Health Care Costs and Savings Associated with Increased Dairy Consumption among Adults in the United States


Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Dairy Consumption and Health Outcomes
2.2.1. Identification of Health Outcomes
2.2.2. Costs Associated with Health Outcomes
2.2.3. Dairy Consumption among Adults in the US
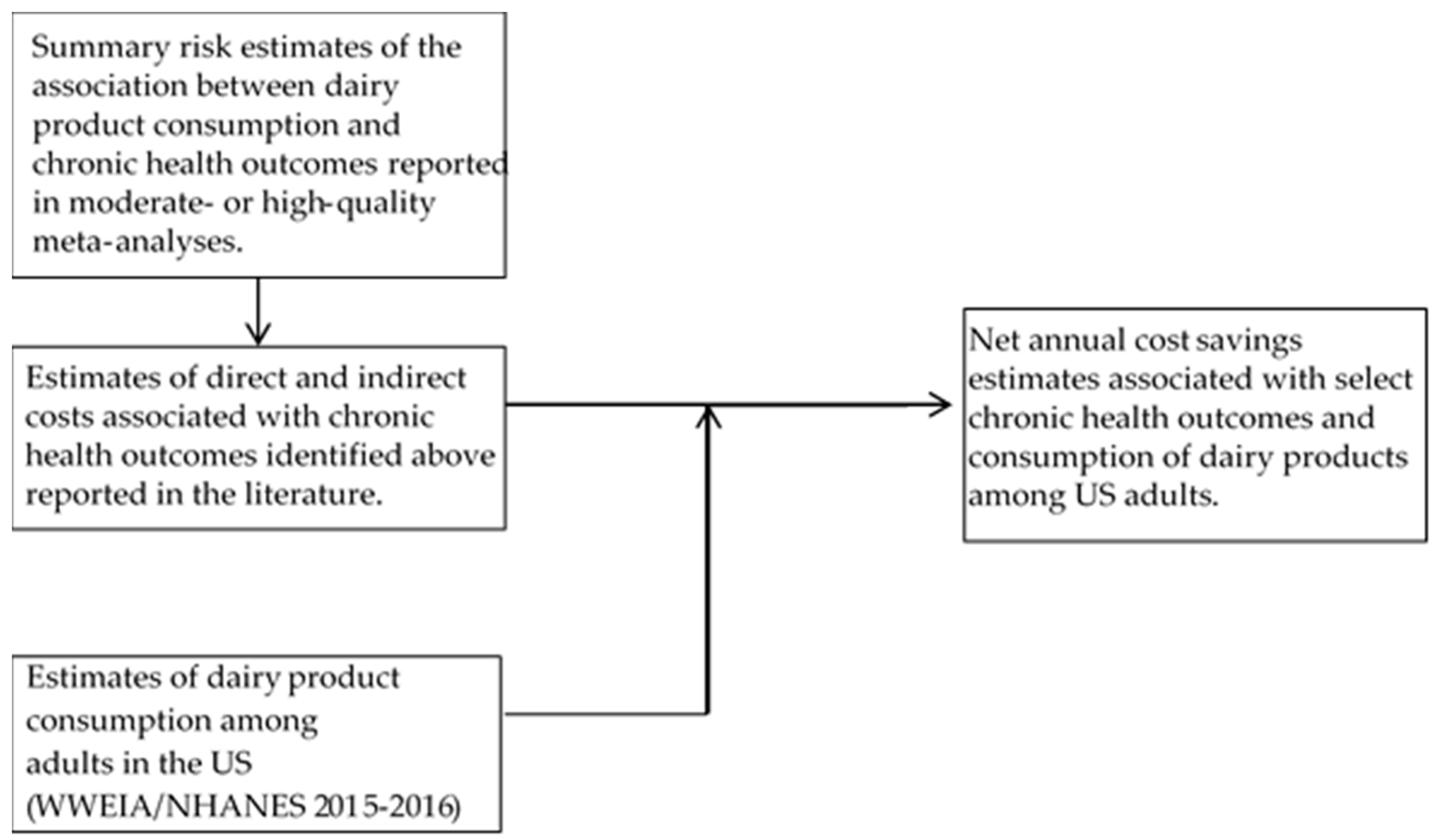
2.2.4. Model Structure
- ΔCosti = total annual change in costs for selected health outcome;
- i = index for selected health outcome (e.g., type 2 diabetes);
- ΔDCUS adults = change in dairy consumption (g/day) to meet DGA recommendation of 3 c-eq/day (Table 4).
- = total net change in annual costs;
- i = index for selected health outcome (e.g., type 2 diabetes);
- n = number of health outcomes included for each dairy type;
- = annual change in costs associated with health outcome i.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; U.S. Department of Health and Human Services; U.S. Department of Agriculture: Washington, DC, USA, 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 12 July 2019).
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; Dietary Guidelines Advisory Committee: Washington, DC, USA, 2015. [Google Scholar]
- Scrafford, C.G.; Bi, X.; Multani, J.K.; Murphy, M.M.; Schmier, J.K.; Barraj, L.M. Health Economic Evaluation Modeling Shows Potential Health Care Cost Savings with Increased Conformance with Healthy Dietary Patterns among Adults in the United States. J. Acad. Nutr. Diet. 2019, 119, 599–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doidge, J.C.; Segal, L.; Gospodarevskaya, E. Attributable risk analysis reveals potential healthcare savings from increased consumption of dairy products. J. Nutr. 2012, 142, 1772–1780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietary Guidelines Advisory Committee. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010, to the Secretary of Agriculture and the Secretary of Health and Human Services; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2010.
- Soedamah-Muthu, S.S.; Verberne, L.D.; Ding, E.L.; Engberink, M.F.; Geleijnse, J.M. Dairy consumption and incidence of hypertension: A dose-response meta-analysis of prospective cohort studies. Hypertension 2012, 60, 1131–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gijsbers, L.; Ding, E.L.; Malik, V.S.; de Goede, J.; Geleijnse, J.M.; Soedamah-Muthu, S.S. Consumption of dairy foods and diabetes incidence: A dose-response meta-analysis of observational studies. Am. J. Clin. Nutr. 2016, 103, 1111–1124. [Google Scholar] [CrossRef] [Green Version]
- De Goede, J.; Soedamah-Muthu, S.S.; Pan, A.; Gijsbers, L.; Geleijnse, J.M. Dairy Consumption and Risk of Stroke: A Systematic Review and Updated Dose-Response Meta-Analysis of Prospective Cohort Studies. J. Am. Heart Assoc. 2016, 5, e002787. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.M.; Knuppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.C.; Wang, Y.; Tong, X.; Szeto, I.M.; Smit, G.; Li, Z.N.; Qin, L.Q. Cheese consumption and risk of cardiovascular disease: A meta-analysis of prospective studies. Eur. J. Nutr. 2017, 56, 2565–2575. [Google Scholar] [CrossRef]
- Vieira, A.R.; Abar, L.; Chan, D.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef]
- Sun, Y.; Lin, L.J.; Sang, L.X.; Dai, C.; Jiang, M.; Zheng, C.Q. Dairy product consumption and gastric cancer risk: A meta-analysis. World J. Gastroenterol. 2014, 20, 15879–15898. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Navarro Rosenblatt, D.A.; Chan, D.S.; Vieira, A.R.; Vieira, R.; Greenwood, D.C.; Vatten, L.J.; Norat, T. Dairy products, calcium, and prostate cancer risk: A systematic review and meta-analysis of cohort studies. Am. J. Clin. Nutr. 2015, 101, 87–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, W.; Ju, C.; Jiang, H.; Zhang, D. Dairy foods intake and risk of Parkinson’s disease: A dose-response meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2014, 29, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Drouin-Chartier, J.P.; Brassard, D.; Tessier-Grenier, M.; Cote, J.A.; Labonte, M.E.; Desroches, S.; Couture, P.; Lamarche, B. Systematic Review of the Association between Dairy Product Consumption and Risk of Cardiovascular-Related Clinical Outcomes. Adv. Nutr. 2016, 7, 1026–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Astrup, A.; Lovegrove, J.A.; Gijsbers, L.; Givens, D.I.; Soedamah-Muthu, S.S. Milk and dairy consumption and risk of cardiovascular diseases and all-cause mortality: Dose-response meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2017, 32, 269–287. [Google Scholar] [CrossRef] [Green Version]
- Gholami, F.; Khoramdad, M.; Shakiba, E.; Alimohamadi, Y.; Shafiei, J.; Firouzi, A. Subgroup dairy products consumption on the risk of stroke and CHD: A systematic review and meta-analysis. Med. J. Islam. Repub. Iran 2017, 31, 25. [Google Scholar] [CrossRef] [Green Version]
- Gholami, F.; Khoramdad, M.; Esmailnasab, N.; Moradi, G.; Nouri, B.; Safiri, S.; Alimohamadi, Y. The effect of dairy consumption on the prevention of cardiovascular diseases: A meta-analysis of prospective studies. J. Cardiovasc. Thorac. Res. 2017, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Alexander, D.D.; Bylsma, L.C.; Vargas, A.J.; Cohen, S.S.; Doucette, A.; Mohamed, M.; Irvin, S.R.; Miller, P.E.; Watson, H.; Fryzek, J.P. Dairy consumption and CVD: A systematic review and meta-analysis. Br. J. Nutr. 2016, 115, 737–750. [Google Scholar] [CrossRef] [Green Version]
- Mullie, P.; Pizot, C.; Autier, P. Daily milk consumption and all-cause mortality, coronary heart disease and stroke: A systematic review and meta-analysis of observational cohort studies. BMC Public Health 2016, 16, 1236. [Google Scholar] [CrossRef] [Green Version]
- Schlesinger, S.; Neuenschwander, M.; Schwedhelm, C.; Hoffmann, G.; Bechthold, A.; Boeing, H.; Schwingshackl, L. Food Groups and Risk of Overweight, Obesity, and Weight Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2019, 10, 205–218. [Google Scholar] [CrossRef] [Green Version]
- Bechthold, A.; Boeing, H.; Schwedhelm, C.; Hoffmann, G.; Knuppel, S.; Iqbal, K.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; Schlesinger, S.; et al. Food groups and risk of coronary heart disease, stroke and heart failure: A systematic review and dose-response meta-analysis of prospective studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 1071–1090. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knuppel, S.; Iqbal, K.; Andriolo, V.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food Groups and Risk of Hypertension: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2017, 8, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knuppel, S.; Laure Preterre, A.; Iqbal, K.; Bechthold, A.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; et al. Food groups and risk of colorectal cancer. Int. J. Cancer 2018, 142, 1748–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, S.; Hu, J.; Zhang, K.; Wang, Y.; Yu, M.; Ma, J. Dairy product consumption and risk of hip fracture: A systematic review and meta-analysis. BMC Public Health 2018, 18, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity, and Cancer: A Global Perspective. Continuous Update Project Expert Report 2018. Available online: https://www.wcrf.org/sites/default/files/Summary-of-Third-Expert-Report-2018.pdf (accessed on 22 July 2019).
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of Parkinson’s disease: Risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report from the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Association, A.D. Economic costs of diabetes in the U.S. in 2012. Diabetes Care 2013, 36, 1033–1046. [Google Scholar] [CrossRef] [Green Version]
- Mariotto, A.B.; Yabroff, K.R.; Shao, Y.; Feuer, E.J.; Brown, M.L. Projections of the cost of cancer care in the United States: 2010–2020. J. Natl. Cancer Inst. 2011, 103, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Kowal, S.L.; Dall, T.M.; Chakrabarti, R.; Storm, M.V.; Jain, A. The current and projected economic burden of Parkinson’s disease in the United States. Mov. Disord. 2013, 28, 311–318. [Google Scholar] [CrossRef]
- Bureau of Labor Statistics. Medical Care in U.S. City Average, All Urban Consumers, Seasonally Adjusted. Databases, Tables & Calculators by Subject; United States Department of Labor: Washington, DC, USA, 2019.
- Hogan, P.; Dall, T.; Nikolov, P. Economic costs of diabetes in the US in 2002. Diabetes Care 2003, 26, 917–932. [Google Scholar]
- Zaorsky, N.G.; Churilla, T.M.; Egleston, B.L.; Fisher, S.G.; Ridge, J.A.; Horwitz, E.M.; Meyer, J.E. Causes of death among cancer patients. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 400–407. [Google Scholar] [CrossRef]
- American Diabetes Association. Statistics about Diabetes. 2019. Available online: http://www.diabetes.org/diabetes-basics/statistics/ (accessed on 22 July 2019).
- Dall, T.M.; Zhang, Y.; Chen, Y.J.; Quick, W.W.; Yang, W.G.; Fogli, J. The economic burden of diabetes. Health Aff. 2010, 29, 297–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute. Cancer Stat Facts: Colon and Rectum Cancer. Statistics at a Glance. 2017. Available online: https://seer.cancer.gov/statfacts/ (accessed on 11 May 2017).
- Pike, C.; Birnbaum, H.G.; Schiller, M.; Sharma, H.; Burge, R.; Edgell, E.T. Direct and indirect costs of non-vertebral fracture patients with osteoporosis in the US. Pharmacoeconomics 2010, 28, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Meehan, J.P.; Blumenfeld, T.; Szabo, R.M. Hip fractures in the United States: 2008 nationwide emergency department sample. Arthritis Care Res. (Hoboken) 2012, 64, 751–757. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. National Health and Nutrition Examination Survey Data 2015–2016. 2018. Available online: https://wwwn.cdc.gov/nchs/nhanes/search/datapage.aspx?Component=Dietary&CycleBeginYear=2015 (accessed on 12 July 2019).
- Bowman, S.A.; Clemens, J.C.; Shimizu, M.; Friday, J.E.; Moshfegh, A.J. Food Patterns Equivalents Database 2015–2016: Methodology and User Guide [Online]; Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S. Department of Agriculture: Beltsville, MD, USA, 2018. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 12 July 2019).
- McCarron, D.A.; Heaney, R.P. Estimated healthcare savings associated with adequate dairy food intake. Am. J. Hypertens. 2004, 17, 88–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Hoffmann, G.; Schwedhelm, C.; Kalle-Uhlmann, T.; Missbach, B.; Knuppel, S.; Boeing, H. Consumption of Dairy Products in Relation to Changes in Anthropometric Variables in Adult Populations: A Systematic Review and Meta-Analysis of Cohort Studies. PLoS ONE 2016, 11, e0157461. [Google Scholar] [CrossRef] [PubMed]
- Dall, T.M.; Yang, W.; Halder, P.; Pang, B.; Massoudi, M.; Wintfeld, N.; Semilla, A.P.; Franz, J.; Hogan, P.F. The economic burden of elevated blood glucose levels in 2012: Diagnosed and undiagnosed diabetes, gestational diabetes mellitus, and prediabetes. Diabetes Care 2014, 37, 3172–3179. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.J.; Kaltenboeck, A.; Diener, M.; Birnbaum, H.G.; Grubb, E.; Castelli-Haley, J.; Siderowf, A.D. Costs of Parkinson’s disease in a privately insured population. Pharmacoeconomics 2013, 31, 799–806. [Google Scholar] [CrossRef] [Green Version]
- Luengo-Fernandez, R.; Gray, A.M.; Rothwell, P.M. Costs of stroke using patient-level data: A critical review of the literature. Stroke 2009, 40, e18–e23. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Health Outcome(s) | Selected Study (MOOSE Rating) | Study Population | Endpoints Measured | Dairy Types | Comparator |
|---|---|---|---|---|---|
| Cardiovascular diseases and related outcomes | Bechthold et al. 2017 [23] (81%) | N = 24 studies (Europe = 15, US = 8, Asia = 1) 5.4–26 y of follow-up Prospective cohort studies, case-cohort, nested case-control, RCTs | Fatal/nonfatal coronary heart disease; stroke; heart failure | Total dairy (low-fat and high-fat) | High vs. low intake; 200 g/day |
| de Goede et al. 2016 [8] (97%) | N = 18 studies (US, Europe, Nordic countries, Australia, Japan, China, Singapore); 8 to 26 years of follow-up; 762,414 individuals and 29,943 stroke events Prospective cohort studies | Total stroke and ischemic, hemorrhagic, or fatal stroke | Total dairy (low-fat and high-fat) Fermented dairy Milk (low-fat and high-fat), cheese, yogurt | Milk: 200 g/day Cheese: 40 g/day Yogurt:100 g/day | |
| Hypertension | Schwingshackl et al. 2017 [24] (86%) | N = 9 studies (Europe = 5, US = 3, Asia = 1) 116,415 subjects 2–15 y of follow-up Prospective cohort studies, case-cohort, nested case-control, RCTs | Incidence (SBP ≥ 140 mm Hg OR DBP ≥ 90 mm hg OR anti-HT medication use) | Total dairy (low-fat and high-fat) | High vs. low intake; 200 g/day |
| Soedamah-Muthu et al. 2012 [6] (72%) | N = 9 studies Prospective cohort studies Duration of follow-up: 2 to 15 y | Incidence (SBP ≥ 140 mm Hg OR DBP ≥ 90 mm hg OR anti-HT medication use) | Total dairy (low-fat and high-fat) Milk, cheese, yogurt | 200 g/day | |
| Colorectal cancer | Schwingshackl et al. 2017 [25] (89%) | N = 18 studies (Europe = 8, US = 8, Asia = 2) 1,629,366 subjects Duration of follow-up: 3.3–26 y Prospective cohort, longitudinal, follow-up, case-cohort, nested case control studies | Colorectal cancer | Total dairy (low-fat and high-fat) | High vs. low intake; 200 g/day |
| Vieira et al. 2017 [11] (72%) | N = 10 studies (Europe and US) Prospective cohort studies, case-cohort, nested case-control, RCTs | Colorectal cancer | Total dairy Milk | Total dairy: 400 g/day Milk: 200 g/day | |
| Prostate cancer | Aune et al. 2015 [13] (86%) | N = 15 studies (total dairy, milk); N = 11 studies (cheese); N = 6 studies (yogurt) Prospective cohort studies | Total prostate cancer, non-advanced, advanced, fatal | Total dairy, milk, low-fat milk, whole milk, cheese, yogurt | Total dairy: 400 g/day Milk:200 g/ day Cheese: 50 g/day Yogurt: 100 g/day |
| Type 2 diabetes | Schwingshackl et al. 2017 [9] (78%) | N = 21 studies (Europe N = 8, US N = 7, Asia N = 4, Australia N = 2) Prospective cohort studies, nested case-control studies, case-cohort studies | Type 2 diabetes | Total dairy (low-fat and high-fat) | Total dairy: 200 g/day |
| Gijsbers et al. 2016 [7] (81%) | N = 20 articles/22 studies/23 populations (US, Europe, Asia, Australia) Prospective cohort studies Duration of follow-up: 2.6–30 y | Type 2 diabetes | Total dairy (low-fat and high-fat) Milk, cheese, yogurt | Total dairy/milk:200 g/day Cheese: 10 g/day Yogurt: 50 g/day | |
| Parkinson’s disease | Jiang et al. 2014 [14] (72%) | N = 5 studies (US, Finland, Greece) and 7 data points; follow-up from 8.45 to 41 y Prospective cohort studies | Parkinson’s disease | Total dairy, milk | Total dairy: high vs. low intake Milk: 200 g/day |
| Hip fracture | Bian et al. 2018 [26] (78%) | N = 18 studies (Europe = 7, US = 5, Asia = 4, Australia = 1, Europe/Canada/Australia = 1) 381,987 subjects Prospective cohort and case control studies | Hip fracture | Total dairy Milk, yogurt, cheese, cream | High vs. low intake; Milk: 200 g/day |
| Health Outcome | Relative Risk (95%CI) | Comparator | Source |
|---|---|---|---|
| Total dairy | |||
| Stroke | 0.96 (0.94, 0.98) | per 200 g/day | [23] |
| Hypertension | 0.95 (0.94, 0.97) | per 200 g/day | [24] |
| Type 2 diabetes | 0.97 (0.94, 0.99) | per 200 g/day | [9] |
| Hip fractures | 1.02 (0.93, 1.12) | High vs. low | [26] |
| Colorectal cancer | 0.93 (0.91, 0.94) | per 200 g/day | [25] |
| Parkinson’s disease | 1.40 (1.20, 1.63) | High vs. low | [14] |
| Prostate cancer | 1.07 (1.02, 1.12) | per 400 g/day | [13] |
| High-fat dairy | |||
| Stroke | 0.99 (0.97, 1.02) | per 200 g/day | [23] |
| Hypertension | 0.97 (0.93, 0.98) | per 200 g/day | [24] |
| Type 2 diabetes | 1.00 (0.96, 1.04) | per 200 g/day | [9] |
| Hip fractures | -- | -- | |
| Colorectal cancer | 0.91 (0.86, 0.97) | per 200 g/day | [25] |
| Parkinson’s disease | -- | -- | |
| Prostate cancer | -- | -- | |
| Low-fat dairy | |||
| Stroke | 0.98 (0.95, 1.00) | per 200 g/day | [23] |
| Hypertension | 0.96 (0.93, 0.99) | per 200 g/day | [24] |
| Type 2 diabetes | 0.97 (0.94, 1.00) | per 200 g/day | [9] |
| Hip fractures | -- | -- | |
| Colorectal cancer | 0.94 (0.88, 1.00) | per 200 g/day | [25] |
| Parkinson’s disease | -- | -- | |
| Prostate cancer | -- | -- | |
| Milk | |||
| Stroke | 0.93 (0.88, 0.98) | per 200 g/day | [8] |
| Hypertension | 0.96 (0.94, 0.98) | per 200 g/day | [6] |
| Type 2 diabetes | 0.97 (0.93, 1.02) | per 200 g/day | [7] |
| Hip fractures | 1.00 (0.94, 1.07) | per 200 g/day | [26] |
| Colorectal cancer | 0.94 (0.92, 0.96) | per 200 g/day | [11] |
| Parkinson’s disease | 1.17 (1.06, 1.30) | per 200 g/day | [14] |
| Prostate cancer | 1.03 (1.00, 1.06) | per 200 g/day | [13] |
| Cheese | |||
| Stroke | 0.97 (0.94, 1.01) | per 40 g/day | [8] |
| Hypertension | 1.00 (0.98, 1.03) | per 200 g/day | [6] |
| Type 2 diabetes | 1.00 (0.99, 1.02) | per 10 g/day | [7] |
| Hip fractures | 0.68 (0.61, 0.77) | High vs. low | [26] |
| Colorectal cancer | -- | -- | |
| Parkinson’s disease | 1.26 (0.99, 1.60) | High vs. low | [14] |
| Prostate cancer | 1.10 (1.03, 1.18) | per 50 g/day | [13] |
| Yogurt | |||
| Stroke | 1.02 (0.90, 1.17) | per 100 g/day | [8] |
| Hypertension | 0.99 (0.96, 1.01) | per 200 g/day | [6] |
| Type 2 diabetes | 0.94 (0.90, 0.97) | per 50 g/day | [7] |
| Hip fractures | 0.75 (0.66, 0.86) | High vs. low | [26] |
| Colorectal cancer | -- | -- | |
| Parkinson’s disease | 0.95 (0.76, 1.20) | High vs. low | [14] |
| Prostate cancer | 1.08 (0.93, 1.24) | per 100 g/day | [13] |
| Annual Direct and Indirect Costs (Billions $) | ||||
|---|---|---|---|---|
| Health Outcome | Direct | Indirect | Total | Assumptions and Adjustments |
| Stroke | 30.3 | 18.9 | 49.2 | Annual average cost from 2015–2016 [29]. |
| Hypertension | 55.5 | 5.0 | 60.4 | Annual average cost from 2015–2016; limited to hypertension without heart disease [29]. |
| Type 2 diabetes | 207.6 | 105.6 | 313.2 | Annual average cost from 2017 for total expenditures and indirect costs for diabetes ($327B) [30] and assuming 96% of diabetes cases are type 2 diabetes based on a cited prevalence of 1.25 million type 1 diabetes cases out of total prevalence of 30.3 million Americans with diabetes in 2015 [36]. The proportion of total costs allocated to direct and indirect costs was based on estimates from Dall et al. (2010) [37]. |
| Type 2 diabetes (adjusted for costs associated with cardiovascular disease complications) | 167.7 | 65.3 | 233.0 | 19.2% of direct medical costs [34] and 38.2% of indirect costs [30] estimated to be associated with cardiovascular disease and therefore, subtracted out from the total costs for type 2 diabetes estimated above. |
| Colorectal cancer | 14.4 | -- | 14.4 | Modelled estimates of annual medical costs per case for stages of treatment for adults <65 years and ≥65 years associated with colorectal or prostate cancer in 2010 using SEER [31]. Combined estimate for the total adult US population estimated by combining cost data for all age and treatment categories weighted according to the prevalence of adults in each category [31] and the total prevalence of colorectal cancer in 2016 adjusted to reflect the 2018 US adult population [38]. |
| Prostate cancer | 4.7 | -- | 4.7 | |
| Parkinson’s disease | 10.0 | 7.9 | 17.9 | Annual average cost from 2010 [32]. |
| Hip fractures | 17.6 | -- | 17.6 | Costs of osteoporotic hip fractures among privately-insured young adults (18–64 years) and Medicare-insured elderly adults were compared with matched controls with osteoporosis and no fractures [39]. Direct medical costs were calculated; indirect costs (lost work productivity) were available for a subset of working patients (2006 dollars). The number of hip fractures annually in the US was estimated to be approximately 341,000 (based on patients visiting emergency departments) [40]. |
| Dairy Product | Dairy Intake among Adults in the US | Scenario 1 | Scenario 2 | |||
|---|---|---|---|---|---|---|
| Increase Required to Meet DGA Recommendation | Increase Required to Meet DGA Recommendation | |||||
| c-eq/day | g/day | c-eq/day | g/day | c-eq/day | g/day | |
| Total dairy * | 1.49 | 246 | 1.51 | 249 | 1.51 | 249 |
| Total dairy (Men only) | 1.71 | 282 | 1.29 | 213 | 1.29 | 213 |
| Milk | 0.63 | 155 | 0.94 | 231 | 1.51 | 369 |
| Milk (Men only) | 0.70 | 172 | 0.87 | 214 | 1.29 | 316 |
| Cheese | 0.73 | 49 | 0.62 | 41 | 1.51 | 101 |
| Cheese (Men only) | 0.89 | 2759 | 0.46 | 31 | 1.29 | 86 |
| Yogurt | 0.09 | 21 | 0 | 0 | 0.4 | 100 |
| Health Outcome | Total Dairy (Billions $ (Range)) | High-Fat Dairy (Billions $ (Range)) | Low-Fat Dairy (Billions $ (Range)) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Direct | Indirect | Total | Direct | Indirect | Total | Direct | Indirect | Total | |
| Stroke | 1.5 (0.8, 2.3) | 0.9 (0.5, 1.4) | 2.4 (1.3, 3.7) | -- | -- | -- | 0.8 (0, 1.9) | 0.5 (0, 1.2) | 1.3 (0, 3.1) |
| Hypertension | 3.4 (2.1, 4.1) | 0.3 (0.2, 0.4) | 3.7 (2.3, 4.5) | 2.1 (1.4, 4.8) | 0.2 (0.1, 0.4) | 2.3 (1.5, 5.2) | 2.8 (0.7, 4.8) | 0.2 (0.1, 0.4) | 3 (0.8, 5.2) |
| Type 2 diabetes | 6.3 (2.1, 12.5) | 2.4 (0.8, 4.9) | 8.7 (2.9, 17.4) | -- | -- | -- | 6.3 (0, 12.5) | 2.4 (0, 4.9) | 8.7 (0, 17.4) |
| Colorectal cancer a | 1.3 (1.1, 1.6) | -- | 1.3 (1.1, 1.6) | 1.6 (0.5, 2.5) | -- | 1.6 (0.5, 2.5) | 1.1 (0, 2.2) | -- | 1.1 (0, 2.2) |
| Parkinson’s disease | −1.9 (−3, −0.9) | −1.5 (−2.3, −0.7) | −3.4 (−5.3, −1.6) | -- | -- | -- | -- | -- | -- |
| Prostate cancer a | −0.2 (−0.3, 0) | -- | −0.2 (−0.3, 0) | -- | -- | -- | -- | -- | -- |
| Total (primary) b | 10.4 (2.8, 19.6) | 2.1 (−0.8, 6.0) | 12.5 (2.0, 25.6) | 3.7 (1.9, 7.3) | 0.2 (0.1, 0.4) | 3.9 (2.0, 7.7) | 11 (0.7, 21.4) | 3.1 (0.06, 6.5) | 14.1 (0.8, 27.9) |
| Total (secondary) b,c | 12.5 (6.1, 20.5) | 3.6 (1.5, 6.7) | 16.1 (7.6, 27.2) | 3.7 (1.9, 7.3) | 0.2 (0.1, 0.4) | 3.9 (2.0, 7.7) | 11 (0.7, 21.4) | 3.1 (0.06, 6.5) | 14.1 (0.8, 27.9) |
| Milk (Billions $ (Range)) | Cheese (Billions $ (Range)) | Yogurt (Billions $ (Range)) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Health Outcome | Direct | Indirect | Total | Direct | Indirect | Total | Direct | Indirect | Total |
| Scenario 1: Mean Intakes of Milk, Cheese and Yogurt Were Each Increased to Result in Total Proportions by Type as Specified in USDA Food Intake Patterns [2] | |||||||||
| Stroke | 2.4 (0.7, 4.2) | 1.5 (0.4, 2.6) | 3.9 (1.1, 6.8) | -- | -- | -- | -- | -- | -- |
| Hypertension | 2.6 (1.3, 3.8) | 0.2 (0.1, 0.3) | 2.8 (1.4, 4.1) | -- | -- | -- | -- | -- | -- |
| Type 2 diabetes | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| Hip Fractures a | -- | -- | -- | 1.7 (1.2, 2.1) | -- | 1.7 (1.2, 2.1) | -- | -- | -- |
| Colorectal cancer b | 1 (0.7, 1.3) | -- | 1 (0.7, 1.3) | -- | -- | -- | -- | -- | -- |
| Parkinson’s disease | −2 (−3.5, −0.7) | −1.5 (−2.7, −0.5) | −3.5 (−6.2, −1.2) | -- | -- | -- | -- | -- | -- |
| Prostate cancer b | −0.1 (−0.3, 0) | -- | −0.1 (−0.3, 0) | −0.3 (−0.5, 0.09) | -- | −0.3 (−0.5, 0.09) | -- | -- | -- |
| Total (primary) c | 3.9 (−1.1, 8.6) | 0.2 (−2.2, 2.4) | 4.1 (−3.3, 11) | 1.4 (0.7, 2.0) | -- | 1.4 (0.7, 2.0) | -- | -- | -- |
| Total (secondary) c,d | 6 (2.7, 9.3) | 1.7 (0.5, 2.9) | 7.7 (3.2, 12.2) | 1.7 (1.2, 2.1) | -- | 1.7 (1.2, 2.1) | -- | -- | -- |
| Scenario 2: Mean Intake of Each Type of Dairy Product Was Increased Assuming the Consumption of Only That Dairy Type to Meet the 3 C-Eq/Day Recommendation | |||||||||
| Stroke | 3.9 (1.1, 6.7) | 2.4 (0.7, 4.2) | 6.3 (1.8, 10.9) | -- | -- | -- | -- | -- | -- |
| Hypertension | 4.1 (2, 6.1) | 0.4 (0.2, 0.6) | 4.5 (2.2, 6.7) | -- | -- | -- | -- | -- | -- |
| Type 2 diabetes | -- | -- | -- | -- | -- | -- | 20.2 (10.1, 33.7) | 7.9 (3.9, 13.1) | 28.1 (14, 46.8) |
| Hip Fractures a | -- | -- | -- | 4.2 (3.0, 5.2) | -- | 4.2 (3.0, 5.2) | 4.4 (2.5, 6) | -- | 4.4 (2.5, 6) |
| Colorectal cancer b | 1.6 (1.1, 2.1) | -- | 1.6 (1.1, 2.1) | -- | -- | -- | -- | -- | -- |
| Parkinson’s disease | −3.1 (−5.6, −1.1) | −2.5 (−4.4, −0.9) | −5.6 (−10.0, −2.0) | -- | -- | -- | -- | -- | -- |
| Prostate cancer b | −0.2 (−0.4, 0) | -- | −0.2 (−0.4, 0) | −0.8 (−1.4, −0.2) | -- | −0.8 (−1.4, −0.2) | -- | -- | -- |
| Total (primary) c | 6.3 (−1.8, 13.8) | 0.3 (−3.5, 3.9) | 6.6 (−5.3, 17.7) | 3.4 (1.4, 5.0) | -- | 3.4 (1.6, 5.0) | 24.6 (12.6, 39.7) | 7.9 (3.9, 13.1) | 32.5 (16.5, 52.8) |
| Total (secondary) c,d | 9.6 (4.2, 14.9) | 2.8 (0.9, 4.8) | 12.4 (5.1, 19.7) | 4.2 (3.0, 5.2) | -- | 4.2 (3.0, 5.2) | 24.6 (12.6, 39.7) | 7.9 (3.9, 13.1) | 32.5 (16.5, 52.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scrafford, C.G.; Bi, X.; Multani, J.K.; Murphy, M.M.; Schmier, J.K.; Barraj, L.M. Health Care Costs and Savings Associated with Increased Dairy Consumption among Adults in the United States. Nutrients 2020, 12, 233. https://doi.org/10.3390/nu12010233
Scrafford CG, Bi X, Multani JK, Murphy MM, Schmier JK, Barraj LM. Health Care Costs and Savings Associated with Increased Dairy Consumption among Adults in the United States. Nutrients. 2020; 12(1):233. https://doi.org/10.3390/nu12010233
Chicago/Turabian StyleScrafford, Carolyn G., Xiaoyu Bi, Jasjit K. Multani, Mary M. Murphy, Jordana K. Schmier, and Leila M. Barraj. 2020. "Health Care Costs and Savings Associated with Increased Dairy Consumption among Adults in the United States" Nutrients 12, no. 1: 233. https://doi.org/10.3390/nu12010233
APA StyleScrafford, C. G., Bi, X., Multani, J. K., Murphy, M. M., Schmier, J. K., & Barraj, L. M. (2020). Health Care Costs and Savings Associated with Increased Dairy Consumption among Adults in the United States. Nutrients, 12(1), 233. https://doi.org/10.3390/nu12010233