Longitudinal Changes of Mineral Concentrations in Preterm and Term Human Milk from Lactating Swiss Women

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Data Collection
2.3. Human Milk Sampling and Processing
2.4. Mineral Quantification
2.5. Statistics
3. Results
3.1. General Characteristics of the Subjects
3.2. Mineral Concentration and Longitudinal Change in Preterm and Term Human Milk at the Same Postpartum Age
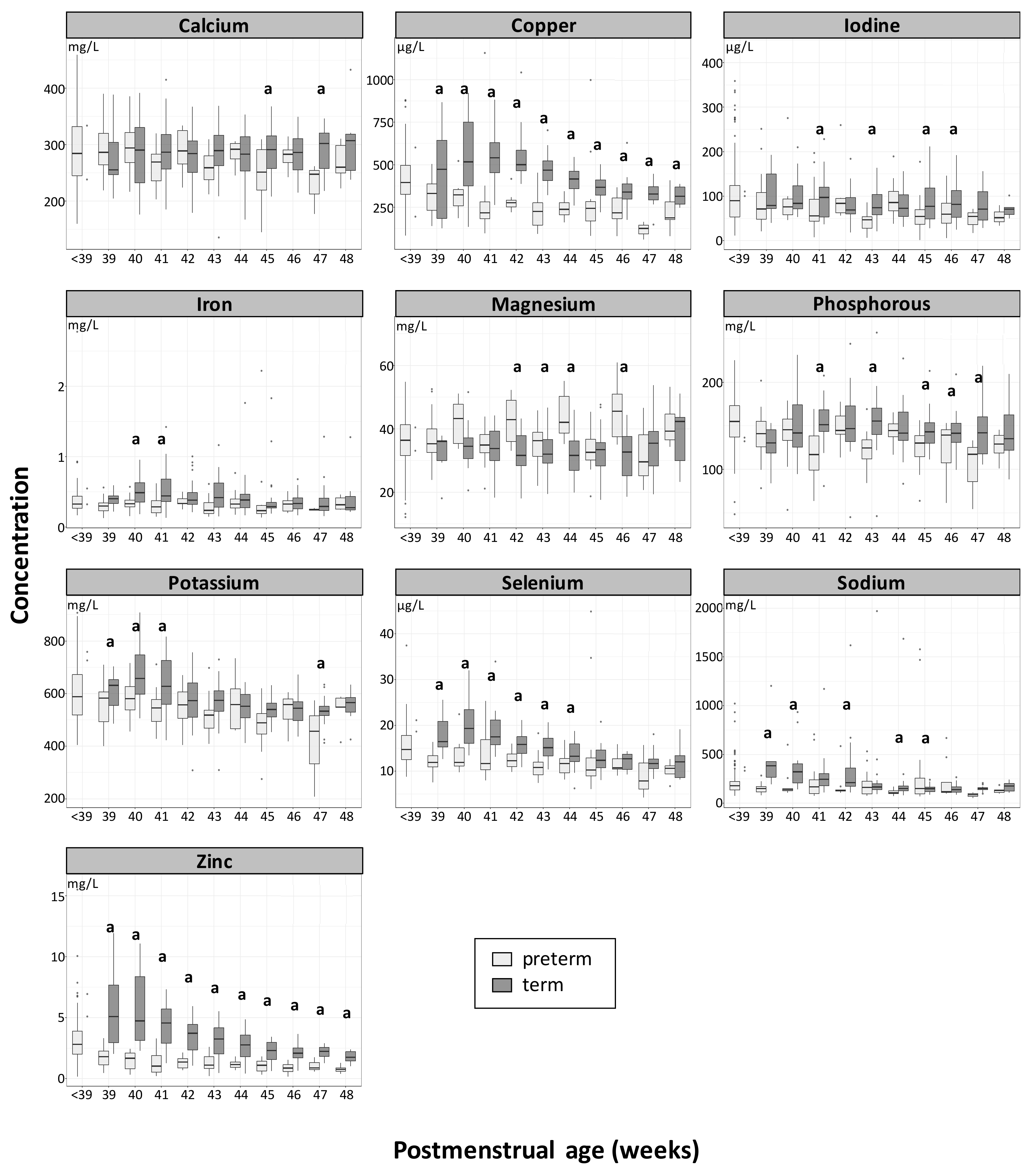
3.3. Longitudinal Changes of Mineral Concentration in Term and Preterm Human Milk at an Equivalent Postmenstrual Age
4. Discussion
4.1. Mineral Concentration and Longitudinal Change in Preterm and Term Human Milk at the Same Postpartum Age
4.2. Longitudinal Changes of Mineral Concentration in Term and Preterm Human Milk at an Equivalent Postmenstrual Age
4.3. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- March of Dimes; PMNCH; Save the Children; WHO. Born Too Soon: The Global Action Report on Preterm Birth; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Finch, C.W. Review of trace mineral requirements for preterm infants: What are the current recommendations for clinical practice? Nutr. Clin. Pract. 2015, 30, 44–58. [Google Scholar] [CrossRef] [PubMed]
- Aggett, P.J.; Agostoni, C.; Axelsson, I.; De Curtis, M.; Goulet, O.; Hernell, O.; Koletzko, B.; Lafeber, H.N.; Michaelsen, K.F.; Puntis, J.W.; et al. Feeding preterm infants after hospital discharge: A commentary by the espghan committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Ramel, S.E.; Georgieff, M.K. Preterm nutrition and the brain. World Rev. Nutr. Diet. 2014, 110, 190–200. [Google Scholar] [PubMed]
- Mimouni, F.B.; Mandel, D.; Lubetzky, R.; Senterre, T. Calcium, phosphorus, magnesium and vitamin d requirements of the preterm infant. World Rev. Nutr. Diet. 2014, 110, 140–151. [Google Scholar] [PubMed]
- Fusch, C.; Jochum, F. Water, sodium, potassium and chloride. World Rev. Nutr. Diet. 2014, 110, 99–120. [Google Scholar] [PubMed]
- Patel, P.; Bhatia, J. Human milk: The prefered firts food for premature infants. J. Hum. Nutr. Food Sci. 2016, 4. [Google Scholar]
- Tudehope, D.I. Human milk and the nutritional needs of preterm infants. J. Pediatr. 2013, 162, S17–S25. [Google Scholar] [CrossRef]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellof, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral nutrient supply for preterm infants: Commentary from the european society of paediatric gastroenterology, hepatology and nutrition committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Boquien, C.Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of human milk for preterm infants: Update and recommendations of the european milk bank association (emba) working group on human milk fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef]
- van de Lagemaat, M.; Rotteveel, J.; van Weissenbruch, M.M.; Lafeber, H.N. Increased gain in bone mineral content of preterm infants fed an isocaloric, protein-, and mineral-enriched postdischarge formula. Eur. J. Nutr. 2013, 52, 1781–1785. [Google Scholar] [CrossRef]
- Dror, D.K.; Allen, L.H. Overview of nutrients in human milk. Adv. Nutr. 2018, 9, 278S–294S. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Rodenas, C.L.; De Castro, C.A.; Jenni, R.; Thakkar, S.K.; Beauport, L.; Tolsa, J.F.; Fischer-Fumeaux, C.J.; Affolter, M. Temporal changes of major protein concentrations in preterm and term human milk. A prospective cohort study. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Fischer Fumeaux, C.J.; Garcia-Rodenas, C.L.; De Castro, C.A.; Courtet-Compondu, M.C.; Thakkar, S.K.; Beauport, L.; Tolsa, J.F.; Affolter, M. Longitudinal analysis of macronutrient composition in preterm and term human milk: A prospective cohort study. Nutrients 2019, 11, 1525. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, S.K.; De Castro, C.A.; Beauport, L.; Tolsa, J.F.; Fischer Fumeaux, C.J.; Affolter, M.; Giuffrida, F. Temporal progression of fatty acids in preterm and term human milk of mothers from switzerland. Nutrients 2019, 11, 112. [Google Scholar] [CrossRef] [PubMed]
- Austin, S.; De Castro, C.A.; Sprenger, N.; Binia, A.; Affolter, M.; Garcia-Rodenas, C.L.; Beauport, L. Human milk oligosaccharides in the milk of mothers delivering term versus preterm infants. Nutrients 2019, 11, 1282. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Gerss, J. Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants. Clin. Nutr. 2011, 30, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Gross, S.J.; David, R.J.; Bauman, L.; Tomarelli, R.M. Nutritional composition of milk produced by mothers delivering preterm. J. Pediatr. 1980, 96, 641–644. [Google Scholar] [CrossRef]
- Dorea, J.G. Breast milk calcium and phosphorus concentrations. Nutrition 2000, 16, 146–147. [Google Scholar] [CrossRef]
- Salamon, S.; Csapó, J. Composition of mother’s milk iii. Macroand microelements contents. A review. Acta Univ. Sapiente. Alimentaria 2009, 2, 235–275. [Google Scholar]
- Dorea, J.G. Magnesium in human milk. J. Am. Coll. Nutr. 2000, 19, 210–219. [Google Scholar] [CrossRef]
- Dorea, J.G. Zinc and copper concentrations in breastmilk. Indian Pediatr. 2012, 49, 592. [Google Scholar] [CrossRef] [PubMed]
- Dorea, J.G. Iron and copper in human milk. Nutrition 2000, 16, 209–220. [Google Scholar] [CrossRef]
- Dorea, J.G. Iodine nutrition and breast feeding. J. Trace Elem. Med. Biol. 2002, 16, 207–220. [Google Scholar] [CrossRef]
- Kim, S.Y.; Park, J.H.; Kim, E.A.; Lee-Kim, Y.C. Longitudinal study on trace mineral compositions (selenium, zinc, copper, manganese) in korean human preterm milk. J. Korean Med. Sci. 2012, 27, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.; Picciano, M.F.; Smith, A.M.; Hamosh, M.; Mehta, N.R. The impact of gestational length on human milk selenium concentration and glutathione peroxidase activity. Pediatr. Res. 1990, 27, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Saini, S.; Prasad, R. Changes in preterm human milk composition with particular reference to introduction of mixed feeding. Indian Pediatr. 2014, 51, 997–999. [Google Scholar] [CrossRef]
- Lemons, J.A.; Moye, L.; Hall, D.; Simmons, M. Differences in the composition of preterm and term human milk during early lactation. Pediatr. Res. 1982, 16, 113–117. [Google Scholar] [CrossRef]
- Picciano, M.F.; Guthrie, H.A. Copper, iron, and zinc contents of mature human milk. Am. J. Clin. Nutr. 1976, 29, 242–254. [Google Scholar] [CrossRef] [Green Version]
- Zhao, A.; Ning, Y.; Zhang, Y.; Yang, X.; Wang, J.; Li, W.; Wang, P. Mineral compositions in breast milk of healthy chinese lactating women in urban areas and its associated factors. Chin. Med. J. (Engl.) 2014, 127, 2643–2648. [Google Scholar]
- Ereman, R.R.; Lonnerdal, B.; Dewey, K.G. Maternal sodium intake does not affect postprandial sodium concentrations in human milk. J. Nutr. 1987, 117, 1154–1157. [Google Scholar] [CrossRef]
- Finley, D.A.; Lonnerdal, B.; Dewey, K.G.; Grivetti, L.E. Inorganic constituents of breast milk from vegetarian and nonvegetarian women: Relationships with each other and with organic constituents. J. Nutr. 1985, 115, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Schupbach, R.; Wegmuller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M. Oligoéléments en suisse et en europe. Rev. Med. Suisse 2012, 8, 2078–2084. [Google Scholar] [PubMed]
- Atkinson, S.A.; Radde, I.C.; Chance, G.W.; Bryan, M.H.; Anderson, G.H. Macro-mineral content of milk obtained during early lactation from mothers of premature infants. Early Hum. Dev. 1980, 4, 5–14. [Google Scholar] [CrossRef]
- Grumach, A.S.; Jeronimo, S.E.; Hage, M.; Carneiro-Sampaio, M.M. Nutritional factors in milk from brazilian mothers delivering small for gestational age neonates. Rev. Saude Publica 1993, 27, 455–462. [Google Scholar] [CrossRef] [PubMed]
- De Figueiredo, C.S.; Palhares, D.B.; Melnikov, P.; Moura, A.J.; dos Santos, S.C. Zinc and copper concentrations in human preterm milk. Biol. Trace Elem. Res. 2010, 136, 1–7. [Google Scholar] [CrossRef]
- Fernandez-Menendez, S.; Fernandez-Sanchez, M.L.; Fernandez-Colomer, B.; de la Flor St Remy, R.R.; Cotallo, G.D.; Freire, A.S.; Braz, B.F.; Santelli, R.E.; Sanz-Medel, A. Total zinc quantification by inductively coupled plasma-mass spectrometry and its speciation by size exclusion chromatography-inductively coupled plasma-mass spectrometry in human milk and commercial formulas: Importance in infant nutrition. J. Chromatogr. A. 2016, 1428, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Ares, S.; Quero, J.; Duran, S.; Presas, M.J.; Herruzo, R.; Morreale de Escobar, G. Iodine content of infant formulas and iodine intake of premature babies: High risk of iodine deficiency. Arch Dis. Child. Fetal Neonatal Ed. 1994, 71, F184–F191. [Google Scholar] [CrossRef]
- Hunt, C.D.; Friel, J.K.; Johnson, L.K. Boron concentrations in milk from mothers of full-term and premature infants. Am. J. Clin. Nutr. 2004, 80, 1327–1333. [Google Scholar] [CrossRef]
- Atinmo, T.; Omololu, A. Trace element content of breastmilk from mothers of preterm infants in nigeria. Early Hum. Dev. 1982, 6, 309–313. [Google Scholar] [CrossRef]
- Perrone, L.; Di Palma, L.; Di Toro, R.; Gialanella, G.; Moro, R. Interaction of trace elements in a longitudinal study of human milk from full-term and preterm mothers. Biol. Trace Elem. Res. 1994, 41, 321–330. [Google Scholar] [CrossRef]
- Trugo, N.M.; Donangelo, C.M.; Koury, J.C.; Silva, M.I.; Freitas, L.A. Concentration and distribution pattern of selected micronutrients in preterm and term milk from urban brazilian mothers during early lactation. Eur. J. Clin. Nutr. 1988, 42, 497–507. [Google Scholar]
- Mendelson, R.A.; Anderson, G.H.; Bryan, M.H. Zinc, copper and iron content of milk from mothers of preterm and full-term infants. Early Hum. Dev. 1982, 6, 145–151. [Google Scholar] [CrossRef]
- Fernández-Sánchez, M.L.; De la Flor St. Remy, R.; González Iglesias, H.; López-Sastre, J.B.; Fernández-Colomer, B.; Pérez-Solís, D.; Sanz-Medel, A. Iron content and its speciation in human milk from mothers of preterm and full-term infants at early stages of lactation: A comparison with commercial infant milk formulas. Microchem. J. 2012, 105, 108–114. [Google Scholar]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef]
- Rigo, J.; Pieltain, C.; Salle, B.; Senterre, J. Enteral calcium, phosphate and vitamin d requirements and bone mineralization in preterm infants. Acta Paediatr. 2007, 96, 969–974. [Google Scholar] [CrossRef]
- Butte, N.F.; Garza, C.; Johnson, C.A.; Smith, E.O.; Nichols, B.L. Longitudinal changes in milk composition of mothers delivering preterm and term infants. Early Hum. Dev. 1984, 9, 153–162. [Google Scholar] [CrossRef]
- Aquilio, E.; Spagnoli, R.; Seri, S.; Bottone, G.; Spennati, G. Trace element content in human milk during lactation of preterm newborns. Biol. Trace Elem. Res. 1996, 51, 63–70. [Google Scholar] [CrossRef]
- Sann, L.; Bienvenu, F.; Lahet, C.; Bienvenu, J.; Bethenod, M. Comparison of the composition of breast milk from mothers of term and preterm infants. Acta Paediatr. Scand. 1981, 70, 115–116. [Google Scholar] [CrossRef]
- Koo, W.W.; Gupta, J.M. Breast milk sodium. Arch Dis. Child. 1982, 57, 500–502. [Google Scholar] [CrossRef]
- Anderson, G.H. The effect of prematurity on milk composition and its physiological basis. Fed. Proc. 1984, 43, 2438–2442. [Google Scholar]
- Chatterton, R.T., Jr.; Hill, P.D.; Aldag, J.C.; Hodges, K.R.; Belknap, S.M.; Zinaman, M.J. Relation of plasma oxytocin and prolactin concentrations to milk production in mothers of preterm infants: Influence of stress. J. Clin. Endocrinol. Metab. 2000, 85, 3661–3668. [Google Scholar] [CrossRef] [PubMed]
- Hill, P.D.; Aldag, J.C.; Demirtas, H.; Naeem, V.; Parker, N.P.; Zinaman, M.J.; Chatterton, R.T., Jr. Association of serum prolactin and oxytocin with milk production in mothers of preterm and term infants. Biol. Res. Nurs. 2009, 10, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Ackland, M.L.; Michalczyk, A.A. Zinc and infant nutrition. Arch Biochem. Biophys. 2016, 611, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Tindell, R.; Tipple, T. Selenium: Implications for outcomes in extremely preterm infants. J. Perinatol. 2018, 38, 197–202. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Population | Preterm | Term | p-Value * |
|---|---|---|---|
| Mothers (drop outs) | N = 27 (2) | N = 34 (2) | |
| Age (years) | 32.4 ± 5.6 | 31.2 ± 4.2 | 0.3173 |
| BMI before pregnancy (Kg/m2) | 22.8 ± 3.3 | 23.2 ± 4.9 | 0.6990 |
| BMI at child birth (Kg/m2) | 25.8 ± 3.7 | 26.9 ± 4.7 | 0.3141 |
| Delivery type: caesarean (%) | 63 | 23.5 | 0.0019 |
| Infants | N = 33 | N = 34 | |
| Gestational age at birth (weeks) | 30.8 ± 1.4 | 39.5 ± 1.0 | <0.0001 |
| Males (%) | 54.5 | 52.9 | 0.8952 |
| Twins (%) | 36.4 | 0.0 | 0.0001 |
| Height (cm) | 40.4 ± 3.2 | 49.4 ± 1.7 | <0.0001 |
| Weight (g) | 1421.4 ± 372.8 | 3277.6 ± 353.6 | <0.0001 |
| Head circumference (cm) | 27.8 ± 2.1 | 34.4 ± 1.5 | <0.0001 |
| Minerals | Statistic | Preterm Milk | Term Milk | Literature Range |
|---|---|---|---|---|
| (mg/L) | ||||
| Potassium | Mean | 578 ± 107 | 575 ± 92 | 515$ [17], 688$ [18] |
| Median | 569 (209–907) | 562 (308–908) | - | |
| Calcium | Mean | 281 ± 51 | 286 ± 47 | - |
| Median | 282 (145–459) | 287 (136–433) | 252 (84–462)# [19] | |
| Sodium | Mean | 205 ± 177 | 235 ± 237 | 135–371# [20] |
| Median | 160 (54–1577) | 170 (84–1969) | - | |
| Phosphorus | Mean | 145 ± 32 | 148 ± 30 | - |
| Median | 145 (48–225) | 146 (45–257) | 143 (17–278)# [19] | |
| Magnesium | Mean | 37 ± 9 | 32 ± 7 | - |
| Median | 36 (12–70) | 33 (17–53) | 31 (15–64)# [21] | |
| Zinc | Mean | 2.4 ± 1.7 | 3.2 ± 1.9 | 2.2–2.5; 2.9–3.9; 1.7–5.3# [22] |
| Median | 2.1 (0.2–15.5) | 2.7 (0.4–11.9) | - | |
| Iron | Mean | 0.36 ± 0.23 | 0.44 ± 0.26 | - |
| Median | 0.32 (0.13–2.78) | 0.36 (0.13–1.8) | 0.47 (0.04–1.92)# [23] | |
| Copper | Mean | 0.36 ± 0.16 | 0.44 ± 0.15 | - |
| Median | 0.35 (0.06–1.1) | 0.42 (0.13–1.0) | 0.33 (0.03–2.19)# [23] | |
| (µg/L) | ||||
| Iodine | Mean | 92 ± 67 | 87 ± 41 | 15–150# [20] |
| Median | 76 (2–422) | 76 (18–228) | 62 (5.4–2170)# [24] | |
| Selenium | Mean | 14.3 ± 4.7 | 15.0 ± 4.2 | 11$ [25]–28$ [26] |
| Median | 13 (4–45) | 14 (6–34) | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabatier, M.; Garcia-Rodenas, C.L.; De Castro, C.A.; Kastenmayer, P.; Vigo, M.; Dubascoux, S.; Andrey, D.; Nicolas, M.; Richoz Payot, J.; Bordier, V.; et al. Longitudinal Changes of Mineral Concentrations in Preterm and Term Human Milk from Lactating Swiss Women. Nutrients 2019, 11, 1855. https://doi.org/10.3390/nu11081855
Sabatier M, Garcia-Rodenas CL, De Castro CA, Kastenmayer P, Vigo M, Dubascoux S, Andrey D, Nicolas M, Richoz Payot J, Bordier V, et al. Longitudinal Changes of Mineral Concentrations in Preterm and Term Human Milk from Lactating Swiss Women. Nutrients. 2019; 11(8):1855. https://doi.org/10.3390/nu11081855
Chicago/Turabian StyleSabatier, Magalie, Clara L. Garcia-Rodenas, Carlos A. De Castro, Peter Kastenmayer, Mario Vigo, Stéphane Dubascoux, Daniel Andrey, Marine Nicolas, Janique Richoz Payot, Valentine Bordier, and et al. 2019. "Longitudinal Changes of Mineral Concentrations in Preterm and Term Human Milk from Lactating Swiss Women" Nutrients 11, no. 8: 1855. https://doi.org/10.3390/nu11081855
APA StyleSabatier, M., Garcia-Rodenas, C. L., De Castro, C. A., Kastenmayer, P., Vigo, M., Dubascoux, S., Andrey, D., Nicolas, M., Richoz Payot, J., Bordier, V., Thakkar, S. K., Beauport, L., Tolsa, J. -F., Fischer Fumeaux, C. J., & Affolter, M. (2019). Longitudinal Changes of Mineral Concentrations in Preterm and Term Human Milk from Lactating Swiss Women. Nutrients, 11(8), 1855. https://doi.org/10.3390/nu11081855