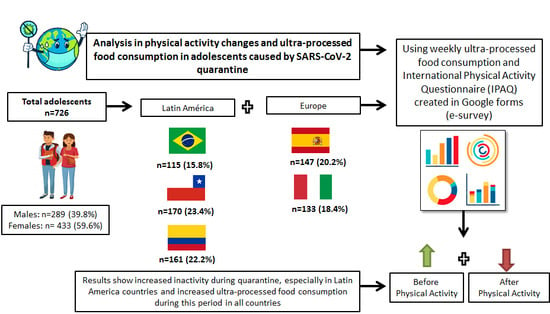
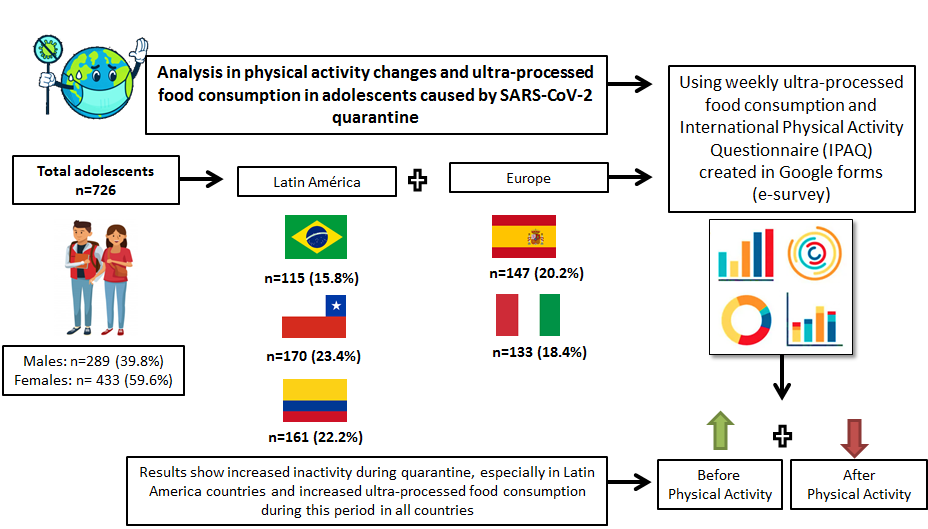
Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study

 ,
,  ,
,  ,
,  , , ,
, , ,  ,
,  ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population, Eligibility Criteria
2.3. Data Privacity
2.4. Data Collection
2.5. Data Processing and Statistical Analysis
2.6. Ethical Issues
3. Results
Socio-Demographic Characteristics and Physical Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 4 April 2020).
- World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 4 April 2020).
- Scarmozzino, F.; Visioli, F. Covid-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The influence of physical activity, sedentary behavioron health related quality of life among the general population of children and adolescents: A systematic review. PLoS ONE 2017, 9, e0187668. [Google Scholar]
- Bann, D.; Sholes, S.; Fluharty, M.; Shure, N. Adolescents’ physicalactivity: Cross-National comparisons of levels, distributions and disparities across 52 countries. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Cureau, F.V.; Da Silva, T.L.N.; Bloch, K.V.; Fujimori, E.; Belfort, D.R.; De Carvalho, K.M.B.; De Leon, E.B.; De Vasconcellos, M.T.L.; Ekelund, U.; Schaan, B.D. ERICA: Leisure-Time physical inactivity in Brazilian adolescents. Rev. Saúde Pública 2016, 50. [Google Scholar] [CrossRef] [PubMed]
- Enes, C.C.; Camargo, C.M.; Justino, M.I.C. Consumo de alimentos ultraprocessados e obesidade em adolescentes. Rev. Nutr. 2019, 32, 170–180. [Google Scholar]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- R Development Core Team. R Foundation for Statistical Computing; R Development Core Team: Vienna, Austria, 2008. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy-Costa, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2017, 21, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows; Version 24.0; IBM Corporation: Armonk, NY, USA, 2016. [Google Scholar]
- Pinto, R.O.; Pattussi, M.P.; Fontoura, L.P.; Poletto, S.; Grapiglia, V.L.; Balbinot, A.D.; Teixeira, V.A.; Horta, R.L. Validação de instrumento desenvolvido para avaliação da promoção de saúde na escola. Rev. Saúde Pública 2016, 50, 2. [Google Scholar] [PubMed] [Green Version]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu, N.; Dias, I.; Cascais, M.; Luz, A.; Moleiro, P. Quais os diagnósticos mais frequentes na adolescência? A realidade de uma consulta de Medicina do Adolescente. Einstein São Paulo 2018, 16, eAO4225. [Google Scholar] [PubMed]
- Tremblay, M.S.; Barnes, J.D.; González, S.A.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R.; GMR Team. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S343–S366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, J.J.; Tremblay, M.S.; Léger, L.; Olds, T.; Tomkinson, G.R. International variability in 20 m shuttle run performance in children and youth: Who are the fittest from a 50-country comparison? A systematic literature review with pooling of aggregate results. Br. J. Sports Med. 2016, 52, 276. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Public Health. Time to tackle the physical activity gender gap. Lancet Public Health 2019, 4, e360. [Google Scholar] [CrossRef]
- Laird, Y.; Fawkner, S.; Kelly, P.; McNamee, L.; Niven, A. The role of social support on physical activity behaviour in adolescent girls: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 79. [Google Scholar] [CrossRef] [Green Version]
- Mediouni, M.; Madiouni, R.; Kaczor-Urbanowicz, K.E. COVID-19: How the Quarantine could lead to the Depreobesity. Obes. Med. 2020, 100255. [Google Scholar] [CrossRef]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Elgar, F.J.; Pförtner, T.-K.; Moor, I.; De Clercq, B.; Stevens, G.W.J.M.; Currie, C. Socioeconomic inequalities in adolescent health 2002–2010: A time-series analysis of 34 countries participating in the Health Behaviour in School-aged Children study. Lancet 2015, 385, 2088–2095. [Google Scholar] [CrossRef] [Green Version]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Rauber, F.; Campagnolo, P.D.; Hoffman, D.J.; Vitolo, M.R. Consumption of ultra-processed food products and its effects on children’s lipid profiles: A longitudinal study. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 116–122. [Google Scholar] [CrossRef]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Returning Chinese school-aged children and adolescents to physical activity in the wake of COVID-19: Actions and precautions. J. Sport Health Sci. 2020. ahead of print. [Google Scholar] [CrossRef]
- Levy, R.B.; De Castro, I.R.R.; Cardoso, L.D.O.; Tavares, L.F.; Sardinha, L.M.V.; Gomes, F.D.S.; Da Costa, A.W.N. Consumo e comportamento alimentar entre adolescentes brasileiros: Pesquisa Nacional de Saúde do Escolar (PeNSE), 2009. Ciênc. Saúde Colet. 2010, 15, 3085–3097. [Google Scholar] [CrossRef]
- Santaliestra-Pasías, A.M.; Mouratidou, T.; Verbestel, V.; Huybrechts, I.; Gottrand, F.; Le Donne, C.; Cuenca-García, M.; Díaz, L.E.; Kafatos, A.; Manios, Y.; et al. Food Consumption and Screen-Based Sedentary Behaviors in European Adolescents: The Helena study. Arch. Pediatr. Adolesc. Med. 2012, 166, 1010–1020. [Google Scholar] [CrossRef] [Green Version]
- Pearson, N.; Biddle, S.J.H. Sedentary Behavior and Dietary Intake in Children, Adolescents, and Adults: A systematic review. Am. J. Prev. Med. 2011, 41, 178–188. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos Costa, C.; Ramos Flores, T.; Wendt, A.; Garcia Neves, R.; Formoso Assunção, M.C.; Santos, I.S. Comportamento sedentário e consumo de alimentos ultraprocessados entre adolescentes brasileiros: Pesquisa Nacional de Saúde do Escolar (PeNSE), 2015. Cad. Saúde Pública 2018, 34, 1–12. [Google Scholar]
- Mais, L.A.; Warkentin, S.; Latorre, M.D.R.D.D.O.; Carnell, S.; Taddei, J.A.A.D.C. Parental Feeding Practices among Brazilian School-Aged Children: Associations with Parent and Child Characteristics. Front. Nutr. 2017, 4, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rydén, P.J.; Hagfors, L. Diet cost, diet quality and socio-economic position: How are they related and what contributes to differences in diet costs? Public Health Nutr. 2011, 14, 1680–1692. [Google Scholar] [CrossRef] [Green Version]
- Molina, M.B.; Lopéz, P.M.; Faria, C.P.; Cade, N.V. Zandonade, E. Preditores socioeconômicos da qualidade da alimentação de crianças. Rev. Saúde Pública 2010, 44, 732–785. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Alvira, J.M.; Mouratidou, T.; Bammann, K.; Hebestreit, A.; Barba, G.; Sieri, S.; Reisch, L.; Eiben, G.; Hadjigeorgiou, C.; Kovacs, E.; et al. Parental education and frequency of food consumption in European children: The IDEFICS study. Public Health Nutr. 2012, 16, 487–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Roso, M.B.; Padilha, P.D.C.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Peres, W.A.F.; Martorell, M.; Aires, M.T.; Cardoso, L.D.O.; et al. Covid-19 Confinement and Changes of Adolescent’s Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef]
- Hallal, P.; Knuth, A.G.; Cruz, D.K.A.; Mendes, M.I.; Malta, D.C. Prática de atividade física em adolescentes brasileiros. Ciênc. Saúde Colet. 2010, 15, 3035–3042. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Brazil (n = 115) | Chile (n = 170) | Colombia (n = 161) | Spain (n = 147) | Italy (n = 133) | Overall (n = 726) | |
|---|---|---|---|---|---|---|
| Age group (years) | ||||||
| 10–15 | 67 (58.3%) | 106 (62.4%) | 49 (30.4%) | 66 (44.9%) | 44 (33.1%) | 332 (45.7%) |
| 16–19 | 48 (41.7%) | 64 (37.6%) | 112 (69.6%) | 81 (55.1%) | 89 (66.9%) | 394 (54.3%) |
| Sex | ||||||
| Female | 65 (56.5%) | 97 (57.1%) | 91 (56.5%) | 87 (59.2%) | 93 (69.9%) | 433 (59.6%) |
| Male | 50 (43.5%) | 72 (42.4%) | 69 (42.9%) | 60 (40.8%) | 38 (28.6%) | 289 (39.8%) |
| Maternal education | ||||||
| Middle school or less | 7 (6.1%) | 20 (11.8%) | 17 (10.6%) | 21 (14.3%) | 1 (0.8%) | 66 (9.1%) |
| High school | 13 (11.3%) | 42 (24.7%) | 104 (64.6%) | 28 (19.0%) | 44 (33.1%) | 231 (31.8%) |
| College | 91 (79.1%) | 105 (61.8%) | 35 (21.7%) | 92 (62.6%) | 81 (60.9%) | 404 (55.6%) |
| Does not know | 4 (3.5%) | 3 (1.8%) | 5 (3.1%) | 6 (4.1%) | 7 (5.3%) | 25 (3.4%) |
| Number of residents at home | ||||||
| 1–3 people | 48 (41.7%) | 60 (35.3%) | 31 (19.3%) | 23 (15.6%) | 23 (17.3%) | 185 (25.5%) |
| 4 or more people | 67 (58.3%) | 110 (63.5%) | 130 (80.7%) | 124 (83.7%) | 110 (82.7%) | 541 (74.1%) |
| Lives with the father | ||||||
| Does not live | 0 (0%) | 63 (37.1%) | 41 (25.5%) | 24 (16.3%) | 15 (11.3%) | 143 (19.7%) |
| Lives | 115 (100%) | 107 (62.9%) | 120 (74.5%) | 123 (83.7%) | 118 (88.7%) | 583 (80.3%) |
| Lives with the mother | ||||||
| Does not live | 9 (7.8%) | 7 (4.1%) | 24 (14.9%) | 4 (2.7%) | 2 (1.5%) | 46 (6.3%) |
| Lives | 106 (92.2%) | 163 (95.9%) | 137 (85.1%) | 143 (97.3%) | 131 (98.5%) | 680 (93.7%) |
| PA 1 before | ||||||
| Inactive | 47 (40.9%) | 136 (80.0%) | 117 (72.7%) | 116 (78.9%) | 114 (85.7%) | 530 (73.0%) |
| Active | 68 (59.1%) | 34 (20.0%) | 44 (27.3%) | 31 (21.1%) | 19 (14.3%) | 196 (27.0%) |
| PA1 during | ||||||
| Inactive | 107 (93.0%) | 154 (90.6%) | 114 (70.8%) | 104 (70.7%) | 98 (73.7%) | 577 (79.5%) |
| Active | 8 (7.0%) | 16 (9.4%) | 47 (29.2%) | 43 (29.3%) | 35 (26.3%) | 149 (20.5%) |
| PA status | ||||||
| Active before/during | 6 (5.2%) | 7 (4.1%) | 23 (14.3%) | 15 (10.2%) | 12 (9.0%) | 63 (8.7%) |
| Active during | 2 (1.7%) | 9 (5.3%) | 24 (14.9%) | 28 (19.0%) | 23 (17.3%) | 86 (11.8%) |
| Not active before/during | 45 (39.1%) | 127 (74.7%) | 93 (57.8%) | 88 (59.9%) | 91 (68.4%) | 444 (61.2%) |
| Not active during | 62 (53.9%) | 27 (15.9%) | 21 (13.0%) | 16 (10.9%) | 7 (5.3%) | 133 (18.3%) |
| Change in PA status | ||||||
| Status changed | 64 (55.7%) | 36 (21.2%) | 45 (28.0%) | 44 (29.9%) | 30 (22.6%) | 219 (30.2%) |
| Status did not change | 51 (44.3%) | 134 (78.8%) | 116 (72.0%) | 103 (70.1%) | 103 (77.4%) | 507 (69.8%) |
| Ultra-processed foods consumption | ||||||
| ≥5 ×/week | 70 (60.9%) | 118 (69.4%) | 96 (59.6%) | 115 (78.2%) | 88 (66.1%) | 487 (81.3%) |
| ≤5 ×/week | 45 (39.1%) | 52 (22.6%) | 65 (41.4%) | 32 (21.8%) | 45 (33.9%) | 239 (18.7%) |
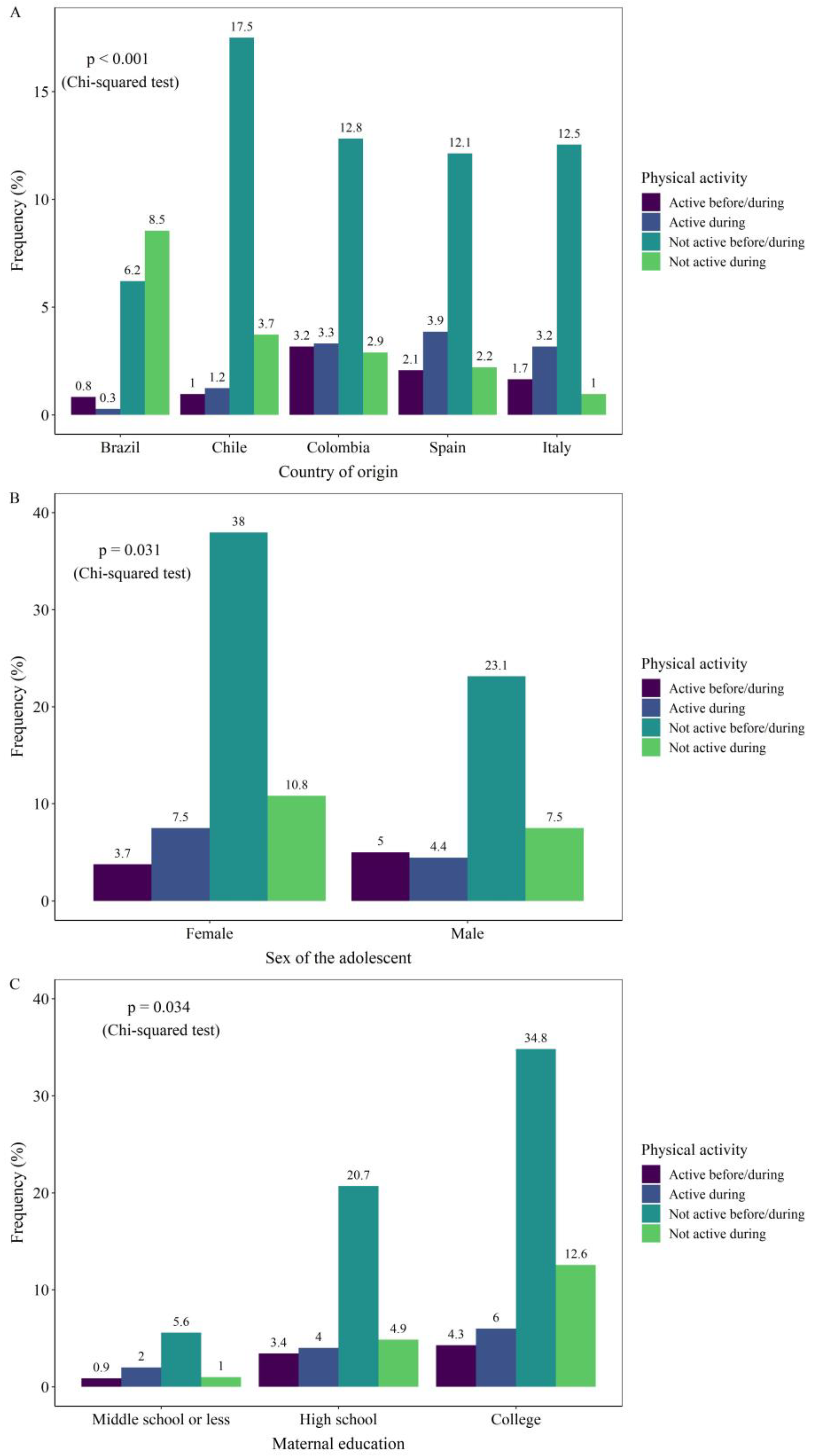
| Active Before/During (n = 63) | Active During (n = 86) | Not Active Before/During (n = 444) | Not Active During (n = 133) | p-Value * | |
|---|---|---|---|---|---|
| Country | |||||
| Brazil | 6 (9.5%) | 2 (2.3%) | 45 (10.1%) | 62 (46.6%) | <0.001 |
| Chile | 7 (11.1%) | 9 (10.5%) | 127 (28.6%) | 27 (20.3%) | |
| Colombia | 23 (36.5%) | 24 (27.9%) | 93 (20.9%) | 21 (15.8%) | |
| Spain | 15 (23.8%) | 28 (32.6%) | 88 (19.8%) | 16 (12.0%) | |
| Italy | 12 (19.0%) | 23 (26.7%) | 91 (20.5%) | 7 (5.3%) | |
| Continent | |||||
| Europe | 27 (42.9%) | 51 (59.3%) | 179 (40.3%) | 23 (17.3%) | <0.001 |
| Latin America | 36 (57.1%) | 35 (40.7%) | 265 (59.7%) | 110 (82.7%) | |
| Age group (years) | |||||
| 10–15 | 25 (39.7%) | 40 (46.5%) | 204 (45.9%) | 63 (47.4%) | 0.777 |
| 16–19 | 38 (60.3%) | 46 (53.5%) | 240 (54.1%) | 70 (52.6%) | |
| Sex | |||||
| Female | 27 (42.9%) | 54 (62.8%) | 274 (61.7%) | 78 (58.6%) | 0.031 |
| Male | 36 (57.1%) | 32 (37.2%) | 167 (37.6%) | 54 (40.6%) | |
| Maternal education | |||||
| Middle school or less | 6 (9.5%) | 14 (16.3%) | 39 (8.8%) | 7 (5.3%) | 0.034 |
| High school | 24 (38.1%) | 28 (32.6%) | 145 (32.7%) | 34 (25.6%) | |
| College | 30 (47.6%) | 42 (48.8%) | 244 (55.0%) | 88 (66.2%) | |
| Does not know | 3 (4.8%) | 2 (2.3%) | 16 (3.6%) | 4 (3.0%) | |
| Number of residents at home | |||||
| 1–3 people | 8 (12.7%) | 16 (18.6%) | 112 (25.2%) | 49 (36.8%) | 0.001 |
| 4 or more people | 55 (87.3%) | 70 (81.4%) | 329 (74.1%) | 84 (63.2%) | |
| Lives with the father | |||||
| Does not live | 12 (19.0%) | 20 (23.3%) | 90 (20.3%) | 21 (15.8%) | 0.556 |
| Lives | 51 (81.0%) | 66 (76.7%) | 354 (79.7%) | 112 (84.2%) | |
| Lives with the mother | |||||
| Does not live | 3 (4.8%) | 5 (5.8%) | 28 (6.3%) | 10 (7.5%) | 0.893 |
| Lives | 60 (95.2%) | 81 (94.2%) | 416 (93.7%) | 123 (92.5%) |
| Active Before/During * | Active During * | Inactive During * | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Crude model | ||||||
| Continent | ||||||
| Latin America ** | 0.90 (0.53–1.54) | 0.701 | 0.46 (0.29–0.74) | 0.001 | 3.23 (1.98–5.26) | <0.001 |
| Adjusted model | ||||||
| Continent | ||||||
| Latin America | 0.85 (0.48–.51) | 0.586 | 0.42 (0.26–0.70) | 0.001 | 2.98 (1.80–4.94) | <0.001 |
| Sex | ||||||
| Male | 2.22 (1.28–3.86) | 0.005 | 1.04 (0.63–1.70) | 0.878 | 0.96 (0.63–1.46) | 0.858 |
| Maternal education | ||||||
| High school | 0.99 (0.37–2.62) | 0.982 | 0.53 (0.25–1.12) | 0.096 | 1.35 (0.55–3.32) | 0.507 |
| College | 0.69 (0.26–1.79) | 0.445 | 0.41 (0.20–0.84) | 0.015 | 2.32 (0.99–5.44) | 0.053 |
| Number of residents at home | ||||||
| 4 or more people | 2.40 (1.05–5.53) | 0.039 | 1.22 (0.67–2.24) | 0.518 | 0.65 (0.42–1.01) | 0.42 |
| Variables | Crude Model | Adjusted Model | ||||
|---|---|---|---|---|---|---|
| OR | IC95% | p | OR | IC95% | P | |
| Maternal Education | ||||||
| High School College | 0.73 EU | 0.45–1.21 | 0.130 | 0.76 EU | 0.44–1.21 | 0.235 |
| Time of Physical Activity | ||||||
| <60 min/day ≥60 min/day | 0.90 EU | 0.66–1.23 | 0.123 | 0.80 EU | 0.58–1.11 | 0.200 |
| Continent | ||||||
| Latin America Europe | 1.50 EU | 1.08–2.08 | 0.014 | 1.58 EU | 1.13–2.22 | 0.007 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. https://doi.org/10.3390/nu12082289
Ruíz-Roso MB, de Carvalho Padilha P, Matilla-Escalante DC, Brun P, Ulloa N, Acevedo-Correa D, Arantes Ferreira Peres W, Martorell M, Rangel Bousquet Carrilho T, de Oliveira Cardoso L, et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients. 2020; 12(8):2289. https://doi.org/10.3390/nu12082289
Chicago/Turabian StyleRuíz-Roso, María Belén, Patricia de Carvalho Padilha, Diana C. Matilla-Escalante, Paola Brun, Natalia Ulloa, Diofanor Acevedo-Correa, Wilza Arantes Ferreira Peres, Miquel Martorell, Thais Rangel Bousquet Carrilho, Letícia de Oliveira Cardoso, and et al. 2020. "Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study" Nutrients 12, no. 8: 2289. https://doi.org/10.3390/nu12082289
APA StyleRuíz-Roso, M. B., de Carvalho Padilha, P., Matilla-Escalante, D. C., Brun, P., Ulloa, N., Acevedo-Correa, D., Arantes Ferreira Peres, W., Martorell, M., Rangel Bousquet Carrilho, T., de Oliveira Cardoso, L., Carrasco-Marín, F., Paternina-Sierra, K., Lopez de las Hazas, M. -C., Rodriguez-Meza, J. E., Villalba-Montero, L. F., Bernabè, G., Pauletto, A., Taci, X., Cárcamo-Regla, R., ... Dávalos, A. (2020). Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients, 12(8), 2289. https://doi.org/10.3390/nu12082289