Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review


Abstract
:1. Introduction
2. ACNs and Blood Pressure
- ACNs have been consistently shown to increase endothelial-derived nitric oxide (NO), via modulation of endothelial NO synthase (eNOS) expression and activity. Nitric oxide is one of the major contributors to endothelium-dependent vasorelaxation. It causes vascular smooth muscle relaxation following activation of soluble guanylate cyclase, which in turn increases cGMP. This blocks the release of intracellular calcium, preventing it from causing vascular smooth muscle contraction [15].
- Reactive oxygen species damage NO, thus promoting vasoconstriction and hypertension. Due to their strong antioxidant activity, ACNs act to prevent NO oxidative damage and radical-induced NO conversion, such as the reaction caused by NADPH oxidase [16].
- ACNs have been shown to reduce synthesis of vasoconstricting molecules, such as angiotensin II via inhibition of the angiotensin-converting enzyme (ACE) activity, endothelin-1, and thromboxanes via inhibition of the cyclooxygenase (COX) pathway [17].
2.1. Epidemiological and Meta-Analysis Data
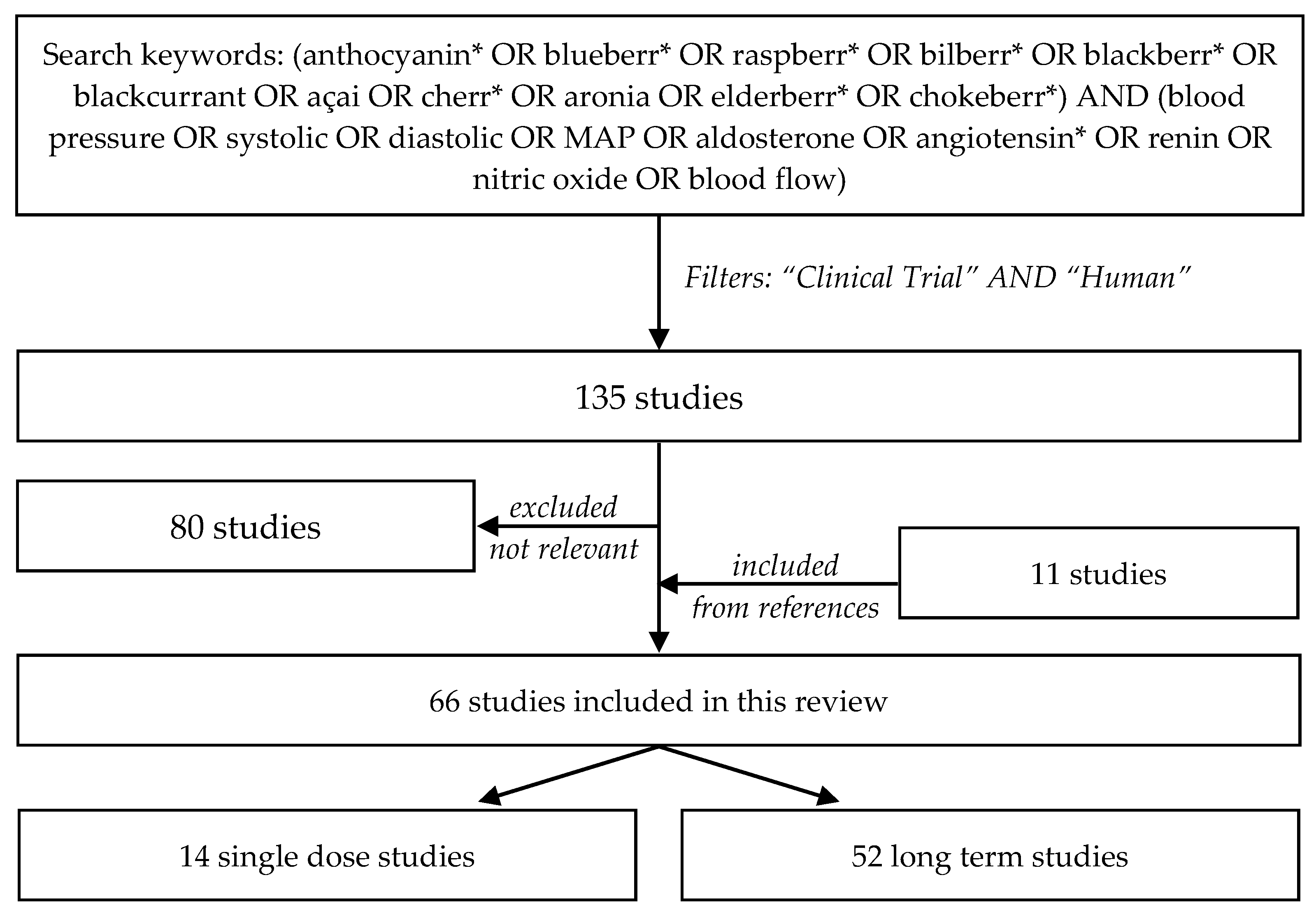
2.2. Literature Search
2.3. Single-Dose Interventions
2.4. Long-Term Interventions
3. Potential Factors Influencing ACN Effects on Blood Pressure
3.1. Baseline Characteristics of the Population
3.2. Dose Effect
3.3. Study Duration
3.4. Systolic vs. Diastolic Blood Pressure
3.5. Effect on Angiotensin-Converting Enzyme (ACE)
3.6. Synergistic Effects
3.7. Differential Effect of Individual ACNs
3.8. ACN Absorption and Metabolism
3.9. Interaction with Gut Microbiota
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Clark, J.L.; Zahradka, P.; Taylor, C.G. Efficacy of flavonoids in the management of high blood pressure. Nutr. Rev. 2015, 73, 799–822. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Colletti, A. Food and plant bioactives for reducing cardiometabolic disease risk: An evidence based approach. Food Funct. 2017, 8, 2076–2088. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Grassi, D.; Tocci, G.; Galletti, F.; Borghi, C.; Ferri, C. Nutrients and Nutraceuticals for the Management of High Normal Blood Pressure: An Evidence-Based Consensus Document. High Blood Press Cardiovasc. Prev. 2019, 26, 9–25. [Google Scholar] [CrossRef] [PubMed]
- De Ferrars, R.M.; Czank, C.; Zhang, Q.; Botting, N.P.; Kroon, P.A.; Cassidy, A.; Kay, C.D. The pharmacokinetics of anthocyanins and their metabolites in humans. Br. J. Pharmacol. 2014, 171, 3268–3282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoner, G.D.; Sardo, C.; Apseloff, G.; Mullet, D.; Wargo, W.; Pound, V.; Singh, A.; Sanders, J.; Aziz, R.; Casto, B.; et al. Pharmacokinetics of anthocyanins and ellagic acid in healthy volunteers fed freeze-dried black raspberries daily for 7 days. J. Clin. Pharmacol. 2005, 45, 1153–1164. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Beecher, G.R.; Holden, J.M.; Haytowitz, D.B.; Gebhardt, S.E.; Prior, R.L. Concentrations of anthocyanins in common foods in the United States and estimation of normal consumption. J. Agric. Food Chem. 2006, 54, 4069–4075. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C. Anthocyanins in cardiovascular disease. Adv. Nutr. 2011, 2, 1–7. [Google Scholar] [CrossRef]
- Mink, P.J.; Scrafford, C.G.; Barraj, L.M.; Harnack, L.; Hong, C.P.; Nettleton, J.A.; Jacobs, D.R., Jr. Flavonoid intake and cardiovascular disease mortality: A prospective study in postmenopausal women. Am. J. Clin. Nutr. 2007, 85, 895–909. [Google Scholar] [CrossRef]
- Vendrame, S.; Klimis-Zacas, D. Anti-inflammatory effect of anthocyanins via modulation of nuclear factor-κB and mitogen-activated protein kinase signaling cascades. Nutr. Rev. 2015, 73, 348–358. [Google Scholar] [CrossRef]
- Vendrame, S.; Del Bo’, C.; Ciappellano, S.; Riso, P.; Klimis-Zacas, D. Berry Fruit Consumption and Metabolic Syndrome. Antioxidants 2016, 5, 34. [Google Scholar] [CrossRef]
- Jurikova, T.; Mlcek, J.; Skrovankova, S.; Sumczynski, D.; Sochor, J.; Hlavacova, I.; Snopek, L.; Orsavova, J. Fruits of Black Chokeberry Aronia melanocarpa in the Prevention of Chronic Diseases. Molecules 2017, 22, 944. [Google Scholar] [CrossRef] [PubMed]
- García-Conesa, M.T.; Chambers, K.; Combet, E.; Pinto, P.; Garcia-Aloy, M.; Andrés-Lacueva, C.; de Pascual-Teresa, S.; Mena, P.; Konic Ristic, A.; Hollands, W.J.; et al. Meta-Analysis of the Effects of Foods and Derived Products Containing Ellagitannins and Anthocyanins on Cardiometabolic Biomarkers: Analysis of Factors Influencing Variability of the Individual Responses. Int. J. Mol. Sci. 2018, 19, 694. [Google Scholar] [CrossRef]
- Kelley, D.S.; Adkins, Y.; Laugero, K.D. A Review of the Health Benefits of Cherries. Nutrients 2018, 10, 368. [Google Scholar] [CrossRef]
- Corona, G.; Tang, F.; Vauzour, D.; Rodriguez-Mateos, A.; Spencer, J. Assessment of the anthocyanidin content of common fruits and development of a test diet rich in a range of anthocyanins. J. Berry Res. 2011, 1, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Bell, D.R.; Gochenaur, K. Direct vasoactive and vasoprotective properties of anthocyanin-rich extracts. J. Appl. Physiol. 2006, 100, 1164–1170. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.N.; Han, S.N.; Ha, T.J.; Kim, H.K. Black soybean anthocyanins attenuate inflammatory responses by suppressing reactive oxygen species production and mitogen activated protein kinases signaling in lipopolysaccharide-stimulated macrophages. Nutr. Res. Pract. 2017, 11, 357–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parichatikanond, W.; Pinthong, D.; Mangmool, S. Blockade of the renin-angiotensin system with delphinidin, cyanin, and quercetin. Planta Med. 2012, 78, 1626–1632. [Google Scholar] [CrossRef]
- Qin, Y.; Zhai, Q.; Li, Y.; Cao, M.; Xu, Y.; Zhao, K.; Wang, T. Cyanidin-3-O-glucoside ameliorates diabetic nephropathy through regulation of glutathione pool. Biomed. Pharmacother. 2018, 103, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, A.; O’Reilly, É.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Jennings, A.; Welch, A.A.; Fairweather-Tait, S.J.; Kay, C.; Minihane, A.M.; Chowienczyk, P.; Jiang, B.; Cecelja, M.; Spector, T.; Macgregor, A.; et al. Higher anthocyanin intake is associated with lower arterial stiffness and central blood pressure in women. Am. J. Clin. Nutr. 2012, 96, 781–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Chen, G.; Liao, D.; Zhu, Y.; Xue, X. Effects of Berries Consumption on Cardiovascular Risk Factors: A Meta-analysis with Trial Sequential Analysis of Randomized Controlled Trials. Sci. Rep. 2016, 6, 23625. [Google Scholar] [CrossRef]
- Yang, L.; Ling, W.; Du, Z.; Chen, Y.; Li, D.; Deng, S.; Liu, Z.; Yang, L. Effects of Anthocyanins on Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2017, 8, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Daneshzad, E.; Shab-Bidar, S.; Mohammadpour, Z.; Djafarian, K. Effect of anthocyanin supplementation on cardio-metabolic biomarkers: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2019, 38, 1153–1165. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Bo, Y.; Wang, X.; Lu, W.; Wang, X.; Han, Z.; Qiu, C. The Effect of Anthocyanins on Blood Pressure: A PRISMA-Compliant Meta-Analysis of Randomized Clinical Trials. Medicine (Baltimore) 2016, 95, e3380. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Sun, J.; Lu, W.; Wang, X.; Wang, X.; Han, Z.; Qiu, C. Effects of blueberry supplementation on blood pressure: A systematic review and meta-analysis of randomized clinical trials. J. Hum. Hypertens. 2017, 31, 165–171. [Google Scholar] [CrossRef]
- Alqurashi, R.M.; Galante, L.A.; Rowland, I.R.; Spencer, J.P.; Commane, D.M. Consumption of a flavonoid-rich açai meal is associated with acute improvements in vascular function and a reduction in total oxidative status in healthy overweight men. Am. J. Clin. Nutr. 2016, 104, 1227–1235. [Google Scholar] [CrossRef]
- Castro-Acosta, M.L.; Smith, L.; Miller, R.J.; McCarthy, D.I.; Farrimond, J.A.; Hall, W.L. Drinks containing anthocyanin-rich blackcurrant extract decrease postprandial blood glucose, insulin and incretin concentrations. J. Nutr. Biochem. 2016, 38, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Del Bo’, C.; Porrini, M.; Fracassetti, D.; Campolo, J.; Klimis-Zacas, D.; Riso, P. A single serving of blueberry (V. corymbosum) modulates peripheral arterial dysfunction induced by acute cigarette smoking in young volunteers: A randomized-controlled trial. Food Funct. 2014, 5, 3107–3116. [Google Scholar] [CrossRef]
- Del Bo’, C.; Deon, V.; Campolo, J.; Lanti, C.; Parolini, M.; Porrini, M.; Klimis-Zacas, D.; Riso, P. A serving of blueberry (V. corymbosum) acutely improves peripheral arterial dysfunction in young smokers and non-smokers: Two randomized, controlled, crossover pilot studies. Food Funct. 2017, 8, 4108–4117. [Google Scholar] [CrossRef]
- Igwe, E.O.; Charlton, K.E.; Roodenrys, S.; Kent, K.; Fanning, K.; Netzel, M.E. Anthocyanin-rich plum juice reduces ambulatory blood pressure but not acute cognitive function in younger and older adults: A pilot crossover dose-timing study. Nutr. Res. 2017, 47, 28–43. [Google Scholar] [CrossRef]
- Keane, K.M.; George, T.W.; Constantinou, C.L.; Brown, M.A.; Clifford, T.; Howatson, G. Effects of Montmorency tart cherry (Prunus Cerasus, L.) consumption on vascular function in men with early hypertension. Am. J. Clin. Nutr. 2016, 103, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Keane, K.M.; Haskell-Ramsay, C.F.; Veasey, R.C.; Howatson, G. Montmorency Tart cherries (Prunus cerasus L.) modulate vascular function acutely, in the absence of improvement in cognitive performance. Br. J. Nutr. 2016, 116, 1935–1944. [Google Scholar] [CrossRef] [PubMed]
- Keane, K.M.; Bailey, S.J.; Vanhatalo, A.; Jones, A.M.; Howatson, G. Effects of montmorency tart cherry (L. Prunus Cerasus) consumption on nitric oxide biomarkers and exercise performance. Scand. J. Med. Sci. Sports 2018, 28, 1746–1756. [Google Scholar] [CrossRef] [PubMed]
- Kent, K.; Charlton, K.E.; Jenner, A.; Roodenrys, S. Acute reduction in blood pressure following consumption of anthocyanin-rich cherry juice may be dose-interval dependant: A pilot cross-over study. Int. J. Food Sci. Nutr. 2016, 67, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Takenami, E.; Iwasaki-Kurashige, K.; Osada, T.; Katsumura, T.; Hamaoka, T. Effects of blackcurrant anthocyanin intake on peripheral muscle circulation during typing work in humans. Eur. J. Appl. Physiol. 2005, 94, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Mateos, A.; Rendeiro, C.; Bergillos-Meca, T.; Tabatabaee, S.; George, T.W.; Heiss, C.; Spencer, J.P. Intake and time dependence of blueberry flavonoid-induced improvements in vascular function: A randomized, controlled, double-blind, crossover intervention study with mechanistic insights into biological activity. Am. J. Clin. Nutr. 2013, 98, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Mateos, A.; Del Pino-García, R.; George, T.W.; Vidal-Diez, A.; Heiss, C.; Spencer, J.P. Impact of processing on the bioavailability and vascular effects of blueberry (poly)phenols. Mol. Nutr. Food Res. 2014, 58, 1952–1961. [Google Scholar] [CrossRef] [PubMed]
- Ataie-Jafari, A.; Hosseini, S.; Karimi, F.; Pajouhi, M. Effects of sour cherry juice on blood glucose and some cardiovascular risk factors improvements in diabetic women: A pilot study. Nutr. Food Sci. 2008, 38, 355–360. [Google Scholar] [CrossRef]
- Barona, J.; Aristizabal, J.C.; Blesso, C.N.; Volek, J.S.; Fernandez, M.L. Grape polyphenols reduce blood pressure and increase flow-mediated vasodilation in men with metabolic syndrome. J. Nutr. 2012, 142, 1626–1632. [Google Scholar] [CrossRef]
- Basu, A.; Du, M.; Leyva, M.J.; Sanchez, K.; Betts, N.M.; Wu, M.; Aston, C.E.; Lyons, T.J. Blueberries decrease cardiovascular risk factors in obese men and women with metabolic syndrome. J. Nutr. 2010, 140, 1582–1587. [Google Scholar] [CrossRef]
- Broncel, M.; Kozirog, M.; Duchnowicz, P.; Koter-Michalak, M.; Sikora, J.; Chojnowska-Jezierska, J. Aronia melanocarpa extract reduces blood pressure, serum endothelin, lipid, and oxidative stress marker levels in patients with metabolic syndrome. Med. Sci. Monit. 2010, 16, CR28–CR34. [Google Scholar] [PubMed]
- Chai, S.C.; Davis, K.; Wright, R.S.; Kuczmarski, M.F.; Zhang, Z. Impact of tart cherry juice on systolic blood pressure and low-density lipoprotein cholesterol in older adults: A randomized controlled trial. Food Funct. 2018, 9, 3185–3194. [Google Scholar] [CrossRef]
- Cook, M.D.; Myers, S.D.; Gault, M.L.; Edwards, V.C.; Willems, M.E. Cardiovascular function during supine rest in endurance-trained males with New Zealand blackcurrant: A dose-response study. Eur. J. Appl. Physiol. 2017, 117, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.D.; Myers, S.D.; Gault, M.L.; Willems, M.E.T. Blackcurrant Alters Physiological Responses and Femoral Artery Diameter during Sustained Isometric Contraction. Nutrients 2017, 9, 556. [Google Scholar] [CrossRef]
- Curtis, P.J.; Kroon, P.A.; Hollands, W.J.; Walls, R.; Jenkins, G.; Kay, C.D.; Cassidy, A. Cardiovascular disease risk biomarkers and liver and kidney function are not altered in postmenopausal women after ingesting an elderberry extract rich in anthocyanins for 12 weeks. J. Nutr. 2009, 139, 2266–2271. [Google Scholar] [CrossRef] [PubMed]
- Davinelli, S.; Bertoglio, J.C.; Zarrelli, A.; Pina, R.; Scapagnini, G. A Randomized Clinical Trial Evaluating the Efficacy of an Anthocyanin-Maqui Berry Extract (Delphinol®) on Oxidative Stress Biomarkers. J. Am. Coll. Nutr. 2015, 34, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Desai, T.; Bottoms, L.; Roberts, M. The effects of Montmorency tart cherry juice supplementation and FATMAX exercise on fat oxidation rates and cardio-metabolic markers in healthy humans. Eur. J. Appl. Physiol. 2018, 118, 2523–2539. [Google Scholar] [CrossRef] [Green Version]
- Draijer, R.; de Graaf, Y.; Slettenaar, M.; de Groot, E.; Wright, C.I. Consumption of a polyphenol-rich grape-wine extract lowers ambulatory blood pressure in mildly hypertensive subjects. Nutrients 2015, 7, 3138–3153. [Google Scholar] [CrossRef]
- Erlund, I.; Koli, R.; Alfthan, G.; Marniemi, J.; Puukka, P.; Mustonen, P.; Mattila, P.; Jula, A. Favorable effects of berry consumption on platelet function; blood pressure; and HDL cholesterol. Am. J. Clin. Nutr. 2008, 87, 323–331. [Google Scholar] [CrossRef]
- Gurrola-Díaz, C.M.; García-López, P.M.; Sánchez-Enríquez, S.; Troyo-Sanromán, R.; Andrade-González, I.; Gómez-Leyva, J.F. Effects of Hibiscus sabdariffa extract powder and preventive treatment (diet) on the lipid profiles of patients with metabolic syndrome (MeSy). Phytomedicine 2010, 17, 500–505. [Google Scholar] [CrossRef]
- Habanova, M.; Saraiva, J.A.; Haban, M.; Schwarzova, M.; Chlebo, P.; Predna, L.; Gažo, J.; Wyka, J. Intake of bilberries (Vaccinium myrtillus L.) reduced risk factors for cardiovascular disease by inducing favorable changes in lipoprotein profiles. Nutr. Res. 2016, 36, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Hassellund, S.S.; Flaa, A.; Sandvik, L.; Kjeldsen, S.E.; Rostrup, M. Effects of anthocyanins on blood pressure and stress reactivity: A double-blind randomized placebo-controlled crossover study. J. Hum. Hypertens. 2012, 26, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.S.; Kim, S.; Hong, S.J.; Choi, S.C.; Choi, J.H.; Kim, J.H.; Park, C.Y.; Cho, J.Y.; Lee, T.B.; Kwon, J.W.; et al. Black Raspberry Extract Increased Circulating Endothelial Progenitor Cells and Improved Arterial Stiffness in Patients with Metabolic Syndrome: A Randomized Controlled Trial. J. Med. Food 2016, 19, 346–352. [Google Scholar] [CrossRef]
- Jeong, H.S.; Hong, S.J.; Cho, J.Y.; Lee, T.B.; Kwon, J.W.; Joo, H.J.; Park, J.H.; Yu, C.W.; Lim, D.S. Effects of Rubus occidentalis extract on blood pressure in patients with prehypertension: Randomized, double-blinded, placebo-controlled clinical trial. Nutrition 2016, 32, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.A.; Figueroa, A.; Navaei, N.; Wong, A.; Kalfon, R.; Ormsbee, L.T.; Feresin, R.G.; Elam, M.L.; Hooshmand, S.; Payton, M.E.; et al. Daily blueberry consumption improves blood pressure and arterial stiffness in postmenopausal women with pre- and stage 1-hypertension: A randomized, double-blind, placebo-controlled clinical trial. J. Acad. Nutr. Diet. 2015, 115, 369–377. [Google Scholar] [CrossRef]
- Kardum, N.; Petrović-Oggiano, G.; Takic, M.; Glibetić, N.; Zec, M.; Debeljak-Martacic, J.; Konić-Ristić, A. Effects of glucomannan-enriched, aronia juice-based supplement on cellular antioxidant enzymes and membrane lipid status in subjects with abdominal obesity. Sci. World J. 2014, 2014, 869250. [Google Scholar] [CrossRef] [PubMed]
- Kardum, N.; Konić-Ristić, A.; Savikin, K.; Spasić, S.; Stefanović, A.; Ivanišević, J.; Miljković, M. Effects of polyphenol-rich chokeberry juice on antioxidant/pro-oxidant status in healthy subjects. J. Med. Food 2014, 17, 869–874. [Google Scholar] [CrossRef]
- Kardum, N.; Milovanović, B.; Šavikin, K.; Zdunić, G.; Mutavdžin, S.; Gligorijević, T.; Spasić, S. Beneficial Effects of Polyphenol-Rich Chokeberry Juice Consumption on Blood Pressure Level and Lipid Status in Hypertensive Subjects. J. Med. Food 2015, 18, 1231–1238. [Google Scholar] [CrossRef]
- Karlsen, A.; Retterstøl, L.; Laake, P.; Paur, I.; Bøhn, S.K.; Sandvik, L.; Blomhoff, R. Anthocyanins inhibit nuclear factor-kappaB activation in monocytes and reduce plasma concentrations of pro-inflammatory mediators in healthy adults. J. Nutr. 2007, 137, 1951–1954. [Google Scholar] [CrossRef]
- Kelley, D.S.; Adkins, Y.; Reddy, A.; Woodhouse, L.R.; Mackey, B.E.; Erickson, K.L. Sweet bing cherries lower circulating concentrations of markers for chronic inflammatory diseases in healthy humans. J. Nutr. 2013, 143, 340–344. [Google Scholar] [CrossRef]
- Kent, K.; Charlton, K.; Roodenrys, S.; Batterham, M.; Potter, J.; Traynor, V.; Gilbert, H.; Morgan, O.; Richards, R. Consumption of anthocyanin-rich cherry juice for 12 weeks improves memory and cognition in older adults with mild-to-moderate dementia. Eur. J. Nutr. 2017, 56, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Ray, S.; Craigie, A.M.; Kennedy, G.; Hill, A.; Barton, K.L.; Broughton, J.; Belch, J.J. Lowering of oxidative stress improves endothelial function in healthy subjects with habitually low intake of fruit and vegetables: A randomized controlled trial of antioxidant- and polyphenol-rich blackcurrant juice. Free Radic. Biol. Med. 2014, 72, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Kolehmainen, M.; Mykkänen, O.; Kirjavainen, P.V.; Leppänen, T.; Moilanen, E.; Adriaens, M.; Laaksonen, D.E.; Hallikainen, M.; Puupponen-Pimiä, R.; Pulkkinen, L.; et al. Bilberries reduce low-grade inflammation in individuals with features of metabolic syndrome. Mol. Nutr. Food Res. 2012, 56, 1501–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehtonen, H.M.; Suomela, J.P.; Tahvonen, R.; Yang, B.; Venojärvi, M.; Viikari, J.; Kallio, H. Different berries and berry fractions have various but slightly positive effects on the associated variables of metabolic diseases on overweight and obese women. Eur. J. Clin. Nutr. 2011, 65, 394–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.; Sorn, S.R.; Park, Y.; Park, H.K. Anthocyanin Rich-Black Soybean Testa Improved Visceral Fat and Plasma Lipid Profiles in Overweight/Obese Korean Adults: A Randomized Controlled Trial. J. Med. Food 2016, 19, 995–1003. [Google Scholar] [CrossRef]
- Li, D.; Zhang, Y.; Liu, Y.; Sun, R.; Xia, M. Purified anthocyanin supplementation reduces dyslipidemia; enhances antioxidant capacity; and prevents insulin resistance in diabetic patients. J. Nutr. 2015, 145, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Loo, B.M.; Erlund, I.; Koli, R.; Puukka, P.; Hellström, J.; Wähälä, K.; Mattila, P.; Jula, A. Consumption of chokeberry (Aronia mitschurinii) products modestly lowered blood pressure and reduced low-grade inflammation in patients with mildly elevated blood pressure. Nutr. Res. 2016, 36, 1222–1230. [Google Scholar] [CrossRef]
- Lynn, A.; Mathew, S.; Moore, C.T.; Russell, J.; Robinson, E.; Soumpasi, V.; Barker, M.E. Effect of a tart cherry juice supplement on arterial stiffness and inflammation in healthy adults: A randomised controlled trial. Plant Foods Hum. Nutr. 2014, 69, 122–127. [Google Scholar] [CrossRef]
- McAnulty, S.R.; McAnulty, L.S.; Morrow, J.D.; Khardouni, D.; Shooter, L.; Monk, J.; Gross, S.; Brown, V. Effect of daily fruit ingestion on angiotensin converting enzyme activity, blood pressure, and oxidative stress in chronic smokers. Free Radic. Res. 2005, 39, 1241–1248. [Google Scholar] [CrossRef]
- McAnulty, L.S.; Collier, S.R.; Landram, M.J.; Whittaker, D.S.; Isaacs, S.E.; Klemka, J.M.; Cheek, S.L.; Arms, J.C.; McAnulty, S.R. Six weeks daily ingestion of whole blueberry powder increases natural killer cell counts and reduces arterial stiffness in sedentary males and females. Nutr. Res. 2014, 34, 577–584. [Google Scholar] [CrossRef]
- Naruszewicz, M.; Laniewska, I.; Millo, B.; Dłuzniewski, M. Combination therapy of statin with flavonoids rich extract from chokeberry fruits enhanced reduction in cardiovascular risk markers in patients after myocardial infraction (MI). Atherosclerosis 2007, 194, e179–e184. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.; Salo, I.; Plaza, M.; Björck, I. Effects of a mixed berry beverage on cognitive functions and cardiometabolic risk markers; A randomized cross-over study in healthy older adults. PLoS ONE 2017, 12, e0188173. [Google Scholar] [CrossRef] [PubMed]
- Ohguro, H.; Ohguro, I.; Yagi, S. Effects of black currant anthocyanins on intraocular pressure in healthy volunteers and patients with glaucoma. J. Ocul. Pharmacol. Ther. 2013, 29, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Ohguro, H.; Ohguro, I.; Katai, M.; Tanaka, S. Two-year randomized, placebo-controlled study of black currant anthocyanins on visual field in glaucoma. Ophthalmologica 2012, 228, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Xia, M.; Ma, J.; Hao, Y.; Liu, J.; Mou, H.; Cao, L.; Ling, W. Anthocyanin supplementation improves serum LDL- and HDL-cholesterol concentrations associated with the inhibition of cholesteryl ester transfer protein in dyslipidemic subjects. Am. J. Clin. Nutr. 2009, 90, 485–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puupponen-Pimiä, R.; Seppänen-Laakso, T.; Kankainen, M.; Maukonen, J.; Törrönen, R.; Kolehmainen, M.; Leppänen, T.; Moilanen, E.; Nohynek, L.; Aura, A.M.; et al. Effects of ellagitannin-rich berries on blood lipids; gut microbiota; and urolithin production in human subjects with symptoms of metabolic syndrome. Mol. Nutr. Food Res. 2013, 57, 2258–2263. [Google Scholar] [CrossRef]
- Riso, P.; Klimis-Zacas, D.; Del Bo’, C.; Martini, D.; Campolo, J.; Vendrame, S.; Møller, P.; Loft, S.; De Maria, R.; Porrini, M. Effect of a wild blueberry (Vaccinium angustifolium) drink intervention on markers of oxidative stress, inflammation and endothelial function in humans with cardiovascular risk factors. Eur. J. Nutr. 2013, 52, 949–961. [Google Scholar] [CrossRef]
- Skoczynska, A.; Jedrychowska, I.; Poręba, R.; Affelska-Jercha, A.; Turczyn, B.; Wojakowska, A.; Andrzejak, R.; Jedrychowska-Bianchi, I. Influence of chokeberry juice on arterial blood pressure and lipid parameters in men with mild hypercholesterolemia. Pharmacol. Rep. 2007, 59, 177–182. [Google Scholar]
- Sikora, J.; Broncel, M.; Mikiciuk-Olasik, E. Aronia melanocarpa Elliot reduces the activity of angiotensin i-converting enzyme-in vitro and ex vivo studies. Oxid. Med. Cell. Longev. 2014, 2014, 739721. [Google Scholar] [CrossRef]
- Stull, A.J.; Cash, K.C.; Johnson, W.D.; Champagne, C.M.; Cefalu, W.T. Bioactives in Blueberries Improve Insulin Sensitivity in Obese; Insulin-Resistant Men and Women. J. Nutr. 2010, 140, 1764–1768. [Google Scholar] [CrossRef]
- Stull, A.J.; Cash, K.C.; Champagne, C.M.; Gupta, A.K.; Boston, R.; Beyl, R.A.; Johnson, W.D.; Cefalu, W.T. Blueberries improve endothelial function, but not blood pressure, in adults with metabolic syndrome: A randomized, double-blind, placebo-controlled clinical trial. Nutrients 2015, 7, 4107–4123. [Google Scholar] [CrossRef]
- Thompson, K.; Hosking, H.; Pederick, W.; Singh, I.; Santhakumar, A.B. The effect of anthocyanin supplementation in modulating platelet function in sedentary population: A randomised, double-blind, placebo-controlled, cross-over trial. Br. J. Nutr. 2017, 118, 368–374. [Google Scholar] [CrossRef]
- Tjelle, T.E.; Holtung, L.; Bøhn, S.K.; Aaby, K.; Thoresen, M.; Wiik, S.Å.; Paur, I.; Karlsen, A.S.; Retterstøl, K.; Iversen, P.O.; et al. Polyphenol-rich juices reduce blood pressure measures in a randomised controlled trial in high normal and hypertensive volunteers. Br. J. Nutr. 2015, 114, 1054–1063. [Google Scholar] [CrossRef] [Green Version]
- Udani, J.K.; Singh, B.B.; Singh, V.; Barrett, M.L. Effects of Açai (Euterpe oleracea Mart.) berry preparation on metabolic parameters in a healthy overweight population: A pilot study. Nutr. J. 2011, 10, 45. [Google Scholar] [CrossRef]
- Whyte, A.R.; Cheng, N.; Fromentin, E.; Williams, C.M. A Randomized, Double-Blinded, Placebo-Controlled Study to Compare the Safety and Efficacy of Low Dose Enhanced Wild Blueberry Powder and Wild Blueberry Extract (ThinkBlue™) in Maintenance of Episodic and Working Memory in Older Adults. Nutrients 2018, 10, 660. [Google Scholar] [CrossRef]
- Xie, L.; Vance, T.; Kim, B.; Lee, S.G.; Caceres, C.; Wang, Y.; Hubert, P.A.; Lee, J.Y.; Chun, O.K.; Bolling, B.W. Aronia berry polyphenol consumption reduces plasma total and low-density lipoprotein cholesterol in former smokers without lowering biomarkers of inflammation and oxidative stress: A randomized controlled trial. Nutr. Res. 2017, 37, 67–77. [Google Scholar] [CrossRef]
- Zhang, P.W.; Chen, F.X.; Li, D.; Ling, W.H.; Guo, H.H. A CONSORT-compliant; randomized; double-blind; placebo-controlled pilot trial of purified anthocyanin in patients with nonalcoholic fatty liver disease. Medicine (Baltimore) 2015, 94, e758. [Google Scholar] [CrossRef]
- Zhu, Y.; Ling, W.; Guo, H.; Song, F.; Ye, Q.; Zou, T.; Li, D.; Zhang, Y.; Li, G.; Xiao, Y.; et al. Anti-inflammatory effect of purified dietary anthocyanin in adults with hypercholesterolemia: A randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 843–849. [Google Scholar] [CrossRef]
- Kay, C.D.; Mazza, G.; Holub, B.J.; Wang, J. Anthocyanin metabolites in human urine and serum. Br. J. Nutr. 2004, 91, 933–942. [Google Scholar] [CrossRef] [Green Version]
- Mazza, G.; Kay, C.D.; Cottrell, T.; Holub, B.J. Absorption of anthocyanins from blueberries and serum antioxidant status in human subjects. J. Agric. Food Chem. 2002, 50, 7731–7737. [Google Scholar] [CrossRef]
- Fracassetti, D.; Del Bo’, C.; Simonetti, P.; Gardana, C.; Klimis-Zacas, D.; Ciappellano, S. Effect of Time and storage temperature on anthocyanin decay and antioxidant activity in wild blueberry (Vaccinium angustifolium) powder. J. Agric. Food Chem. 2013, 61, 2999–3005. [Google Scholar] [CrossRef]
- Wiseman, W.; Egan, J.M.; Slemmer, J.E.; Shaughnessy, K.S.; Ballem, K.; Gottschall-Pass, K.T.; Sweeney, M.I. Feeding blueberry diets inhibits angiotensin II-converting enzyme (ACE) activity in spontaneously hypertensive stroke-prone rats. Can. J. Physiol. Pharmacol. 2011, 89, 67–71. [Google Scholar] [CrossRef]
- Zhai, C.; Cong, H.; Zhang, H.; Hou, K.; Zhang, Y.; Zhang, Y. M235T polymorphism in the angiotensinogen gene and cardiovascular disease: An updated meta-analysis of 39 case-control comparisons. Anatol. J. Cardiol. 2019, 21, 222–232. [Google Scholar] [CrossRef]
- Rechner, A.R.; Kroner, C. Anthocyanins and colonic metabolites of dietary polyphenols inhibit platelet function. Thromb. Res. 2005, 116, 327–334. [Google Scholar] [CrossRef]
- McGhie, T.K.; Walton, M.C. The bioavailability and absorption of anthocyanins: Towards a better understanding. Mol. Nutr. Food Res. 2007, 51, 702–713. [Google Scholar] [CrossRef]
- Jama, H.; Beale, A.; Shihata, W.A.; Marques, F.Z. The effect of diet on hypertensive pathology: Is there a link via gut microbiota-driven immune-metabolism? Cardiovasc. Res. 2019, cvz091. [Google Scholar] [CrossRef]
- Williamson, G.; Clifford, M.N. Colonic metabolites of berry polyphenols: The missing link to biological activity? Br. J. Nutr. 2010, 104, S48–S66. [Google Scholar] [CrossRef]
- Krga, I.; Tamaian, R.; Mercier, S.; Boby, C.; Monfoulet, L.E.; Glibetic, M.; Morand, C.; Milenkovic, D. Anthocyanins and their gut metabolites attenuate monocyte adhesion and transendothelial migration through nutrigenomic mechanisms regulating endothelial cell permeability. Free Radic. Biol. Med. 2018, 124, 364–379. [Google Scholar] [CrossRef]
- Zhang, X.; Sandhu, A.; Edirisinghe, I.; Burton-Freeman, B. An exploratory study of red raspberry (Rubus idaeus L.) (poly)phenols/metabolites in human biological samples. Food Funct. 2018, 9, 806–818. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Study Design | Control | Participants a | Source of ACN | Daily Dose of ACN b | Effect on Blood Pressure c |
|---|---|---|---|---|---|---|
| Alquarashi [26] | Crossover | Double-blind, controlled | 23 healthy male, age 46 ± 9, BMI 28 ± 2 | Açai-based smoothie, (control: macronutrient-matched smoothie), following high-fat meal | 493 mg | = SBP, =DBP at 2 and 6 h |
| Castro-Acosta [27] | Crossover | Double-blind | 23 healthy, age 46 ± 14, BMI 26 ± 3.8 | Blackcurrant extract drink, following high-carbohydrate meal | 150, 300, or 600 mg ACN | = SBP, =DBP after 2 h |
| Del Bo [28] | Crossover | Controlled | 10 younger adults, age 21 ± 2, BMI 23 ± 2 | Blueberry smoothie (control: sugar matched jelly) | 348 mg | = SBP, =DBP |
| Del Bo [28] | Crossover | Controlled | 16 smokers, age 24 ± 1, BMI 23 ± 1 | Blueberry drink (control: sugar matched drink), followed by smoking 1 cigarette | 348 mg | < SBP post smoke, = DBP |
| Del Bo [29] | Crossover | Controlled | 12 healthy male, age 24 ± 1, BMI 23 ± 1 | Blueberry drink (control: sugar matched drink) | 309 mg | =SBP, =DBP |
| Del Bo [29] | Crossover | Controlled | 12 healthy male smokers, age 15 ± 2, BMI 23 ± 1 | Blueberry drink (control: sugar matched drink), followed by smoking 1 cigarette | 309 mg | Did not restore blood pressure |
| Igwe [30] | Crossover | Controlled | 12 young (age 31 ± 8, 23 ± 2) and 12 older adults (age 77 ± 6, BMI, 26 ± 3) | Plum juice | 369 mg | <SBP, <DBP, <MAP in both age groups, compared to baseline |
| Keane [31] | Crossover | Single-blind, placebo-controlled | 15 male with early hypertension, age 31 ± 9, BMI 27 ± 4 | Tart cherry juice | 73.5 mg | <SBP, <MAP, = DBP |
| Keane [32] | Crossover | Double-blind, placebo-controlled | 27 healthy, age 50 ± 6, BMI 26 ± 5 | Tart cherry juice | 68 mg | <SBP |
| Keane [33] | Crossover | Double-blind, placebo-controlled | 10 athletes, age 28 ± 7, BW 78 ± 9 | Tart cherry juice | 68 mg | <SBP, =DBP, =MAP |
| Kent [34] | Crossover | Controlled | 6 young (age 22 ± 1, BMI 26 ± 4) and 7 older adults (age 78 ± 6, BMI 29 ± 4) | Cherry juice, in single dose or three doses over 2 hours | 207 mg | < SBP, <DBP at 2 h after consumption, if given in a single dose (but not if split in three doses given 1 hour apart) |
| Matsumoto [35] | Crossover | Double-blind, placebo-controlled | 9 healthy male, age 30 ± 1, BMI? | Blackcurrant ACN extract | (17 mg/kg) | =SBP, =DBP |
| Rodriguez-Mateos [36] | Crossover | Double-blind, controlled | 10 healthy male, age 27 ± 3, BMI 25 ± 3 | Blueberry drink or nutrient-matched control | 310 mg | =SBP, =DBP |
| Rodriguez-Mateos [37] | Crossover | Double-blind, controlled | 10 healthy, age 27 ± 1, BMI 25 ± 1 | Freeze-dried blueberry drink, blueberry baked product (with same amount of blueberry powder), or baked control | 339 mg in drink, 196 mg in baked product | =SBP, =DBP |
| Reference | Duration | Study Design | Control | Participants a | Source of ACN | Daily Dose of ACN b | Effect on Blood Pressure c |
|---|---|---|---|---|---|---|---|
| Ataie-Jafari [38] | 6 weeks | Pre-post | - | 19 women with diabetes, age 53 ± 9, BMI 30 ± 4 | Sour cherry juice | 720 mg | <SBP, <DBP |
| Barona [39] | 4 weeks | Crossover | Double-blind, placebo-controlled | 24 male with, age 51 ± 10, BMI 32 ± 5 | Freeze-dried grape phenolic extract | 35 mg | <SBP, =DBP |
| Basu [40] | 8 weeks | Parallel arms | Controlled | 48 with MetS, age 50 ± 3, BMI 38 ± 2 | Freeze-dried blueberry beverage (control: water) | 742 mg | <SBP, <DBP |
| Broncel [41] | 8 weeks | Pre-post | - | 25 with MetS, age 42–65, BMI 31 ± 3 | Aronia extract | 300 mg | <SBP, <DBP |
| Chai [42] | 12 weeks | Parallel arms | Controlled | 34 overweight older adults, age 70 ± 4, BMI 28 ± 4 | Tart cherry juice (control: energy and sugar matched drink) | (451 mg total phenolics) | < SBP, =DBP |
| Cook [43] | 12 days | Crossover | Controlled | 15 athletes, age 38 ± 12, BW 76 ± 10 | Blackcurrant extract (control: no extract) | 105, 210, or 315 mg | = SBP, =DBP, <MAP with 210 and 315 |
| Cook [44] | 1 week | Crossover | Double-blind, placebo-controlled | 13 healthy male, age 26 ± 4, BMI 25 ± 3 | Blackcurrant extract | 315 mg | = SBP, =DBP, =MAP at rest, <SBP, <DBP, <MAP during isomeric contraction |
| Curtis [45] | 12 weeks | Parallel arms | Double-blind, placebo-controlled | 52 healthy postmenopausal women, age 58 ± 6, BMI 25 ± 4 | ACN-rich elderberry extract capsule | 500 mg | = SBP, =DBP |
| Davinelli [46] | 4 weeks | Parallel arms | Double-blind, placebo-controlled | 42 overweight, age 45–65, BMI 29 ± 4 | ACN-rich maqui berry extract | 486 mg | = SBP, =DBP |
| Desai [47] | 20 days | Parallel arms | Single-blind, placebo-controlled | 11 healthy, age 30 ± 10, BMI 24 ± 3 | Tart cherry juice | 540 mg | = SBP, =DBP pre or post exercise |
| Draijer [48] | 4 weeks | Crossover | Double-blind, placebo-controlled | 60 mildly hypertensive, age 58 ± 10, BMI 26 ± 4 | Grape and grape wine extracts | (800 mg total phenolics) | <SBP, <DBP with grape wine but not grape alone |
| Erlund [49] | 8 weeks | Parallel arms | Single-blind, placebo-controlled | 72 with CVD risk factors, age 58 ± 6, BMI 26 ± 3 | Berry mix (bilberries, lingonberries, black currant, strawberry, chokeberry, and raspberry) | 515 mg | <SBP, =DBP |
| Gurrola-Diaz [50] | 4 weeks | Parallel arms | Controlled | 73 healthy and 51 MetS patients, age 49 ± 7, BMI 29 ± 5 | Hibiscus sabdariffa extract powder (control: preventive diet) | 19 mg | = SBP, =DBP in healthy and MetS patients |
| Habanova [51] | 6 weeks | Pre-post | - | 36 healthy, age 48 ± 6, BMI 27 ± 4 | Frozen bilberries, 3 times a week | 456 mg, 3 times/week | = SBP, =DBP |
| Hassellund [52] | 4 weeks | Crossover | Double-blind, placebo-controlled | 31 moderately hypertensive male, age 41 ± 3, BMI 27 ± 3 | ACN capsule (isolated from bilberry and blackcurrant) | 640 mg | = sitting, supine, or 24h-ambulatory blood pressure, or blood pressure during stress test |
| Jeong [53] | 8 weeks | Parallel arms | Double-blind, placebo-controlled | 45 prehypertensive, age 57 ± 12, BMI 25 ± 3 | Dried unripe black raspberry powder | (1500 mg or 2500 mg powder) | <SBP with high dose, =DBP |
| Jeong [54] | 12 weeks | Parallel arms | Double-blind, placebo-controlled | 51 with MetS, age 59 ± 10, BMI 25 ± 4 | Dried unripe black raspberry powder | (750 mg of dry powder) | =SBP, =DBP |
| Johnson [55] | 8 weeks | Parallel arms | Double-blind, placebo-controlled | 48 postmenopausal women with pre- and stage 1-hypertension, age 59 ± 5, BMI 31 ± 6 | Freeze-dried blueberry powder mixed with water | 469 mg | <SBP, <DBP |
| Kardum [56] | 4 weeks | Pre-post | - | 20 abdominally obese postmenopausal women, age 53 ± 5, BMI 36 ± 4 | Glucomannan-enriched aronia juice-based supplement | 25 mg | <SBP, =DBP |
| Kardum [57] | 12 weeks | Pre-post | - | 29 healthy women, age 35 ± 8, BMI 23 ± 4 | Glucomannan-enriched aronia juice-based supplement | 25 mg | = SBP, =DBP |
| Kardum [58] | 4 weeks | Pre-post | - | 23 pre- or stage 1 hypertensive, age 48 ± 10, weight 82 ± 20 | Aronia juice | 358 mg | <SBP, <DBP, < average 24 h BP |
| Karlsen [59] | 3 weeks | Parallel arms | Placebo-controlled | 118 adults, age 61 ±?, BMI 25 ±? | Purified ACN capsule from bilberry and blackcurrant | 300 mg | =SBP, =DBP |
| Kelley [60] | 4 weeks | Pre-post | - | 18 healthy, age 50 ± 4, BMI 26 ± 4 | Fresh sweet cherries | (280 g fresh cherries) | =SBP, =DBP at the end of the trial and after 1 month |
| Kent [61] | 12 weeks | Parallel arms | Controlled | 49 older adults, age 80 ± 6, BMI 26 ± 3 | Cherry juice (control: ACN free apple juice) | 138 mg | <SBP, =DBP |
| Khan [62] | 6 weeks | Parallel arms | Placebo-controlled | 66 healthy adults, age 52 ± 10, BMI 29 ± 6 | Blackcurrant juice, low or high dose | 40 mg or 143 mg | =SBP, =DBP |
| Kolehmanen [63] | 8 weeks | Parallel arms | Controlled | 27 with MetS, age 51 ± 6, BMI 32 ± 4 | Bilberries (400 g fresh) | 1381 mg | =SBP, =DBP |
| Lehtonen [64] | 20 weeks | Parallel arms | Controlled | 61 women, age 43 ±?, BMI 29 ±? | 163 g mix of 18 berries (control: lifestyle intervention) | (equivalent to 163 g fresh berries) | =SBP, =DBP |
| Lee [65] | 8 weeks | Parallel arms | Double-blind, placebo-controlled | 63 overweight or obese, age 31 ± 9, BMI 28 ± 2 | ACN-rich black soybean extract | 31.45 mg | =SBP, =DBP |
| Li [66] | 24 weeks | Parallel arms | Double-blind, placebo-controlled | 58 with type II diabetes, age 58 ± 3, BMI 24 ± 3, | ACN capsules (isolated from bilberry and black currant) | 320 mg | <SBP, =DBP |
| Loo [67] | 16 weeks | Crossover | Single-blind, placebo-controlled | 37 with mild hypertension, age 40–70, BMI 26 ± 3 | Cold-pressed Aronia juice and oven-dried Aronia powder | 1024 mg | <daytime DBP (recorded over 15 hours), =SBP |
| Lynn [68] | 6 weeks | Parallel arms | Controlled | 47 healthy adults, age 38 ± 6, BMI 24 ± 3 | Tart cherry concentrate, (control: energy matched drink) | 274.5 mg | =SBP, =DBP |
| Matsumoto [35] | 2 weeks | Crossover | Double-blind, placebo-controlled | 11 healthy, age 39 ± 12, BMI? | Blackcurrant ACN extract | (7.7 mg/kg) | =SBP, =DBP after 30 minutes typing workload |
| McAnulty [69] | 3 weeks | Parallel arms | Controlled | 20 smokers, age 28 ± 4, BMI 29 ± 3 | Blueberry 250 g | =SBP, =DBP, = ACE activity | |
| McAnulty [70] | 6 weeks | Parallel arms | Placebo-controlled | 25 healthy, age 43 ± 12, BMI 26 ± 4 | Freeze-dried blueberry powder, equivalent to 250 g berries | <aortic systolic pressures, <SBP, =DBP, <DBP in the subset of prehypertensive subjects (9 subjects) | |
| Naruszewicz [71] | 6 weeks | Parallel arms | Double-blind, placebo-controlled | 44 post myocardial infarction patients, receiving statin therapy, age 66 ± 8, BMI 27 ± 3 | 255 mg/day Aronia flavonoid extract | 64 mg | <SBP, <DBP |
| Nilsson [72] | 5 weeks | Crossover | Controlled | 40 healthy, age 63 ± 1, BMI 24 ± 1 | Mixed berry drink (1/3 blueberries, 1/9 blackcurrant, 1/9 elderberry, 1/9 lingonberry, 1/9 strawberry, 2/9 tomato), or sugar-matched control | 248 mg | =SBP, =DBP |
| Ohguro [73] | 4 weeks | Crossover | Double-blind, placebo-controlled | 12 healthy, age 39 ± 8, BMI? | Blackcurrant ACN extract | 50 mg | < intraocular pressure, =SBP, =DBP |
| Ohguro [74] | 2 years | Parallel arms | Double-blind, placebo-controlled | 21 glaucoma patients, age 61 ± 7, BMI? | Blackcurrant ACN extract | 50 mg | < intraocular pressure, =SBP, =DBP |
| Qin [75] | 12 weeks | Parallel arms | Double-blind, placebo-controlled | 120 dyslipidemic, age 55 ± 5, BMI 26 ± 4 | ACN capsule (from bilberry and blackcurrant) | 160 mg | =SBP, =DBP |
| Puupponen-Pimia [76] | 8 weeks | Parallel arms | Controlled | 37 overweight with MetS, age 51 ± 7, BMI 32 ± 4 | 300 g frozen berries (raspberries, strawberries, and cloudberries) | (equivalent to 300 g fresh berries) | =SBP, =DBP |
| Riso [77] | 6 weeks | Crossover | Placebo-controlled | 18 male with risk factors for CVD, age 48 ± 10, BMI 25 ± 3 | Wild blueberry drink | 400 mg | =SBP, =DBP |
| Skoczynska [78] | 6 weeks | Pre-post | - | 58 male with mild hypercholesterolemia, age 54 ± 6, BMI 28 ± 3 | Aronia juice 250 mL | 90 mg | <SBP after 12 weeks, <DBP after 6 and 12 weeks |
| Sikora [79] | 8 weeks | Pre-post | - | 23 with untreated MetS (BMI 31 ± 4), reference group with 25 treated MetS patients (BMI 29 ± 3) and 20 healthy controls (BMI 23 ± 1) | Aronia extract supplements or ACE-inhibitors | 60 mg | <SBP, <DBP, <ACE activity |
| Stull [80] | 6 weeks | Parallel arms | Double-blind, placebo-controlled | 32 obese with insulin-resistance, age 52 ± 3, BMI 37 ± 1 | Blueberry powder added to smoothie smoothie and yogurt | 580 mg | =SBP, =DBP |
| Stull [81] | 6 weeks | Parallel arms | Double-blind, placebo-controlled | 44 adults, age 57 ± 2, BMI 36 ± 1 | Blueberry powder added to smoothie and yogurt | 580 mg | =SBP, =DBP |
| Thompson [82] | 4 weeks | Crossover | Double-blind, placebo-controlled | 16 sedentary, age 38 ± 12, BMI 23 ± 2 | ACN capsule | 320 mg | =SBP, =DBP |
| Tjelle [83] | 12 weeks | Parallel arms | Double-blind, placebo-controlled | 134 prehypertensive or hypertensive, age 52 ± 6, BMI 26 ± 3 | Mixed berry fruit juice (red grape, aronia, cherry, and bilberry) or same juice enriched with black currant press residue | 43 mg or 210 mg | <SBP in both juice groups, more pronounced if high BP baseline value, =DBP |
| Udani [84] | 4 weeks | Pre-post | - | 10 overweight, age 28 ±?, BMI 27 ± 2 | 100 g açai pulp | 0.77 mg/mL ACN (density unknown) | =SBP, =DBP |
| Whyte [85] | 6 months | Parallel arms | Double-blind, placebo-controlled | 122 older adults, age 71 ± 4, BW 71 ± 4 | Whole wild blueberry powder 1 or 2 g, or extract 200 mg | 2.7, or 5.4 or 14 mg | <SBP with extract, but not with powders, at 3 and 6 months |
| Xie [86] | 12 weeks | Parallel arms | Placebo-controlled | 49 healthy former smokers, age 35 ± 3, BMI 26 ± 1 | 500 mg aronia extract | 45.1 mg | =SBP, =DBP |
| Zhang [87] | 12 weeks | Parallel arms | Double-blind, placebo-controlled | 72 patients with nonalcoholic fatty liver disease, age 46 ± 8, BMI 27 ± 3 | ACN capsules (isolated from bilberry and black currant) | 320 mg | =SBP, =DBP |
| Zhu [88] | 24 weeks | Parallel arms | Double-blind, placebo-controlled | 146 hypercholesterolemic, age 56 ± 6, BMI 27 ± 2 | ACN capsules (isolated from bilberry and black currant) | 320 mg | =SBP, =DBP |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vendrame, S.; Klimis-Zacas, D. Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review. Nutrients 2019, 11, 1431. https://doi.org/10.3390/nu11061431
Vendrame S, Klimis-Zacas D. Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review. Nutrients. 2019; 11(6):1431. https://doi.org/10.3390/nu11061431
Chicago/Turabian StyleVendrame, Stefano, and Dorothy Klimis-Zacas. 2019. "Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review" Nutrients 11, no. 6: 1431. https://doi.org/10.3390/nu11061431
APA StyleVendrame, S., & Klimis-Zacas, D. (2019). Potential Factors Influencing the Effects of Anthocyanins on Blood Pressure Regulation in Humans: A Review. Nutrients, 11(6), 1431. https://doi.org/10.3390/nu11061431