Selenium and Health: An Update on the Situation in the Middle East and North Africa


Abstract
:1. Introduction
2. Selenium: A Focus on Biology
2.1. Selenoproteins as Mediators of Se Actions
2.2. Synthesis and Co-Translational Incorporation of Selenocysteine in Humans
3. Selenium in Health and Disease: The Importance of a Balanced Intake
3.1. Pregnancy
3.2. Diabetes Mellitus
3.3. Cardiovascular Disease (CVD)
3.4. Cancer
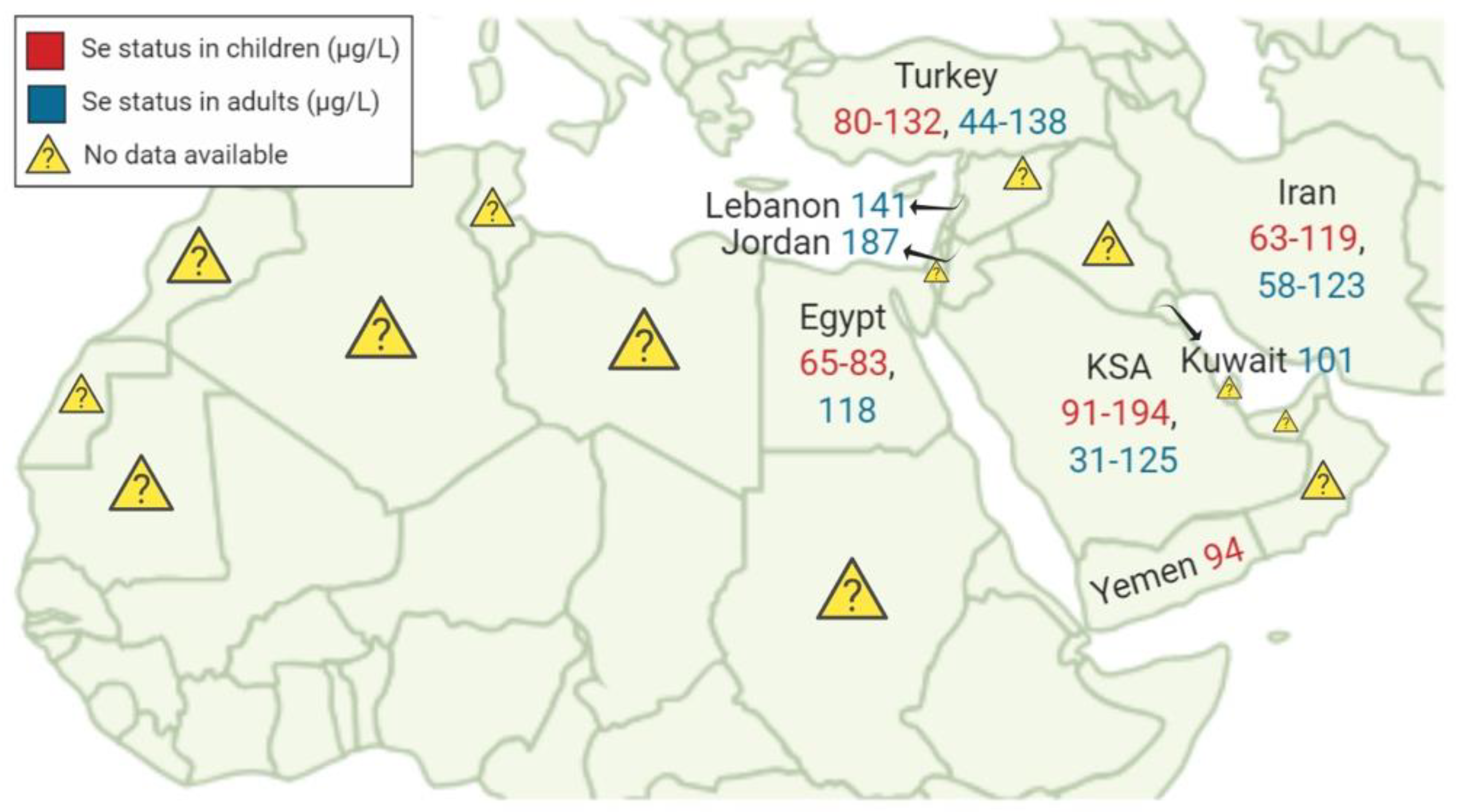
4. Regional Variability of Se Status: A Focus on the Situation in the Middle Eastern and North Africa (MENA) Region
4.1. Turkey
4.2. Jordan
4.3. Iran
4.4. Kingdom of Saudi Arabia (KSA)
4.5. Egypt
4.6. Qatar
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weeks, M.E. The discovery of the elements. VI. Tellurium and selenium. J. Chem. Educ. 1932, 9, 474. [Google Scholar] [CrossRef]
- Zachariah, M. High Selenium Induces Endothelial Dysfunction Via Endoplasmic Reticulum Stress. Ph.D. Thesis, University of Surrey, Guildford, UK, 2017. [Google Scholar]
- Stoffaneller, R.; Morse, L.N. A Review of Dietary Selenium Intake and Selenium Status in Europe and the Middle East. Nutrients 2015, 7, 1494–1537. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, K.S.; Lei, X.G. Selenium. Adv. Nutr. 2016, 7, 415–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Al-Attas, O.; Yakout, S.; Aljohani, N.; Al-Fawaz, H.; Alokail, M.S. Dietary products consumption in relation to serum 25-hydroxyvitamin D and selenium level in Saudi children and adults. Int. J. Clin. Exp. Med. 2015, 8, 1305–1314. [Google Scholar] [PubMed]
- Qazi, I.H.; Angel, C.; Yang, H.; Pan, B.; Zoidis, E.; Zeng, C.J.; Han, H.; Zhou, G.B. Selenium, Selenoproteins, and Female Reproduction: A Review. Molecules 2018, 23, 3053. [Google Scholar] [CrossRef] [PubMed]
- Bleys, J.; Navas-Acien, A.; Guallar, E. Serum selenium levels and all-cause, cancer, and cardiovascular mortality among US adults. Arch. Intern. Med. 2008, 168, 404–410. [Google Scholar] [CrossRef]
- Rocourt, C.R.; Cheng, W.H. Selenium supranutrition: Are the potential benefits of chemoprevention outweighed by the promotion of diabetes and insulin resistance? Nutrients 2013, 5, 1349–1365. [Google Scholar] [CrossRef]
- Pieczyńska, J.; Grajeta, H. The role of selenium in human conception and pregnancy. J. Trace Elem. Med. Biol. 2015, 29, 31–38. [Google Scholar] [CrossRef]
- Combs, F., Jr. Biomarkers of selenium status. Nutrients 2015, 7, 2209–2236. [Google Scholar] [CrossRef]
- Papp, L.V.; Lu, J.; Holmgren, A.; Khanna, K.K. From selenium to selenoproteins: Synthesis, identity, and their role in human health. Antioxid. Redox Signal. 2007, 9, 775–806. [Google Scholar] [CrossRef]
- Rayman, M.P. The importance of selenium to human health. Lancet 2000, 356, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Xu, X.-M.; Carlson, B.A.; Mix, H.; Zhang, Y.; Saira, K.; Glass, R.S.; Berry, M.J.; Gladyshev, V.N.; Hatfield, D.L. Biosynthesis of selenocysteine on its tRNA in eukaryotes. PLoS Biol. 2007, 5, e4. [Google Scholar] [CrossRef] [PubMed]
- Turanov, A.A.; Xu, X.-M.; Carlson, B.A.; Yoo, M.-H.; Gladyshev, V.N.; Hatfield, D.L. Biosynthesis of selenocysteine, the 21st amino acid in the genetic code, and a novel pathway for cysteine biosynthesis. Adv. Nutr. 2011, 2, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.L.; Simonović, M. Synthesis and decoding of selenocysteine and human health. Croat. Med. J. 2012, 53, 535–550. [Google Scholar] [CrossRef] [PubMed]
- Labunskyy, V.M.; Hatfield, D.L.; Gladyshev, V.N. Selenoproteins: Molecular pathways and physiological roles. Physiol. Rev. 2014, 94, 739–777. [Google Scholar] [CrossRef]
- Kim, J.; Chung, H.S.; Choi, M.-K.; Roh, Y.K.; Yoo, H.J.; Park, J.H.; Kim, D.S.; Yu, J.M.; Moon, S. Association between Serum Selenium Level and the Presence of Diabetes Mellitus: A Meta-Analysis of Observational Studies. Diabetes Metab. J. 2019, 43, e1. [Google Scholar] [CrossRef] [PubMed]
- Lewicka, I.; Kocyłowski, R.; Grzesiak, M.; Gaj, Z.; Oszukowski, P.; Suliburska, J. Selected trace elements concentrations in pregnancy and their possible role—Literature review. Ginekol. Pol. 2017, 88, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, M.; Cvetkovic, M.; Ljubic, A.; Kosanovic, M.; Nedeljkovic, S.; Jovanovic, I.; Pesut, O. Selenium and malondialdehyde content and glutathione peroxidase activity in maternal and umbilical cord blood and amniotic fluid. Biol. Trace Elem. Res. 2000, 73, 47–54. [Google Scholar] [CrossRef]
- Mistry, H.D.; Broughton Pipkin, F.; Redman, C.W.; Poston, L. Selenium in reproductive health. Am. J. Obstet. Gynecol. 2012, 206, 21–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cengiz, B.; Soylemez, F.; Ozturk, E.; Cavdar, A.O. Serum zinc, selenium, copper, and lead levels in women with second-trimester induced abortion resulting from neural tube defects: A preliminary study. Biol. Trace Elem. Res. 2004, 97, 225–235. [Google Scholar] [CrossRef]
- Zachara, B.A. Chapter Five-Selenium in Complicated Pregnancy. A Review. Adv. Clin. Chem. 2018, 86, 157–178. [Google Scholar]
- Zhou, J.; Huang, K.; Lei, X.G. Selenium and diabetes-evidence from animal studies. Free Radic. Biol. Med. 2013, 65, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.C.; Combs, G.F.; Turnbull, B.W.; Slate, E.H.; Chalker, D.K.; Chow, J.; Davis, L.S.; Glover, R.A.; Graham, G.F.; Gross, E.G.; et al. Effects of selenium supplementation for cancer prevention in patients with carcinoma of the skin. A randomized controlled trial. Nutritional Prevention of Cancer Study Group. JAMA 1996, 276, 1957–1963. [Google Scholar] [CrossRef] [PubMed]
- Stranges, S.; Marshall, J.R.; Natarajan, R.; Donahue, R.P.; Trevisan, M.; Combs, G.F.; Cappuccio, F.P.; Ceriello, A.; Reid, M.E. Effects of long-term selenium supplementation on the incidence of type 2 diabetes: A randomized trial. Ann. Intern. Med. 2007, 147, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Lippman, S.M.; Klein, E.A.; Goodman, P.J.; Lucia, M.S.; Thompson, I.M.; Ford, L.G.; Parnes, H.L.; Minasian, L.M.; Gaziano, J.M.; Hartline, J.A.; et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2009, 301, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Ashbeck, E.L.; Roe, D.J.; Fales, L.; Buckmeier, J.; Wang, F.; Bhattacharyya, A.; Hsu, C.H.; Chow, H.H.; Ahnen, D.J.; et al. Selenium Supplementation for Prevention of Colorectal Adenomas and Risk of Associated Type 2 Diabetes. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef]
- Wang, X.-L.; Yang, T.-B.; Wei, J.; Lei, G.-H.; Zeng, C. Association between serum selenium level and type 2 diabetes mellitus: A non-linear dose-response meta-analysis of observational studies. Nutr. J. 2016, 15, 48. [Google Scholar] [CrossRef]
- Benstoem, C.; Goetzenich, A.; Kraemer, S.; Borosch, S.; Manzanares, W.; Hardy, G.; Stoppe, C. Selenium and its supplementation in cardiovascular disease—What do we know? Nutrients 2015, 7, 3094–3118. [Google Scholar] [CrossRef]
- Thomson, C.D. Assessment of requirements for selenium and adequacy of selenium status: A review. Eur. J. Clin. Nutr. 2004, 58, 391–402. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, C.; Guo, J.; Song, Y. Selenium status and cardiovascular diseases: Meta-analysis of prospective observational studies and randomized controlled trials. Eur. J. Clin. Nutr. 2016, 70, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.W.; Mo, H.-Y.; Lau, A.T.Y.; Xu, Y.-M. Selenium Species: Current Status and Potentials in Cancer Prevention and Therapy. Int. J. Mol. Sci. 2018, 20, 75. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, D.L.; Tsuji, P.A.; Carlson, B.A.; Gladyshev, V.N. Selenium and selenocysteine: Roles in cancer, health, and development. Trends Biochem. Sci. 2014, 39, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Dreno, B.; Euvrard, S.; Frances, C.; Moyse, D.; Nandeuil, A. Effect of selenium intake on the prevention of cutaneous epithelial lesions in organ transplant recipients. Eur. J. Dermatol. EJD 2007, 17, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Karp, D.D.; Lee, S.J.; Keller, S.M.; Wright, G.S.; Aisner, S.; Belinsky, S.A.; Johnson, D.H.; Johnston, M.R.; Goodman, G.; Clamon, G.; et al. Randomized, double-blind, placebo-controlled, phase III chemoprevention trial of selenium supplementation in patients with resected stage I non-small-cell lung cancer: ECOG 5597. J. Clin. Oncol. 2013, 31, 4179–4187. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.R.; Tangen, C.M.; Sakr, W.A.; Wood, D.P.; Berry, D.L.; Klein, E.A.; Lippman, S.M.; Parnes, H.L.; Alberts, D.S.; Jarrard, D.F.; et al. Phase III trial of selenium to prevent prostate cancer in men with high-grade prostatic intraepithelial neoplasia: SWOG S9917. Cancer Prev. Res. 2011, 4, 1761–1769. [Google Scholar] [CrossRef]
- Algotar, A.M.; Stratton, M.S.; Ahmann, F.R.; Ranger-Moore, J.; Nagle, R.B.; Thompson, P.A.; Slate, E.; Hsu, C.H.; Dalkin, B.L.; Sindhwani, P.; et al. Phase 3 clinical trial investigating the effect of selenium supplementation in men at high-risk for prostate cancer. Prostate 2013, 73, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Lubinski, J.; Jaworska, K.; Durda, K.; Jakubowska, A.; Huzarski, T.; Byrski, T.; Stawicka, M.; Gronwald, J.; Górski, B.; Wasowicz, W.; et al. Selenium and the risk of cancer in BRCA1 carriers. Hered. Cancer Clin. Pract. 2011, 9, A5. [Google Scholar] [CrossRef]
- Vinceti, M.; Filippini, T.; Del Giovane, C.; Dennert, G.; Zwahlen, M.; Brinkman, M.; Zeegers, M.P.; Horneber, M.; D’Amico, R.; Crespi, C.M. Selenium for preventing cancer. Cochrane Database Syst. Rev. 2018, 1, CD005195. [Google Scholar] [CrossRef]
- Yanardag, R.; Orak, H. Selenium content of milk and milk products of Turkey. II. Biol. Trace Elem. Res. 1999, 68, 79–95. [Google Scholar] [CrossRef]
- Ayar, A.; Sert, D.; Akin, N. The trace metal levels in milk and dairy products consumed in middle Anatolia-Turkey. Environ. Monit. Assess. 2009, 152, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hincal, F. Trace elements in growth: Iodine and selenium status of Turkish children. J. Trace Elem. Med. Biol. 2007, 21, 40–43. [Google Scholar] [CrossRef]
- Erkekoglu, P.; Asci, A.; Ceyhan, M.; Kizilgun, M.; Schweizer, U.; Atas, C.; Kara, A.; Kocer Giray, B. Selenium levels, selenoenzyme activities and oxidant/antioxidant parameters in H1N1-infected children. Turk. J. Pediatr. 2013, 55, 271–282. [Google Scholar] [PubMed]
- Eroglu, M.; Sahin, S.; Durukan, B.; Ozakpinar, O.B.; Erdinc, N.; Turkgeldi, L.; Sofuoglu, K.; Karateke, A. Blood serum and seminal plasma selenium, total antioxidant capacity and coenzyme q10 levels in relation to semen parameters in men with idiopathic infertility. Biol. Trace Elem. Res. 2014, 159, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, H.S.; Karadas, F.; Pappas, A.C.; Cassey, P.; Oto, G.; Tuncer, O. The selenium levels of mothers and their neonates using hair, breast milk, meconium, and maternal and umbilical cord blood in Van Basin. Biol. Trace Elem. Res. 2008, 122, 206–215. [Google Scholar] [CrossRef]
- Hincal, F.; Basaran, N.; Yetgin, S.; Gokmen, O. Selenium status in Turkey. II. Serum selenium concentration in healthy residents of different ages in Ankara. J. Trace Elem. Electrol. Health Dis. 1994, 8, 9–12. [Google Scholar]
- Kilinc, M.; Guven, M.A.; Ezer, M.; Ertas, I.E.; Coskun, A. Evaluation of serum selenium levels in Turkish women with gestational diabetes mellitus, glucose intolerants, and normal controls. Biol. Trace Elem. Res. 2008, 123, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Seven, M.; Basaran, S.Y.; Cengiz, M.; Unal, S.; Yuksel, A. Deficiency of selenium and zinc as a causative factor for idiopathic intractable epilepsy. Epilepsy Res. 2013, 104, 35–39. [Google Scholar] [CrossRef]
- Bay, A.; Dogan, M.; Bulan, K.; Kaba, S.; Demir, N.; Oner, A.F. A study on the effects of pica and iron-deficiency anemia on oxidative stress, antioxidant capacity and trace elements. Hum. Exp. Toxicol. 2013, 32, 895–903. [Google Scholar] [CrossRef]
- Coskun, A.; Arikan, T.; Kilinc, M.; Arikan, D.C.; Ekerbicer, H.C. Plasma selenium levels in Turkish women with polycystic ovary syndrome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 168, 183–186. [Google Scholar] [CrossRef]
- Arikan, D.C.; Coskun, A.; Ozer, A.; Kilinc, M.; Atalay, F.; Arikan, T. Plasma selenium, zinc, copper and lipid levels in postmenopausal Turkish women and their relation with osteoporosis. Biol. Trace Elem. Res. 2011, 144, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Sakiz, D.; Kaya, A.; Kulaksizoglu, M. Serum Selenium Levels in Euthyroid Nodular Thyroid Diseases. Biol. Trace Elem. Res. 2016, 174, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Arikan, T.A. Plasma Selenium Levels in First Trimester Pregnant Women with Hyperthyroidism and the Relationship with Thyroid Hormone Status. Biol. Trace Elem. Res. 2015, 167, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Aydemir, B.; Akdemir, R.; Vatan, M.B.; Cinemre, F.B.; Cinemre, H.; Kiziler, A.R.; Bahtiyar, N.; Buyukokuroglu, M.E.; Gurol, G.; Ogut, S. The Circulating Levels of Selenium, Zinc, Midkine, Some Inflammatory Cytokines, and Angiogenic Factors in Mitral Chordae Tendineae Rupture. Biol. Trace Elem. Res. 2015, 167, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Kuisi, M.A.; Abdel-Fattah, A. Groundwater vulnerability to selenium in semi-arid environments: Amman Zarqa Basin, Jordan. Environ. Geochem. Health 2010, 32, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Arafa, M.A.; Waly, M.I.; Jriesat, S.; Al Khafajei, A.; Sallam, S. Dietary and lifestyle characteristics of colorectal cancer in Jordan: A case-control study. Asian Pac. J. Cancer Prev. 2011, 12, 1931–1936. [Google Scholar] [PubMed]
- Massadeh, A.; Gharibeh, A.; Omari, K.; Al-Momani, I.; Alomary, A.; Tumah, H.; Hayajneh, W. Simultaneous determination of Cd, Pb, Cu, Zn, and Se in human blood of jordanian smokers by ICP-OES. Biol. Trace Elem. Res. 2010, 133, 1–11. [Google Scholar] [CrossRef]
- Alqhazo, M.; Rashaid, A.B. The concentrations of bioelements in the hair samples of Jordanian children who stutter. Int. J. Pediatr. Otorhinolaryngol. 2018, 112, 158–162. [Google Scholar] [CrossRef]
- Mirzaeian, S.; Ghiasvand, R.; Sadeghian, F.; Sheikhi, M.; Khosravi, Z.S.; Askari, G.; Shiranian, A.; Yadegarfar, G. Assessing the micronutrient and macronutrient intakes in female students and comparing them with the set standard values. J. Educ. Health Promot. 2013, 2, 1. [Google Scholar] [CrossRef]
- Darvishi, L.; Ghiasvand, R.; Ashrafi, M.; Ashrafzadeh, E.; Askari, G.; Shiranian, A.; Hasanzadeh, A. Relationship between junk foods intake and weight in 6–7 years old children, Shahin Shahr and Meymeh, Iran. J. Educ. Health Promot. 2013, 2, 2. [Google Scholar] [CrossRef]
- Mansour, A.; Ahadi, Z.; Qorbani, M.; Hosseini, S. Association between dietary intake and seasonal variations in postmenopausal women. J. Diabetes Metab. Disord. 2014, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Rahimzadeh-Barzoki, H.; Joshaghani, H.; Beirami, S.; Mansurian, M.; Semnani, S.; Roshandel, G. Selenium levels in rice samples from high and low risk areas for esophageal cancer. Saudi Med. J. 2014, 35, 617–620. [Google Scholar] [PubMed]
- Safaralizadeh, R.; Kardar, G.A.; Pourpak, Z.; Moin, M.; Zare, A.; Teimourian, S. Serum concentration of selenium in healthy individuals living in Tehran. Nutr. J. 2005, 4, 32. [Google Scholar] [CrossRef] [PubMed]
- Safaralizadeh, R.; Sirjani, M.; Pourpak, Z.; Kardar, G.; Teimourian, S.; Shams, S.; Namdar, Z.; Kazemnejad, A.; Moin, M. Serum selenium concentration in healthy children living in Tehran. Biofactors 2007, 31, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Dabbaghmanesh, M.H.; Sadegholvaad, A.; Ejtehadi, F.; Omrani, G. Low serum selenium concentration as a possible factor for persistent goiter in Iranian school children. Biofactors 2007, 29, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Farzin, L.; Moassesi, M.E.; Sajadi, F.; Amiri, M.; Shams, H. Serum levels of antioxidants (Zn, Cu, Se) in healthy volunteers living in Tehran. Biol. Trace Elem. Res. 2009, 129, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Farzin, L.; Sajadi, F. Comparison of serum trace element levels in patients with or without pre-eclampsia. J. Res. Med. Sci. 2012, 17, 938–941. [Google Scholar] [PubMed]
- Farzin, L.; Moassesi, M.E. A comparison of serum selenium, zinc and copper level in visceral and cutaneous leishmaniasis. J. Res. Med. Sci. 2014, 19, 355–357. [Google Scholar]
- Parizadeh, S.M.; Moohebati, M.; Ghafoori, F.; Ghayour-Mobarhan, M.; Kazemi-Bajestani, S.M.; Tavallaie, S.; Azimi-Nezhad, M.; Ferns, G.A. Serum selenium and glutathione peroxidase concentrations in Iranian patients with angiography-defined coronary artery disease. Angiology 2009, 60, 186–191. [Google Scholar] [CrossRef]
- Rafraf, M.; Mahdavi, R.; Rashidi, M.R. Serum selenium levels in healthy women in Tabriz, Iran. Food Nutr. Bull. 2008, 29, 83–86. [Google Scholar] [CrossRef]
- Tara, F.; Rayman, M.P.; Boskabadi, H.; Ghayour-Mobarhan, M.; Sahebkar, A.; Yazarlu, O.; Ouladan, S.; Tavallaie, S.; Azimi-Nezhad, M.; Shakeri, M.T.; et al. Selenium supplementation and premature (pre-labour) rupture of membranes: A randomised double-blind placebo-controlled trial. J. Obstet. Gynaecol. 2010, 30, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Mahyar, A.; Ayazi, P.; Fallahi, M.; Javadi, A. Correlation between serum selenium level and febrile seizures. Pediatric Neurol. 2010, 43, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Esalatmanesh, K.; Jamshidi, A.; Shahram, F.; Davatchi, F.; Masoud, S.A.; Soleimani, Z.; Salesi, M.; Ghaffarpasand, I. Study of the correlation of serum selenium level with Behcet’s disease. Int. J. Rheum. Dis. 2011, 14, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Ghaemian, A.; Salehifar, E.; Shiraj, H.; Babaee, Z. A Comparison of Selenium Concentrations between Congestive Heart Failure Patients and Healthy Volunteers. J. Tehran Heart Cent. 2012, 7, 53–57. [Google Scholar] [PubMed]
- Ghaemi, S.Z.; Forouhari, S.; Dabbaghmanesh, M.H.; Sayadi, M.; Bakhshayeshkaram, M.; Vaziri, F.; Tavana, Z. A prospective study of selenium concentration and risk of preeclampsia in pregnant Iranian women: A nested case-control study. Biol. Trace Elem. Res. 2013, 152, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Maleki, A.; Fard, M.K.; Zadeh, D.H.; Mamegani, M.A.; Abasaizadeh, S.; Mazloomzadeh, S. The relationship between plasma level of Se and preeclampsia. Hypertens. Pregnancy 2011, 30, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, I.A.; Al-Jaloud, A.; Al-Doush, I.; El-Din, G. The distribution of selenium levels in Saudi dairy farms: A preliminary report from Al-Kharj. J. Environ. Pathol. Toxicol. Oncol. Off. Organ Int. Soc. Environ. Toxicol. Cancer 1999, 18, 37–46. [Google Scholar]
- Al-Ahmary, K.M. Selenium content in selected foods from the Saudi Arabia market and estimation of the daily intake. Arab. J. Chem. 2009, 2, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Al-Othman, A.M.; Al-Othman, Z.A.; El-Desoky, G.E.; Aboul-Soud, M.A.; Habila, M.A.; Giesy, J.P. Daily intake of selenium and concentrations in blood of residents of Riyadh City, Saudi Arabia. Environ. Geochem. Health 2012, 34, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, I.; Al-Doush, I. Selenium levels in infant milk formula. Biometals Int. J. Role Met. Ions Biol. Biochem. Med. 1997, 10, 299–302. [Google Scholar] [CrossRef]
- Al-Saleh, I.; Al-Doush, I.; Faris, R. Selenium levels in breast milk and cow’s milk: A preliminary report from Saudi Arabia. J. Environ. Pathol. Toxicol. Oncol. Off. Organ Int. Soc. Environ. Toxicol. Cancer 1997, 16, 41–46. [Google Scholar]
- Al-Saleh, I.; El-Doush, I.; Billedo, G.; Mohamed Gel, D.; Yosef, G. Status of selenium, vitamin E, and vitamin A among Saudi adults: Potential links with common endemic diseases. J. Environ. Pathol. Toxicol. Oncol. Off. Organ Int. Soc. Environ. Toxicol. Cancer 2007, 26, 221–243. [Google Scholar] [CrossRef]
- Al-Saleh, I.; Billedo, G. Determination of selenium concentration in serum and toenail as an indicator of selenium status. Bull. Environ. Contam. Toxicol. 2006, 77, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, I.; Al-Doush, I.; Ibrahim, M.; Rabbah, A. Serum selenium levels in Saudi new-borns. Int. J. Environ. Health Res. 1998, 8, 269–275. [Google Scholar] [CrossRef]
- Al-Saleh, I.; Billedo, G.; El-Doush, I.; El-Din Mohamed, G.; Yosef, G. Selenium and vitamins status in Saudi children. Clin. Chim. Acta Int. J. Clin. Chem. 2006, 368, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, E.; Nandakumaran, M.; Al-Rashdan, I.; Al-Harmi, J.; Al-Shammari, M. Maternal-foetal status of copper, iron, molybdenum, selenium and zinc in obese gestational diabetic pregnancies. Acta Diabetol. 2007, 44, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Alissa, E.M.; Ahmed, W.H.; Al-ama, N.; Ferns, G.A. Selenium status and cardiovascular risk profile in healthy adult Saudi males. Molecules 2008, 14, 141–159. [Google Scholar] [CrossRef] [PubMed]
- El-Yazigi, A.; Legayada, E. Urinary selenium in healthy and diabetic Saudi Arabians. Biol. Trace Elem. Res. 1996, 52, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Ghneim, H.K.; Alshebly, M.M. Biochemical Markers of Oxidative Stress in Saudi Women with Recurrent Miscarriage. J. Korean Med. Sci. 2016, 31, 98–105. [Google Scholar] [CrossRef] [Green Version]
- El-Ansary, A.; Bjorklund, G.; Tinkov, A.A.; Skalny, A.V.; Al Dera, H. Relationship between selenium, lead, and mercury in red blood cells of Saudi autistic children. Metab. Brain Dis. 2017, 32, 1073–1080. [Google Scholar] [CrossRef]
- Meguid, N.A.; Anwar, M.; Bjorklund, G.; Hashish, A.; Chirumbolo, S.; Hemimi, M.; Sultan, E. Dietary adequacy of Egyptian children with autism spectrum disorder compared to healthy developing children. Metab. Brain Dis. 2017, 32, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Saad, K.; Farghaly, H.S.; Badry, R.; Othman, H.A. Selenium and antioxidant levels decreased in blood of children with breath-holding spells. J. Child Neurol. 2014, 29, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Sherief, L.M.; Abd El-Salam, S.M.; Kamal, N.M.; El safy, O.; Almalky, M.A.A.; Azab, S.F.; Morsy, H.M.; Gharieb, A.F. Nutritional Biomarkers in Children and Adolescents with Beta-Thalassemia-Major: An Egyptian Center Experience. BioMed Res. Int. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Azab, S.F.A.; Saleh, S.H.; Elsaeed, W.F.; Elshafie, M.A.; Sherief, L.M.; Esh, A.M.H. Serum trace elements in obese Egyptian children: A case-control study. Ital. J. Pediatr. 2014, 40, 20. [Google Scholar] [CrossRef] [PubMed]
- El-Mazary, A.-A.M.; Abdel-Aziz, R.A.; Mahmoud, R.A.; El-Said, M.A.; Mohammed, N.R. Correlations between maternal and neonatal serum selenium levels in full term neonates with hypoxic ischemic encephalopathy. Ital. J. Pediatr. 2015, 41, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qatar General Electricity & Water Corporation (Kahramaa). Overview on: Kahramaa Drinking Water Quality Requirement; Kahramaa Publications: Doha, Qatar, 2014. [Google Scholar]
- Rowell, C.; Kuiper, N.; Al-Saad, K.; Nriagu, J.; Shomar, B. A market basket survey of As, Zn and Se in rice imports in Qatar: Health implications. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2014, 70, 33–39. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Selenoprotein | Symbol | Function and Significance |
|---|---|---|
| Glutathione peroxidase 1 | GPX1 | Reduces cellular H2O2. Overexpression of GPX1 increases risk of diabetes. |
| Glutathione peroxidase 2 | GPX2 | Reduces peroxide in gut. GPX1/GPX2 double-knockout mice develop intestinal cancer; one allele of GPX2 added back confers protection. |
| Glutathione peroxidase 3 | GPX3 | Reduces peroxide in blood. Important for cardiovascular protection, perhaps through modulation of nitric oxide levels; antioxidant in thyroid gland. |
| Glutathione peroxidase 4 | GPX4 | Reduces phospholipid peroxide. Genetic deletion is embryonic lethal; GPX4 acts as crucial antioxidant, and sensor of oxidative stress and pro-apoptotic signals; required for spermatozoa function. |
| Glutathione peroxidase 6 | GPX6 | Importance unknown. |
| Iodothyronine deiodinase 1 | DIO1 | Important for systemic active thyroid hormone levels. |
| Iodothyronine deiodinase 2 | DIO2 | Important for local active thyroid hormone levels. |
| Iodothyronine deiodinase 3 | DIO3 | Inactivates thyroid hormone. |
| Thioredoxin reductase 1 | TXNRD1 | Reduction of cytosolic thioredoxin. Genetic deletion is embryonic lethal. |
| Thioredoxin reductase 2 | TXNRD2 | Reduction of mitochondrial thioredoxin. Genetic deletion is embryonic lethal. |
| Thioredoxin-glutathione reductase | TXNRD3 | Reduction of thioredoxin, testes-specific expression. |
| Selenoprotein H | SELENOH | Involved in transcription. Essential for cell survival and antioxidant defense in Drosophila. |
| Selenoprotein I | SELENOI | Possibly involved in phospholipid biosynthesis. |
| Selenoprotein K | SELENOK | Involved in calcium flux in immune cells and endoplasmic reticulum (ER)-associated degradation. |
| Selenoprotein M | SELENOM | Thiol-disulfide oxidoreductase localized in the ER. Possibly involved in protein folding. |
| Selenoprotein F | SELENOF | Thiol-disulfide oxidoreductase localized in the ER. Possibly involved in protein folding. |
| Selenoprotein N | SELENON | Potential role in early muscle development. Mutations lead to multiminicore disease and other myopathies. |
| Selenoprotein O | SELENOO | Potential redox function, but importance remains unknown. |
| Selenoprotein P | SELENOP | Se transport to tissues particularly brain and testis. It also functions as intracellular antioxidant in phagocytes. Knockout leads to neurological problems and male sterility. |
| Methionine-R-sulfoxide reductase 1 | MSRB1 | Functions as a methionine sulfoxide reductase and MSRB1 knockouts show mild damage to oxidative insult. |
| Selenoprotein S | SELENOS | Transmembrane protein found in plasma membrane and ER. Reduces ER stress. |
| Selenoprotein T | SELENOT | ER protein involved in calcium mobilization. |
| Selenoprotein V | SELENOV | Testes-specific expression, potential role in male reproduction. |
| Selenoprotein W | SELENOW | Potential antioxidant role, perhaps important in muscle growth. |
| Selenophosphate synthetase 2 | SEPHS2 | Involved in the synthesis of all selenoproteins. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, S.A.Z.; Kerkadi, A.; Agouni, A. Selenium and Health: An Update on the Situation in the Middle East and North Africa. Nutrients 2019, 11, 1457. https://doi.org/10.3390/nu11071457
Ibrahim SAZ, Kerkadi A, Agouni A. Selenium and Health: An Update on the Situation in the Middle East and North Africa. Nutrients. 2019; 11(7):1457. https://doi.org/10.3390/nu11071457
Chicago/Turabian StyleIbrahim, Sohayla A. Z., Abdelhamid Kerkadi, and Abdelali Agouni. 2019. "Selenium and Health: An Update on the Situation in the Middle East and North Africa" Nutrients 11, no. 7: 1457. https://doi.org/10.3390/nu11071457
APA StyleIbrahim, S. A. Z., Kerkadi, A., & Agouni, A. (2019). Selenium and Health: An Update on the Situation in the Middle East and North Africa. Nutrients, 11(7), 1457. https://doi.org/10.3390/nu11071457