Biomarkers of Micronutrients in Regular Follow-Up for Tyrosinemia Type 1 and Phenylketonuria Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Parameters
2.3. Statistical Analyses
3. Results
3.1. Tyrosinemia Type 1 (TT1) versus Phenylketonuria (PKU)-nBH4 versus PKU-BH4
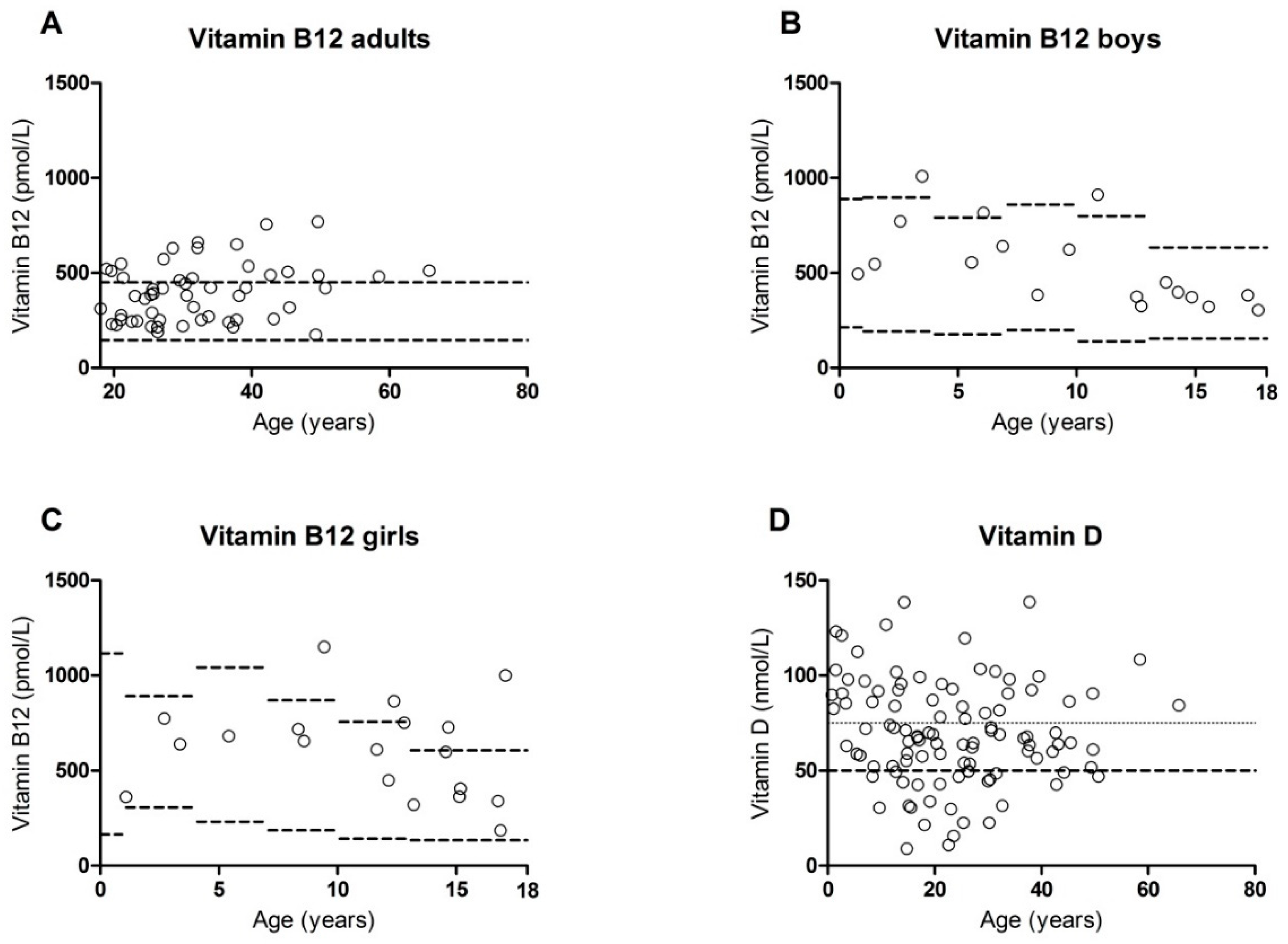
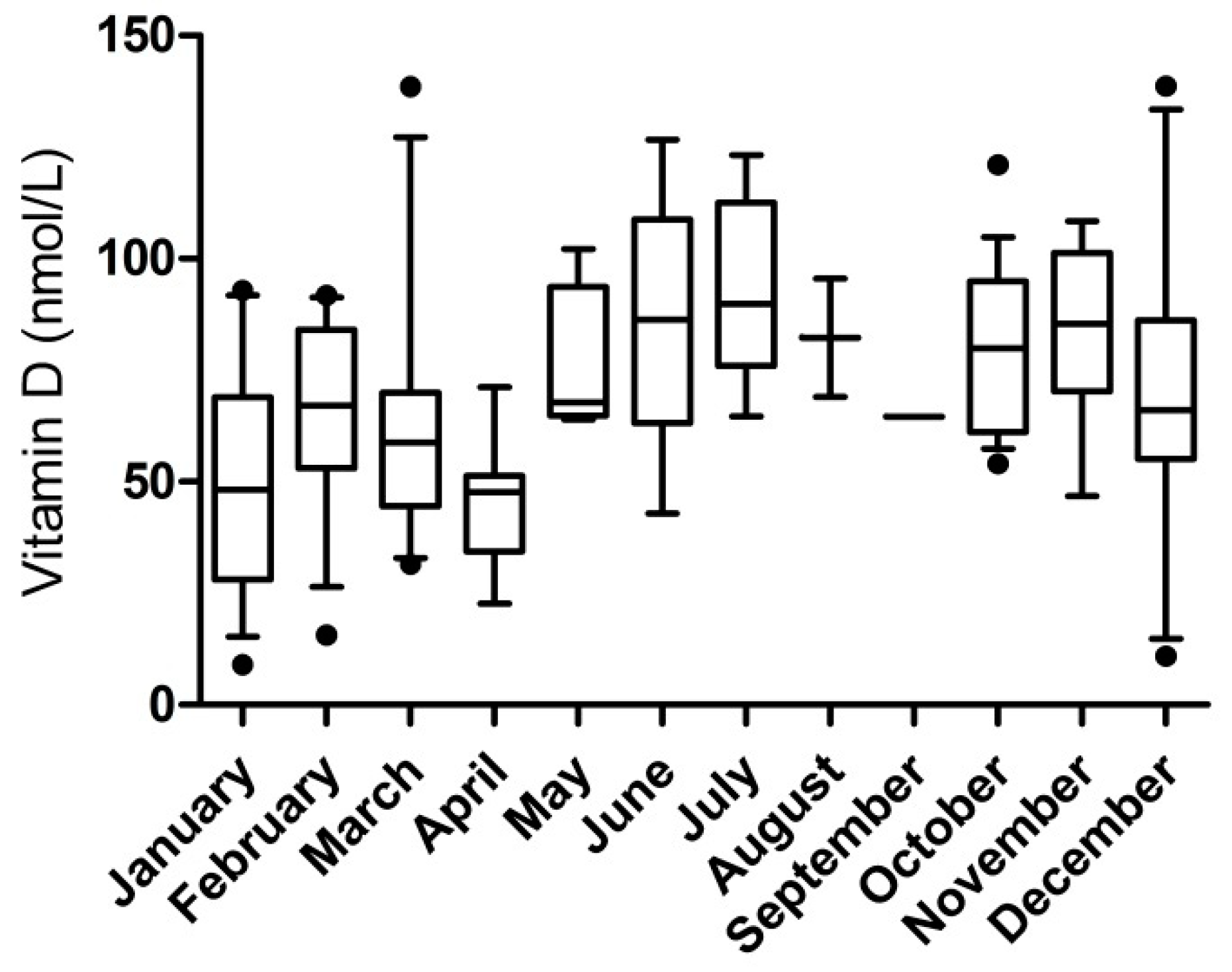
3.2. Deficiencies or Excesses
3.3. Correlations with Dietary Intake
3.4. Correlations with Phenylalanine and Tyrosine Concentrations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Blau, N.; van Spronsen, F.J.; Levy, H.L. Phenylketonuria. Lancet 2010, 376, 1417–1427. [Google Scholar] [CrossRef]
- Van Spronsen, F.J.; van Wegberg, A.M.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. Key European Guidelines for the Diagnosis and Management of Patients with Phenylketonuria. Lancet Diabet. Endocrinol. 2017, 5, 743–756. [Google Scholar] [CrossRef]
- Hennermann, J.B.; Bührer, C.; Blau, N.; Vetter, B.; Mönch, E. Long-Term Treatment with Tetrahydrobiopterin Increases Phenylalanine Tolerance in Children with Severe Phenotype of Phenylketonuria. Mol. Genet. Metab. 2005, 86 (Suppl. S1), 86–90. [Google Scholar] [CrossRef] [PubMed]
- Robert, M.; Rocha, J.C.; van Rijn, M.; Ahring, K.; Bélanger-Quintana, A.; MacDonald, A.; Dokoupil, K.; Gokmen Ozel, H.; Lammardo, A.M.; Goyens, P.; et al. Micronutrient Status in Phenylketonuria. Mol. Genet. Metab. 2013, 110 (Suppl. S6). [Google Scholar] [CrossRef] [PubMed]
- Kose, E.; Arslan, N. Vitamin/Mineral and Micronutrient Status in Patients with Classical Phenylketonuria. Clin. Nutr. 2019, 38, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Crujeiras, V.; Aldámiz-Echevarría, L.; Dalmau, J.; Vitoria, I.; Andrade, F.; Roca, I.; Leis, R.; Fernandez-Marmiesse, A.; Couce, M.L. Vitamin and Mineral Status in Patients with Hyperphenylalaninemia. Mol. Genet. Metab. 2015, 115, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Thiele, A.G.; Weigel, J.F.; Ziesch, B.; Rohde, C.; Mütze, U.; Ceglarek, U.; Thiery, J.; Müller, A.S.; Kiess, W.; Beblo, S. Nutritional Changes and Micronutrient Supply in Patients with Phenylketonuria Under Therapy with Tetrahydrobiopterin (BH(4)). JIMD Rep. 2013, 9, 31–40. [Google Scholar]
- Rohde, C.; von Teeffelen-Heithoff, A.; Thiele, A.G.; Arelin, M.; Mütze, U.; Kiener, C.; Gerloff, J.; Baerwald, C.; Schultz, S.; Heller, C.; et al. PKU Patients on a Relaxed Diet may be at Risk for Micronutrient Deficiencies. Eur. J. Clin. Nutr. 2014, 68, 119–124. [Google Scholar] [CrossRef]
- Brantley, K.D.; Douglas, T.D.; Singh, R.H. One-Year Follow-Up of B Vitamin and Iron Status in Patients with Phenylketonuria Provided Tetrahydrobiopterin (BH4). Orphanet. J. Rare Dis. 2018, 13, 192. [Google Scholar] [CrossRef]
- De Laet, C.; Dionisi-Vici, C.; Leonard, J.V.; McKiernan, P.; Mitchell, G.; Monti, L.; de Baulny, H.O.; Pintos-Morell, G.; Spiekerkötter, U. Recommendations for the Management of Tyrosinaemia Type 1. Orphanet. J. Rare Dis. 2013, 8, 8. [Google Scholar] [CrossRef]
- Lindstedt, S.; Holme, E.; Lock, E.A.; Hjalmarson, O.; Strandvik, B. Treatment of Hereditary Tyrosinaemia Type I by Inhibition of 4-Hydroxyphenylpyruvate Dioxygenase. Lancet 1992, 340, 813–817. [Google Scholar] [CrossRef]
- Bendadi, F.; de Koning, T.J.; Visser, G.; Prinsen, H.C.; de Sain, M.G.; Verhoeven-Duif, N.; Sinnema, G.; van Spronsen, F.J.; van Hasselt, P.M. Impaired Cognitive Functioning in Patients with Tyrosinemia Type I Receiving Nitisinone. J. Pediatr. 2014, 164, 398–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Ginkel, W.G.; Jahja, R.; Huijbregts, S.C.J.; Daly, A.; MacDonald, A.; De Laet, C.; Cassiman, D.; Eyskens, F.; Körver-Keularts, I.M.L.W.; Goyens, P.J.; et al. Neurocognitive Outcome in Tyrosinemia Type 1 Patients Compared to Healthy Controls. Orphanet. J. Rare Dis. 2016, 11, 87. [Google Scholar] [CrossRef] [PubMed]
- García, M.I.; de la Parra, A.; Arias, C.; Arredondo, M.; Cabello, J.F. Long-Term Cognitive Functioning in Individuals with Tyrosinemia Type 1 Treated with Nitisinone and Protein-Restricted Diet. Mol. Genet. Metab. Rep. 2017, 11, 12–16. [Google Scholar] [CrossRef] [PubMed]
- De Laet, C.; Munoz, V.T.; Jaeken, J.; François, B.; Carton, D.; Sokal, E.M.; Dan, B.; Goyens, P.J. Neuropsychological Outcome of NTBC-Treated Patients with Tyrosinaemia Type 1. Dev. Med. Child Neurol. 2011, 53, 962–964. [Google Scholar] [CrossRef]
- Thimm, E.; Richter-Werkle, R.; Kamp, G.; Molke, B.; Herebian, D.; Klee, D.; Mayatepek, E.; Spiekerkoetter, U. Neurocognitive Outcome in Patients with Hypertyrosinemia Type I After Long-Term Treatment with NTBC. J. Inherit. Metab. Dis. 2012, 35, 263–268. [Google Scholar] [CrossRef]
- Boonman-de Winter, L.J.M.; Albersen, A.; Mohrmann, K.; Bakx-van Baal Carla MA, C.; Meijer Timmerman Thijssen Dirk, W.; Bressers, J.P. [High Prevalence of Vitamin D Deficiency in the South-West Netherlands]. Ned Tijdschr Geneeskd 2015, 159, A8167. [Google Scholar]
- MaCdonald, A.; van Rijn, M.; Feillet, F.; Lund, A.M.; Bernstein, L.; Bosch, A.M.; Gizewska, M.; van Spronsen, F.J. Adherence Issues in Inherited Metabolic Disorders Treated by Low Natural Protein Diets. Ann. Nutr. Metab. 2012, 61, 289–295. [Google Scholar] [CrossRef]
- Malik, S.; NiMhurchadha, S.; Jackson, C.; Eliasson, L.; Weinman, J.; Roche, S.; Walter, J. Treatment Adherence in Type 1 Hereditary Tyrosinaemia (HT1): A Mixed-Method Investigation into the Beliefs, Attitudes and Behaviour of Adolescent Patients, their Families and their Health-Care Team. JIMD Rep. 2015, 18, 13–22. [Google Scholar]
- Demirdas, S.; van Spronsen, F.J.; Hollak, C.E.M.; van der Lee, J.H.; Bisschop, P.H.; Vaz, F.M.; Ter Horst, N.M.; Rubio-Gozalbo, M.E.; Bosch, A.M. Micronutrients, Essential Fatty Acids and Bone Health in Phenylketonuria. Ann. Nutr. Metab. 2017, 70, 111–121. [Google Scholar] [CrossRef]
- Vugteveen, I.; Hoeksma, M.; Monsen, A.B.; Fokkema, M.R.; Reijngoud, D.; van Rijn, M.; van Spronsen, F.J. Serum Vitamin B12 Concentrations within Reference Values do Not Exclude Functional Vitamin B12 Deficiency in PKU Patients of various Ages. Mol. Genet. Metab. 2011, 102, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Demirdas, S.; Coakley, K.E.; Bisschop, P.H.; Hollak, C.E.M.; Bosch, A.M.; Singh, R.H. Bone Health in Phenylketonuria: A Systematic Review and Meta-Analysis. Orphanet. J. Rare Dis. 2015, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Gentz, J.; Jagenburg, R.; Zetterstroem, R. Tyrosinemia. J. Pediatr. 1965, 66, 670–696. [Google Scholar] [CrossRef]
- MacDonald, A.; Rocha, J.C.; van Rijn, M.; Feillet, F. Nutrition in Phenylketonuria. Mol. Genet. Metab. 2011, 104 (Suppl. S10). [Google Scholar] [CrossRef] [PubMed]
- Sumanszki, C.; Kiss, E.; Simon, E.; Galgoczi, E.; Soos, A.; Patocs, A.; Kovacs, B.; Nagy, E.V.; Reismann, P. The Association of Therapy Adherence and Thyroid Function in Adult Patients with Phenylketonuria. Ann. Nutr. Metab. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Measurement | TT1 | PKU-nBH4 | PKU-BH4 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Unit | Min–Max | Median | N | Min–Max | Median | N | Min–Max | Median | N | |
| Age | years | 0.79–28.54 | 11.85 | 12 | 1.49–65.77 | 25.73 | 59 | 1.08–43.18 | 19.15 | 33 |
| Phenylalanine | µmol/L | 18– 61 | 43 | 12 | 63–1757 | 667 | 58 | 84–676 | 313 | 33 |
| Tyrosine | µmol/L | 237–742 | 489 | 12 | 24–149 | 60 | 58 | 29–107 | 58 | 33 |
| Anthropometrics | ||||||||||
| Height | sds | −1.03–0.88 | -0.18 | 11 | −2.64–2.48 | -0.46 | 50 | −2.42–1.00 | −0.17 | 32 |
| Weight | sds | −0.61–1.91 | 0.70 | 12 | −1.61–4.72 | 0.97 | 36 | −1.59–3.84 | 0.25 | 26 |
| BMI | sds | 0.24–2.48 | 1.20 | 11 | −1.21–4.03 | 1.08 | 51 | −2.10–3.60 | 0.61 | 31 |
| Hematology | ||||||||||
| Leucocytes | 109/L | 4.2–10.3 | 6.9 | 12 | 3.6–13.9 | 6.8 | 54 | 4.4–11.4 | 6.9 | 32 |
| Hemoglobin | mmol/L | 6.4–10.9 | 8.3 | 12 | 6.7–10.8 | 8.5 | 55 | 6.8–10.5 | 8.5 | 33 |
| Hematocrit | L/L | 0.31–0.49 | 0.38 | 12 | 0.31–0.49 | 0.40 | 52 | 0.33–0.47 | 0.41 | 30 |
| MCV * | fL | 74.1–93.8 | 84.6 | 12 | 74.2–95.8 | 88.1 | 55 | 73.8–97.7 | 89.8 | 33 |
| Thrombocytes | 109/L | 114 - 464 | 281 | 12 | 138 - 470 | 258 | 54 | 151–412 | 266 | 32 |
| Micronutrients and related parameters | ||||||||||
| Sodium | mmol/L | 137–142 | 139 | 11 | 135–144 | 140 | 54 | 138–142 | 140 | 30 |
| Potassium | mmol/L | 3.6–5.0 | 3.9 | 11 | 3.4–4.5 | 4.0 | 54 | 3.6–4.6 | 4.0 | 29 |
| Chloride | mmol/L | 100–105 | 104 | 7 | 101–107 | 104 | 24 | 102–106 | 104 | 12 |
| Creatinine | µmol/L | 14–84 | 44 | 12 | 25–87 | 61 | 52 | 32–90 | 63 | 29 |
| Urea | mmol/L | 2.1–7.2 | 3.7 | 10 | 1.2–6.5 | 4.0 | 53 | 1.8–5.8 | 4.0 | 30 |
| Calcium | mmol/L | 2.37–2.52 | 2.43 | 4 | 2.28–2.56 | 2.43 | 43 | 2.20–2.61 | 2.42 | 24 |
| Phosphate | mmol/L | 0.67–1.95 | 1.37 | 11 | 0.56–1.65 | 0.98 | 51 | 0.70–1.63 | 1.06 | 28 |
| Magnesium | mmol/L | 0.74–1.00 | 0.79 | 9 | 0.76–0.97 | 0.84 | 43 | 0.77–0.98 | 0.85 | 22 |
| Albumin | g/L | 48–48 | 48 | 1 | 43–53 | 48 | 18 | 44–53 | 49 | 13 |
| Total protein | g/L | 70–78 | 73 | 11 | 58–84 | 73 | 50 | 66–81 | 74 | 29 |
| Alkaline phosphatase | U/L | 49–434 | 214 | 11 | 46–370 | 85 | 42 | 50–283 | 83 | 21 |
| Ferritin | µg/L | 16–188 | 54 | 11 | 15–331 | 52 | 47 | 15–351 | 66 | 25 |
| Vitamin B12 | pmol/L | 252–1150 | 630 | 11 | 174–1000 | 423 | 49 | 214–682 | 377 | 30 |
| MMA | nmol/L | 114.8–304.7 | 168.7 | 11 | 47.4–527.8 | 158.9 | 56 | 94.3–562.9 | 196.5 | 32 |
| Total homocysteine | µmol/L | 4.1–9.6 | 5.4 | 11 | 3.3–17.7 | 6.3 | 44 | 3.6–21.0 | 7.6 | 28 |
| 25-OH-Vitamin D3 | nmol/L | 9.1–138.6 | 61.0 | 12 | 10.9–138.7 | 67.5 | 59 | 22.7–99.5 | 67.8 | 33 |
| Pre albumin | g/L | 0.15–0.48 | 0.32 | 11 | 0.15–0.51 | 0.30 | 54 | 0.17–0.45 | 0.30 | 27 |
| TSH | mU/L | 0.58–3.88 | 3.31 | 10 | 0.73–6.00 | 1.71 | 49 | 0.46–7.60 | 1.76 | 23 |
| Patients with a Deficiency | Patients with an Excess | |||||
|---|---|---|---|---|---|---|
| TT1 | PKU-nBH4 | PKU-BH4 | TT1 | PKU-nBH4 | PKU-BH4 | |
| N | N | N | N | N | N | |
| Blood count | ||||||
| Leucocytes | 1 (8%) | 2 (4%) | 0 | 0 | 4 (8%) | 3 (9%) |
| Hemoglobin | 0 | 2 (4%) | 1 (3%) | 0 | 0 | 0 |
| Hematocrit | 0 | 1 (2%) | 0 | 1 (8%) | 3 (6%) | 5 (16%) |
| MCV | 0 | 0 | 0 | 0 | 1 (2%) | 5 (15%) |
| Thrombocytes | 1 (8%) | 4 (8%) | 0 | 2 (17%) | 4 (7%) | 2 (6%) |
| Micronutrients and related parameters | ||||||
| Sodium | 0 | 0 | 0 | 0 | 0 | 0 |
| Potassium | 0 | 2 (4%) | 0 | 0 | 0 | 0 |
| Chloride | 0 | 0 | 0 | 0 | 0 | 0 |
| Creatinine | 1 (8%) | 2 (4%) | 1 (3%) | 0 | 0 | 0 |
| Urea | 0 | 5 (10%) | 1 (3%) | 0 | 0 | 0 |
| Calcium | 0 | 0 | 0 | 0 | 0 | 1 (4%) |
| Phosphate | 1 (9%) | 2 (4%) | 1 (3%) | 0 | 0 | 0 |
| Magnesium | 0 | 0 | 0 | 0 | 0 | 0 |
| Albumin | 0 | 0 | 0 | 0 | 4 (24%) | 3 (23%) |
| Total protein | 0 | 1 (2%) | 0 | 0 | 1 (2%) | 3 (10%) |
| Alkaline phosphatase | 0 | 0 | 0 | 1 (9%) | 2 (5%) | 1 (5%) |
| Ferritin | 0 | 2 (4%) | 2 (8%) | 0 | 3 (7%) | 0 |
| Vitamin B12 | 0 | 0 | 0 | 4 (36%) | 16 (33%) | 6 (20%) |
| MMA | 0 | 4 (7%) | 0 | 0 | 2 (4%) | 3 (9%) |
| Total homocysteine | 0 | 0 | 0 | 0 | 1 (2%) | 1 (3%) |
| 25-OH-Vitamin D3 | 1 (8%) | 17 (29%) | 8 (24%) | 0 | 0 | 0 |
| Pre albumin | 1 (9%) | 6 (11%) | 1 (4%) | 3 (27%) | 4 (8%) | 3 (11%) |
| TSH | 0 | 0 | 1 (4%) | 0 | 3 (6%) | 1 (4%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Vliet, K.; Rodenburg, I.L.; van Ginkel, W.G.; Lubout, C.M.A.; Wolffenbuttel, B.H.R.; van der Klauw, M.M.; Heiner-Fokkema, M.R.; van Spronsen, F.J. Biomarkers of Micronutrients in Regular Follow-Up for Tyrosinemia Type 1 and Phenylketonuria Patients. Nutrients 2019, 11, 2011. https://doi.org/10.3390/nu11092011
van Vliet K, Rodenburg IL, van Ginkel WG, Lubout CMA, Wolffenbuttel BHR, van der Klauw MM, Heiner-Fokkema MR, van Spronsen FJ. Biomarkers of Micronutrients in Regular Follow-Up for Tyrosinemia Type 1 and Phenylketonuria Patients. Nutrients. 2019; 11(9):2011. https://doi.org/10.3390/nu11092011
Chicago/Turabian Stylevan Vliet, Kimber, Iris L. Rodenburg, Willem G. van Ginkel, Charlotte M.A. Lubout, Bruce H.R. Wolffenbuttel, Melanie M. van der Klauw, M. Rebecca Heiner-Fokkema, and Francjan J. van Spronsen. 2019. "Biomarkers of Micronutrients in Regular Follow-Up for Tyrosinemia Type 1 and Phenylketonuria Patients" Nutrients 11, no. 9: 2011. https://doi.org/10.3390/nu11092011
APA Stylevan Vliet, K., Rodenburg, I. L., van Ginkel, W. G., Lubout, C. M. A., Wolffenbuttel, B. H. R., van der Klauw, M. M., Heiner-Fokkema, M. R., & van Spronsen, F. J. (2019). Biomarkers of Micronutrients in Regular Follow-Up for Tyrosinemia Type 1 and Phenylketonuria Patients. Nutrients, 11(9), 2011. https://doi.org/10.3390/nu11092011