Affective and Enjoyment Responses to Short-Term High-Intensity Interval Training with Low-Carbohydrate Diet in Overweight Young Women

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Instruments of Affect and Enjoyment
2.3. Experimental Procedures
2.4. Diet Intervention
2.5. Training Intervention
2.6. Pre- and Post-Intervention Tests
2.7. Statistical Analysis
3. Results
3.1. The Demographic Characteristics of the Participants
3.2. Dietary Intake, Daily Physical Activity and Training Data
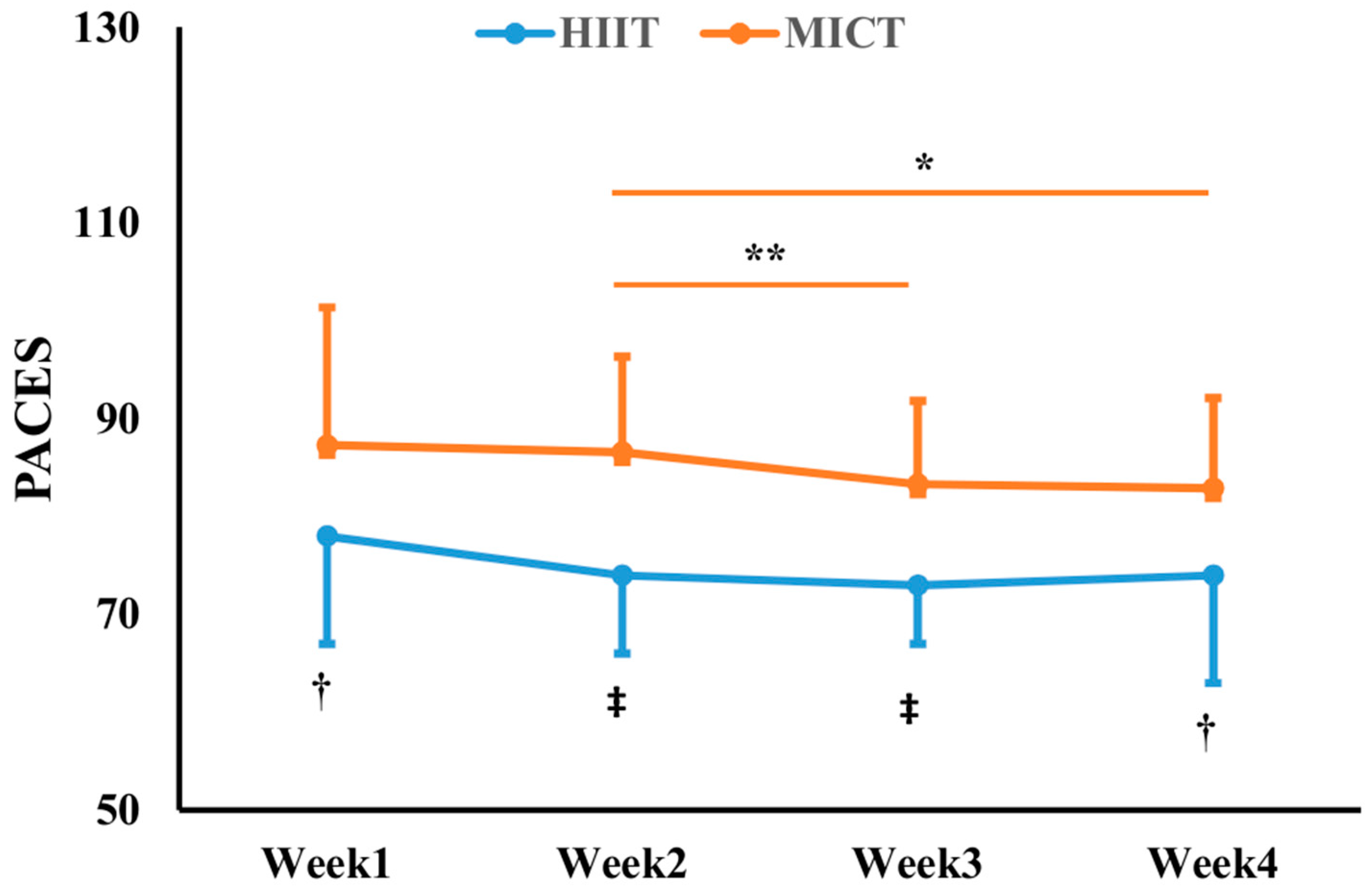
3.3. Affective and Enjoyment Responses to the Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- de Onis, M.; Martinez-Costa, C.; Nunez, F.; Nguefack-Tsague, G.; Montal, A.; Brines, J. Association between WHO cut-offs for childhood overweight and obesity and cardiometabolic risk. Public Health Nutr. 2013, 16, 625–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Spadano, J.; Coakley, E.H.; Field, A.E.; Colditz, G.; Dietz, W.H. The disease burden associated with overweight and obesity. JAMA 1999, 282, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Suvan, J.; D’Aiuto, F.; Moles, D.R.; Petrie, A.; Donos, N. Association between overweight/obesity and periodontitis in adults. A systematic review. Obes. Rev. 2011, 12, e381–e404. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Colditz, G. Prevalence of overweight and obesity in the United States, 2007–2012. JAMA Intern. Med. 2015, 175, 1412–1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, A.M.; Johnston, C.S.; Swan, P.D.; Tjonn, S.L.; Sears, B. Blood ketones are directly related to fatigue and perceived effort during exercise in overweight adults adhering to low-carbohydrate diets for weight loss: A pilot study. J. Am. Diet. Assoc. 2007, 107, 1792–1796. [Google Scholar] [CrossRef]
- Sun, S.; Kong, Z.; Shi, Q.; Hu, M.; Zhang, H.; Zhang, D.; Nie, J. Non-Energy-Restricted Low-Carbohydrate Diet Combined with Exercise Intervention Improved Cardiometabolic Health in Overweight Chinese Females. Nutrients 2019, 11, 3051. [Google Scholar] [CrossRef] [Green Version]
- Leibel, R.L.; Seeley, R.J.; Darsow, T.; Berg, E.G.; Smith, S.R.; Ratner, R. Biologic responses to weight loss and weight regain: Report from an American Diabetes Association Research Symposium. Diabetes 2015, 64, 2299–2309. [Google Scholar] [CrossRef] [Green Version]
- Pavlou, K.N.; Krey, S.; Steffee, W.P. Exercise as an adjunct to weight loss and maintenance in moderately obese subjects. Am. J. Clin. Nutr. 1989, 49, 1115–1123. [Google Scholar] [CrossRef] [Green Version]
- Ramos, J.S.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.S.; Coombes, J.S. The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: A systematic review and meta-analysis. Sports Med. 2015, 45, 679–692. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Oliveira, B.R.R.; Santos, T.M.; Kilpatrick, M.; Pires, F.O.; Deslandes, A.C. Affective and enjoyment responses in high intensity interval training and continuous training: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0197124. [Google Scholar] [CrossRef] [Green Version]
- Urbain, P.; Strom, L.; Morawski, L.; Wehrle, A.; Deibert, P.; Bertz, H. Impact of a 6-week non-energy-restricted ketogenic diet on physical fitness, body composition and biochemical parameters in healthy adults. Nutr. Metab. 2017, 14, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilis, K.; Pilis, A.; Stec, K.; Pilis, W.; Langfort, J.; Letkiewicz, S.; Michalski, C.; Czuba, M.; Zych, M.; Chalimoniuk, M. Three-Year Chronic Consumption of Low-Carbohydrate Diet Impairs Exercise Performance and Has a Small Unfavorable Effect on Lipid Profile in Middle-Aged Men. Nutrients 2018, 10, 1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekkekakis, P.; Parfitt, G.; Petruzzello, S.J. The pleasure and displeasure people feel when they exercise at different intensities: Decennial update and progress towards a tripartite rationale for exercise intensity prescription. Sports Med. 2011, 41, 641–671. [Google Scholar] [CrossRef]
- Townsend, L.K.; Islam, H.; Dunn, E.; Eys, M.; Robertson-Wilson, J.; Hazell, T.J. Modified sprint interval training protocols. Part II. Psychological responses. Appl. Physiol. Nutr. Metab. 2016, 42, 347–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vella, C.A.; Taylor, K.; Drummer, D. High-intensity interval and moderate-intensity continuous training elicit similar enjoyment and adherence levels in overweight and obese adults. Eur. J. Sport Sci. 2017, 17, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Clark, A.; De La Rosa, A.; De Revere, J.L. Enjoyment and affective responses to two regimes of high intensity interval training in inactive women with obesity. Eur. J. Sport Sci. 2019, 19, 1377–1385. [Google Scholar] [CrossRef]
- Jung, M.E.; Bourne, J.E.; Little, J.P. Where does HIT fit? An examination of the affective response to high-intensity intervals in comparison to continuous moderate-and continuous vigorous-intensity exercise in the exercise intensity-affect continuum. PLoS ONE 2014, 9, e114541. [Google Scholar] [CrossRef] [Green Version]
- Kong, Z.; Fan, X.; Sun, S.; Song, L.; Shi, Q.; Nie, J. Comparison of high-intensity interval training and moderate-to-vigorous continuous training for cardiometabolic health and exercise enjoyment in obese young women: A randomized controlled trial. PLoS ONE 2016, 11, e0158589. [Google Scholar] [CrossRef]
- Sun, S.Y.; Zhang, H.F.; Kong, Z.W.; Shi, Q.D.; Tong, T.K.; Nie, J.L. Twelve weeks of low volume sprint interval training improves cardio-metabolic health outcomes in overweight females. J. Sport Sci. 2019, 37, 1257–1264. [Google Scholar] [CrossRef]
- Shi, Q.; Tong, T.K.; Sun, S.; Kong, Z.; Chan, C.K.; Liu, W.; Nie, J. Influence of recovery duration during 6-s sprint interval exercise on time spent at high rates of oxygen uptake. J. Exerc. Sci. Fit. 2018, 16, 16–20. [Google Scholar] [CrossRef] [PubMed]
- McKie, G.L.; Islam, H.; Townsend, L.K.; Robertson-Wilson, J.; Eys, M.; Hazell, T.J. Modified sprint interval training protocols: Physiological and psychological responses to 4 weeks of training. Appl. Physiol. Nutr. Metab. 2018, 43, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Islam, H.; Townsend, L.K.; Hazell, T.J. Modified sprint interval training protocols. Part I. Physiological responses. Appl. Physiol. Nutr. Metab. 2017, 42, 339–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, D.; Utesch, T.; Wu, J.; Robertson, S.; Liu, J.; Hu, G.; Chen, H. Effects of different protocols of high intensity interval training for VO2max improvements in adults: A meta-analysis of randomised controlled trials. J. Sci. Med. Sport 2019, 22, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Butki, B.D.; Baumstark, J.; Driver, S. Effects of a Carbohydrate-Restricted Diet on Affective Responses to Acute Exercise among Physically Active Participants. Percept. Motor Skills 2003, 96, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Spriet, L.L.; Peters, S.J. Influence of diet on the metabolic responses to exercise. Proc. Nutr. Soc. 1998, 57, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Galbo, H.; Holst, J.J.; Christensen, N.J. The effect of different diets and of insulin on the hormonal response to prolonged exercise. Acta Physiol. Scand. 1979, 107, 19–32. [Google Scholar] [CrossRef]
- Burke, L.M.; Kiens, B.; Ivy, J.L. Carbohydrates and fat for training and recovery. J. Sports Sci. 2004, 22, 15–30. [Google Scholar] [CrossRef] [Green Version]
- Pinckaers, P.J.; Churchward-Venne, T.A.; Bailey, D.; van Loon, L.J. Ketone Bodies and Exercise Performance: The Next Magic Bullet or Merely Hype? Sports Med. 2017, 47, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Phinney, S.D. Ketogenic diets and physical performance. Nutr. Metab. 2004, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Paoli, A.; Bianco, A.; Grimaldi, K.A. The Ketogenic Diet and Sport: A Possible Marriage? Exerc. Sport Sci. Rev. 2015, 43, 153–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costill, D.L.; Kenney, W.L.; Wilmore, J. Physiology of Sport and Exercise; Human Kinetics: Champaign, IL, USA, 2008; Volume 448, p. 51. [Google Scholar]
- Rhyu, H.S.; Cho, S.Y. The effect of weight loss by ketogenic diet on the body composition, performance-related physical fitness factors and cytokines of Taekwondo athletes. J. Exerc. Rehabil. 2014, 10, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Stork, M.J.; Banfield, L.E.; Gibala, M.J.; Martin Ginis, K.A. A scoping review of the psychological responses to interval exercise: Is interval exercise a viable alternative to traditional exercise? Health Psychol. Rev. 2017, 11, 324–344. [Google Scholar] [CrossRef] [PubMed]
- Havemann, L.; West, S.J.; Goedecke, J.H.; Macdonald, I.A.; St Clair Gibson, A.; Noakes, T.D.; Lambert, E.V. Fat adaptation followed by carbohydrate loading compromises high-intensity sprint performance. J. Appl. Physiol. 2006, 100, 194–202. [Google Scholar] [CrossRef]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Kilpatrick, M.W.; Greeley, S.J.; Collins, L.H. The Impact of Continuous and Interval Cycle Exercise on Affect and Enjoyment. Res. Q. Exerc. Sport 2015, 86, 244–251. [Google Scholar] [CrossRef]
- Stork, M.J.; Gibala, M.J.; Ginis, K.A.M. Psychological and Behavioral Responses to Interval and Continuous Exercise. Med. Sci. Sports Exerc. 2018, 50, 2110–2121. [Google Scholar] [CrossRef]
- Stanley, D.M.; Cumming, J. Are we having fun yet? Testing the effects of imagery use on the affective and enjoyment responses to acute moderate exercise. Psychol. Sport Exerc. 2010, 11, 582–590. [Google Scholar] [CrossRef]
- Martinez, N.; Kilpatrick, M.W.; Salomon, K.; Jung, M.E.; Little, J.P. Affective and Enjoyment Responses to High-Intensity Interval Training in Overweight-to-Obese and Insufficiently Active Adults. J. Sport Exerc. Psychol. 2015, 37, 138–149. [Google Scholar] [CrossRef]
- Kendzierski, D.; DeCarlo, K.J. Physical Activity Enjoyment Scale: Two Validation Studies. J. Sport Exerc. Psychol. 1991, 13, 50–64. [Google Scholar] [CrossRef]
- Urbain, P.; Bertz, H. Monitoring for compliance with a ketogenic diet: What is the best time of day to test for urinary ketosis? Nutr. Metab. 2016, 13, 77. [Google Scholar] [CrossRef] [Green Version]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work Environ. Health 1990, 16 (Suppl. 1), 55–58. [Google Scholar] [CrossRef] [PubMed]
- Kirk, R.E. Practical significance: A concept whose time has come. Educ. Psychol. Meas. 1996, 56, 746–759. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Saanijoki, T.; Nummenmaa, L.; Eskelinen, J.J.; Savolainen, A.M.; Vahlberg, T.; Kalliokoski, K.K.; Hannukainen, J.C. Affective Responses to Repeated Sessions of High-Intensity Interval Training. Med. Sci. Sports Exerc. 2015, 47, 2604–2611. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A.; Pratt, G. A Description of the Affective Quality Attributed to Environments. J. Personal. Soc. Psychol. 1980, 38, 311–322. [Google Scholar] [CrossRef]
- Haile, L.; Gallagher, M.; Robertson, R.J. Perceived Exertion Laboratory Manual; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Raedeke, T.D. The Relationship Between Enjoyment and Affective Responses to Exercise. J. Appl. Sport Psychol. 2007, 19, 105–115. [Google Scholar] [CrossRef]
- Frazão, D.T.; de Farias Junior, L.F.; Dantas, T.C.B.; Krinski, K.; Elsangedy, H.M.; Prestes, J.; Hardcastle, S.J.; Costa, E.C. Feeling of pleasure to high-intensity interval exercise is dependent of the number of work bouts and physical activity status. PLoS ONE 2016, 11, e0152752. [Google Scholar]
- Stepto, N.K.; Carey, A.L.; Staudacher, H.M.; Cummings, N.K.; Burke, L.M.; Hawley, J.A. Effect of short-term fat adaptation on high-intensity training. Med. Sci. Sports Exerc. 2002, 34, 449–455. [Google Scholar] [CrossRef]
- McSwiney, F.T.; Wardrop, B.; Hyde, P.N.; Lafountain, R.A.; Volek, J.S.; Doyle, L. Keto-adaptation enhances exercise performance and body composition responses to training in endurance athletes. Metabolism 2018, 81, 25–34. [Google Scholar] [CrossRef]
- Henderson, B.J.; Whissell, C. Changes in Women’s Emotions as a Function of Emotion Valence, Self-Determined Category of Premenstrual Distress, and Day in the Menstrual Cycle. Psychol. Rep. 1997, 80, 1272–1274. [Google Scholar] [CrossRef]
- Westman, E.C.; Mavropoulos, J.; Yancy, W.S.; Volek, J.S. A review of low-carbohydrate ketogenic diets. Curr. Atheroscler. Rep. 2003, 5, 476–483. [Google Scholar] [CrossRef]


{kind=link}
| CON (n = 15) | HIIT (n = 15) | MICT (n = 13) | |
|---|---|---|---|
| Age (y) | 20.9 ± 3.7 | 20.8 ± 2.7 | 21.5 ± 3.1 |
| Height (cm) | 161.3 ± 4.7 | 162.9 ± 6.2 | 160.9 ± 4.3 |
| Weight (kg) | 65.1 ± 7.3 | 67.9 ± 10.3 | 64.5 ± 6.4 |
| BMI (kg/m2) | 25.0 ± 2.9 | 25.5 ± 3.1 | 24.9 ± 1.9 |
| V̇O2peak (mL/min) | 1652 ± 211 | 1576 ± 278 | 1506 ± 294 |
| V̇O2peak (mL/min/kg) | 24.3 ± 2.6 | 23.8 ± 2.8 | 23.4 ± 4.4 |
| Pre_Week 1 | Pre_Week 2 | Week 1 | Week 2 | Week 3 | Week 4 | |
|---|---|---|---|---|---|---|
| Energy intake (kcal) | ||||||
| CON | 1824 ± 433 | 1921 ± 377 | 1755 ± 587 | 1573 ± 609 | 1639 ± 435 | 1568 ± 439 |
| HIIT | 2254 ± 720 | 2229 ± 444 | 1793 ± 247 | 1851 ± 272 | 1839 ± 287 | 1855 ± 487 |
| MICT | 2176 ± 410 | 2006 ± 539 | 2109 ± 487 | 2059 ± 538 | 2000 ± 550 | 1956 ± 431 |
| Carbohydrate (% of energy intake) | ||||||
| CON | 44.7 ± 7.9 | 46.6 ± 12.5 | 10.4 ± 6.1 | 9.4 ± 7.6 | 9.8 ± 5.6 | 9.9 ± 9.0 |
| HIIT | 47.9 ± 7.3 | 45.2 ± 9.9 | 13.4 ± 8.5 | 10.8 ± 5.7 | 9.7 ± 6.1 | 7.6 ± 3.0 |
| MICT | 45.1 ± 9.2 | 46.2 ± 10.3 | 12.7 ± 8.1 | 11.1 ± 6.0 | 8.8 ± 3.0 | 8.5 ± 3.2 |
| Fat (% of energy intake) | ||||||
| CON | 38.5 ± 6.8 | 37.1 ± 9.7 | 67.7 ± 6.9 | 66.3 ± 7.7 | 67.9 ± 5.0 | 68.7 ± 9.3 |
| HIIT | 36.3 ± 6.2 | 37.0 ± 7.7 | 63.1 ± 9.3 | 64.3 ± 8.3 | 68.3 ± 7.8 | 68.5 ± 10.2 |
| MICT | 36.8 ± 8.9 | 34.9 ± 8.6 | 63.8 ± 8.4 | 64.4 ± 7.0 | 68.2 ± 6.0 | 68.8 ± 7.6 |
| Protein (% of energy intake) | ||||||
| CON | 15.3 ± 4.1 | 15.2 ± 5.1 | 21.9 ± 4.3 | 24.2 ± 5.1 | 22.9 ± 5.6 | 21.6 ± 5.1 |
| HIIT | 14.9 ± 2.1 | 15.3 ± 3.0 | 23.6 ± 5.4 | 25.1 ± 7.3 | 22.0 ± 4.4 | 23.7 ± 8.1 |
| MICT | 14.1 ± 2.7 | 15.1 ± 2.6 | 23.4 ± 5.1 | 24.6 ± 4.6 | 23.1 ± 5.1 | 22.9 ± 5.5 |
| Daily physical activities (steps) | ||||||
| CON | 8852 ± 1846 | 7823 ± 1952 | 8029 ± 2012 | 8312 ± 3061 | 7694 ± 2978 | 7483 ± 1725 |
| HIIT | 7933 ± 3385 | 7763 ± 2747 | 8472 ± 1819 | 8331 ± 2244 | 9050 ± 1811 | 8147 ± 2092 |
| MICT | 7885 ± 2485 | 8229 ± 1392 | 9140 ± 1786 | 9315 ± 2305 | 8797 ± 1666 | 9109 ± 1851 |
| HIIT (n = 15) | MICT (n = 13) | |
|---|---|---|
| Total Time (min) | 50 | 600 |
| %HRmax | 82 ± 4 | 75 ± 3 † |
| %HRR | 68 ± 5 | 57 ± 5 † |
| RPE | 4 ± 1 | 1 ± 1 † |
| Mean power (W) | 249 ± 34 | 54 ± 10 † |
| HIIT (n = 15) | MICT (n = 13) | |||||||
|---|---|---|---|---|---|---|---|---|
| W1 | W2 | W3 | W4 | W1 | W2 | W3 | W4 | |
| RPE0-10 | ||||||||
| Pre | 0.3 ± 0.3 | 0.3 ± 0.3 | 0.5 ± 0.3 | 0.4 ± 0.3 | 0.4 ± 0.5 | 0.5 ± 0.5 | 0.5 ± 0.5 | 0.5 ± 0.4 |
| Post | 4.5 ± 1.8 *,† | 4.9 ± 1.4 *,† | 5.2 ± 1.2 *,† | 5.3 ± 0.9 *,† | 1.8 ± 1.0 * | 1.6 ± 0.9 * | 2.1 ± 1.4 * | 2.0 ± 1.1 * |
| FS | ||||||||
| Pre | 1.4 ± 1.5 | 1.4 ± 1.7 | 1.4 ± 1.6 | 1.6 ± 1.9 | 1.4 ± 1.5 | 1.4 ± 1.4 | 1.3 ± 1.4 | 1.4 ± 1.5 |
| Post | 1.3 ± 1.4 | 1.3 ± 1.6 | 1.3 ± 1.3 | 1.4 ± 1.9 | 1.6 ± 1.5 | 1.5 ± 1.5 | 1.5 ± 1.6 | 1.5 ± 1.6 |
| FAS | ||||||||
| Pre | 3.3 ± 1.0 | 3.2 ± 1.1 | 3.2 ± 1.1 | 3.3 ± 1.1 | 3.5 ± 0.8 | 3.6 ± 0.8 | 3.6 ± 0.9 | 3.6 ± 1.0 |
| Post | 3.7 ± 1.0 * | 3.9 ± 0.9 * | 3.8 ± 1.0 * | 3.9 ± 0.9 * | 4.2 ± 0.7 * | 4.1 ± 0.7 * | 4.1 ± 0.8 * | 4.0 ± 0.9 * |
| EES | ||||||||
| Pre | 4.0 ± 0.7 | 4.2 ± 1.2 | 4.1 ± 1.1 | 4.2 ± 0.9 | 3.9 ± 0.6 | 4.1 ± 0.7 | 4.0 ± 0.9 | 3.9 ± 0.9 |
| Post | 4.2 ± 0.7 | 4.1 ± 1.0 | 4.0 ± 1.0 | 4.1 ± 0.9 | 4.2 ± 0.6 * | 4.1 ± 0.7 | 4.0 ± 0.8 | 3.9 ± 0.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kong, Z.; Hu, M.; Liu, Y.; Shi, Q.; Zou, L.; Sun, S.; Zhang, H.; Nie, J. Affective and Enjoyment Responses to Short-Term High-Intensity Interval Training with Low-Carbohydrate Diet in Overweight Young Women. Nutrients 2020, 12, 442. https://doi.org/10.3390/nu12020442
Kong Z, Hu M, Liu Y, Shi Q, Zou L, Sun S, Zhang H, Nie J. Affective and Enjoyment Responses to Short-Term High-Intensity Interval Training with Low-Carbohydrate Diet in Overweight Young Women. Nutrients. 2020; 12(2):442. https://doi.org/10.3390/nu12020442
Chicago/Turabian StyleKong, Zhaowei, Mingzhu Hu, Yang Liu, Qingde Shi, Liye Zou, Shengyan Sun, Haifeng Zhang, and Jinlei Nie. 2020. "Affective and Enjoyment Responses to Short-Term High-Intensity Interval Training with Low-Carbohydrate Diet in Overweight Young Women" Nutrients 12, no. 2: 442. https://doi.org/10.3390/nu12020442
APA StyleKong, Z., Hu, M., Liu, Y., Shi, Q., Zou, L., Sun, S., Zhang, H., & Nie, J. (2020). Affective and Enjoyment Responses to Short-Term High-Intensity Interval Training with Low-Carbohydrate Diet in Overweight Young Women. Nutrients, 12(2), 442. https://doi.org/10.3390/nu12020442