Exploring the Experiences of People with Obesity Using Portion Control Tools—A Qualitative Study


Abstract
:1. Introduction
2. Materials and Methods
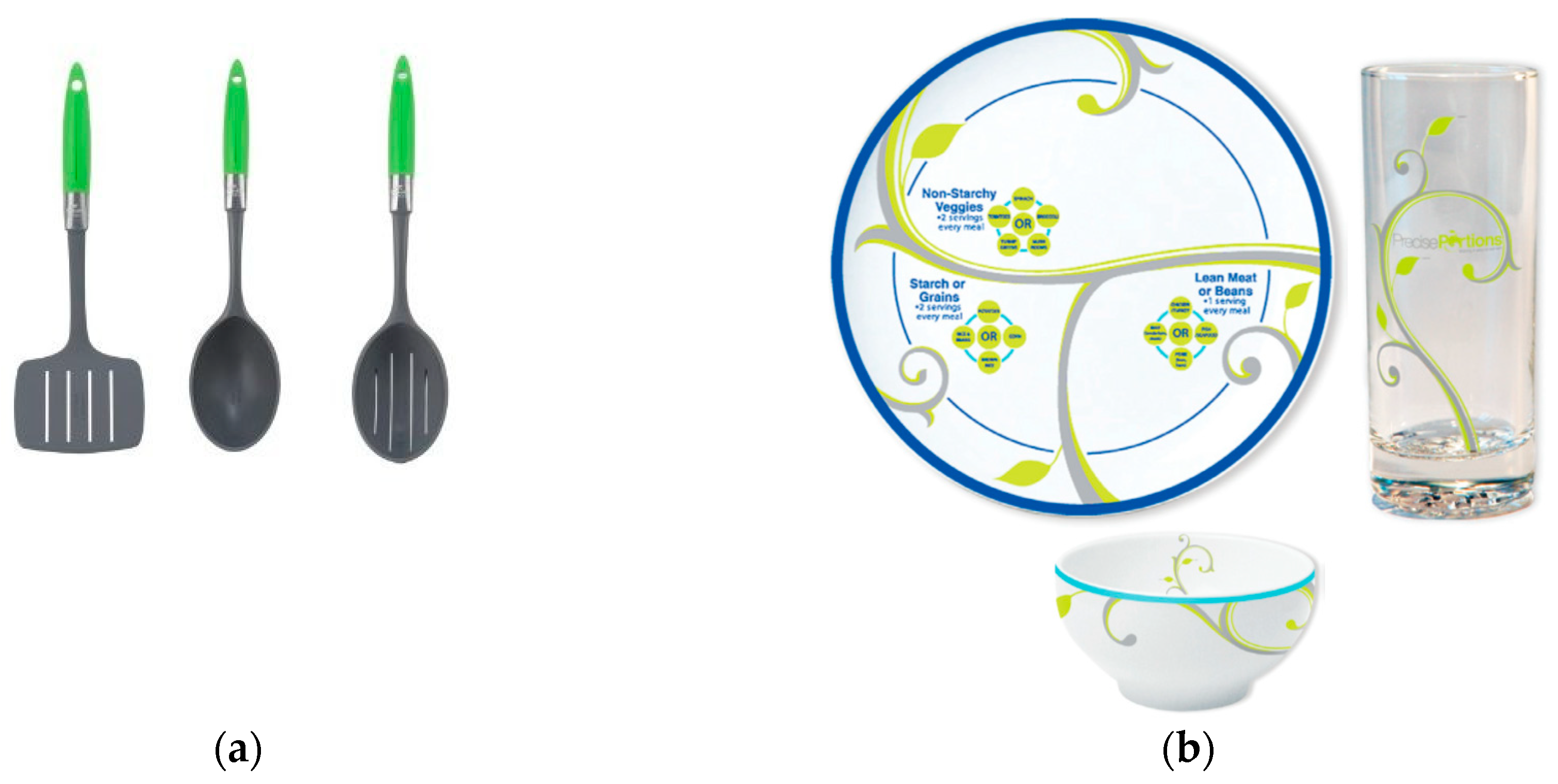
2.1. Portion-Control Tools
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Participants
3.2. Main Themes
3.2.1. Educational
3.2.2. Usability
3.2.3. Acceptability
3.2.4. Feasibility
3.2.5. Overall experience
4. Discussion
4.1. Limitations
4.2. Implications for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Lewis, H.B.; Wei, Y.; Higgins, J.P.; Ogilvie, D. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Database Syst. Rev. 2015, 9, CD011045. [Google Scholar] [CrossRef]
- Zlatevska, N.; Dubelaar, C.; Holden, S.S. Sizing Up the Effect of Portion Size on Consumption: A Meta-Analytic Review. J. Mark. 2014, 78, 140–154. [Google Scholar] [CrossRef]
- Rolls, B.J. What is the role of portion control in weight management? Int. J. Obes. 2014, 38 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavanagh, K.; Vartanian, L.R.; Herman, C.P.; Polivy, J. The effect of portion size on food intake is robust to brief education and mindfulness exercises. J. Health Psychol. 2014, 19, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Spanos, S.; Kenda, A.S.; Vartanian, L.R. Can serving-size labels reduce the portion-size effect? A pilot study. Eat. Behav. 2015, 16, 40–42. [Google Scholar] [CrossRef]
- Benton, D. Porton size: What we know and what we need to know. Crit. Rev. Food Sci. Nutr. 2015, 77, 988–1004. [Google Scholar] [CrossRef]
- Steenhuis, I.H.; Vermeer, W.M. Portion size: Review and framework for interventions. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 58. [Google Scholar] [CrossRef]
- Robinson, E.; Oldham, M.; Cuckson, I.; Brunstrom, J.M.; Rogers, P.J.; Hardman, C.A. Visual exposure to large and small portion sizes and perceptions of portion size normality: Three experimental studies. Appetite 2016, 98, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Marteau, T.M.; Hollands, G.J.; Shemilt, I.; Jebb, S.A. Downsizing: Policy options to reduce portion sizes to help tackle obesity. BMJ 2015, 351, h5863. [Google Scholar] [CrossRef]
- Almiron-Roig, E.; Forde, C.G.; Hollands, G.J.; Vargas, M.A.; Brunstrom, J.M. Portion-size Reduction: A review of evidence supporting current strategies, challenges, and opportunities. Nutr. Rev. 2019, in press. [Google Scholar]
- FSA. Food Standards Agency. The Eatwell Plate. 2010. Available online: http://www.eatwell.gov.uk/healthy/eatwellplate/ (accessed on 1 April 2010).
- Mayo Foundation for Medical Education and Research. Portion Control for Weight Loss. 2015. Available online: http://www.mayoclinic.org/healthy-lifestyle/weight-loss/multimedia/portion-control/sls-20076148 (accessed on 15 May 2019).
- World Cancer Research Fund. What Is a Healthy Portion Size? Cancer Prevention. Together We Can. 2016. Available online: https://www.wcrf-uk.org/sites/default/files/healthy-portions-poster.pdf%0A (accessed on 6 February 2019).
- Anderson, A.S.; Barton, K.; Craigie, A.; Freeman, J.; Gregor, A.; Stead, M.; Tasker, S.; Wrieden, W.L. Exploration of Adult Food Portion Size Tools; NHS Health Scotland: Edinburgh, UK, 2008. [Google Scholar]
- Rolls, B.J.; Roe, L.S.; James, B.L.; Sanchez, C.E. Does the incorporation of portion-control strategies in a behavioral program improve weight loss in a 1-yr randomized controlled trial? Int. J. Obes. 2017, 41, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Lewis, H.B.; Ahern, A.L.; Jebb, S.A. How much should I eat? A comparison of suggested portion sizes in the UK. Public Health Nutr. 2012, 15, 2110–2117. [Google Scholar] [CrossRef] [Green Version]
- RosemaryConley.com. Rosemary Conley Portion Pots. Available online: https://www.rosemaryconley.com/shop/products/portion-pots?taxon_id=24 (accessed on 15 May 2019).
- PrecisePortions. Precise Portions Nutrition Control Systems. 2010. Available online: https://www.preciseportions.com/ (accessed on 15 May 2019).
- Healthy Steps Portion Control Serving Set. 2012. Available online: https://www.jokari.com/collections/healthy-steps-1/products/serving-set (accessed on 15 May 2019).
- Holden, S.S.; Zlatevska, N.; Dubelaar, C. Whether Smaller Plates Reduce Consumption Depends on Who’s Serving and Who’s Looking: A Meta-Analysis. J. Assoc. Consum. Res. 2016, 1, 134–146. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, S.D.; Kang, J.; Kline, G.A. Portion control plate for weight loss in obese patients with type 2 diabetes mellitus: A controlled clinical trial. Arch. Intern. Med. 2007, 167, 1277–1283. [Google Scholar] [CrossRef]
- Almiron-Roig, E.; Domínguez, A.; Vaughan, D.; Solis-Trapala, I.; Jebb, S.A. Acceptability and potential effectiveness of commercial portion control tools amongst people with obesity. Br. J. Nutr. 2016, 116, 1974–1983. [Google Scholar] [CrossRef] [Green Version]
- Raghubir, P.; Krishna, A. Vital Dimensions in Volume Perception: Can the Eye Fool the Stomach? J. Mark. Res. 1999, 36, 313–326. [Google Scholar] [CrossRef]
- Nelson, M.; Atkinson, M.; Darbyshire, S. Food photography I: The perception of food portion size from photographs. Br. J. Nutr. 1994, 72, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Versluis, I.; Papies, E.K.; Marchiori, D. Preventing the pack size effect: Exploring the effectiveness of pictorial and non-pictorial serving size recommendations. Appetite 2015, 87, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Kesman, R.L.; Ebbert, J.O.; Harris, K.I.; Schroeder, D.R. Portion control for the treatment of obesity in the primary care setting. BMC Res. Notes 2011, 4, 346. [Google Scholar] [CrossRef]
- Huber, J.M.; Shapiro, J.S.; Wieland, M.L.; Croghan, I.T.; Douglas, K.S.; Schroeder, D.R.; Hathaway, J.C.; Ebbert, J.O. Telecoaching plus a portion control plate for weight care management: A randomized trial. Trials 2015, 16, 323. [Google Scholar] [CrossRef] [PubMed]
- Department for Communities and Local Government. English Indices of Deprivation 2015; Department for Communities and Local Government: London, UK, 2015. Available online: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2015 (accessed on 3 February 2017).
- Draper, A.; Swift, J.A. Qualitative research in nutrition and dietetics: Data collection issues. J. Hum. Nutr. Diet. 2011, 24, 3–12. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence (NICE). Adams Portion Pot Weight Management System. Shared Learning Database. NICE. 2009. Available online: https://www.nice.org.uk/sharedlearning/adams-portion-pot-weight-management-system (accessed on 15 May 2019).
- KitchenCraft. Colourworks Set of Five Mesuring Spoons. Available online: https://www.kitchencraft.co.uk/categories/baking_sugarcraft/scales_measuring/5_piece_measuring_spoon_set_cwmspoonset.htm (accessed on 15 May 2019).
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, J.; Spencer, L. Qualitative data analysis for applied policy research. In Analyzing Qualitative Data; Bryman, A., Burgess, R., Eds.; Routledge: Abingdon, Oxfordshire, UK, 1994; pp. 173–194. [Google Scholar]
- Pope, C.; Ziebland, S.; Mays, N. Qualitative research in health care. Analysing qualitative data. BMJ 2000, 320, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Wansink, B.; Cheney, M.M. Super Bowls: Serving bowl size and food consumption. J. Am. Med. Assoc. 2005, 293, 1727–1728. [Google Scholar] [CrossRef]
- Marchiori, D.; Corneille, O.; Klein, O. Container size influences snack food intake independently of portion size. Appetite 2012, 58, 814–817. [Google Scholar] [CrossRef] [Green Version]
- Attwood, A.S.; Scott-Samuel, N.E.; Stothart, G.; Munafo, M.R. Glass shape influences consumption rate for alcoholic beverages. PLoS ONE 2012, 7, e43007. [Google Scholar] [CrossRef]
- Wansink, B.; van Ittersum, K.; Painter, J.E. Ice cream illusions bowls, spoons, and self-served portion sizes. Am. J. Prev. Med. 2006, 31, 240–243. [Google Scholar] [CrossRef]
- Rolls, B.J.; Roe, L.S.; Halverson, K.H.; Meengs, J.S. Using a smaller plate did not reduce energy intake at meals. Appetite 2007, 49, 652–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, M.B.E.; Pourshahidi, L.K. Portion Size and Obesity. Adv. Nutr. Am. Int. Rev. J. 2014, 5, 829–834. [Google Scholar] [CrossRef]
- Berg, C.; Forslund, H.B. The Influence of Portion Size and Timing of Meals on Weight Balance and Obesity. Curr. Obes. Rep. 2015, 4, 11–18. [Google Scholar] [CrossRef]
- Lewis, H.B.; Forwood, S.E.; Ahern, A.L.; Verlaers, K.; Robinson, E.; Higgs, S.; Jebb, S.A. Personal and social norms for food portion sizes in lean and obese adults. Int. J. Obes. 2015, 39, 1319–1324. [Google Scholar] [CrossRef] [Green Version]
- Robinson, E.; Thomas, J.; Aveyard, P.; Higgs, S. What everyone else is eating: A systematic review and meta-analysis of the effect of informational eating norms on eating behavior. J. Acad. Nutr. Diet. 2014, 114, 414–429. [Google Scholar] [CrossRef]
- Geier, A.B.; Rozin, P.; Doros, G. Unit bias. A new heuristic that helps explain the effect of portion size on food intake. Psychol. Sci. 2006, 17, 521–525. [Google Scholar] [CrossRef]
- Fay, S.H.; Ferriday, D.; Hinton, E.C.; Shakeshaft, N.G.; Rogers, P.J.; Brunstrom, J.M. What determines real-world meal size? Evidence for pre-meal planning. Appetite 2011, 56, 284–289. [Google Scholar] [CrossRef] [Green Version]
- Robinson, E.; Aveyard, P.; Daley, A.; Jolly, K.; Lewis, A.; Lycett, D.; Higgs, S. Eating attentively: A systematic review and meta-analysis of the effect of food intake memory and awareness on eating. Am. J. Clin. Nutr. 2013, 97, 728–742. [Google Scholar] [CrossRef]
- Brunstrom, J.M.; Collingwood, J.; Rogers, P.J. Perceived volume, expected satiation, and the energy content of self-selected meals. Appetite 2010, 55, 25–29. [Google Scholar] [CrossRef]
- Pilnick, A.; Swift, J.A. Qualitative research in nutrition and dietetics: Assessing quality. J. Hum. Nutr. Diet. 2011, 24, 209–214. [Google Scholar] [CrossRef]
- Britten, N. Qualitative interviews in medical research. BMJ 1995, 311, 251–253. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | |
|---|---|
| Male, % (n) | 37.9 (11) |
| Female, % (n) | 62.1 (18) |
| Age, years (mean ± SD) | 49 ± 13 |
| White ethnic background, % (n) | 96.6 (1) |
| History of mental illness, % (n) | 10.3 (3) |
| BMI at baseline, kg/m2 (mean ± SD) | 40.9 ± 5.8 |
| Weight at baseline, kg (mean ± SD) | 115.9 ± 22.5 |
| Weight at end, kg (mean ± SD) 1 | 114.2 ± 21.5 |
| Following special diet 2, % (n) | 48.3 (14) |
| Previous experience with portion size tools, % (n) | 3.4 (1) |
| Prepares meals for self only, % (n) | 17.2 (5) |
| Prepares meals for self and others, % (n) | 79.3 (23) |
| Over-Arching Themes | Themes | Sub-Themes (n of Participants Forming Sub-Theme) | Example of Response |
|---|---|---|---|
| Educational | Portion guidance on appropriate size Awareness of previously over-sized portions | Learning achieved (developed ability to control portions without tool) (n = 8) Confirmation of previous attempts to control through guesswork (n = 8) Feeling full on fewer calories (n = 2) Achieving portion goal (n = 10) | The spoons helped me to realise how much bigger my original portion size was (ID130, 51 years old, F, 34.4 kg/m2, lost 1.7 kg) The fact that I now know my portions for some foods was too big (ID116, 72 years old, M, 39.2 kg/m2, lost 1 kg) Has been helpful but now using smaller plates for smaller portions (ID109, 55 years old, M, 39.7 kg/m2, lost 4.2 kg) |
| Usability | Ease of use Functionality Versatility | Clarity and simplicity (n = 15) Helpful to measure portions accurately and precisely (n = 3) Remaining hungry (more snacking) (n = 3) Failure to achieve portion goal (n = 3) Easy to cheat with (snacking more, second helpings, piling upwards) (n = 5) Not suitable for certain foods (dry/raw, mixed meals) (n = 4) Not suitable for children, special diets (n = 2) Single person use (need plate for partner) (n = 1) | Hassle-free and easy way to limit portions (ID106, 31 years old, M, 54.4 kg/m2, lost 6.2 kg) You could see on the plate the right amount of foods (ID110, 47 years old, M, 44.9 kg/m2, gained 2.3 kg) That the plate has made me stick to a small portion of meat and potatoes (ID104, 33 years old, F, 30.8 kg/m2, lost 5.8 kg) [Liked aspect] The amount that constitutes a portion (ID140, 24 years old, F, 35.4 kg/m2, lost 2.4 kg) It’s a bit messy to organize the food to sort it out (ID117, 33 years old, M, 42.1 kg/m2, lost 10.5 kg) It didn’t measure ‘mixed food’(ID129, 37 years old, F, 35.9 kg/m2, lost 1.6 kg) |
| Acceptability | Quality Attractiveness of design | Weight (too light, too heavy) (n = 1) Material (too flimsy) (n = 8) Finish (visible glue, chipping easily) Size (too large, too small) (n = 9) Design (clever, easy to find, not blending in) (n = 9) | [Referring to crockery] They look too small (ID122, 39 years old, 34.7 kg/m2, M, lost 1.4 kg) |
| Feasibility | Convenience Appropriateness Adherence | Not convenient for eating on the go, at work Difficult during festivities, for eating with guests, for children (n = 5) Not seen as necessary (n = 3) Forgetting to use (n = 6) | I would of liked to use the plate for my lunch. However taking it to work was inconvenient but I did use it to measure the portions (ID140, 24 years old, F, 35.4 kg/m2, lost 2.4 kg) |
| Overall experience | Grateful for having tried/taking part Enthusiasm for tool Added value of tool Beneficial improvements | Wanting it for self and others (n = 8) Liking it but not planning to adhere (n = 4) Reducing waste (n = 4) Helping other family with portion control (n = 1) Easy to clean (n = 3) Saving time (n = 2) | Wish I could buy a full set for everybody (ID146, 37 years old, F, 54.7 kg/m2, lost 0.4 kg) It helped considerably when portioning/serving food not only for myself but also my family, also helping to reduce less food wastage (ID142, 57 years old, F, 44.3 kg/m2, missing data for weight change) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almiron-Roig, E.; Majumdar, A.; Vaughan, D.; Jebb, S.A. Exploring the Experiences of People with Obesity Using Portion Control Tools—A Qualitative Study. Nutrients 2019, 11, 1095. https://doi.org/10.3390/nu11051095
Almiron-Roig E, Majumdar A, Vaughan D, Jebb SA. Exploring the Experiences of People with Obesity Using Portion Control Tools—A Qualitative Study. Nutrients. 2019; 11(5):1095. https://doi.org/10.3390/nu11051095
Chicago/Turabian StyleAlmiron-Roig, Eva, Anne Majumdar, David Vaughan, and Susan A. Jebb. 2019. "Exploring the Experiences of People with Obesity Using Portion Control Tools—A Qualitative Study" Nutrients 11, no. 5: 1095. https://doi.org/10.3390/nu11051095
APA StyleAlmiron-Roig, E., Majumdar, A., Vaughan, D., & Jebb, S. A. (2019). Exploring the Experiences of People with Obesity Using Portion Control Tools—A Qualitative Study. Nutrients, 11(5), 1095. https://doi.org/10.3390/nu11051095