Oral Nutrition during and after Critical Illness: SPICES for Quality of Care!

 ,
,
Abstract
:1. Introduction
2. Oral Nutrition during and after Critical Illness
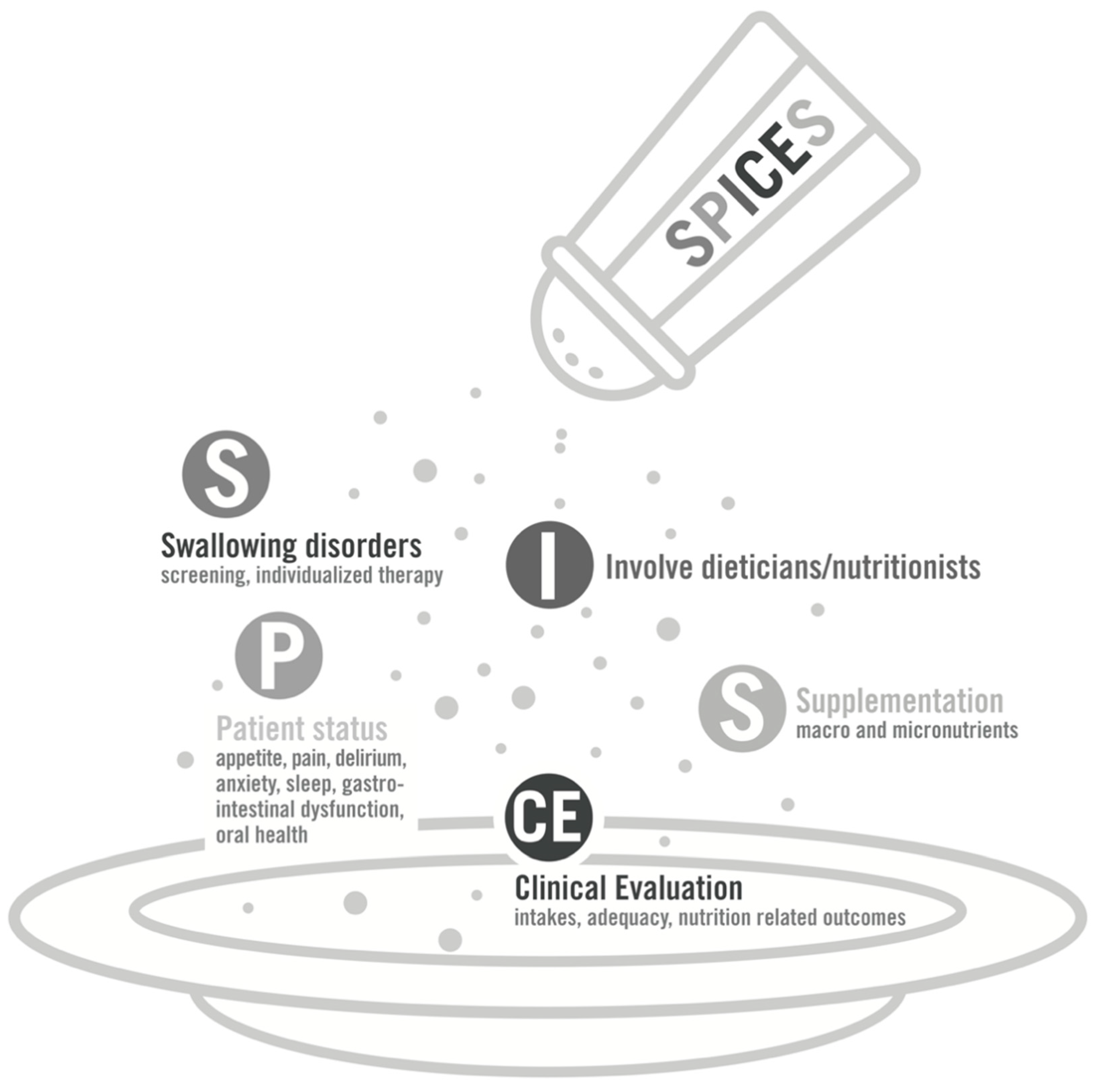
3. Strategies to Optimize Oral Nutrition during and after Critical Illness
- S: Swallowing disorders screening and management
- P: Patient global status overview
- I: Involvement of dieticians and nutritionists
- CE: Clinical Evaluation of nutritional intakes and outcomes
- S: Supplementation in macro- and/or micronutrients
4. Perspectives in Nutrition Therapy and Metabolic Support
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Viana, M.V.; Pantet, O.; Bagnoud, G.; Martinez, A.; Favre, E.; Charriere, M.; Favre, D.; Eckert, P.; Berger, M.M. Metabolic and Nutritional Characteristics of Long-Stay Critically Ill Patients. J. Clin. Med. 2019, 8, 985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casaer, M.P.; Van den Berghe, G. Nutrition in the acute phase of critical illness. N. Engl. J. Med. 2014, 370, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Dvir, D.; Cohen, J.; Singer, P. Computerized energy balance and complications in critically ill patients: An observational study. Clin. Nutr. 2006, 25, 37–44. [Google Scholar] [CrossRef]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.; Delarue, J.; Berger, M.M. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef]
- Lew, C.C.H.; Yandell, R.; Fraser, R.J.L.; Chua, A.P.; Chong, M.F.F.; Miller, M. Association between Malnutrition and Clinical Outcomes in the Intensive Care Unit: A Systematic Review. JPEN J. Parenter. Enter. Nutr. 2017, 41, 744–758. [Google Scholar] [CrossRef]
- Klein, C.J.; Stanek, G.S.; Wiles, C.E., 3rd. Overfeeding macronutrients to critically ill adults: Metabolic complications. J. Am. Diet. Assoc. 1998, 98, 795–806. [Google Scholar] [CrossRef]
- Yebenes, J.C.; Campins, L.; Martinez de Lagran, I.; Bordeje, L.; Lorencio, C.; Grau, T.; Montejo, J.C.; Bodi, M.; Serra-Prat, M.; Working Group on Nutrition and Metabolism of the Spanish Society of Critical Care. Nutritrauma: A Key Concept for Minimising the Harmful Effects of the Administration of Medical Nutrition Therapy. Nutrients 2019, 11, 1775. [Google Scholar] [CrossRef] [Green Version]
- Schulman, R.C.; Mechanick, J.I. Metabolic and nutrition support in the chronic critical illness syndrome. Respir. Care 2012, 57, 958–978. [Google Scholar] [CrossRef] [Green Version]
- Needham, D.M.; Davidson, J.; Cohen, H.; Hopkins, R.O.; Weinert, C.; Wunsch, H.; Zawistowski, C.; Bemis-Dougherty, A.; Berney, S.C.; Bienvenu, O.J.; et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care Med. 2012, 40, 502–509. [Google Scholar] [CrossRef]
- Batt, J.; Herridge, M.; Dos Santos, C. Mechanism of ICU-acquired weakness: Skeletal muscle loss in critical illness. Intensive Care Med. 2017, 43, 1844–1846. [Google Scholar] [CrossRef] [PubMed]
- Kress, J.P.; Hall, J.B. ICU-acquired weakness and recovery from critical illness. N. Engl. J. Med. 2014, 370, 1626–1635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, C.; Hussain, S.N.; Mathur, S.; Picard, M.; Herridge, M.; Correa, J.; Bain, A.; Guo, Y.; Advani, A.; Advani, S.L.; et al. Mechanisms of Chronic Muscle Wasting and Dysfunction after an Intensive Care Unit Stay. A Pilot Study. Am. J. Respir. Crit. Care Med. 2016, 194, 821–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bear, D.E.; Wandrag, L.; Merriweather, J.L.; Connolly, B.; Hart, N.; Grocott, M.P.W.; Enhanced Recovery After Critical Illness Programme Group investigators. The role of nutritional support in the physical and functional recovery of critically ill patients: A narrative review. Crit. Care 2017, 21, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendavid, I.; Singer, P.; Theilla, M.; Themessl-Huber, M.; Sulz, I.; Mouhieddine, M.; Schuh, C.; Mora, B.; Hiesmayr, M. NutritionDay ICU: A 7 year worldwide prevalence study of nutrition practice in intensive care. Clin. Nutr. 2017, 36, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Chiolero, R.L.; Pannatier, A.; Cayeux, M.C.; Tappy, L. A 10-year survey of nutritional support in a surgical ICU: 1986–1995. Nutrition 1997, 13, 870–877. [Google Scholar] [CrossRef]
- Peterson, S.J.; Tsai, A.A.; Scala, C.M.; Sowa, D.C.; Sheean, P.M.; Braunschweig, C.L. Adequacy of oral intake in critically ill patients 1 week after extubation. J. Am. Diet. Assoc. 2010, 110, 427–433. [Google Scholar] [CrossRef]
- Rougier, L.; Preiser, J.C.; Fadeur, M.; Verbrugge, A.M.; Paquot, N.; Ledoux, D.; Misset, B.; Rousseau, A.F. Nutrition During Critical Care: An Audit on Actual Energy and Protein Intakes. JPEN J. Parenter. Enter. Nutr. 2020. [Google Scholar] [CrossRef]
- Soguel, L.; Revelly, J.P.; Schaller, M.D.; Longchamp, C.; Berger, M.M. Energy deficit and length of hospital stay can be reduced by a two-step quality improvement of nutrition therapy: The intensive care unit dietitian can make the difference. Crit. Care Med. 2012, 40, 412–419. [Google Scholar] [CrossRef]
- Moisey, L.L.; Pikul, J.; Keller, H.; Yeung, C.Y.E.; Rahman, A.; Heyland, D.K.; Mourtzakis, M. Adequacy of Protein and Energy Intake in Critically Ill Adults Following Liberation From Mechanical Ventilation Is Dependent on Route of Nutrition Delivery. Nutr. Clin. Pract. 2020. [Google Scholar] [CrossRef]
- Johnston, J.D.; Harvey, C.J.; Menzies, I.S.; Treacher, D.F. Gastrointestinal permeability and absorptive capacity in sepsis. Crit. Care Med. 1996, 24, 1144–1149. [Google Scholar] [CrossRef] [PubMed]
- Deane, A.M.; Summers, M.J.; Zaknic, A.V.; Chapman, M.J.; Di Bartolomeo, A.E.; Bellon, M.; Maddox, A.; Russo, A.; Horowitz, M.; Fraser, R.J. Glucose absorption and small intestinal transit in critical illness. Crit. Care Med. 2011, 39, 1282–1288. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef] [PubMed]
- Ridley, E.J.; Parke, R.L.; Davies, A.R.; Bailey, M.; Hodgson, C.; Deane, A.M.; McGuinness, S.; Cooper, D.J. What Happens to Nutrition Intake in the Post-Intensive Care Unit Hospitalization Period? An Observational Cohort Study in Critically Ill Adults. JPEN J. Parenter. Enter. Nutr. 2019, 43, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Chapple, L.S.; Deane, A.M.; Heyland, D.K.; Lange, K.; Kranz, A.J.; Williams, L.T.; Chapman, M.J. Energy and protein deficits throughout hospitalization in patients admitted with a traumatic brain injury. Clin. Nutr. 2016, 35, 1315–1322. [Google Scholar] [CrossRef]
- Macht, M.; White, S.D.; Moss, M. Swallowing dysfunction after critical illness. Chest 2014, 146, 1681–1689. [Google Scholar] [CrossRef] [Green Version]
- Zuercher, P.; Schenk, N.V.; Moret, C.; Berger, D.; Abegglen, R.; Schefold, J.C. Risk Factors for Dysphagia in ICU Patients after Invasive Mechanical Ventilation. Chest 2020, 158, 1983–1991. [Google Scholar] [CrossRef]
- Zielske, J.; Bohne, S.; Brunkhorst, F.M.; Axer, H.; Guntinas-Lichius, O. Acute and long-term dysphagia in critically ill patients with severe sepsis: Results of a prospective controlled observational study. Eur. Arch. Otorhinolaryngol. 2014, 271, 3085–3093. [Google Scholar] [CrossRef]
- Zuercher, P.; Moret, C.S.; Dziewas, R.; Schefold, J.C. Dysphagia in the intensive care unit: Epidemiology, mechanisms, and clinical management. Crit. Care 2019, 23, 103. [Google Scholar] [CrossRef] [Green Version]
- Clave, P.; Arreola, V.; Romea, M.; Medina, L.; Palomera, E.; Serra-Prat, M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin. Nutr. 2008, 27, 806–815. [Google Scholar] [CrossRef]
- Frajkova, Z.; Tedla, M.; Tedlova, E.; Suchankova, M.; Geneid, A. Postintubation Dysphagia During COVID-19 Outbreak-Contemporary Review. Dysphagia 2020, 35, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.M.; Namasivayam-MacDonald, A.M.; Guida, B.T.; Cichero, J.A.; Duivestein, J.; Hanson, B.; Lam, P.; Riquelme, L.F. Creation and Initial Validation of the International Dysphagia Diet Standardisation Initiative Functional Diet Scale. Arch. Phys. Med. Rehabil. 2018, 99, 934–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cichero, J.A.; Lam, P.; Steele, C.M.; Hanson, B.; Chen, J.; Dantas, R.O.; Duivestein, J.; Kayashita, J.; Lecko, C.; Murray, J.; et al. Development of International Terminology and Definitions for Texture-Modified Foods and Thickened Fluids Used in Dysphagia Management: The IDDSI Framework. Dysphagia 2017, 32, 293–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapple, L.S.; Weinel, L.M.; Abdelhamid, Y.A.; Summers, M.J.; Nguyen, T.; Kar, P.; Lange, K.; Chapman, M.J.; Deane, A.M. Observed appetite and nutrient intake three months after ICU discharge. Clin. Nutr. 2019, 38, 1215–1220. [Google Scholar] [CrossRef]
- Merriweather, J.L.; Griffith, D.M.; Walsh, T.S. Appetite during the recovery phase of critical illness: A cohort study. Eur. J. Clin. Nutr. 2018, 72, 986–992. [Google Scholar] [CrossRef] [Green Version]
- Nematy, M.; O’Flynn, J.E.; Wandrag, L.; Brynes, A.E.; Brett, S.J.; Patterson, M.; Ghatei, M.A.; Bloom, S.R.; Frost, G.S. Changes in appetite related gut hormones in intensive care unit patients: A pilot cohort study. Crit. Care 2006, 10, R10. [Google Scholar] [CrossRef] [Green Version]
- Vesnaver, E.; Keller, H.H. Social influences and eating behavior in later life: A review. J. Nutr. Gerontol. Geriatr. 2011, 30, 2–23. [Google Scholar] [CrossRef]
- Wansink, B. Environmental factors that increase the food intake and consumption volume of unknowing consumers. Annu. Rev. Nutr. 2004, 24, 455–479. [Google Scholar] [CrossRef] [Green Version]
- Keller, H.; Allard, J.; Vesnaver, E.; Laporte, M.; Gramlich, L.; Bernier, P.; Davidson, B.; Duerksen, D.; Jeejeebhoy, K.; Payette, H. Barriers to food intake in acute care hospitals: A report of the Canadian Malnutrition Task Force. J. Hum. Nutr. Diet. 2015, 28, 546–557. [Google Scholar] [CrossRef]
- Naithani, S.; Whelan, K.; Thomas, J.; Gulliford, M.C.; Morgan, M. Hospital inpatients’ experiences of access to food: A qualitative interview and observational study. Health Expect 2008, 11, 294–303. [Google Scholar] [CrossRef] [Green Version]
- Preiser, J.C.; Ichai, C.; Orban, J.C.; Groeneveld, A.B. Metabolic response to the stress of critical illness. Br. J. Anaesth. 2014, 113, 945–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preiser, J.C. High protein intake during the early phase of critical illness: Yes or no? Crit. Care 2018, 22, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Zanten, A.R.H.; De Waele, E.; Wischmeyer, P.E. Nutrition therapy and critical illness: Practical guidance for the ICU, post-ICU, and long-term convalescence phases. Crit. Care 2019, 23, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatucu-Babet, O.A.; Fetterplace, K.; Lambell, K.; Miller, E.; Deane, A.M.; Ridley, E.J. Is Energy Delivery Guided by Indirect Calorimetry Associated With Improved Clinical Outcomes in Critically Ill Patients? A Systematic Review and Meta-analysis. Nutr. Metab. Insights 2020, 13. [Google Scholar] [CrossRef]
- Oshima, T.; Berger, M.M.; De Waele, E.; Guttormsen, A.B.; Heidegger, C.P.; Hiesmayr, M.; Singer, P.; Wernerman, J.; Pichard, C. Indirect calorimetry in nutritional therapy. A position paper by the ICALIC study group. Clin. Nutr. 2017, 36, 651–662. [Google Scholar] [CrossRef]
- Delsoglio, M.; Dupertuis, Y.M.; Oshima, T.; van der Plas, M.; Pichard, C. Evaluation of the accuracy and precision of a new generation indirect calorimeter in canopy dilution mode. Clin. Nutr. 2019, 39, 1927–1934. [Google Scholar] [CrossRef]
- Oshima, T.; Delsoglio, M.; Dupertuis, Y.M.; Singer, P.; De Waele, E.; Veraar, C.; Heidegger, C.P.; Wernermann, J.; Wischmeyer, P.E.; Berger, M.M.; et al. The clinical evaluation of the new indirect calorimeter developed by the ICALIC project. Clin. Nutr. 2020, 39, 3105–3111. [Google Scholar] [CrossRef]
- Tatucu-Babet, O.A.; Ridley, E.J.; Tierney, A.C. Prevalence of Underprescription or Overprescription of Energy Needs in Critically Ill Mechanically Ventilated Adults as Determined by Indirect Calorimetry: A Systematic Literature Review. JPEN J. Parenter. Enter. Nutr. 2016, 40, 212–225. [Google Scholar] [CrossRef]
- Fraipont, V.; Preiser, J.C. Energy estimation and measurement in critically ill patients. JPEN J. Parenter. Enter. Nutr. 2013, 37, 705–713. [Google Scholar] [CrossRef]
- Berger, M.M. How to prescribe nutritional support using computers. World Rev. Nutr. Diet. 2013, 105, 32–42. [Google Scholar] [CrossRef]
- Preiser, J.C.; Laureys, S.; van Zanten, A.R.H.; Van Gossum, A. Computer-Assisted Prescription: The Future of Nutrition Care? JPEN J. Parenter. Enter. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Revelly, J.P.; Wasserfallen, J.B.; Schmid, A.; Bouvry, S.; Cayeux, M.C.; Musset, M.; Maravic, P.; Chiolero, R.L. Impact of a computerized information system on quality of nutritional support in the ICU. Nutrition 2006, 22, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Vasiloglou, M.F.; Christodoulidis, S.; Reber, E.; Stathopoulou, T.; Lu, Y.; Stanga, Z.; Mougiakakou, S. What Healthcare Professionals Think of “Nutrition & Diet” Apps: An International Survey. Nutrients 2020, 12, 2214. [Google Scholar] [CrossRef]
- Evans, D.C.; Corkins, M.R.; Malone, A.; Miller, S.; Mogensen, K.M.; Guenter, P.; Jensen, G.L.; Committee, A.M. The Use of Visceral Proteins as Nutrition Markers: An ASPEN Position Paper. Nutr. Clin. Pract. 2020. [Google Scholar] [CrossRef]
- Bear, D.E.; Griffith, D.; Puthucheary, Z.A. Emerging outcome measures for nutrition trials in the critically ill. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 417–422. [Google Scholar] [CrossRef]
- Ridley, E.J.; Chapple, L.S.; Chapman, M.J. Nutrition intake in the post-ICU hospitalization period. Curr. Opin. Clin. Nutr. Metab. Care 2020, 23, 111–115. [Google Scholar] [CrossRef]
- Higgins, T.L.; Murray, M.; Kett, D.H.; Fulda, G.; Kramer, K.M.; Gelmont, D.; Dedhia, H.V.; Levy, H.; Teres, D.; Zaloga, G.P.; et al. Trace element homeostasis during continuous sedation with propofol containing EDTA versus other sedatives in critically ill patients. Intensive Care Med. 2000, 26 (Suppl. 4), S413–S421. [Google Scholar] [CrossRef]
- Kamel, A.Y.; Dave, N.J.; Zhao, V.M.; Griffith, D.P.; Connor, M.J., Jr.; Ziegler, T.R. Micronutrient Alterations During Continuous Renal Replacement Therapy in Critically Ill Adults: A Retrospective Study. Nutr. Clin. Pract. 2018, 33, 439–446. [Google Scholar] [CrossRef]
- Vankrunkelsven, W.; Gunst, J.; Amrein, K.; Bear, D.E.; Berger, M.M.; Christopher, K.B.; Fuhrmann, V.; Hiesmayr, M.; Ichai, C.; Jakob, S.M.; et al. Monitoring and parenteral administration of micronutrients, phosphate and magnesium in critically ill patients: The VITA-TRACE survey. Clin. Nutr. 2020. [Google Scholar] [CrossRef]
- Duncan, A.; Talwar, D.; McMillan, D.C.; Stefanowicz, F.; O’Reilly, D.S. Quantitative data on the magnitude of the systemic inflammatory response and its effect on micronutrient status based on plasma measurements. Am. J. Clin. Nutr. 2012, 95, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Galloway, P.; McMillan, D.C.; Sattar, N. Effect of the inflammatory response on trace element and vitamin status. Ann. Clin. Biochem. 2000, 37, 289–297. [Google Scholar] [CrossRef]
- Manson, J.E.; Bassuk, S.S. Vitamin and Mineral Supplements: What Clinicians Need to Know. JAMA 2018, 319, 859–860. [Google Scholar] [CrossRef]
- Rousseau, A.F.; Losser, M.R.; Ichai, C.; Berger, M.M. ESPEN endorsed recommendations: Nutritional therapy in major burns. Clin. Nutr. 2013, 32, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Casaer, M.P.; Bellomo, R. Micronutrient deficiency in critical illness: An invisible foe? Intensive Care Med. 2019, 45, 1136–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blass, S.C.; Goost, H.; Burger, C.; Tolba, R.H.; Stoffel-Wagner, B.; Stehle, P.; Ellinger, S. Extracellular micronutrient levels and pro-/antioxidant status in trauma patients with wound healing disorders: Results of a cross-sectional study. Nutr. J. 2013, 12, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostermann, M.; Summers, J.; Lei, K.; Card, D.; Harrington, D.J.; Sherwood, R.; Turner, C.; Dalton, N.; Peacock, J.; Bear, D.E. Micronutrients in critically ill patients with severe acute kidney injury—A prospective study. Sci. Rep. 2020, 10, 1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rech, M.; To, L.; Tovbin, A.; Smoot, T.; Mlynarek, M. Heavy metal in the intensive care unit: A review of current literature on trace element supplementation in critically ill patients. Nutr. Clin. Pract. 2014, 29, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Osland, E.; Powlesland, H.; Guthrie, T.; Lewis, C.A.; Memon, M.A. Micronutrient management following bariatric surgery: The role of the dietitian in the postoperative period. Ann. Transl. Med. 2020, 8, S9. [Google Scholar] [CrossRef]
- Berger, M.M.; Pantet, O.; Schneider, A.; Ben-Hamouda, N. Micronutrient Deficiencies in Medical and Surgical Inpatients. J. Clin. Med. 2019, 8, 931. [Google Scholar] [CrossRef] [Green Version]
- Lasocki, S.; Lefebvre, T.; Mayeur, C.; Puy, H.; Mebazaa, A.; Gayat, E.; Frog-Icu Study Group. Iron deficiency diagnosed using hepcidin on critical care discharge is an independent risk factor for death and poor quality of life at one year: An observational prospective study on 1161 patients. Crit. Care 2018, 22, 314. [Google Scholar] [CrossRef]
- Haas, J.D.; Brownlie, T.T. Iron deficiency and reduced work capacity: A critical review of the research to determine a causal relationship. J. Nutr. 2001, 131, 676S–690S. [Google Scholar] [CrossRef] [Green Version]
- Van Dronkelaar, C.; van Velzen, A.; Abdelrazek, M.; van der Steen, A.; Weijs, P.J.M.; Tieland, M. Minerals and Sarcopenia; The Role of Calcium, Iron, Magnesium, Phosphorus, Potassium, Selenium, Sodium, and Zinc on Muscle Mass, Muscle Strength, and Physical Performance in Older Adults: A Systematic Review. J. Am. Med Dir. Assoc. 2018, 19, 6–11.e13. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.; Venkatesh, B.; Center, J.R. Vitamin D deficiency and supplementation in critical illness-the known knowns and known unknowns. Crit. Care 2018, 22, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amrein, K.; Papinutti, A.; Mathew, E.; Vila, G.; Parekh, D. Vitamin D and critical illness: What endocrinology can learn from intensive care and vice versa. Endocr. Connect. 2018, 7, R304–R315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girgis, C.M. Vitamin D and Skeletal Muscle: Emerging Roles in Development, Anabolism and Repair. Calcif. Tissue Int. 2020, 106, 47–57. [Google Scholar] [CrossRef]
- Ceglia, L. Vitamin D and skeletal muscle tissue and function. Mol. Asp. Med. 2008, 29, 407–414. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Lee, P. How deficient are vitamin D deficient critically ill patients? Crit. Care 2011, 15, 154. [Google Scholar] [CrossRef] [Green Version]
- Amrein, K.; Schnedl, C.; Holl, A.; Riedl, R.; Christopher, K.B.; Pachler, C.; Urbanic Purkart, T.; Waltensdorfer, A.; Munch, A.; Warnkross, H.; et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vitamin D deficiency: The VITdAL-ICU randomized clinical trial. JAMA 2014, 312, 1520–1530. [Google Scholar] [CrossRef] [Green Version]
- Stockton, K.A.; Mengersen, K.; Paratz, J.D.; Kandiah, D.; Bennell, K.L. Effect of vitamin D supplementation on muscle strength: A systematic review and meta-analysis. Osteoporos. Int. 2011, 22, 859–871. [Google Scholar] [CrossRef]
- Ebid, A.A.; El-Shamy, S.M.; Amer, M.A. Effect of vitamin D supplementation and isokinetic training on muscle strength, explosive strength, lean body mass and gait in severely burned children: A randomized controlled trial. Burns 2017, 43, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, A.F.; Foidart-Desalle, M.; Ledoux, D.; Remy, C.; Croisier, J.L.; Damas, P.; Cavalier, E. Effects of cholecalciferol supplementation and optimized calcium intakes on vitamin D status, muscle strength and bone health: A one-year pilot randomized controlled trial in adults with severe burns. Burns 2015, 41, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.E.; Evans, A.M. Carnitine and acylcarnitines: Pharmacokinetic, pharmacological and clinical aspects. Clin. Pharmacokinet. 2012, 51, 553–572. [Google Scholar] [CrossRef] [PubMed]
- Bonafe, L.; Berger, M.M.; Que, Y.A.; Mechanick, J.I. Carnitine deficiency in chronic critical illness. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.E.; Murphy, K.G.; Singer, M. Ghrelin, appetite and critical illness. Curr. Opin. Crit. Care 2012, 18, 199–205. [Google Scholar] [CrossRef]
- Heyland, D.K.; van Zanten, A.R.H.; Grau-Carmona, T.; Evans, D.; Beishuizen, A.; Schouten, J.; Hoiting, O.; Bordeje, M.L.; Krell, K.; Klein, D.J.; et al. A multicenter, randomized, double-blind study of ulimorelin and metoclopramide in the treatment of critically ill patients with enteral feeding intolerance: PROMOTE trial. Intensive Care Med. 2019, 45, 647–656. [Google Scholar] [CrossRef]
- Wischmeyer, P.E.; Suman, O.E.; Kozar, R.; Wolf, S.E.; Molinger, J.; Pastva, A.M. Role of anabolic testosterone agents and structured exercise to promote recovery in ICU survivors. Curr. Opin. Crit. Care 2020, 26, 508–515. [Google Scholar] [CrossRef]
- Parry, S.M.; Chapple, L.S.; Mourtzakis, M. Exploring the Potential Effectiveness of Combining Optimal Nutrition With Electrical Stimulation to Maintain Muscle Health in Critical Illness: A Narrative Review. Nutr. Clin. Pract. 2018, 33, 772–789. [Google Scholar] [CrossRef]
- Heyland, D.K.; Stapleton, R.D.; Mourtzakis, M.; Hough, C.L.; Morris, P.; Deutz, N.E.; Colantuoni, E.; Day, A.; Prado, C.M.; Needham, D.M. Combining nutrition and exercise to optimize survival and recovery from critical illness: Conceptual and methodological issues. Clin. Nutr. 2016, 35, 1196–1206. [Google Scholar] [CrossRef]
- Nakamura, K.; Nakano, H.; Naraba, H.; Mochizuki, M.; Takahashi, Y.; Sonoo, T.; Hashimoto, H.; Morimura, N. High protein versus medium protein delivery under equal total energy delivery in critical care: A randomized controlled trial. Clin. Nutr. 2020. [Google Scholar] [CrossRef]
- Morton, R.W.; Traylor, D.A.; Weijs, P.J.M.; Phillips, S.M. Defining anabolic resistance: Implications for delivery of clinical care nutrition. Curr. Opin. Crit. Care 2018, 24, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Brett, E.M. Endocrine and metabolic issues in the management of the chronically critically ill patient. Crit. Care Clin. 2002, 18, 619–641. [Google Scholar] [CrossRef]
- Wehbeh, L.; Dobs, A.S. Opioids and the Hypothalamic-Pituitary-Gonadal (HPG) Axis. J. Clin. Endocrinol. Metab. 2020, 105, e3105–e3113. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Guo, Y.; Yang, Z.; Roy, M.; Guo, Q. The efficacy and safety of oxandrolone treatment for patients with severe burns: A systematic review and meta-analysis. Burns 2016, 42, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Takala, J.; Ruokonen, E.; Webster, N.R.; Nielsen, M.S.; Zandstra, D.F.; Vundelinckx, G.; Hinds, C.J. Increased mortality associated with growth hormone treatment in critically ill adults. N. Engl. J. Med. 1999, 341, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Demling, R.H. Comparison of the anabolic effects and complications of human growth hormone and the testosterone analog, oxandrolone, after severe burn injury. Burns 1999, 25, 215–221. [Google Scholar] [CrossRef]
- Herndon, D.N.; Hart, D.W.; Wolf, S.E.; Chinkes, D.L.; Wolfe, R.R. Reversal of catabolism by beta-blockade after severe burns. N. Engl. J. Med. 2001, 345, 1223–1229. [Google Scholar] [CrossRef]
- Porro, L.J.; Al-Mousawi, A.M.; Williams, F.; Herndon, D.N.; Mlcak, R.P.; Suman, O.E. Effects of propranolol and exercise training in children with severe burns. J. Pediatr. 2013, 162, 799–803.e791. [Google Scholar] [CrossRef] [Green Version]
- Chiolero, R.L.; Breitenstein, E.; Thorin, D.; Christin, L.; de Tribolet, N.; Freeman, J.; Jequier, E.; Schutz, Y. Effects of propranolol on resting metabolic rate after severe head injury. Crit. Care Med. 1989, 17, 328–334. [Google Scholar] [CrossRef]
- Ham, D.J.; Caldow, M.K.; Lynch, G.S.; Koopman, R. Leucine as a treatment for muscle wasting: A critical review. Clin. Nutr. 2014, 33, 937–945. [Google Scholar] [CrossRef]
- Bear, D.E.; Langan, A.; Dimidi, E.; Wandrag, L.; Harridge, S.D.R.; Hart, N.; Connolly, B.; Whelan, K. beta-Hydroxy-beta-methylbutyrate and its impact on skeletal muscle mass and physical function in clinical practice: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 109, 1119–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Register Identifier | Design | Region | Inclusion Criteria | Primary Outcome | Secondary Outcomes | Intervention | Comparator | Planned Sample Size |
|---|---|---|---|---|---|---|---|---|
| NCT 04549961 | Observ. | Austria | Admitted to ICU on nutritionDay. | 60 days hospital mortality. Length of ICU stay. Route of nutrition. Planned and delivered amount of nutrition in kcal from all routes. | Number of ICU beds. Human resources. | NA | NA | 3500 |
| NCT 04274322 | Observ. | China | Anticipated length of ICU stay >48 h. Diagnosed with 2019 coronavirus disease (COVID-19). Food intake difficulties. | 28-day all-cause mortality. | From admission to 28 days after discharge: All-cause infection. Rate of complications. Length of ICU stay. Duration of mechanical ventilation. | NA | NA | 117 |
| NCT 02920086 | PRT open label | Canada | 1/ For patients: >60 years of age OR 55 years to 59 years old with one or more comorbidities. Projected duration of ICU dependency of >72 h from time of final assessment. 2/ For family member: Present and expected to visit regularly. The nominated or legally appointed substitute decision-maker. Able to communicate in English. | Nutritional adequacy during the ICU stay. Consumption of ONS. Caloric intakes on hospital wards. Hand grip strength. Use of shared decision-making. Change in decisional conflict. Family satisfaction with decision-making. Overall family satisfaction with ICU. | Not provided. | 1/Nutrition Education Program involving families. 2/Decision support program involving families. | Usual care | 150 |
| ACTRN12620001025921p | Observ. | Australia and New Zealand | Adults admitted in ICU for >48 h. | Energy prescription and intakes. Feeding intolerances. Delivery of dietetic services. | Protein prescription and intakes. Descriptions in nutrition practice variability across Australia and New Zealand. Hospital length-of-stay. Infectious complications. | NA | NA | 500 |
| ACTRN12620000602921 | Observ. | Australia | Patients included in Short Period Incidence Study of Severe Acute Respiratory Infection (SPRINT-SARI): adults with a suspected or proven acute respiratory infection requiring new inpatient admission with onset within past 14 days. | Nutrition service delivery. Nutrition provision. Proportion of patients diagnosed with malnutrition using any of the validated malnutrition screening and assessment tools. | Data about nutritional management during prone position. | NA | NA | 200 |
| UMIN 000040290 | Interv. Single arm, open and not randomized | Japan | Adults admitted in ICU, with an expected hospital stay ≥10 days. | Femoral muscle volume change from day 1 through 10 | MRC score, FSS-ICU, EQ-5D at ICU discharge. Barthel Index at hospital discharge. Target nutrition achievement rate N-titin level of days 1, 3, 5, and 7. | Rehabilitation (including electrical stimulation of lower limbs) and nutrition administration. | Historical control. | 50 |
| UMIN 000042057 | Observ. | Japan | Adults admitted in ICU for >3 days. | Protein/non protein calories ratio, from ICU admission to the day before hospital discharge. | Muscle mass and Barthel Index the day before hospital discharge. | NA | NA | 180 |
| Difficult or Painful Chewing or Swallowing |
| Regurgitation of undigested food. |
| Difficulty of controlling solids or liquids in the mouth. |
| Drooling. |
| Coughing during or after swallowing. |
| Feeling of obstruction. |
| Frequent throat clearing. |
| Recurrent bronchitis or pulmonary infections. |
| Clinical Situation | Micronutrient Supplementation |
|---|---|
| Suboptimal eating patterns. Energy intake < 1500 kcal/day. | Multivitamins/multiminerals, vitamin D, calcium, vitamin B12, magnesium. |
| Prolonged ICU and/or hospital stay. | Vitamin D, calcium. |
| Prolonged wound healing, polytrauma. | Multivitamins/multiminerals. |
| PPI (long term treatment). | Vitamin B12, magnesium, calcium. |
| Severe acute kidney injury, CRRT. | Multivitamins/multiminerals. |
| Persistent kidney disease. | Vitamin D, vitamin K. |
| Post-bariatric surgery status. | Multivitamins/multiminerals, vitamin D, calcium, vitamin B12, iron. |
| Alcohol abuse. | Vitamins B, fat-soluble vitamins, zinc. |
| Liver disease (i.e., fatty liver). | Zinc, selenium, vitamins A, D, K, and B12. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fadeur, M.; Preiser, J.-C.; Verbrugge, A.-M.; Misset, B.; Rousseau, A.-F. Oral Nutrition during and after Critical Illness: SPICES for Quality of Care! Nutrients 2020, 12, 3509. https://doi.org/10.3390/nu12113509
Fadeur M, Preiser J-C, Verbrugge A-M, Misset B, Rousseau A-F. Oral Nutrition during and after Critical Illness: SPICES for Quality of Care! Nutrients. 2020; 12(11):3509. https://doi.org/10.3390/nu12113509
Chicago/Turabian StyleFadeur, Marjorie, Jean-Charles Preiser, Anne-Marie Verbrugge, Benoit Misset, and Anne-Françoise Rousseau. 2020. "Oral Nutrition during and after Critical Illness: SPICES for Quality of Care!" Nutrients 12, no. 11: 3509. https://doi.org/10.3390/nu12113509
APA StyleFadeur, M., Preiser, J. -C., Verbrugge, A. -M., Misset, B., & Rousseau, A. -F. (2020). Oral Nutrition during and after Critical Illness: SPICES for Quality of Care! Nutrients, 12(11), 3509. https://doi.org/10.3390/nu12113509