association between maternal adherence to healthy lifestyle practices and risk of obesity in offspring: results from two prospective cohort studies of mother-child pairs in the United States. BMJ 2018, 362. [Google Scholar] [CrossRef]
- Hann, C.S.; Rock, C.; King, I.; Drewnowski, A. Validation of the Healthy Eating Index with use of plasma biomarkers in a clinical sample of women. Am. J. Clin. Nutr. 2001, 74, 479–486. [Google Scholar] [CrossRef]
- Pick, M.E.; Edwards, M.; Moreau, D.; Ryan, E. Assessment of diet quality in pregnant women using the Healthy Eating Index. J. Am. Diet Assoc. 2005, 105, 240–246. [Google Scholar] [CrossRef]
- Chong, M.F.; Chia, A.R.; Colega, M.; Tint, M.T.; Aris, I.M.; Chong, Y.S.; Gluckman, P.; Godfrey, K.M.; Kwek, K.; Saw, S.M.; et al. Maternal protein intake during pregnancy is not associated with offspring birth weight in a multiethnic Asian population. J. Nutr. 2015, 145, 1303–1310. [Google Scholar] [CrossRef]
- Moore, V.M.; Davies, M.J.; Willson, K.J.; Worsley, A.; Robinson, J.S. Dietary composition of pregnant women is related to size of the baby at birth. J. Nutr. 2004, 134, 1820–1826. [Google Scholar] [CrossRef]
- Mikkelsen, T.B.; Østerdal, M.L.; Knudsen, V.K.; Haugen, M.; Meltzer, H.M.; Bakketeig, L.; Olsen, S.F. Association between a Mediterranean-type diet and risk of preterm birth among Danish women: a prospective cohort study. Acta Obstet. Gynecol. Scand. 2008, 87, 325–330. [Google Scholar] [CrossRef]
- Dunford, A.R.; Sangster, J.M. Maternal and paternal periconceptional nutrition as an indicator of offspring metabolic syndrome risk in later life through epigenetic imprinting: A systematic review. Diabetes Metab. Syndr. 2017, 11, S655–S662. [Google Scholar] [CrossRef]
- Slyvka, Y.; Zhang, Y.; Nowak, F.V. Epigenetic effects of paternal diet on offspring: Emphasis on obesity. Endocrine 2015, 48, 36–46. [Google Scholar] [CrossRef]
- Eriksen, K.G.; Radford, E.J.; Silver, M.J.; Fulford, A.J.C.; Wegmüller, R.; Prentice, A.M. Influence of intergenerational in utero parental energy and nutrient restriction on offspring growth in rural Gambia. FASEB J. 2017, 31, 4928–4934. [Google Scholar] [CrossRef] [Green Version]
- Lawlor, D.A.; Leary, S.; Smith, G.D. Theoretical underpinning for the use of intergenerational studies in life course epidemiology. In Family Matters: Designing, Analysing and Understanding Family Based Studies in Life Course Epidemiology; Lawlor, D.A., Mishra, G.D., Eds.; Oxford University Press: Oxford, UK, 2009; pp. 13–38. [Google Scholar] [CrossRef]
- Kobayashi, S.; Asakura, K.; Suga, H.; Sasaki, S. Cohabitational effect of grandparents on dietary intake among young Japanese women and their mothers living together. A multicenter cross-sectional study. Appetite 2015, 91, 287–297. [Google Scholar] [CrossRef]
- Toro-Ramos, T.; Paley, C.; Pi-Sunyer, F.X.; Gallagher, D. Body composition during fetal development and infancy through the age of 5 years. Eur. J. Clin. Nutr. 2015, 69, 1279–1289. [Google Scholar] [CrossRef] [Green Version]
- Crozier, S.R.; Robinson, S.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Women’s dietary patterns change little from before to during pregnancy. J. Nutr. 2009, 139, 1956–1963. [Google Scholar] [CrossRef]
- Fallaize, R.; Livingstone, K.M.; Celis-Morales, C.; Macready, A.L.; San-Cristobal, R.; Navas-Carretero, S.; Marsaux, C.F.M.; O’Donovan, C.B.; Kolossa, S.; Moschonis, G.; et al. Association between Diet-quality scores, adiposity, total cholesterol and markers of nutritional status in European adults: Findings from the Food4Me Study. Nutrients 2018, 10, 49. [Google Scholar] [CrossRef]
- Panizza, C.E.; Shvetsov, Y.B.; Harmon, B.E.; Wilkens, L.R.; Le Marchand, L.; Haiman, C.; Reedy, J.; Boushey, C.J. Testing the predictive validity of the Healthy Eating Index-2015 in the multiethnic cohort: Is the score associated with a reduced risk of all-cause and cause-specific mortality? Nutrients 2018, 10, 452. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Participants | Tertile 1 (Lowest) | Tertile 2 | Tertile 3 (Highest) | p-Value 2 | |
|---|---|---|---|---|---|
| Maternal Characteristics (n = 1082) 3 | |||||
| Maternal HEI score | 52.0 ± 8.6 | 43.4 ± 4.8 | 52.8 ± 1.9 | 62.0 ± 4.1 | |
| Age at mother recruitment (year) | 30.1 ± 5.9 | 28.9 ± 6.0 | 29.7 ± 6.1 | 31.9 ± 5.1 | <0.001 |
| Pre-pregnancy BMI (Kg/m2) | 23.8 ± 4.2 | 24.0 ± 4.3 | 23.9 ± 4.4 | 23.5 ± 3.7 | 0.045 |
| Height (cm) | 163.8 ± 6.4 | 163.5 ± 6.4 | 163.3 ± 6.3 | 164.5 ± 6.4 | 0.03 |
| Education level | |||||
| Below tertiary | 536 (51) | 244 (62) | 176 (52) | 116 (36) | <0.001 |
| Tertiary or above | 522 (49) | 150 (38) | 162 (48) | 210 (64) | |
| Smoking during pregnancy | 264 (25) | 145 (36) | 70 (21) | 49 (15) | <0.001 |
| Alcohol use during pregnancy | 613 (62) | 220 (60) | 189 (61) | 204 (66) | 0.29 |
| Marital status | |||||
| Married/cohabiting | 832 (77) | 289 (71) | 254 (75) | 289 (88) | <0.001 |
| Separated/divorced/single | 241 (23) | 116 (29) | 85 (25) | 40 (12) | |
| Household weekly income | |||||
| <200£ | 134 (14) | 61 (17) | 38 (12) | 35 (12) | 0.002 |
| 200–600£ | 490 (50) | 200 (55) | 146 (48) | 144 (47) | |
| >600£ | 348 (36) | 101 (28) | 121 (40) | 126 (41) | |
| Parity (Non-nulliparous) | 585 (55) | 221 (54) | 185 (55) | 179 (55) | 0.98 |
| Regular activity | 183 (19) | 47 (13) | 58 (19) | 78 (26) | <0.001 |
| Paternal Characteristics (n = 333) 4 | |||||
| Paternal HEI score | 47.7 ± 9.4 | 38.1 ± 4.7 | 48.0 ± 2.5 | 58.7 ± 4.8 | |
| Age at proband child birth (year) | 33.6 ± 5.5 | 32.8 ± 5.8 | 34.0 ± 4.9 | 34.1 ± 5.7 | 0.045 |
| Paternal BMI (Kg/m2) | 26.6 ± 3.9 | 26.3 ± 4.2 | 27.1 ± 4.3 | 26.5 ± 3.4 | 0.53 |
| Height (cm) | 178.2 ± 7.1 | 177.6 ± 7.1 | 177.6 ± 7.1 | 179.4 ± 7.0 | 0.16 |
| Education level | |||||
| Below tertiary | 160 (48) | 72 (60) | 54 (50) | 34 (33) | <0.001 |
| Tertiary or above | 172 (52) | 48 (40) | 55 (50) | 69 (67) | |
| Cigarette smoking | 50 (22) | 20 (27) | 15 (18) | 15 (21) | 0.38 |
| Alcohol intake | 240 (77) | 77 (69) | 82 (79) | 81 (84) | 0.05 |
| Marital status | |||||
| Married/cohabiting | 316 (96) | 113 (94) | 104 (95) | 99 (97) | 0.58 |
| Separated/divorced/single | 15 (4) | 7 (6) | 5 (5) | 3 (3) | |
| Household weekly income | |||||
| <600£ | 155 (49) | 65 (57) | 51 (48) | 39 (39) | 0.02 |
| >600£ | 164 (51) | 48 (43) | 55 (52) | 61 (61) | |
| Regular activity | 134 (42) | 41 (35) | 38 (37) | 55 (54) | 0.01 |
| Maternal HEI Scores Tertiles | Paternal HEI Scores Tertiles | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Tertile 1 (n = 411) | Tertile 2 (n = 340) | Tertile 3 (n = 331) | p Value 2 | Correlation with HEI 3 | Tertile 1 (n = 121) | Tertile 2 (n = 109) | Tertile 3 (n = 103) | p Value 2 | Correlation with HEI 3 | |
| Total energy (Kcal/day) | 2305.9 ± 1084.6 | 2511.2 ± 1094.9 | 2764.2 ± 2119.8 | <0.001 | 0.17 ** | 2361.9 ± 873.4 | 2480.6 ± 1082.9 | 2646.3 ± 837.4 | 0.02 | 0.15 ** |
| Carbohydrate (g/day) | 273.3 ± 134.2 | 318.8 ± 121.1 | 360.0 ± 176.8 | <0.001 | 0.31 ** | 257.4 ± 103.8 | 281.6 ± 122.8 | 321.4 ± 99.3 | <0.001 | 0.28 ** |
| Protein (g/day) | 93.9 ± 51.3 | 105.6 ± 59.2 | 121.4 ± 143.5 | <0.001 | 0.27 ** | 97.0 ± 35.5 | 103.7 ± 34.9 | 112.0 ± 36.2 | 0.002 | 0.20 ** |
| Total fat(g/day) | 99.5 ± 52.3 | 100.9 ± 54.1 | 102.1 ± 110.6 | 0.21 | −0.06 | 106.9 ± 44.3 | 106.1 ± 52.3 | 102.7 ± 45.9 | 0.58 | −0.06 |
| MUFA (g/day) | 32.1 ± 16.9 | 32.4 ± 17.7 | 32.6 ± 35.1 | 0.10 | 0.07 * | 36.3 ± 15.6 | 36.9 ± 19.7 | 34.6 ± 15.6 | 0.36 | −0.07 |
| PUFA (g/day) | 14.4 ± 9.7 | 16.2 ± 8.7 | 18.7 ± 17.1 | <0.001 | 0.20 ** | 12.9 ± 5.6 | 15.3 ± 8.6 | 18.2 ± 13.6 | <0.001 | 0.27 ** |
| SFA (g/day) | 40.4 ± 21.6 | 38.9 ± 21.2 | 36.2 ± 41.5 | <0.001 | −0.19 ** | 44.3 ± 20.1 | 40.6 ± 20.4 | 35.0 ± 14.9 | 0.001 | −0.22 ** |
| Cholesterol (mg/day) | 314.9 ± 188.3 | 326.6 ± 193.2 | 339.9 ± 490.1 | 0.45 | 0.01 | 346.0 ± 159.4 | 324.2 ± 123.8 | 310.3 ± 117.5 | 0.32 | −0.10 |
| Fibre (g/day) | 21.1 ± 8.7 | 26.9 ± 9.7 | 35.4 ± 18.0 | <0.001 | 0.53 ** | 16.7 ± 6.9 | 21.1 ± 8.8 | 29.1 ± 9.9 | <0.001 | 0.57 ** |
| Calcium (mg/day) | 969.9 ± 458.7 | 1077.6 ± 420.1 | 1222.5 ± 673.4 | <0.001 | 0.21 ** | 976.3 ± 399.6 | 1032.7 ± 415.1 | 1114.5 ± 420.7 | 0.04 | 0.13 * |
| Iron (mg/day) | 10.6 ± 5.1 | 13.6 ± 6.7 | 17.1 ± 17.5 | <0.001 | 0.45 ** | 10.3 ± 3.9 | 12.1 ± 4.4 | 15.2 ± 5.2 | <0.001 | 0.45 ** |
| Folate (mg/day) | 298.0 ± 138.9 | 368.4 ± 138.5 | 451.5 ± 248.4 | <0.001 | 0.46 ** | 267.6 ± 91.6 | 307.8 ± 100.7 | 389.4 ± 128.9 | <0.001 | 0.44 ** |
| Phosphorous (mg/day) | 1486.9 ± 633.3 | 1670.7 ± 658.3 | 1971.5 ± 1569.3 | <0.001 | 0.31 ** | 1522.3 ± 473.1 | 1648.7 ± 599.1 | 1832.0 ± 560.6 | <0.001 | 0.25 ** |
| Vitamin C (mg/day) | 125.4 ± 74.0 | 188.0 ± 103.6 | 255.9 ± 136.4 | <0.001 | 0.55 ** | 86.4 ± 51.1 | 103.8 ± 49.5 | 163.9 ± 66.5 | <0.001 | 0.53 ** |
| Vitamin B12 (mg/day) | 4.8 ± 2.8 | 5.5 ± 3.9 | 7.2 ± 8.3 | <0.001 | 0.13 ** | 5.4 ± 2.9 | 5.5 ± 2.4 | 6.0 ± 4.5 | 0.70 | 0.06 |
| Vitamin B6 (mg/day) | 2.7 ± 1.2 | 3.3 ± 1.4 | 3.8 ± 2.8 | <0.001 | 0.38 ** | 2.7 ± 0.9 | 3.0 ± 1.1 | 3.5 ± 1.0 | <0.001 | 0.35 ** |
| Vitamin E (mg/day) | 7.9 ± 4.8 | 9.3 ± 4.1 | 11.3 ± 7.1 | <0.001 | 0.33 ** | 7.2 ± 3.3 | 8.2 ± 3.9 | 10.8 ± 6.1 | <0.001 | 0.35 ** |
| Vitamin D (mg/day) | 3.1 ± 1.9 | 3.8 ± 2.6 | 4.2 ± 4.6 | <0.001 | 0.20 ** | 3.2 ± 1.7 | 3.5 ± 1.9 | 3.8 ± 2.3 | 0.17 | 0.11 |
| Low Birth Weight | Macrosomia | Preterm Birth | Post-Term Birth | Overweight/Obese at 5 Years | Obese at 5 Years | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HEI scores | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable |
| Maternal n(case/total) | ||||||||||||
| 52/1070 | 192/1070 | 54/958 | 45/958 | 191/562 | 50/562 | |||||||
| T2 | 0.62 (0.32, 1.18) | 0.82 (0.37, 1.82) | 1.16 (0.79, 1.70) | 1.15 (0.73, 1.76) | 0.81 (0.42, 1.57) | 0.89 (0.41, 1.87) | 0.60 (0.29, 1.23) | 0.84 (0.45, 1.81) | 0.89 (0.58, 1.36) | 1.21 (0.71, 2.04) | 1.37 (0.65, 2.89) | 1.10 (0.40, 3.42) |
| T3 | 0.38 (0.18, 0.82) * | 0.53 (0.19, 1.02) | 1.30 (0.89, 1.90) | 1.21 (0.54, 1.74) | 0.76 (0.39, 1.49) | 0.67 (0.31, 1.64) | 0.50 (0.23, 0.98) * | 0.73 (0.25, 1.12) | 0.87 (0.57, 1.33) | 0.97 (0.56, 1.62) | 1.58 (0.77, 3.23) | 1.12 (0.65, 2.99) |
| Cont. | 0.61 (0.43, 0.90) * | 0.72 (0.50, 0.99) * | 1.01 (0.99, 1.03) | 1.02 (0.89, 1.14) | 0.98 (0.94, 1.01) | 0.63 (0.51, 1.10) | 0.96 (0.93, 0.99) * | 0.87 (0.80, 0.98) * | 0.99 (0.97, 1.02) | 1.02 (0.99, 1.08) | 1.02 (0.98, 1.05) | 1.01 (0.94, 1.10) |
| Ptrend | 0.01 | 0.04 | 0.36 | 0.45 | 0.15 | 0.23 | 0.03 | 0.04 | 0.83 | 0.66 | 0.28 | 0.31 |
| Paternal n(case/total) | ||||||||||||
| 9/329 | 67/329 | 14/305 | 17/305 | 71/218 | 17/218 | |||||||
| T2 | 1.54 (0.45, 2.51) | 1.64 (0.24, 11.36) | 1.23 (0.62, 2.47) | 1.34 (0.53, 3.35) | 1.73 (1.31, 2.31) * | 1.29 (0.20, 1.94) | 1.11 (0.59, 2.08) | 1.42 (0.93, 2.18) | 1.41 (0.67, 2.82) | 1.51 (0.66, 3.40) | 1.16 (0.84, 2.14) | 1.00 (0.51, 1.39) |
| T3 | 0.66 (0.38, 1.14)) | 0.65 (0.10, 8.14) | 1.41 (0.54, 2.54) | 1.52 (0.58, 3.96) | 1.24 (0.91, 1.68) | 1.61 (0.10, 2.42) | 0.79 (0.40, 1.56) | 0.76 (0.47, 1.22) | 1.22 (0.26, 3.05) | 1.42 (0.60, 3.42) | 0.89 (0.26, 2.77) | 0.74 (0.11, 0.91) * |
| Cont. | 0.92 (0.77, 1.11) | 0.64 (0.33, 1.21) | 1.18 (0.85, 1.65) | 0.98 (0.70, 1.37) | 1.11 (0.96, 1.28) | 1.24 (0.98, 1.52) | 1.11 (0.61, 2.03) | 0.61 (0.48, 1.78) | 1.05 (0.74, 1.50) | 0.93 (0.61, 1.10) | 1.03 (0.42, 1.26) | 0.91 (0.31, 0.96) * |
| Ptrend | 0.92 | 0.49 | 0.31 | 0.47 | 0.14 | 0.08 | 0.72 | 0.50 | 0.76 | 0.10 | 0.14 | 0.04 |
| Low Birth Weight | Macrosomia | Preterm Birth | Post-Term Birth | Overweight/Obese at 5 years | Obese at 5 years | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HEI scores | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable | Unadjusted | Multivariable |
| MGMn (case/total) | 10/281 | 53/281 | 15/259 | 13/259 | 52/177 | 12/177 | ||||||
| T2 | 0.92 (0.12, 1.17) | 0.87 (0.12, 1.64) | 1.18 (0.58, 1.81) | 1.13 (0.73, 1.67) | 0.86 (0.40, 1.84) | 0.90 (0.41, 1.45) | 0.32 (0.14, 2.54) | 0.25 (0.01, 1.81) | 0.65 (0.24, 1.19) | 0.68 (0.29, 1.30) | 0.89 (0.17, 1.85) | 0.90 (0.17, 1.59) |
| T3 | 0.72 (0.23, 0.98) * | 0.95 (0.12, 1.05) | 1.01 (0.70, 1.43) | 0.64 (0.59, 1.16) | 0.59 (0.04, 1.25) | 0.52 (0.21, 1.27) | 0.47 (0.27, 1.22) | 0.87 (0.56, 1.25) | 0.56 (0.22, 1.21) | 0.58 (0.24, 1.24) | 0.81 (0.25, 2.03) | 0.85 (0.27, 2.07) |
| Cont. | 0.97 (0.57, 1.02) | 0.87 (0.61, 0.96) * | 0.97 (0.10, 1.27) | 1.10 (1.01, 1.22) * | 0.75 (0.54, 1.24) | 0.74 (0.53, 1.05) | 0.51 (0.19, 0.98) * | 0.67 (0.14, 1.53) | 0.79 (0.61, 1.20) | 0.82 (0.58, 1.37) | 0.90 (0.60, 1.32) | 0.95 (0.54, 1.40) |
| Ptrend | 0.08 | 0.04 | 0.54 | 0.03 | 0.36 | 0.17 | 0.03 | 0.73 | 0.14 | 0.17 | 0.31 | 0.28 |
| MGFn (case/total) | 5/112 | 20/112 | 4/105 | 3/105 | 23/71 | 2/71 | ||||||
| T2 | 0.94 (0.22, 1.92) | 0.87 (0.15, 1.68) | 0.98 (0.38, 1.16) | 0.85 (0.48, 1.26) | 0.20 (0.10, 1.12) | 0.25 (0.09, 1.31) | 0.84 (0.29, 2.18) | 0.94 (0.10, 2.07) | 1.04 (0.39, 2.74) | 1.10 (0.28, 2.51) | 1.11 (0.31, 2.17) | 1.10 (0.37, 2.69) |
| T3 | 1.10 (0.38, 2.03) | 0.74 (0.25, 1.88) | 1.07 (0.58, 2.04) | 0.98 (0.34, 1.46) | 0.57 (0.16, 1.28) | 0.46 (0.10, 1.08) | 0.79 (0.20, 1.56) | 0.77 (0.23, 1.98) | 0.66 (0.13, 2.33) | 0.77 (0.21, 2.09) | 0.89 (0.26, 2.47) | 0.88 (0.21, 2.15) |
| Cont. | 1.21 (0.70, 2.44) | 0.87 (0.30, 2.13) | 1.03 (0.77, 2.27) | 0.99 (0.65, 2.31) | 0.78 (0.21, 1.22) | 0.65 (0.26, 1.26) | 0.36 (0.14, 1.26) | 0.41 (0.59, 1.88) | 0.82 (0.13, 1.48) | 0.99 (0.18, 1.234) | 0.95 (0.42, 1.65) | 0.96 (0.55, 1.79) |
| Ptrend | 0.83 | 0.68 | 0.25 | 0.41 | 0.30 | 0.46 | 0.34 | 0.39 | 0.19 | 0.29 | 0.88 | 0.58 |
| PGMn(case/total) | 4/161 | 25/161 | 4/147 | 5/147 | 30/97 | 7/97 | ||||||
| T2 | 1.14 (0.23, 2.75) | 1.07 (0.14, 2.71) | 1.01 (0.47, 1.91) | 0.99 (0.36, 2.38) | 1.23 (0.64, 2.25) | 1.02 (0.38, 2.55) | 0.62 (0.17, 1.85) | 0.90 (0.42, 1.87) | 0.48 (0.11, 1.60) | 0.46 (0.15, 1.89) | 1.03 (0.54, 2.62) | 0.99 (0.60, 1.82) |
| T3 | 0.81 (0.33, 1.99) | 0.72 (0.20, 1.90) | 1.07 (0.51, 2.08) | 1.10 (0.54, 1.91) | 1.15 (0.42, 1.85) | 1.13 (0.57, 2.49) | 0.43 (0.27, 1.21) | 0.51 (0.22, 1.38) | 0.65 (0.15, 1.14) | 0.67 (0.32, 1.08) | 0.88 (0.35, 1.76) | 0.79 (0.58, 1.49) |
| Cont. | 0.93 (0.27, 2.01) | 0.92 (0.23, 1.99) | 1.24 (0.40, 2.38) | 1.16 (0.48, 2.27) | 1.06 (0.58, 1.95) | 1.18 (0.80, 2.53) | 0.89 (0.38, 1.53) | 0.75 (0.54, 1.17) | 0.74 (0.14, 0.92) * | 0.84 (0.21, 0.98) * | 0.97 (0.41, 1.32) | 1.00 (0.51, 1.47) |
| Ptrend | 0.11 | 0.15 | 0.68 | 0.51 | 0.24 | 0.33 | 0.63 | 0.24 | 0.02 | 0.04 | 0.28 | 0.42 |
| PGFn(case/total) | 4/98 | 11/98 | 5/86 | 3/86 | 19/58 | 2/58 | ||||||
| T2 | 0.77 (0.24, 1.67) | 0.67 (0.19, 1.54) | 1.14 (0.37, 1.75) | 0.95 (0.17, 1.87) | 0.56 (0.14, 1.55) | 0.51 (0.25, 1.57) | 0.67 (0.31, 1.74) | 0.60 (0.28, 1.82) | 0.79 (0.34, 2.20) | 0.87 (0.52, 2.11) | 0.89 (0.54, 2.11) | 0.79 (0.54, 2.25) |
| T3 | 0.84 (0.34, 1.86) | 0.75 (0.15, 1.97) | 1.08 (0.55, 1.96) | 1.07 (0.64, 1.82) | 0.71 (0.21, 1.81) | 0.62 (0.23, 1.63) | 0.75 (0.15, 2.31) | 0.71 (0.13, 1.79) | 0.98 (0.46, 2.18) | 0.90 (0.35, 2.06) | 0.97 (0.61, 1.97) | 0.82 (0.51, 2.07) |
| Cont. | 0.93 (0.43, 1.64) | 1.10 (0.67, 2.18) | 0.71 (0.47, 1.97) | 0.78 (0.56 1.89) | 0.76 (0.45, 1.89) | 0.67 (0.19, 2.12) | 0.73 (0.25, 2.30) | 0.78 (0.43, 1.95) | 1.23 (0.41, 2.14) | 0.84 (0.22, 2.21) | 1.01 (0.64, 2.86) | 0.96 (0.31, 2.08) |
| Ptrend | 0.32 | 0.27 | 0.49 | 0.31 | 0.41 | 0.19 | 0.19 | 0.21 | 0.48 | 0.61 | 0.79 | 0.64 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro, P.; Mehegan, J.; Murrin, C.M.; Kelleher, C.C.; Phillips, C.M. Adherence to the Healthy Eating Index-2015 across Generations Is Associated with Birth Outcomes and Weight Status at Age 5 in the Lifeways Cross-Generation Cohort Study. Nutrients 2019, 11, 928. https://doi.org/10.3390/nu11040928
Navarro P, Mehegan J, Murrin CM, Kelleher CC, Phillips CM. Adherence to the Healthy Eating Index-2015 across Generations Is Associated with Birth Outcomes and Weight Status at Age 5 in the Lifeways Cross-Generation Cohort Study. Nutrients. 2019; 11(4):928. https://doi.org/10.3390/nu11040928
Chicago/Turabian StyleNavarro, Pilar, John Mehegan, Celine M. Murrin, Cecily C. Kelleher, and Catherine M. Phillips. 2019. "Adherence to the Healthy Eating Index-2015 across Generations Is Associated with Birth Outcomes and Weight Status at Age 5 in the Lifeways Cross-Generation Cohort Study" Nutrients 11, no. 4: 928. https://doi.org/10.3390/nu11040928
APA StyleNavarro, P., Mehegan, J., Murrin, C. M., Kelleher, C. C., & Phillips, C. M. (2019). Adherence to the Healthy Eating Index-2015 across Generations Is Associated with Birth Outcomes and Weight Status at Age 5 in the Lifeways Cross-Generation Cohort Study. Nutrients, 11(4), 928. https://doi.org/10.3390/nu11040928