Hyperosmolarity and Increased Serum Sodium Concentration Are Risks for Developing Hypertension Regardless of Salt Intake: A Five-Year Cohort Study in Japan

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
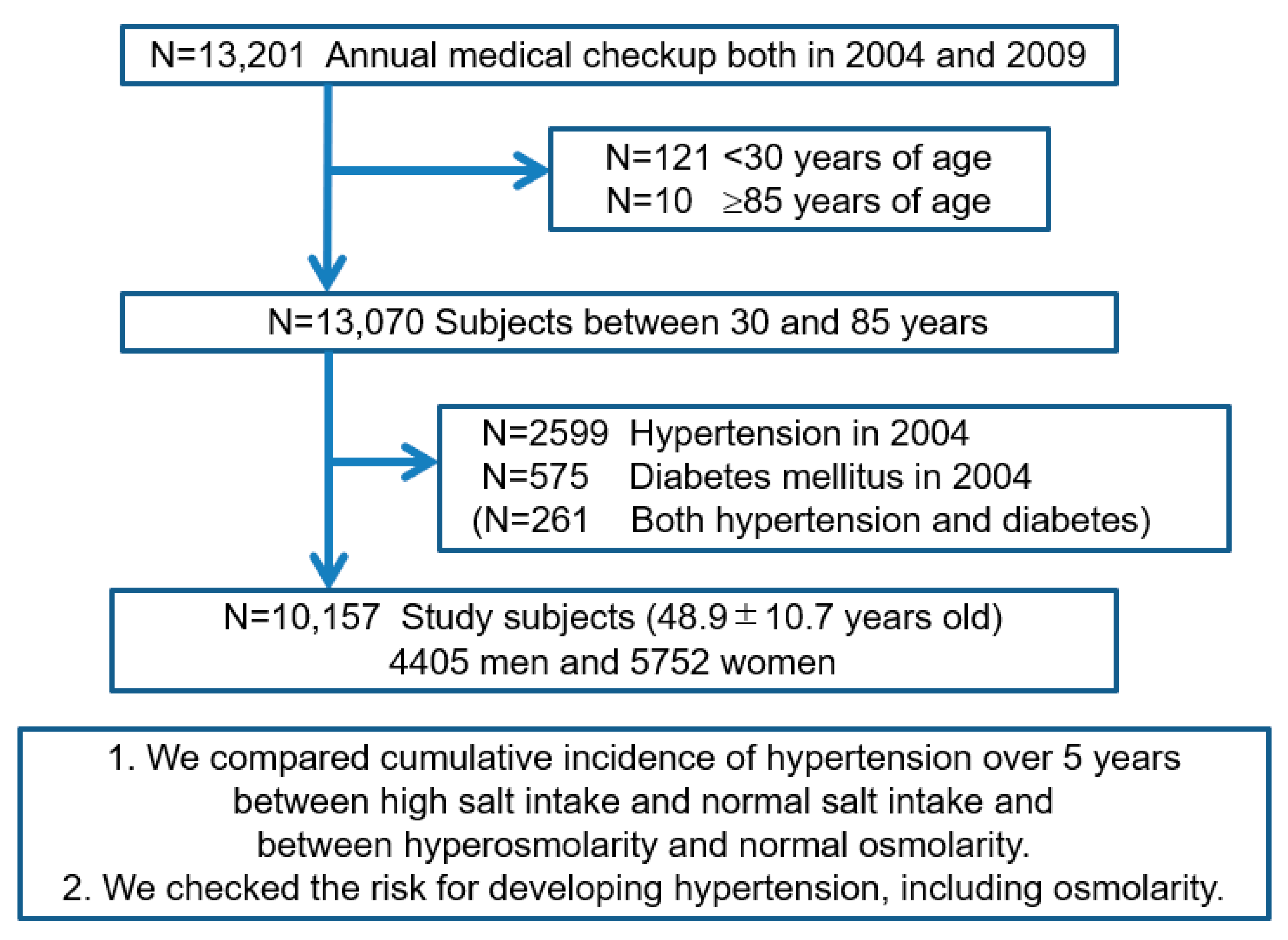
2.1. Study Design and Study Subjects
2.2. Definition of Hypertension, Diabetes, Dyslipidemia, Hyperuricemia, Chronic Kidney Disease, and Serum Osmolarity
2.3. The Cutoff Point between Hyperosmolarity and Normal Osmolarity and between High Salt Intake and Normal Salt Intake
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Characteristics of Study Subjects
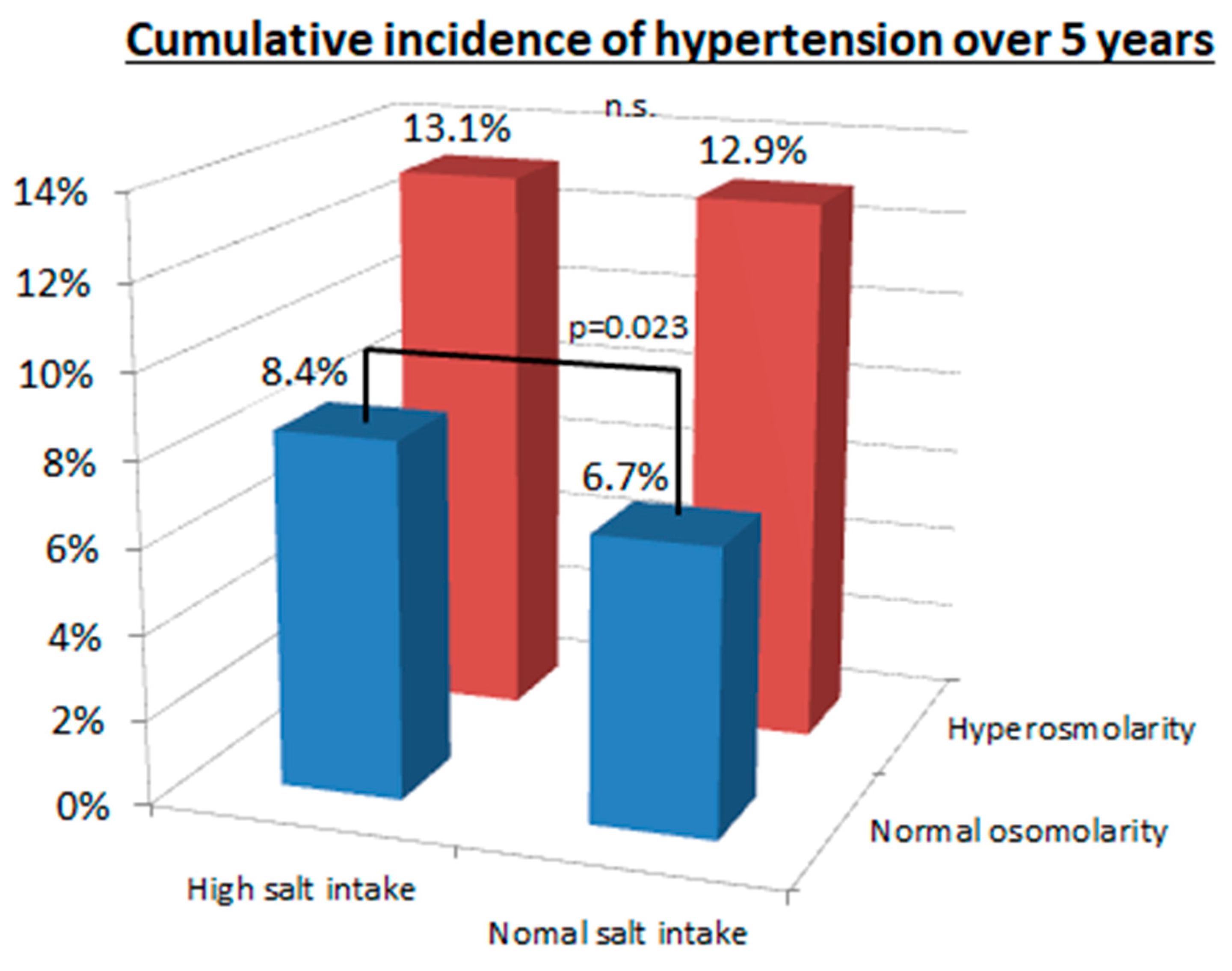
3.2. Cumulative Incidence of Hypertension over Five Years between Hyperosmolarity and Normal Osmolarity and between High and Normal Salt Intake
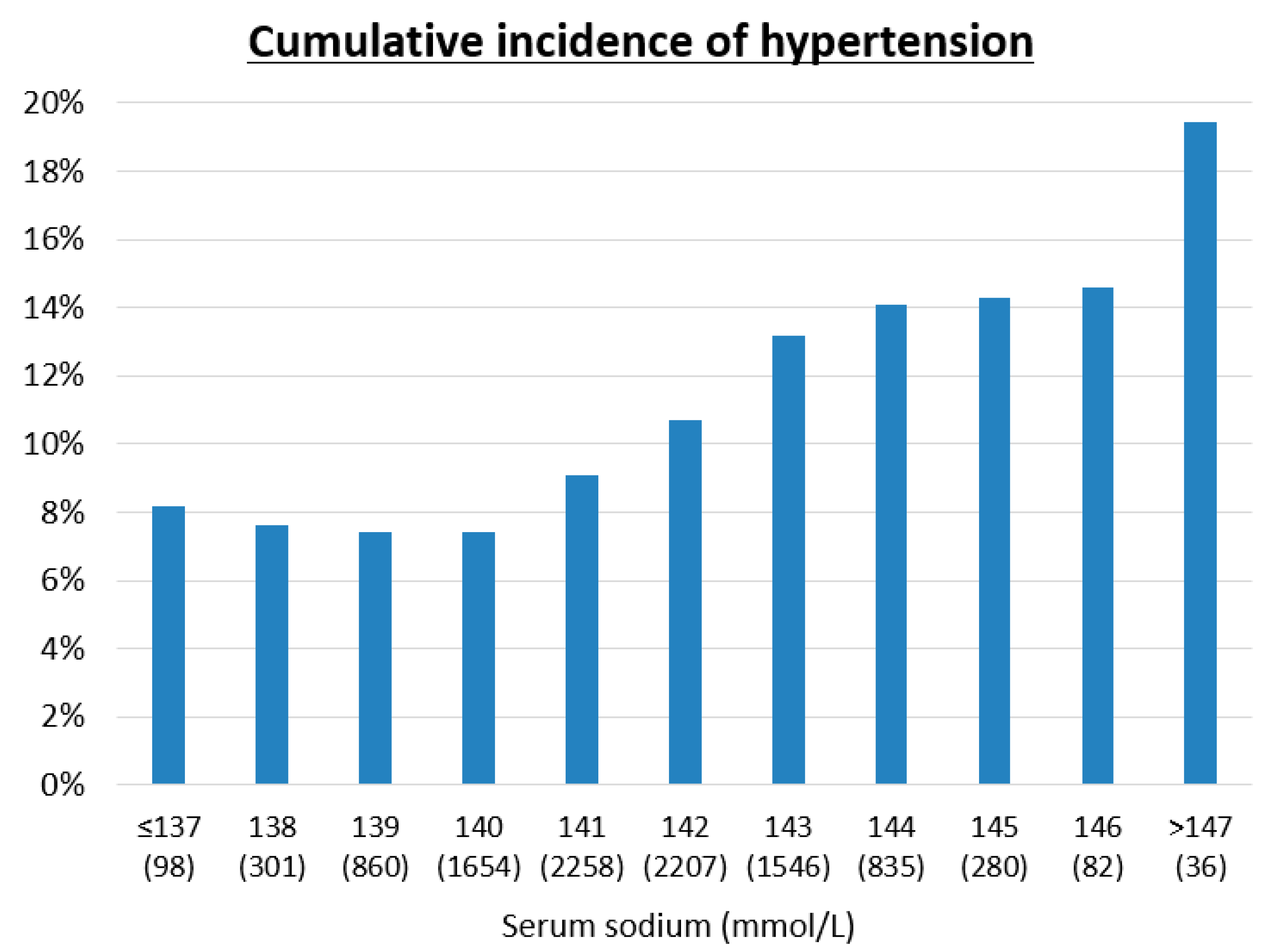
3.3. Risk Factors for Developing Hypertension
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar] [CrossRef]
- Henney, J.E.; Taylor, C.L.; Boon, C.S. (Eds.) Strategies to Reduce Sodium Intake in the United States; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Lanaspa, M.A.; Kuwabara, M.; Andres-Hernando, A.; Li, N.; Cicerchi, C.; Jensen, T.; Orlicky, D.J.; Roncal-Jimenez, C.A.; Ishimoto, T.; Nakagawa, T.; et al. High salt intake causes leptin resistance and obesity in mice by stimulating endogenous fructose production and metabolism. Proc. Natl. Acad. Sci. USA 2018, 115, 3138–3143. [Google Scholar] [CrossRef] [Green Version]
- Graudal, N.; Jurgens, G.; Baslund, B.; Alderman, M.H. Compared with usual sodium intake, low- and excessive-sodium diets are associated with increased mortality: A meta-analysis. Am. J. Hypertens. 2014, 27, 1129–1137. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; Wang, X.; Liu, L.; Yan, H.; Lee, S.F.; Mony, P.; Devanath, A.; et al. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N. Engl. J. Med. 2014, 371, 612–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wald, R.; Jaber, B.L.; Price, L.L.; Upadhyay, A.; Madias, N.E. Impact of hospital-associated hyponatremia on selected outcomes. Arch. Intern. Med. 2010, 170, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Iturbe, B.; Romero, F.; Johnson, R.J. Pathophysiological mechanisms of salt-dependent hypertension. Am. J. Kidney Dis. 2007, 50, 655–672. [Google Scholar] [CrossRef] [PubMed]
- Graudal, N.; Hubeck-Graudal, T.; Jurgens, G.; Taylor, R.S. Dose-response relation between dietary sodium and blood pressure: A meta-regression analysis of 133 randomized controlled trials. Am. J. Clin. Nutr. 2019, 109, 1273–1278. [Google Scholar] [CrossRef]
- Graudal, N.A.; Hubeck-Graudal, T.; Jurgens, G. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. Cochrane Database Syst. Rev. 2017, 4, CD004022. [Google Scholar] [CrossRef]
- Cowley, A.W., Jr.; Roman, R.J. The role of the kidney in hypertension. JAMA 1996, 275, 1581–1589. [Google Scholar] [CrossRef]
- Rodriguez-Iturbe, B.; Pons, H.; Johnson, R.J. Role of the Immune System in Hypertension. Physiol. Rev. 2017, 97, 1127–1164. [Google Scholar] [CrossRef]
- Kanbay, M.; Aslan, G.; Afsar, B.; Dagel, T.; Siriopol, D.; Kuwabara, M.; Incir, S.; Camkiran, V.; Rodriguez-Iturbe, B.; Lanaspa, M.A.; et al. Acute effects of salt on blood pressure are mediated by serum osmolality. J. Clin. Hypertens. (Greenwich) 2018, 20, 1447–1454. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Hisatome, I.; Roncal-Jimenez, C.A.; Niwa, K.; Andres-Hernando, A.; Jensen, T.; Bjornstad, P.; Milagres, T.; Cicerchi, C.; Song, Z.; et al. Increased Serum Sodium and Serum Osmolarity Are Independent Risk Factors for Developing Chronic Kidney Disease; 5 Year Cohort Study. PLoS ONE 2017, 12, e0169137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwabara, M.; Kuwabara, R.; Hisatome, I.; Niwa, K.; Roncal-Jimenez, C.A.; Bjornstad, P.; Andres-Hernando, A.; Sato, Y.; Jensen, T.; Garcia, G.; et al. “Metabolically Healthy” Obesity and Hyperuricemia Increase Risk for Hypertension and Diabetes: 5-year Japanese Cohort Study. Obesity (Silver Spring) 2017, 25, 1997–2008. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Niwa, K.; Hisatome, I.; Nakagawa, T.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Bjornstad, P.; Jensen, T.; Sato, Y.; Milagres, T.; et al. Asymptomatic Hyperuricemia Without Comorbidities Predicts Cardiometabolic Diseases: Five-Year Japanese Cohort Study. Hypertension 2017, 69, 1036–1044. [Google Scholar] [CrossRef]
- Kuwabara, M.; Borghi, C.; Cicero, A.F.G.; Hisatome, I.; Niwa, K.; Ohno, M.; Johnson, R.J.; Lanaspa, M.A. Elevated serum uric acid increases risks for developing high LDL cholesterol and hypertriglyceridemia: A five-year cohort study in Japan. Int. J. Cardiol. 2018, 261, 183–188. [Google Scholar] [CrossRef]
- Kuwabara, M.; Hisatome, I.; Niwa, K.; Hara, S.; Roncal-Jimenez, C.A.; Bjornstad, P.; Nakagawa, T.; Andres-Hernando, A.; Sato, Y.; Jensen, T.; et al. Uric Acid Is a Strong Risk Marker for Developing Hypertension From Prehypertension: A 5-Year Japanese Cohort Study. Hypertension 2018, 71, 78–86. [Google Scholar] [CrossRef]
- Kuwabara, M.; Chintaluru, Y.; Kanbay, M.; Niwa, K.; Hisatome, I.; Andres-Hernando, A.; Roncal-Jimenez, C.; Ohno, M.; Johnson, R.J.; Lanaspa, M.A. Fasting blood glucose is predictive of hypertension in a general Japanese population. J. Hypertens. 2019, 37, 167–174. [Google Scholar] [CrossRef]
- Kuwabara, M.; Bjornstad, P.; Hisatome, I.; Niwa, K.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Jensen, T.; Milagres, T.; Sato, Y.; Garcia, G.; et al. Elevated Serum Uric Acid Level Predicts Rapid Decline in Kidney Function. Am. J. Nephrol. 2017, 45, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Kuwabara, M.; Hisatome, I.; Niwa, K.; Bjornstad, P.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Kanbay, M.; Johnson, R.J.; Lanaspa, M.A. The Optimal Range of Serum Uric Acid for Cardiometabolic Diseases: A 5-Year Japanese Cohort Study. J. Clin. Med. 2020, 9, 942. [Google Scholar] [CrossRef] [Green Version]
- Kuwabara, M.; Niwa, K.; Ohno, M.; Hisatome, I. High rate of calories from protein is associated with higher prevalence of hypertension. J. Hum. Hypertens. 2019, 33, 340–344. [Google Scholar] [CrossRef]
- Grootenhuis, P.A.; Westenbrink, S.; Sie, C.M.; de Neeling, J.N.; Kok, F.J.; Bouter, L.M. A semiquantitative food frequency questionnaire for use in epidemiologic research among the elderly: Validation by comparison with dietary history. J. Clin. Epidemiol. 1995, 48, 859–868. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, N.; Tokudome, S. Reproducibility of self-administered questionnaire in epidemiological surveys. J. Epidemiol. 1997, 7, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Shimamoto, K.; Ando, K.; Fujita, T.; Hasebe, N.; Higaki, J.; Horiuchi, M.; Imai, Y.; Imaizumi, T.; Ishimitsu, T.; Ito, M.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2014). Hypertens. Res. 2014, 37, 253–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Bohm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [CrossRef] [Green Version]
- International Expert, C. International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teramoto, T.; Sasaki, J.; Ishibashi, S.; Birou, S.; Daida, H.; Dohi, S.; Egusa, G.; Hiro, T.; Hirobe, K.; Iida, M.; et al. Executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan -2012 version. J. Atheroscler Thromb. 2013, 20, 517–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamanaka, H.; Japanese Society of, G.; Nucleic Acid, M. Japanese guideline for the management of hyperuricemia and gout: Second edition. Nucleosides Nucleotides Nucleic Acids 2011, 30, 1018–1029. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, C.I.; Garcia-Webb, P.; Fletcher, E.; Beilby, J.P. Calculated vs measured plasma osmolalities revisited. Clin. Chem. 1984, 30, 1703–1705. [Google Scholar] [CrossRef]
- Suckling, R.J.; He, F.J.; Markandu, N.D.; MacGregor, G.A. Dietary salt influences postprandial plasma sodium concentration and systolic blood pressure. Kidney Int. 2012, 81, 407–411. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.J.; Rodriguez-Iturbe, B.; Roncal-Jimenez, C.; Lanaspa, M.A.; Ishimoto, T.; Nakagawa, T.; Correa-Rotter, R.; Wesseling, C.; Bankir, L.; Sanchez-Lozada, L.G. Hyperosmolarity drives hypertension and CKD--water and salt revisited. Nat. Rev. Nephrol. 2014, 10, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, M.; Yilmaz, S.; Dincer, N.; Ortiz, A.; Sag, A.A.; Covic, A.; Sanchez-Lozada, L.G.; Lanaspa, M.A.; Cherney, D.Z.I.; Johnson, R.J.; et al. Antidiuretic Hormone and Serum Osmolarity Physiology and Related Outcomes: What Is Old, What Is New, and What Is Unknown? J. Clin. Endocrinol. Metab. 2019, 104, 5406–5420. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.R.; Stevens, W. Plasma hyperosmolality stimulates leptin secretion acutely by a vasopressin-adrenal mechanism. Am. J. Physiol. Endocrinol. Metab. 2004, 287, E263–E268. [Google Scholar] [CrossRef] [Green Version]
- Do Carmo, J.M.; da Silva, A.A.; Wang, Z.; Fang, T.; Aberdein, N.; de Lara Rodriguez, C.E.; Hall, J.E. Obesity-Induced Hypertension: Brain Signaling Pathways. Curr. Hypertens. Rep. 2016, 18, 58. [Google Scholar] [CrossRef] [Green Version]
- Blaustein, M.P.; Leenen, F.H.; Chen, L.; Golovina, V.A.; Hamlyn, J.M.; Pallone, T.L.; Van Huysse, J.W.; Zhang, J.; Wier, W.G. How NaCl raises blood pressure: A new paradigm for the pathogenesis of salt-dependent hypertension. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, H1031–H1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinewietfeld, M.; Manzel, A.; Titze, J.; Kvakan, H.; Yosef, N.; Linker, R.A.; Muller, D.N.; Hafler, D.A. Sodium chloride drives autoimmune disease by the induction of pathogenic TH17 cells. Nature 2013, 496, 518–522. [Google Scholar] [CrossRef]
- Titze, J.; Machnik, A. Sodium sensing in the interstitium and relationship to hypertension. Curr Opin Nephrol. Hypertens. 2010, 19, 385–392. [Google Scholar] [CrossRef]
- Ha, S.K. Dietary salt intake and hypertension. Electrolyte Blood Press 2014, 12, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Kitada, K.; Daub, S.; Zhang, Y.; Klein, J.D.; Nakano, D.; Pedchenko, T.; Lantier, L.; LaRocque, L.M.; Marton, A.; Neubert, P.; et al. High salt intake reprioritizes osmolyte and energy metabolism for body fluid conservation. J. Clin. Investig. 2017, 127, 1944–1959. [Google Scholar] [CrossRef] [Green Version]
- Bjornholt, J.V.; Erikssen, G.; Aaser, E.; Sandvik, L.; Nitter-Hauge, S.; Jervell, J.; Erikssen, J.; Thaulow, E. Fasting blood glucose: An underestimated risk factor for cardiovascular death. Results from a 22-year follow-up of healthy nondiabetic men. Diabetes Care 1999, 22, 45–49. [Google Scholar] [CrossRef]
- Tatsumi, Y.; Morimoto, A.; Asayama, K.; Sonoda, N.; Miyamatsu, N.; Ohno, Y.; Miyamoto, Y.; Izawa, S.; Ohkubo, T. Fasting Blood Glucose Predicts Incidence of Hypertension Independent of HbA1c Levels and Insulin Resistance in Middle-Aged Japanese: The Saku Study. Am. J. Hypertens. 2019, 32, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Hisatome, I. The Relationship Between Fasting Blood Glucose and Hypertension. Am. J. Hypertens. 2019, 32, 1143–1145. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, J.; Cai, W.; Peppa, M.; Goodman, S.; Ferrucci, L.; Striker, G.; Vlassara, H. Circulating glycotoxins and dietary advanced glycation endproducts: Two links to inflammatory response, oxidative stress, and aging. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 427–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilhovd, B.K.; Juutilainen, A.; Lehto, S.; Ronnemaa, T.; Torjesen, P.A.; Birkeland, K.I.; Berg, T.J.; Hanssen, K.F.; Laakso, M. High serum levels of advanced glycation end products predict increased coronary heart disease mortality in nondiabetic women but not in nondiabetic men: A population-based 18-year follow-up study. Arter. Thromb. Vasc. Biol. 2005, 25, 815–820. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, S.; Yanagibori, R.; Amano, K. Self-administered diet history questionnaire developed for health education: A relative validation of the test-version by comparison with 3-day diet record in women. J. Epidemiol. 1998, 8, 203–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total | Non-HT | HT | p | ||
|---|---|---|---|---|---|
| Number of subjects | 10,157 | 9117 | 1040 | ||
| Age | years old | 48.9 ± 10.7 | 48.3 ± 10.5 | 54.3 ± 10.7 | <0.001 |
| Male | % | 43.4 | 41.8 | 57.1 | <0.001 |
| Body mass index | kg/m2 | 22.0 ± 2.9 | 21.8 ± 2.9 | 23.4 ± 3.2 | <0.001 |
| Smoking | % | 36.3 | 35.5 | 40.8 | <0.001 |
| Drinking alcohol | % | 41.5 | 40.8 | 48.1 | <0.001 |
| Dyslipidemia | % | 34.6 | 33.2 | 47.2 | <0.001 |
| Hyperuricemia | % | 11.8 | 10.8 | 19.9 | <0.001 |
| Chronic kidney disease | % | 2.5 | 2.4 | 3.8 | 0.017 |
| Systolic blood pressure | mmHg | 113.0 ± 13.1 | 111.4 ±12.5 | 127.2 ± 8.7 | <0.001 |
| Diastolic blood pressure | mmHg | 70.5 ± 8.8 | 69.4 ± 8.4 | 79.8 ± 6.3 | <0.001 |
| Fasting blood glucose | mg/dL | 96.9 ± 8.6 | 96.5 ± 8.4 | 100.4 ± 9.3 | <0.001 |
| Blood urea nitrogen | mg/dL | 13.8 ± 3.3 | 13.7 ± 3.3 | 14.4 ± 3.6 | <0.001 |
| Serum sodium | mmol/L | 141.5 ± 1.8 | 141.4 ± 1.7 | 141.9 ± 1.8 | <0.001 |
| Serum potassium | mmol/L | 4.18 ± 0.28 | 4.18 ± 0.28 | 4.21 ± 0.29 | <0.001 |
| Serum osmolarity | mOsmol/L | 293.3 ± 4.0 | 293.1 ± 3.9 | 294.5 ± 3.9 | <0.001 |
| Estimated GFR | mL/min/1.73 m2 | 86.7 ± 15.3 | 87.1 ± 15.3 | 83.5 ± 15.1 | <0.001 |
| Salt intake | g/day | 12.2 ± 3.7 | 12.2 ± 3.6 | 12.6 ± 3.9 | 0.046 |
| (A) | |||||
| Osmolarity (mOsmol/L) | ≤290 | 290–293 | 293–296 | >296 | P |
| Number of subjects | 2128 | 2663 | 2873 | 2493 | |
| Cumulative incidence | 6.3% | 8.4% | 10.9% | 14.8% | <0.001 |
| (B) | |||||
| Salt intake (g/day) | ≤10 | 10–12 | 12–14 | >14 | P |
| Number of subjects | 2925 | 2320 | 2061 | 2842 | |
| Cumulative incidence | 9.3% | 10.1% | 9.7% | 11.7% | 0.006 |
| (A) | OR | 95% CI | p | |
| Age | per 1 year increase | 1.052 | 1.045–1.059 | <0.001 |
| Men | versus women | 1.006 | 0.847–1.195 | 0.95 |
| Body mass index | per 1 kg/m2 increase | 1.170 | 1.145–1.203 | <0.001 |
| Smoking habits | versus negative | 1.012 | 0.867–1.182 | 0.88 |
| Drinking alcohol | versus negative | 1.297 | 1.120–1.502 | <0.001 |
| Dyslipidemia | versus negative | 1.047 | 0.909–1.206 | 0.52 |
| Hyperuricemia | versus negative | 1.295 | 1.070–1.568 | 0.008 |
| Chronic kidney disease | versus negative | 0.710 | 0.493–1.023 | 0.71 |
| Serum osmolarity | per 1 mOsm/L increase | 1.025 | 1.006–1.044 | 0.010 |
| Salt intake | per 1 g/day increase | 0.996 | 0.979–1.014 | 0.66 |
| (B) | OR | 95% CI | p | |
| Age | per 1 year increase | 1.051 | 1.043–1.058 | <0.001 |
| Gender (Male) | versus women | 0.965 | 0.809–1.151 | 0.69 |
| Body mass index | per 1 kg/m2 increase | 1.162 | 1.133–1.191 | <0.001 |
| Smoking habits | versus negative | 1.001 | 0.857–1.170 | 0.99 |
| Drinking alcohol | versus negative | 1.248 | 1.076–1.447 | 0.003 |
| Dyslipidemia | versus negative | 1.030 | 0.894–1.187 | 0.68 |
| Hyperuricemia | versus negative | 1.290 | 1.065–1.562 | 0.009 |
| Chronic kidney disease | versus negative | 0.743 | 0.514–1.073 | 0.113 |
| Blood urea nitrogen | per 1 mg/dL increased | 0.999 | 0.977–1.021 | 0.90 |
| Serum sodium | per 1 mmol/L increased | 1.045 | 1.005–1.087 | 0.028 |
| Fasting blood glucose | per 1 mg/dL increased | 1.018 | 1.010–1.026 | <0.001 |
| Salt intake | per 1 g/day increased | 0.996 | 0.978–1.014 | 0.66 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuwabara, M.; Kanbay, M.; Niwa, K.; Ae, R.; Andres-Hernando, A.; Roncal-Jimenez, C.A.; Garcia, G.; Sánchez-Lozada, L.G.; Rodriguez-Iturbe, B.; Hisatome, I.; et al. Hyperosmolarity and Increased Serum Sodium Concentration Are Risks for Developing Hypertension Regardless of Salt Intake: A Five-Year Cohort Study in Japan. Nutrients 2020, 12, 1422. https://doi.org/10.3390/nu12051422
Kuwabara M, Kanbay M, Niwa K, Ae R, Andres-Hernando A, Roncal-Jimenez CA, Garcia G, Sánchez-Lozada LG, Rodriguez-Iturbe B, Hisatome I, et al. Hyperosmolarity and Increased Serum Sodium Concentration Are Risks for Developing Hypertension Regardless of Salt Intake: A Five-Year Cohort Study in Japan. Nutrients. 2020; 12(5):1422. https://doi.org/10.3390/nu12051422
Chicago/Turabian StyleKuwabara, Masanari, Mehmet Kanbay, Koichiro Niwa, Ryusuke Ae, Ana Andres-Hernando, Carlos A Roncal-Jimenez, Gabriela Garcia, Laura Gabriela Sánchez-Lozada, Bernardo Rodriguez-Iturbe, Ichiro Hisatome, and et al. 2020. "Hyperosmolarity and Increased Serum Sodium Concentration Are Risks for Developing Hypertension Regardless of Salt Intake: A Five-Year Cohort Study in Japan" Nutrients 12, no. 5: 1422. https://doi.org/10.3390/nu12051422
APA StyleKuwabara, M., Kanbay, M., Niwa, K., Ae, R., Andres-Hernando, A., Roncal-Jimenez, C. A., Garcia, G., Sánchez-Lozada, L. G., Rodriguez-Iturbe, B., Hisatome, I., Lanaspa, M. A., & Johnson, R. J. (2020). Hyperosmolarity and Increased Serum Sodium Concentration Are Risks for Developing Hypertension Regardless of Salt Intake: A Five-Year Cohort Study in Japan. Nutrients, 12(5), 1422. https://doi.org/10.3390/nu12051422