Folic Acid Fortification and Neural Tube Defect Risk: Analysis of the Food Fortification Initiative Dataset


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Description of Data Utilized from the Food Fortification Initiative (FFI)
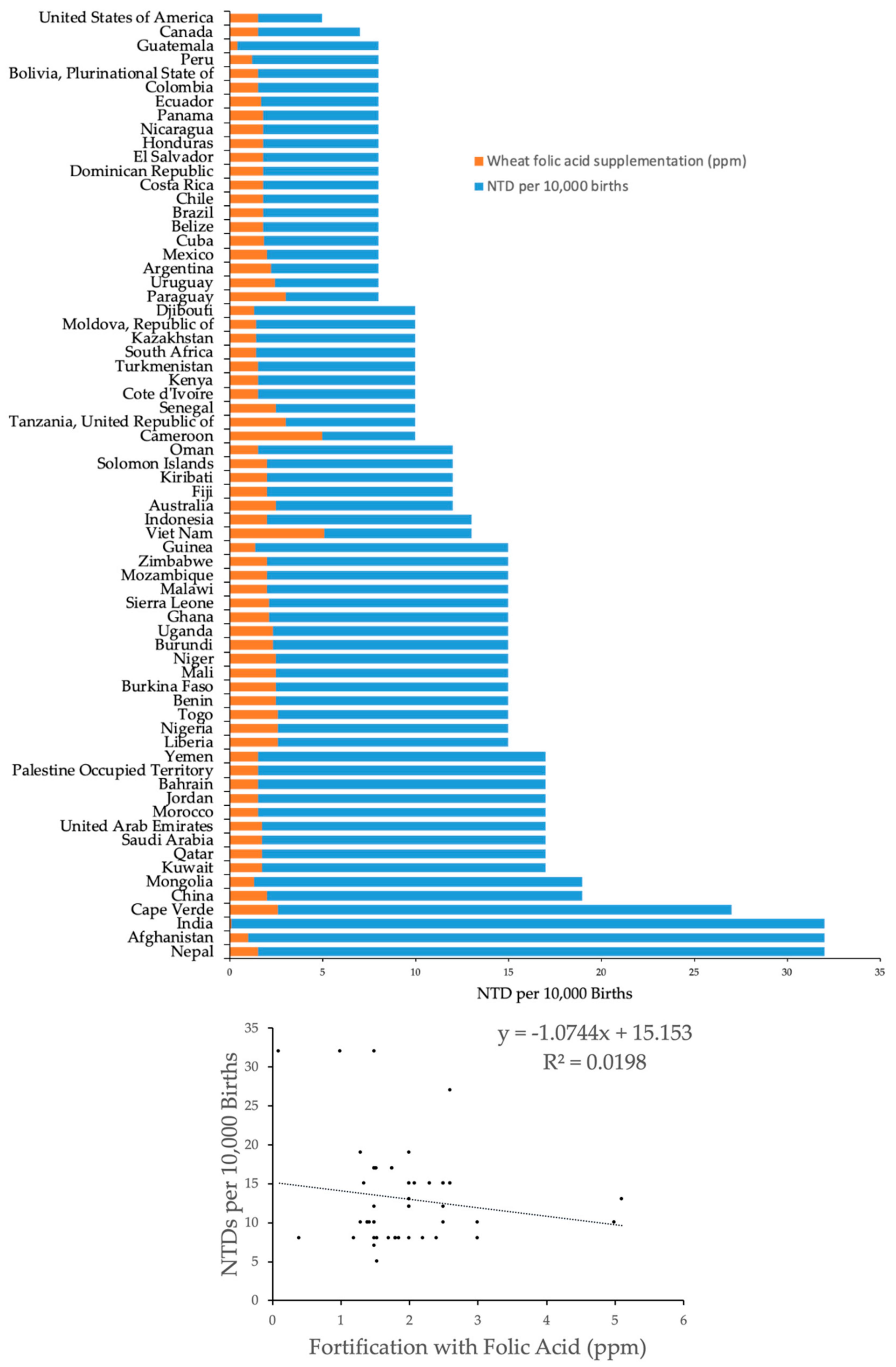
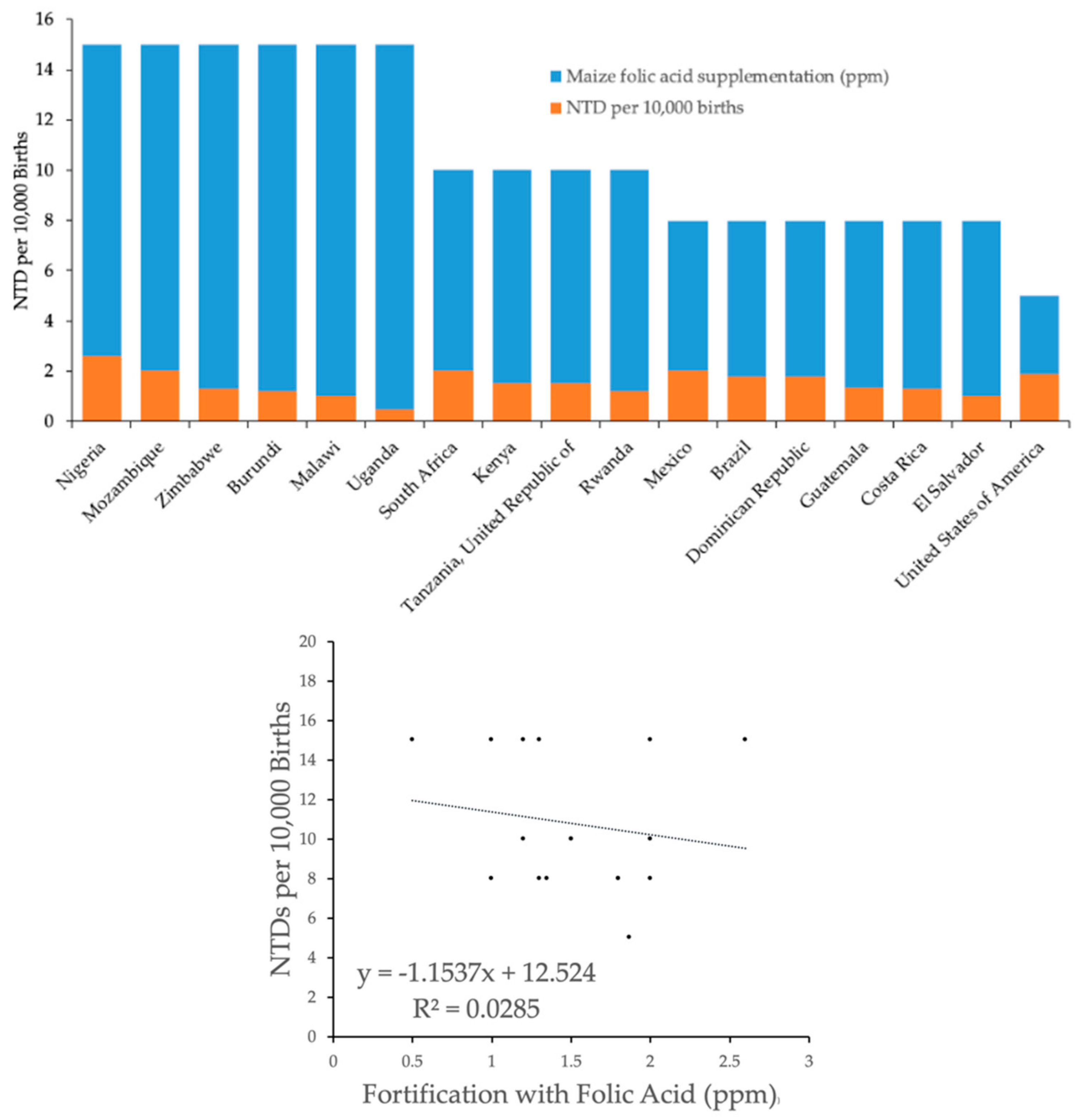
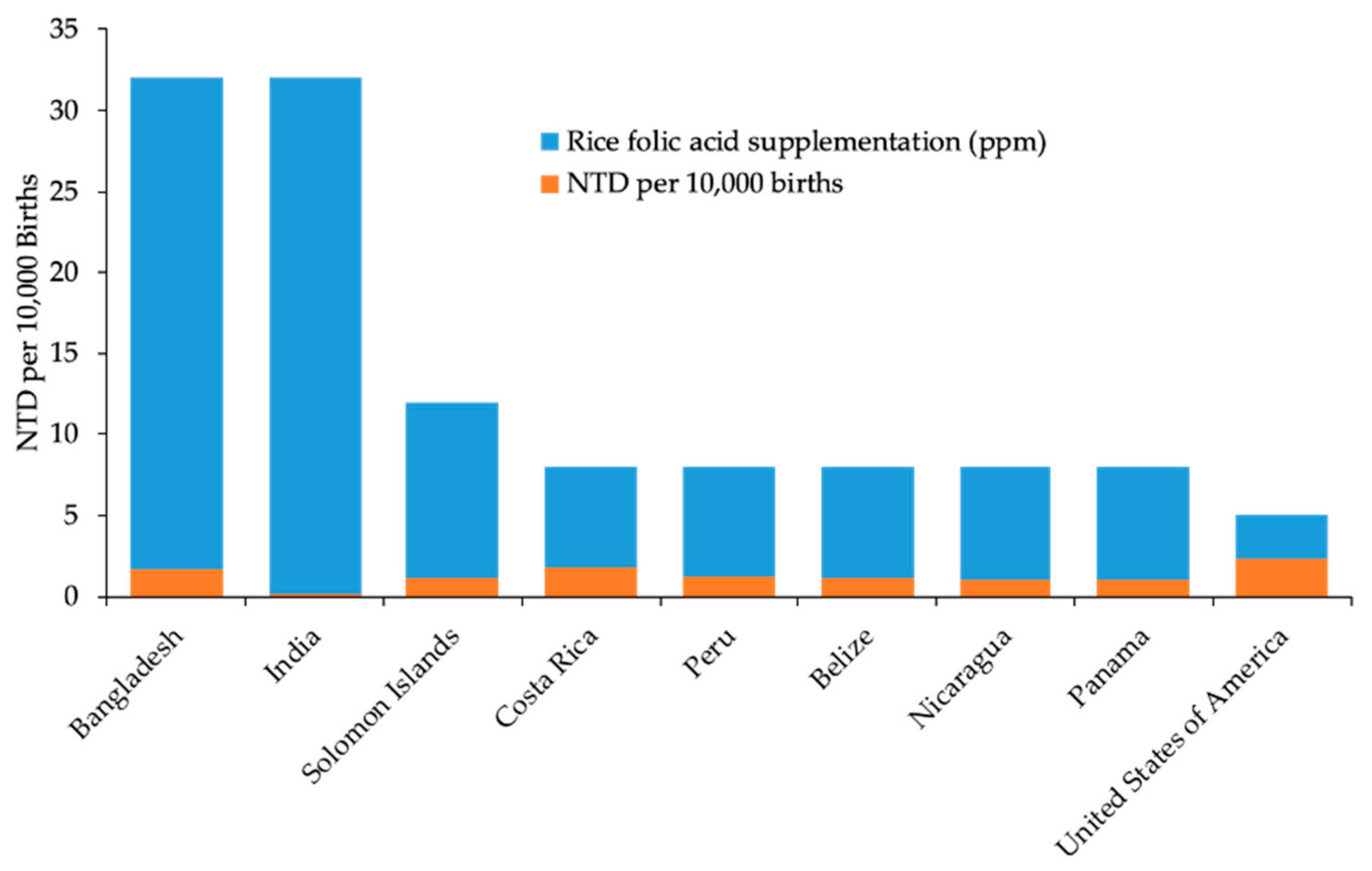
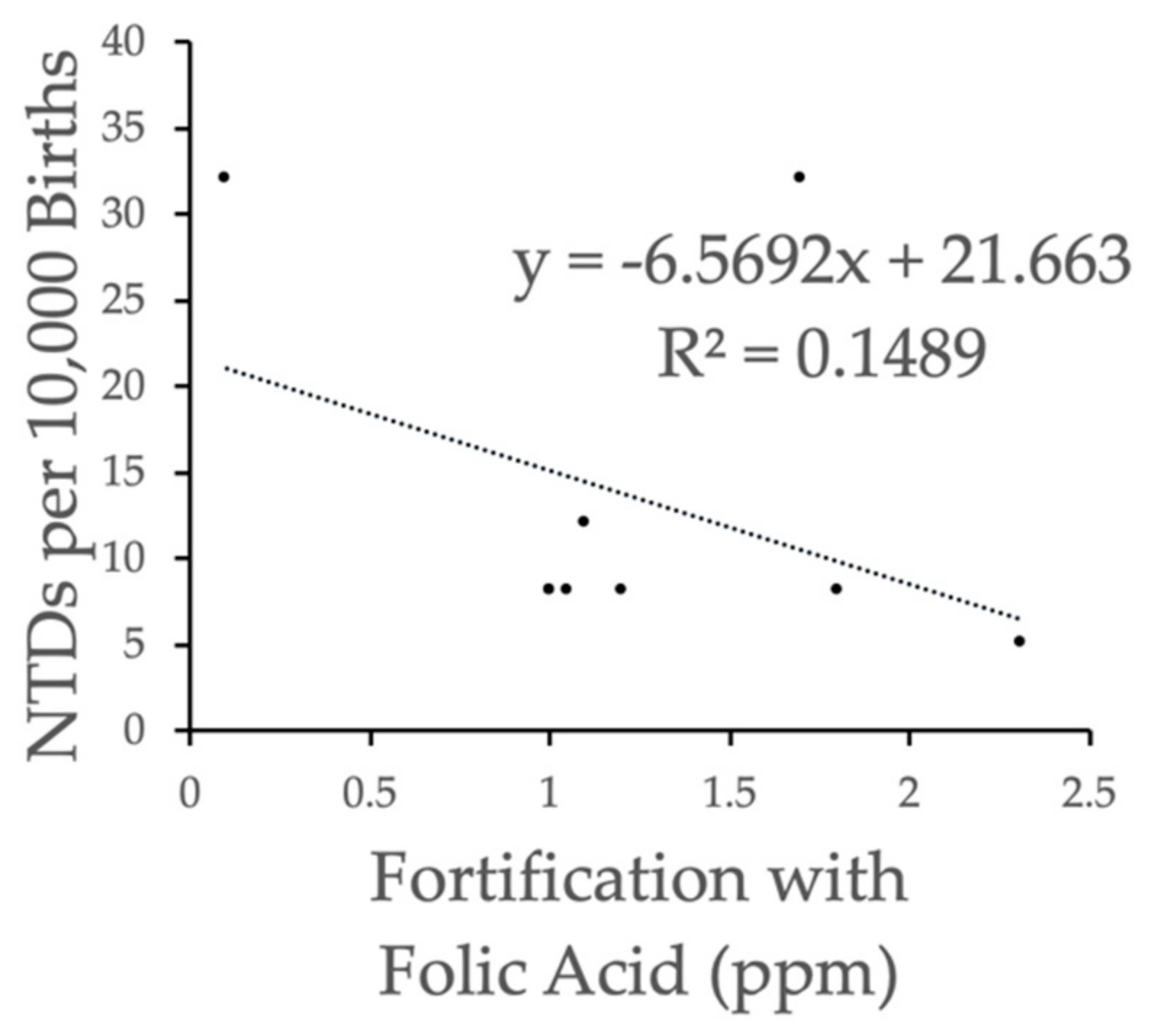
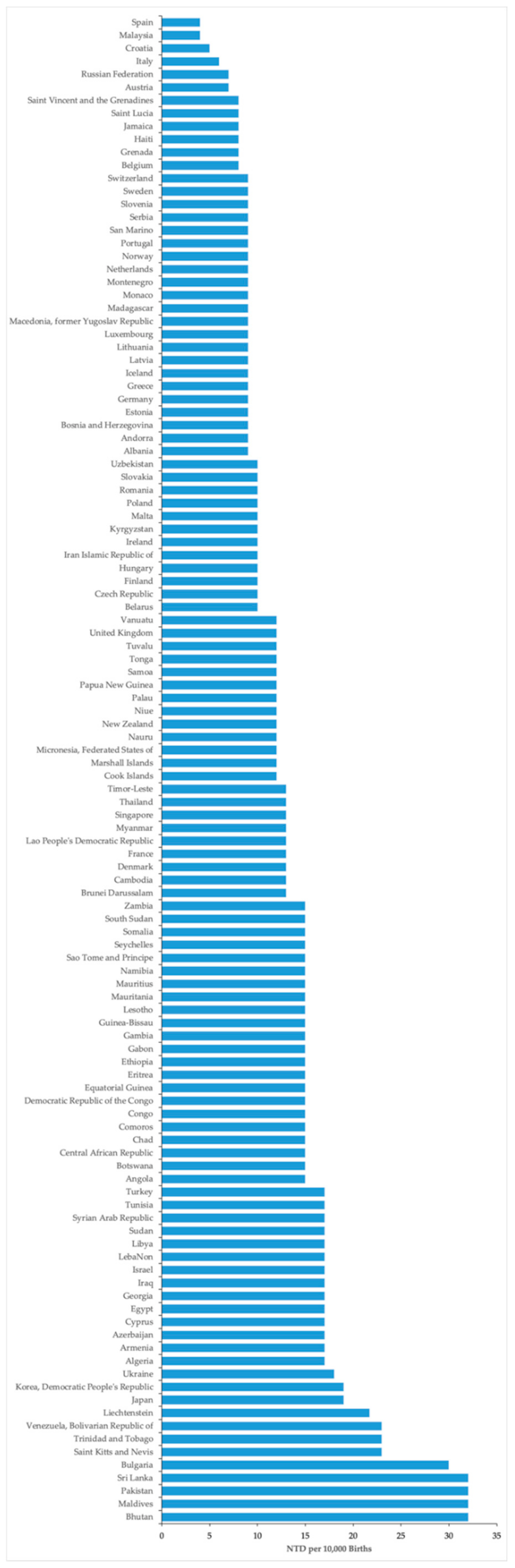
3.2. Prevalence of NTDs as a Function of Folic Acid Fortification in the FFI Dataset
3.3. Prevalence of NTDs after Stratification of the Data Based on Socioeconomic Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blount, J.P.; George, T.M.; Koueik, J.; Iskandar, B.J. Concepts in the neurosurgical care of patients with spinal neural tube defects: An embryologic approach. Birth Defects Res. 2019, 111, 1564–1576. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control (CDC). Economic burden of spina bifida—United States 1980–1990. MMWR 1989, 38, 264–267. [Google Scholar]
- Crider, K.S.; Bailey, L.B.; Berry, R.J. Folic acid food fortification-its history, effect, concerns, and future directions. Nutrients 2011, 3, 370–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Recommendations for the use of folic acid to reduce the number of cases of spina bifida and other neural tube defects. MMWR 1992, 41, 1–7. [Google Scholar]
- Choumenkovitch, S.F.; Selhub, J.; Wilson, P.W.; Rader, J.I.; Rosenberg, I.H.; Jacques, P.F. Folic acid intake from fortification in United States exceeds predictions. J. Nutr. 2002, 132, 2792–2798. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Food standards: Amendment of standards to identify for enriched grain products to require addition of folic acid. Final rule. Fed. Regist. 1996, 61, 8781–8797. [Google Scholar]
- Allen, L.H.; Miller, J.W.; de Groot, L.; Rosenberg, I.H.; Smith, A.D.; Refsum, H.; Raiten, D.J. Biomarkers of nutrition for development (BOND): Vitamin B-12 review. J. Nutr. 2018, 148, 1995S–2027S. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, C.M.; Hughes, J.P.; Lacher, D.A.; Bailey, R.L.; Berry, R.J.; Zhang, M.; Yetley, E.A.; Rader, J.I.; Sempos, C.T.; Johnson, C.L.; et al. Estimation of trends in serum and RBC folate in the U.S. population from pre- to postfortification using assay-adjusted data from the NHANES 1988–2010. J. Nutr. 2012, 142, 886–893. [Google Scholar] [CrossRef]
- Boo, N.Y.; Cheah, I.G.; Thong, M.K. Neural tube defects in Malaysia: Data from the Malaysian National Neonatal Registry. J. Trop. Pediatr. 2013, 59, 338–342. [Google Scholar] [CrossRef] [Green Version]
- Alasfoor, D.; Elsayed, M.K.; Mohammed, A.J. Spina bifida and birth outcome before and after fortification of flour with iron and folic acid in Oman. East. Mediterr. Health J. 2010, 16, 533–538. [Google Scholar] [CrossRef]
- Blencowe, H.; (London School of Hygiene & Tropical Medicine, London, UK). Personal Communication, 2015.
- Neural Tube Defect Ascertainment Project. National Birth Defects Prevention: Birth Defects Surveillance, Research, and Prevention. United States. Available online: http://www.Nbdpn.org/current/2010pdf/NTD%20fact%20sheet%2001-10%20for%20website.Pdf (accessed on 6 November 2019).
- March of Dimes. Global Report on Birth Defects-the Hidden Toll of Dying and Disabled Children. United States of America. 2006. Available online: https://www.Marchofdimes.org/global-Report-on-Birth-Defects-the-Hidden-Toll-of-Dying-and-Disabled-Children-Full-Report.Pdf (accessed on 6 November 2019).
- Centers for Disease Control and Prevention (CDC). CDC grand rounds: Additional opportunities to prevent neural tube defects with folic acid fortification. MMWR 2010, 59, 980–984. [Google Scholar]
- Berry, R.J.; Bailey, L.; Mulinare, J.; Bower, C.; Folic Acid Working Group. Fortification of flour with folic acid. Food Nutr. Bull. 2010, 31, S22–S35. [Google Scholar] [CrossRef] [PubMed]
- Arth, A.; Kancherla, V.; Pachon, H.; Zimmerman, S.; Johnson, Q.; Oakley, G.P., Jr. A 2015 global update on folic acid-preventable spina bifida and anencephaly. Birth Defects Res. Clin. Mol. Teratol. 2016, 106, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.J.; Mai, C.T.; Edmonds, L.D.; Shaw, G.M.; Kirby, R.S.; Hobbs, C.A.; Sever, L.E.; Miller, L.A.; Meaney, F.J.; Levitt, M.; et al. Prevalence of spina bifida and anencephaly during the transition to mandatory folic acid fortification in the United States. Teratology 2002, 66, 33–39. [Google Scholar] [CrossRef]
- De Wals, P.; Tairou, F.; Van Allen, M.I.; Uh, S.H.; Lowry, R.B.; Sibbald, B.; Evans, J.A.; Van den Hof, M.C.; Zimmer, P.; Crowley, M.; et al. Reduction in neural-tube defects after folic acid fortification in Canada. N. Engl. J. Med. 2007, 357, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Hertrampf, E.; Cortes, F. Folic acid fortification of wheat flour: Chile. Nutr. Rev. 2004, 62, S44–S49. [Google Scholar] [CrossRef]
- Atta, C.A.; Fiest, K.M.; Frolkis, A.D.; Jette, N.; Pringsheim, T.; St Germaine-Smith, C.; Rajapakse, T.; Kaplan, G.G.; Metcalfe, A. Global birth prevalence of spina bifida by folic acid fortification status: A systematic review and meta-analysis. Am. J. Public Health 2016, 106, e24–e34. [Google Scholar] [CrossRef]
- March of Dimes. Executive Summary March of Dimes Global Report on Birth Defects the Hidden Toll; March of Dimes Birth Defects Foundation: White Plains, NY, USA, 2006. [Google Scholar]
- Kancherla, V.; Wagh, K.; Johnson, Q.; Oakley, G.P., Jr. A 2017 global update on folic acid-preventable spina bifida and anencephaly. Birth Defects Res. 2018, 110, 1139–1147. [Google Scholar] [CrossRef]
- Centers for Disease Control (CDC). Spina bifida incidence at birth—United States, 1983–1990. MMWR 1992, 41, 497–500. [Google Scholar]
- Reynolds, E.H. What is the safe upper intake level of folic acid for the nervous system? Implications for folic acid fortification policies. Eur. J. Clin. Nutr. 2016, 70, 537–540. [Google Scholar] [CrossRef]
- Ray, J.G. Efficacy of Canadian folic acid food fortification. Food Nutr. Bull. 2008, 29, S225–S230. [Google Scholar] [CrossRef] [PubMed]
- Ray, J.G. Folic acid food fortification in Canada. Nutr. Rev. 2004, 62, S35–S39. [Google Scholar] [CrossRef] [PubMed]
- Centeno Tablante, E.; Pachon, H.; Guetterman, H.M.; Finkelstein, J.L. Fortification of wheat and maize flour with folic acid for population health outcomes. Cochrane Database Syst. Rev. 2019, 7, CD012150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee on Medical Aspects of Food and Nutrition Policy (COMA). Folic Acid and the Prevention of Disease; The Stationary Office: London, UK, 2000. [Google Scholar]
- Marks, K.J.; Luthringer, C.L.; Ruth, L.J.; Rowe, L.A.; Khan, N.A.; De-Regil, L.M.; Lopez, X.; Pachon, H. Review of grain fortification legislation, standards, and monitoring documents. Glob. Health Sci. Pract. 2018, 6, 356–371. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Trends in wheat-flour fortification with folic acid and iron—Worldwide, 2004 and 2007. MMWR 2008, 57, 8–10. [Google Scholar]
- Morris, M.S.; Jacques, P.F.; Rosenberg, I.H.; Selhub, J. Folate and vitamin B-12 status in relation to anemia, macrocytosis, and cognitive impairment in older Americans in the age of folic acid fortification. Am. J. Clin. Nutr. 2007, 85, 193–200. [Google Scholar] [CrossRef]
- Morris, M.C.; Evans, D.A.; Bienias, J.L.; Tangney, C.C.; Hebert, L.E.; Scherr, P.A.; Schneider, J.A. Dietary folate and vitamin B12 intake and cognitive decline among community-dwelling older persons. Arch. Neurol. 2005, 62, 641–645. [Google Scholar] [CrossRef] [Green Version]
- Moore, E.M.; Ames, D.; Mander, A.G.; Carne, R.P.; Brodaty, H.; Woodward, M.C.; Boundy, K.; Ellis, K.A.; Bush, A.I.; Faux, N.G.; et al. Among vitamin B12 deficient older people, high folate levels are associated with worse cognitive function: Combined data from three cohorts. J. Alzheimers Dis. 2014, 39, 661–668. [Google Scholar] [CrossRef]
- Faux, N.G.; Ellis, K.A.; Porter, L.; Fowler, C.J.; Laws, S.M.; Martins, R.N.; Pertile, K.K.; Rembach, A.; Rowe, C.C.; Rumble, R.L.; et al. Homocysteine, vitamin B12, and folic acid levels in Alzheimer’s disease, mild cognitive impairment, and healthy elderly: Baseline characteristics in subjects of the Australian imaging biomarker lifestyle Study. J. Alzheimers Dis. 2011, 27, 909–922. [Google Scholar] [CrossRef]
- Selhub, J.; Rosenberg, I.H. Excessive folic acid intake and relation to adverse health outcome. Biochimie 2016, 126, 71–78. [Google Scholar] [CrossRef]
- Sawaengsri, H.; Bergethon, P.R.; Qiu, W.Q.; Scott, T.M.; Jacques, P.F.; Selhub, J.; Paul, L. Transcobalamin 776C–G polymorphism is associated with peripheral neuropathy in elderly individuals with high folate intake. Am. J. Clin. Nutr. 2016, 104, 1665–1670. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cereal Grain Fortified | Number of Countries | Average Fortification Level (ppm) ± Standard Deviation 1 | Range of Fortification (ppm) 2 |
|---|---|---|---|
| Wheat | 68 | 1.94 (0.75) | 0.1–5.11 |
| Maize | 17 | 1.52 (0.50) | 0.5–2.6 |
| Rice | 9 | 1.25 (0.63) | 0.1–2.31 |
| None | 116 | n/a | n/a |
| Cereal Grain Fortified | n | Average Number of NTDs per 10,000 Births 1 | p2 | Regression Coefficient 3 | 95% CI 4 |
|---|---|---|---|---|---|
| Wheat | 68 | 13.07 (5.76) | 0.78 | −1.07 | −1.44–1.94 |
| Maize | 17 | 10.76 (3.44) | 0.065 | −1.15 | −0.16–5.28 |
| Rice | 9 | 13.44 (10.67) | 0.95 | −6.57 | −4.21–3.97 |
| None | 116 | 13.32 (5.50) | n/a | n/a | n/a |
| SES Quintile 1 | N | Average NTDs With Fortification 2,3 | N | Average NTDs Without Fortification 2,3 | p4 |
|---|---|---|---|---|---|
| 1 | 10 | 8.90 (2.81) | 27 | 11.74 (5.22) | 0.11 |
| 2 | 15 | 10.87 (5.15) | 22 | 12.45 (5.64) | 0.39 |
| 3 | 19 | 13.11 (3.33) | 18 | 10.50 (3.59) | 0.03 |
| 4 | 16 | 15.38 (7.14) | 21 | 16.19 (5.69) | 0.70 |
| 5 | 9 | 16.90 (6.74) | 24 | 15.82 (6.49) | 0.68 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murphy, M.E.; Westmark, C.J. Folic Acid Fortification and Neural Tube Defect Risk: Analysis of the Food Fortification Initiative Dataset. Nutrients 2020, 12, 247. https://doi.org/10.3390/nu12010247
Murphy ME, Westmark CJ. Folic Acid Fortification and Neural Tube Defect Risk: Analysis of the Food Fortification Initiative Dataset. Nutrients. 2020; 12(1):247. https://doi.org/10.3390/nu12010247
Chicago/Turabian StyleMurphy, Michaela E., and Cara J. Westmark. 2020. "Folic Acid Fortification and Neural Tube Defect Risk: Analysis of the Food Fortification Initiative Dataset" Nutrients 12, no. 1: 247. https://doi.org/10.3390/nu12010247
APA StyleMurphy, M. E., & Westmark, C. J. (2020). Folic Acid Fortification and Neural Tube Defect Risk: Analysis of the Food Fortification Initiative Dataset. Nutrients, 12(1), 247. https://doi.org/10.3390/nu12010247