Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region

 ,
, 

 ,
,  ,
,  ,
,  , , ,
, , , 
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Recruitment
2.2. Validation Protocol
2.3. Statistical Methods
3. Results
3.1. Characteristics of the Participants
3.2. Validation of the FFQ-MEDAS against 3d-FD in the Selected Countries: Reliability, Correlation, and Agreement
3.3. Kappa Statistics: Analysis Per Food-Item and Country
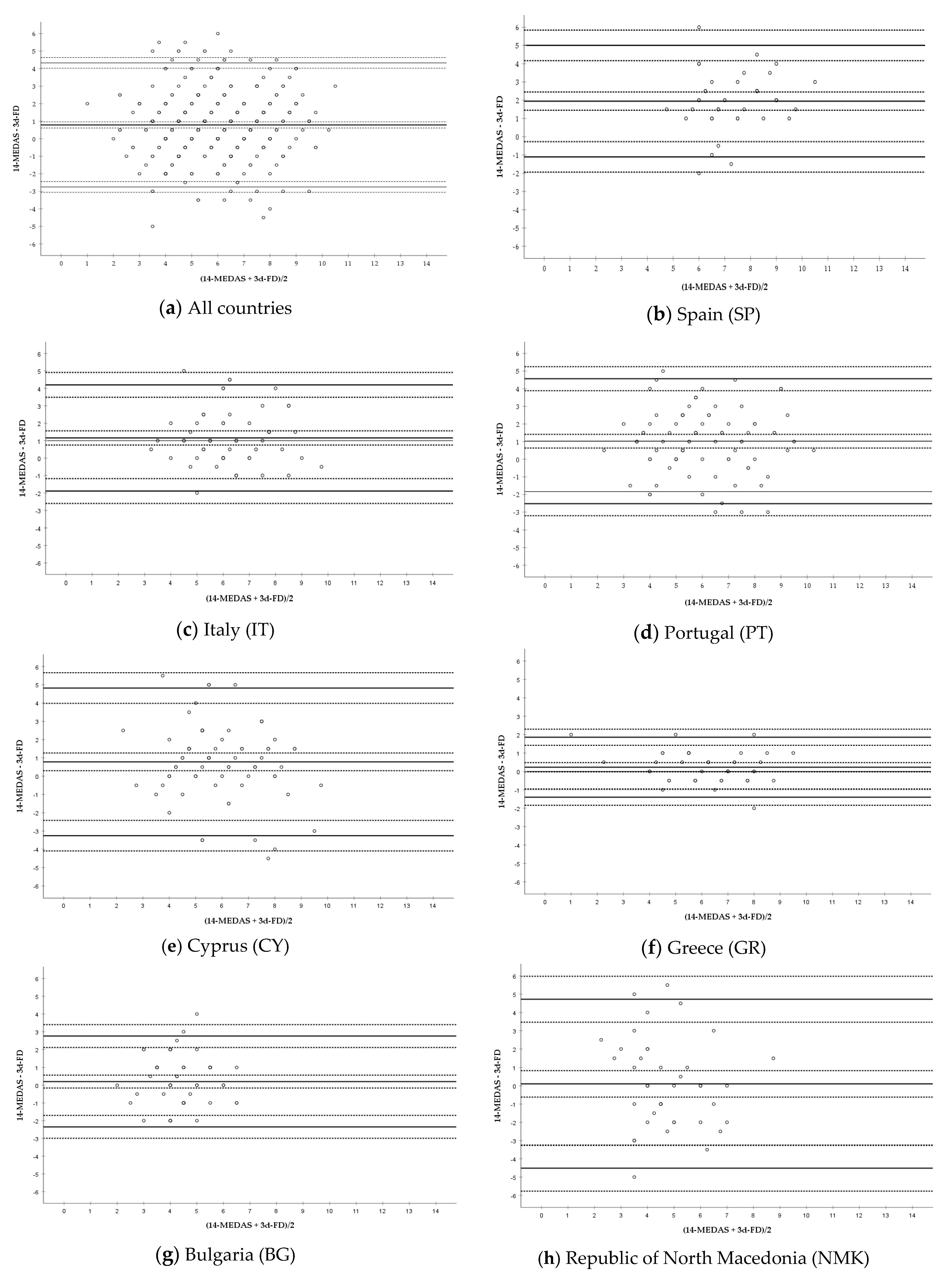
3.4. Bland–Altman Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Godos, J.; Galvano, F. Insights on Mediterranean Diet from the SUN Cohort: Cardiovascular and Cognitive Health. Nutrients 2020, 12, 1332. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trichopoulou, A.; Martinez-Gonzalez, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Hidalgo-Mora, J.J.; Garcia-Vigara, A.; Sanchez-Sanchez, M.L.; Garcia-Perez, M.A.; Tarin, J.; Cano, A. The Mediterranean diet: A historical perspective on food for health. Maturitas 2020, 132, 65–69. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Hebestreit, K.; Yahiaoui-Doktor, M.; Engel, C.; Vetter, W.; Siniatchkin, M.; Erickson, N.; Halle, M.; Kiechle, M.; Bischoff, S.C. Validation of the German version of the Mediterranean Diet Adherence Screener (MEDAS) questionnaire. BMC Cancer 2017, 17, 341. [Google Scholar] [CrossRef]
- Bottcher, M.R.; Marincic, P.Z.; Nahay, K.L.; Baerlocher, B.E.; Willis, A.W.; Park, J.; Gaillard, P.; Greene, M.W. Nutrition knowledge and Mediterranean diet adherence in the southeast United States: Validation of a field-based survey instrument. Appetite 2017, 111, 166–176. [Google Scholar] [CrossRef]
- Papadaki, A.; Johnson, L.; Toumpakari, Z.; England, C.; Rai, M.; Toms, S.; Penfold, C.; Zazpe, I.; Martinez-Gonzalez, M.A.; Feder, G. Validation of the English Version of the 14-Item Mediterranean Diet Adherence Screener of the PREDIMED Study, in People at High Cardiovascular Risk in the UK. Nutrients 2018, 10, 138. [Google Scholar] [CrossRef] [Green Version]
- Kwon, Y.J.; Lee, H.; Yoon, Y.; Kim, H.M.; Chu, S.H.; Lee, J.W. Development and Validation of a Questionnaire to Measure Adherence to the Mediterranean Diet in Korean Adults. Nutrients 2020, 12, 1102. [Google Scholar] [CrossRef] [Green Version]
- Mahdavi-roshan, M.; Salari, A.; Ggholipour, M.; Naghshbandi, M. Dietary Adherence in People with Cardiovascular Risk Factors Living in Northern Iran. J. Babol Univ. Med. Sci. 2017, 19, 62–68. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Draga, D.; Misotti, A.M.; Sieri, S.; Spaggiari, L.; Cassano, E.; Baldini, F.; Soldati, L.; Maisonneuve, P. Validation of a short questionnaire to record adherence to the Mediterranean diet: An Italian experience. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Abu-Saad, K.; Endevelt, R.; Goldsmith, R.; Shimony, T.; Nitsan, L.; Shahar, D.R.; Keinan-Boker, L.; Ziv, A.; Kalter-Leibovici, O. Adaptation and predictive utility of a Mediterranean diet screener score. Clin. Nutr. 2019, 38, 2928–2935. [Google Scholar] [CrossRef] [PubMed]
- Gregorio, M.J.; Rodrigues, A.M.; Salvador, C.; Dias, S.S.; de Sousa, R.D.; Mendes, J.M.; Coelho, P.S.; Branco, J.C.; Lopes, C.; Martinez-Gonzalez, M.A.; et al. Validation of the Telephone-Administered Version of the Mediterranean Diet Adherence Screener (MEDAS) Questionnaire. Nutrients 2020, 12, 1511. [Google Scholar] [CrossRef] [PubMed]
- Bibiloni, M.D.M.; González, M.; Julibert, A.; Llompart, I.; Pons, A.; Tur, J.A. Ten-Year Trends (1999–2010) of Adherence to the Mediterranean Diet among the Balearic Islands’ Adult Population. Nutrients 2017, 9, 749. [Google Scholar] [CrossRef] [Green Version]
- Marventano, S.; Godos, J.; Platania, A.; Galvano, F.; Mistretta, A.; Grosso, G. Mediterranean diet adherence in the Mediterranean healthy eating, aging and lifestyle (MEAL) study cohort. Int. J. Food Sci. Nutr. 2018, 69, 100–107. [Google Scholar] [CrossRef]
- Januszewska, R.; Pieniak, Z.; Verbeke, W. Food choice questionnaire revisited in four countries. Does it still measure the same? Appetite 2011, 57, 94–98. [Google Scholar] [CrossRef]
- Briers, B.; Huh, Y.E.; Chan, E.; Mukhopadhyay, A. The unhealthy = tasty belief is associated with BMI through reduced consumption of vegetables: A cross-national and mediational analysis. Appetite 2020, 150, 104639. [Google Scholar] [CrossRef]
- Watson, P.F.; Petrie, A. Method agreement analysis: A review of correct methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef] [Green Version]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [Green Version]
- Torres, D.; Faria, N.; Sousa, N.; Teixeira, S.; Soares, R.; Amorim, H.; Guiomar, S.; Lobato, L.; Oliveira, C.; Correia, D.; et al. Manual Fotográfico de Quantificação de Alimentos IAN-AF 2015–2016; Universidade do Porto: Porto, Portugal, 2017; ISBN 978-989-746-182-8. [Google Scholar]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. Zagreb 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. Zagreb 2015, 25, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Flegal, K.M.; Graubard, B.; Ioannidis, J.P.A. Use and reporting of Bland–Altman analyses in studies of self-reported versus measured weight and height. Int. J. Obes. 2020, 44, 1311–1318. [Google Scholar] [CrossRef]
- World Health Organization. Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Zaragoza-Marti, A.; Cabanero-Martinez, M.J.; Hurtado-Sanchez, J.A.; Laguna-Perez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ Open 2018, 8, e019033. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.J.; Kim, M.K.; Hwang, S.H.; Ahn, Y.; Shim, J.E.; Kim, D.H. Relative validities of 3-day food records and the food frequency questionnaire. Nutr. Res. Pract. 2010, 4, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth 2017, 11, S80–S89. [Google Scholar] [CrossRef]
- Dogan, N.O. Bland-Altman analysis: A paradigm to understand correlation and agreement. Turk. J. Emerg. Med. 2018, 18, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Caparello, G.; Galluccio, A.; Giordano, C.; Lofaro, D.; Barone, I.; Morelli, C.; Sisci, D.; Catalano, S.; Andò, S.; Bonofiglio, D. Adherence to the Mediterranean diet pattern among university staff: A cross-sectional web-based epidemiological study in Southern Italy. Int. J. Food Sci. Nutr. 2020, 71, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Theodoridis, X.; Grammatikopoulou, M.G.; Gkiouras, K.; Papadopoulou, S.E.; Agorastou, T.; Gkika, I.; Maraki, M.I.; Dardavessis, T.; Chourdakis, M. Food insecurity and Mediterranean diet adherence among Greek university students. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 477–485. [Google Scholar] [CrossRef]
- Nelson, M. The validation of dietary assessment. In Design Concepts in Nutritional Epidemiology; Margetts, B., Nelson, M., Eds.; Oxford Scholarship: London, UK, 1997; pp. 241–721. [Google Scholar] [CrossRef]
- Subar, A.F.; Kipnis, V.; Troiano, R.P.; Midthune, D.; Schoeller, D.A.; Bingham, S.; Sharbaugh, C.O.; Trabulsi, J.; Runswick, S.; Ballard-Barbash, R.; et al. Using intake biomarkers to evaluate the extent of dietary misreporting in a large sample of adults: The OPEN study. Am. J. Epidemiol. 2003, 158, 1–13. [Google Scholar] [CrossRef]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 h recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101 (Suppl. 2), S73–S85. [Google Scholar] [CrossRef] [Green Version]
- Ravelli, M.N.; Schoeller, D.A. Traditional Self-Reported Dietary Instruments Are Prone to Inaccuracies and New Approaches Are Needed. Front. Nutr. 2020, 7, 90. [Google Scholar] [CrossRef]
- Sofi, F.; Dinu, M.; Pagliai, G.; Cesari, F.; Gori, A.M.; Sereni, A.; Becatti, M.; Fiorillo, C.; Marcucci, R.; Casini, A. Low-Calorie Vegetarian Versus Mediterranean Diets for Reducing Body Weight and Improving Cardiovascular Risk Profile: CARDIVEG Study (Cardiovascular Prevention with Vegetarian Diet). Circulation 2018, 137, 1103–1113. [Google Scholar] [CrossRef]
- Scholz, A.; Navarrete-Muñoz, E.M.; de la Hera, M.G.; Gimenez-Monzo, D.; Gonzalez-Palacios, S.; Valera-Gran, D.; Torres-Collado, L.; Vioque, J. Alcohol consumption and Mediterranean Diet adherence among health science students in Spain: The DiSA-UMH Study. Gac. Sanit. 2016, 30, 126–132. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| All Countries | SP | IT | PT | CY | GR | NMK | BG | |
|---|---|---|---|---|---|---|---|---|
| N (%) | 402 | 40 (10.0) | 58 (14.4) | 86 (21.4) | 72 (17.9) | 44 (10.9) | 43 (10.7) | 59 (14.7) |
| Sex distribution: | ||||||||
| Women; N (%) | 238 (59.2) | 23 (57.5) | 34 (58.6) | 57 (66.3) | 38 (52.8) | 25 (56.8) | 25 (58.1) | 36 (61.0) |
| Men; N (%) | 164 (40.8) | 17 (42.5) | 24 (41.4) | 29 (33.7) | 34 (47.2) | 19 (43.2) | 18 (41.9) | 23 (39.0) |
| Age range (years) | 18–81 | 24–71 | 19–65 | 19–73 | 20–74 | 18–80 | 20–81 | 20–80 |
| Age mean ± SD (years) | 39.4 ±15.2 | 45.9 ± 11 | 36.1 ±13.5 | 34.2 ±14.1 | 35.0 ± 15 | 34.3 ±12.0 | 46.3 ±16.2 | 49.9 ±14.6 |
| Age distribution N (%) | ||||||||
| 18–24 (years) | 85 (21.1) | 1 (2.5) | 18 (31.0) | 29 (33.7) | 28 (38.9) | 6 (13.6) | 2 (4.7) | 1 (1.7) |
| 25–34 (years) | 104 (25.9) | 6 (15.0) | 12 (20.7) | 26 (30.2) | 14 (19.4) | 26 (59.1) | 11 (25.6) | 9 (15.3) |
| 35–44 (years) | 75 (18.7) | 14 (35.0) | 8 (13.8) | 8 (9.3) | 14 (19.4) | 6 (13.6) | 10 (23.3) | 15 (25.4) |
| 45–54 (years) | 58 (14.4) | 9 (22.5) | 14 (24.1) | 12 (20.7) | 7 (9.7) | 3 (5.2) | 4 (9.3) | 9 (15.3) |
| 55–64 (years) | 47 (11.7) | 8 (20.0) | 5 (8.6) | 7 (8.1) | 2 (2.8) | 1 (2.3) | 10 (23.3) | 14 (23.7) |
| ≥65 (years) | 33 (8.2) | 2 (5.0) | 1 (1.7) | 4 (4.7) | 7 (9.7) | 2 (4.5) | 6 (14.0) | 11 (18.8) |
| BMI (kg/m2) | ||||||||
| mean ± SD | 25.2 ± 5.0 | 23.4 ± 2.6 | 23.3 ± 3.1 | 24.0 ± 3.6 | 24.9 ± 4.7 | 25.9 ± 5.6 | 26.9 ± 4.9 | 28.5 ± 7.3 |
| BMI distribution 1 N (%) | ||||||||
| Underweight | 9 (2.2) | 1 (2.5) | 1 (1.7) | 1 (1.2) | 1 (1.4) | 0 (0.0) | 1 (2.3) | 2 (3.4) |
| Normal weight | 223 (55.5) | 27 (67.5) | 44 (75.9) | 54 (63.5) | 42 (58.3) | 23 (52.3) | 15 (34.9) | 20 (33.9) |
| Overweight | 113 (28.1) | 11 (27.5) | 12 (20.7) | 24 (28.2) | 20 (27.8) | 13 (29.6) | 17 (39.5) | 15 (25.4) |
| Obesity | 57 (14.2) | 1 (2.5) | 1 (1.7) | 6 (7.1) | 9 (12.5) | 8 (18.2) | 10 (23.3) | 22 (37.3) |
| Weight excess (overweight + obesity) | 170 (42.3) | 12 (30.0) | 13 (22.4) | 30 (35.3) | 29 (40.3) | 21 (47.8) | 27 (62.8) | 37 (62.7) |
| N (Valid Population) 1 | FFQ-MEDAS 2 (1) FFQ-MEDAS (2) | Test–Retest Reliability 3 (r, Sig. Bilateral) | FFQ-MEDAS (Mean Score) | 3d-FD Score | Correlation 4 (r, Sig. Bilateral) | ICC 5 (95%CI, Sig. Bilateral) |
|---|---|---|---|---|---|---|
| All countries (402) | (1) 6.22 ± 2.03 (2) 6.21 ± 2.14 | 0.852, <0.001 Strong positive correlation | 6.22 ± 2.01 | 5.43 ± 1.89 | 0.573, <0.001 Moderate positive correlation | 0.692 (0.552, 0.780; <0.001) Moderate |
| SP (40) | (1) 8.15 ± 1.73 (2) 8.55 ± 1.71 | 0.837, <0.001 Strong positive correlation | 8.35 ± 1.65 | 6.40 ± 1.46 | 0.503, 0.001 Moderate positive correlation | 0.440 (−0.210, 0.745; <0.001) Poor |
| IT (58) | (1) 6.90 ± 1.68 (2) 6.83 ± 1.74 | 0.809, <0.001 Strong positive correlation | 6.86 ± 1.63 | 5.71 ± 1.63 | 0.546, <0.001 Moderate positive correlation | 0.610 (0.150, 0.802; <0.001) Moderate |
| PT (86) | (1) 6.54 ± 2.04 (2) 6.55 ± 2.10 | 0.827, <0.001 Strong positive correlation | 6.55 ± 1.98 | 5.52 ± 2.02 | 0.597, <0.001 Moderate positive correlation | 0.693 (0.420, 0.824; <0.001) Moderate |
| CY (72) | (1) 6.33 ± 1.90 (2) 6.32 ± 2.03 | 0.623, <0.001 Moderate positive correlation | 6.33 ± 1.77 | 5.54 ± 2.06 | 0.427, <0.001 Moderate positive correlation | 0.564 (0.299, 0.728; <0.001) Moderate |
| GR (44) | (1) 6.41 ± 1.67 (2) 6.23 ± 1.83 | 0.842, <0.001 Strong positive correlation | 6.32 ± 1.68 | 6.09 ± 1.87 | 0.895, <0.001 Strong positive correlation | 0.939 (0.887, 0.967: <0.001) Excellent |
| NMK (43) | (1) 4.93 ± 1.62 (2) 4.67 ± 1.76 | 0.919, <0.001 Strong positive correlation | 4.80 ± 1.66 | 4.70 ± 1.91 | 0.131, 0.401 No correlation | 0.234 (−0.434, 0.588; 0.200) No agreement |
| BG (59) | (1) 4.46 ± 1.21 (2) 4.49 ± 1.21 | 0.930, <0.001 Strong positive correlation | 4.47 ± 1.19 | 4.27 ± 1.19 | 0.311, 0.016 Weak correlation | 0.473 (0.118, 0.686; 0.008) Poor |
| Question (Score) | All Countries | SP | IT | PT | CY | GR | NMK | BG |
|---|---|---|---|---|---|---|---|---|
| 1. Olive oil (yes) | 0.590 Moderate | NA 1 | NA | 0.133 Slight | −0.003 No agreement | NA | 0.225 Fair | 0.871 Almost perfect |
| 2. Olive oil (≥4) | 0.361 Fair | 0.228 Fair | −0.063 No agreement | 0.390 Fair | −0.084 No agreement | 0.488 Moderate | NA | −0.017 No agreement |
| 3. Vegetables (≥2) | 0.184 Slight | 0.000 No agreement | 0.419 Moderate | 0.252 Fair | 0.222 Fair | 0.485 Moderate | 0.166 Slight | NA |
| 4. Fruits (≥3) | 0.502 Moderate | 0.459 Moderate | 0.181 Slight | 0.549 Moderate | 0.391 Fair | 0.560 Moderate | −0.042 No agreement | NA |
| 5. Red meat (<1) | 0.114 Slight | −0.080 No agreement | 0.110 Slight | −0.228 Disagreement | NA | 0.440 Moderate | 0.557 Moderate | NA |
| 6. Butter (<1) | 0.257 Fair | 0.655 Substantial | 0.270 Fair | 0.124 Slight | 0.030 Slight | 0.455 Moderate | −0.307 Disagreement | 0.168 Slight |
| 7. Sweet drinks (<1) | 0.281 Fair | 0.362 Fair | 0.097 Slight | 0.449 Moderate | 0.003 No agreement | 0.307 Fair | 0.125 Slight | 0.140 Slight |
| 8. Wine (7 to 14) | 0.391 Fair | 0.538 Moderate | 0.545 Moderate | 0.223 Fair | NA | 0.116 Slight | 0.482 Moderate | 0.676 Substantial |
| 9. Legumes (≥3) | 0.264 Fair | 0.275 Fair | 0.467 Moderate | 0.124 Slight | 0.126 Slight | 0.540 Moderate | −0.116 Disagreement | NA |
| 10. Fish (≥3) | 0.239 Fair | 0.366 Fair | 0.098 Slight | 0.126 Slight | 0.099 Slight | 0.340 Fair | −0.040 No agreement | NA |
| 11. Desserts (<3) | 0.333 Fair | 0.498 Moderate | 0.446 Moderate | 0.268 Fair | 0.035 Slight | 0.035 Slight | 0.094 Slight | NA |
| 12. Nuts (≥3) | 0.403 Fair to moderate | 0.659 Substantial | 0.268 Fair | 0.361 Fair | 0.300 Fair | 0.836 Almost perfect | 0.055 Slight | NA |
| 13. White meat (≤1 or yes) | 0.234 Fair | 0.050 Slight | 0.242 Fair | 0.298 Fair | 0.222 Fair | 0.690 Substantial | 0.073 Slight | 0.050 Slight |
| 14. ‘Sofrito’ (≥2) | 0.204 Slight to fair | 0.050 Slight | 0.190 Slight | −0.024 No agreement | 0.062 Slight | 0.919 Almost perfect | 0.206 Fair | NA |
| Country (N) 1 | Bland–Altman Analysis | |||
|---|---|---|---|---|
| Mean Difference 2 (Bias) ± SD (95% CI) | Upper LOA (95% CI) | Lower LOA (95% CI) | Fitted Linear Regression (Sig. Bilateral) | |
| All countries (402) | 0.79 ± 1.81 (0.61, 0.96) | 4.33 (4.02, 4.63) | −2.75 (−3.06, −2.45) | y = 0.35 + 0.08x (0.150) |
| SP (40) | 1.95 ± 1.56 (1.45, 2.45) | 5.01 (4.17, 5.84) | −1.11 (−1.94, −0.27) | y = 0.78 + 0.16x (0·399) |
| IT (58) | 1.16 ± 1.55 (0.75, 1.56) | 4.20 (3.49, 4.91) | −1.89 (−2.60, −1.18) | y = 1.19 − 0.01x (0·974) |
| PT (86) | 1.02 ± 1.81 (0.64, 1.41) | 4.57 (3.89, 5.25) | −2.52 (−3.20, −1.84) | y = 1.79 − 0.03x (0.815) |
| CY (72) | 0.78 ± 2.06 (0.30, 1.27) | 4.82 (3.99, 5.66) | −3.25 (−4.09, −2.41) | y = 2.03 − 0.21x (0·167) |
| GR (44) | 0.23 ± 0.83 (−0.03, 0.48) | 1.86 (1.42, 2.30) | −1.40 (−1.84, −0.96) | y = 0.91 − 0.11x (0·137) |
| BG (59) | 0.20 ± 1.39 (−0.16, 0.57) | 2.76 (2.11, 3.40) | −2.35 (−3.00, −1.71) | y = 0.20 + 0.001x (0·998) |
| NMK (43) | 0.10 ± 2.36 (−0.62, 0.83) | 4.72 (3.47, 5.98) | −4.51 (−5.77, −3.26) | y = 1.30 − 0.25x (0·361) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Conesa, M.-T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients 2020, 12, 2960. https://doi.org/10.3390/nu12102960
García-Conesa M-T, Philippou E, Pafilas C, Massaro M, Quarta S, Andrade V, Jorge R, Chervenkov M, Ivanova T, Dimitrova D, et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients. 2020; 12(10):2960. https://doi.org/10.3390/nu12102960
Chicago/Turabian StyleGarcía-Conesa, María-Teresa, Elena Philippou, Christos Pafilas, Marika Massaro, Stefano Quarta, Vanda Andrade, Rui Jorge, Mihail Chervenkov, Teodora Ivanova, Dessislava Dimitrova, and et al. 2020. "Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region" Nutrients 12, no. 10: 2960. https://doi.org/10.3390/nu12102960
APA StyleGarcía-Conesa, M. -T., Philippou, E., Pafilas, C., Massaro, M., Quarta, S., Andrade, V., Jorge, R., Chervenkov, M., Ivanova, T., Dimitrova, D., Maksimova, V., Smilkov, K., Ackova, D. G., Miloseva, L., Ruskovska, T., Deligiannidou, G. E., Kontogiorgis, C. A., & Pinto, P. (2020). Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients, 12(10), 2960. https://doi.org/10.3390/nu12102960