Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Methodology and Promotion
2.2. Statistical Analysis
3. Results
3.1. Participants
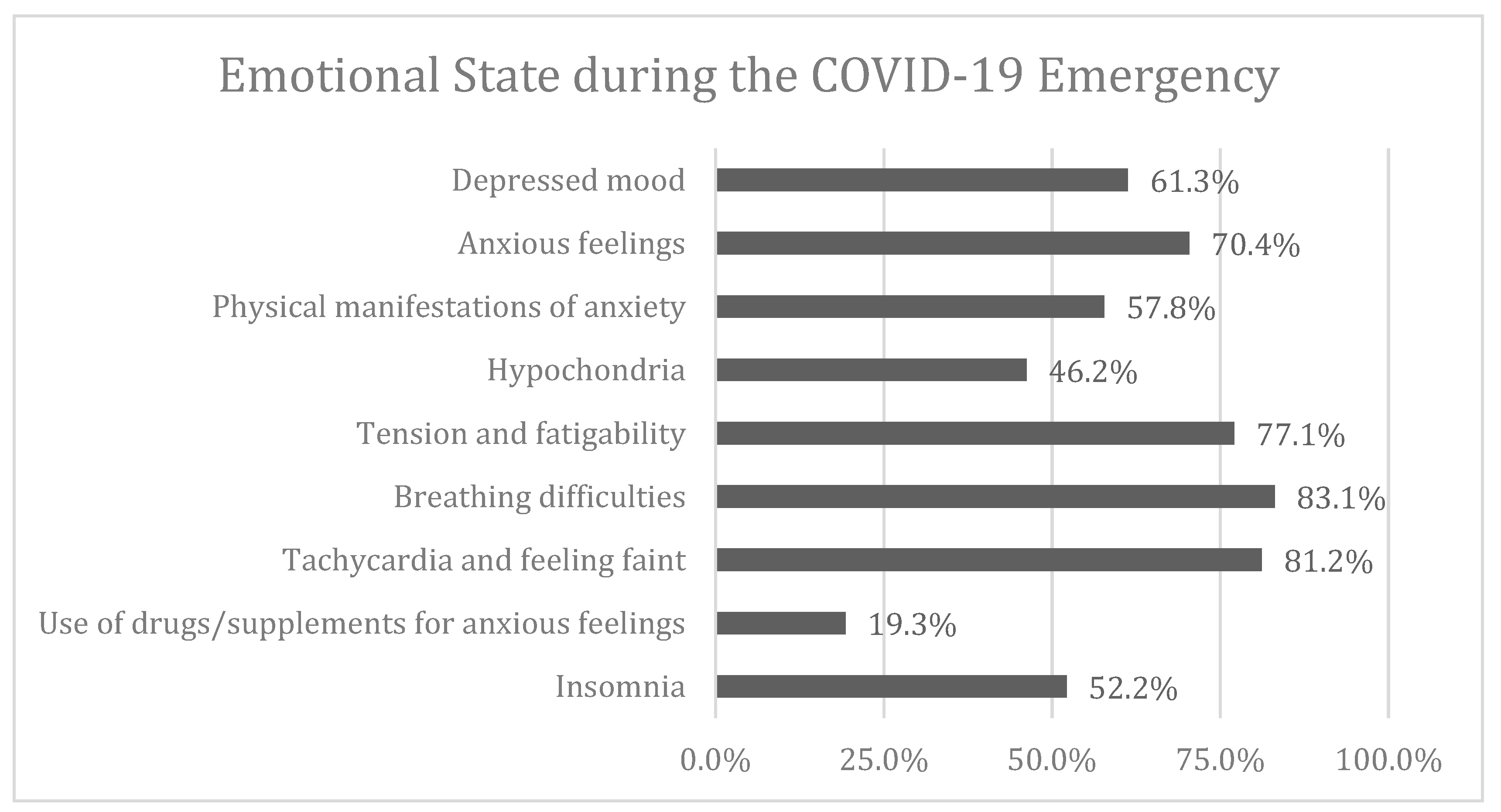
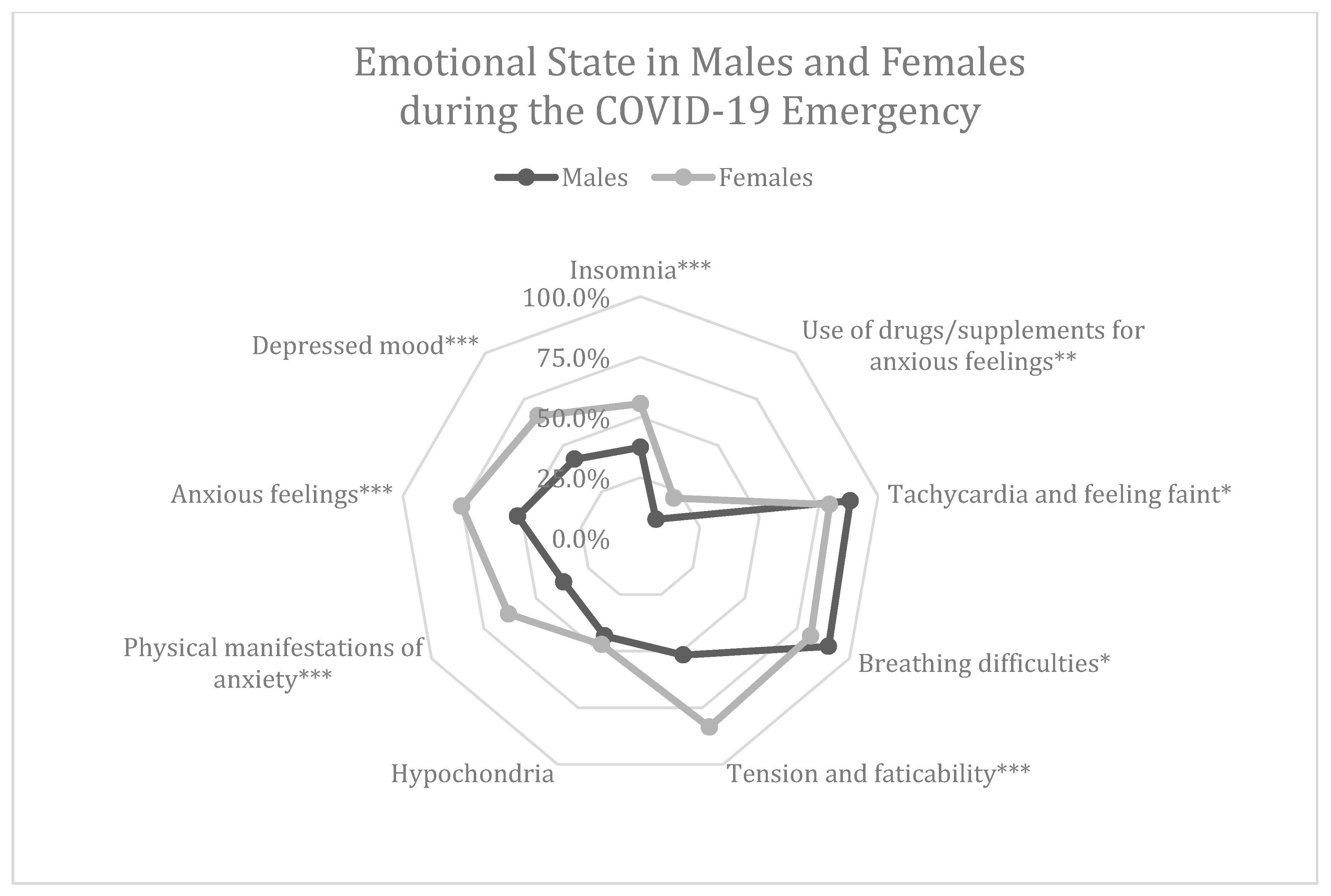
3.2. Emotional State during the COVID-19 Emergency
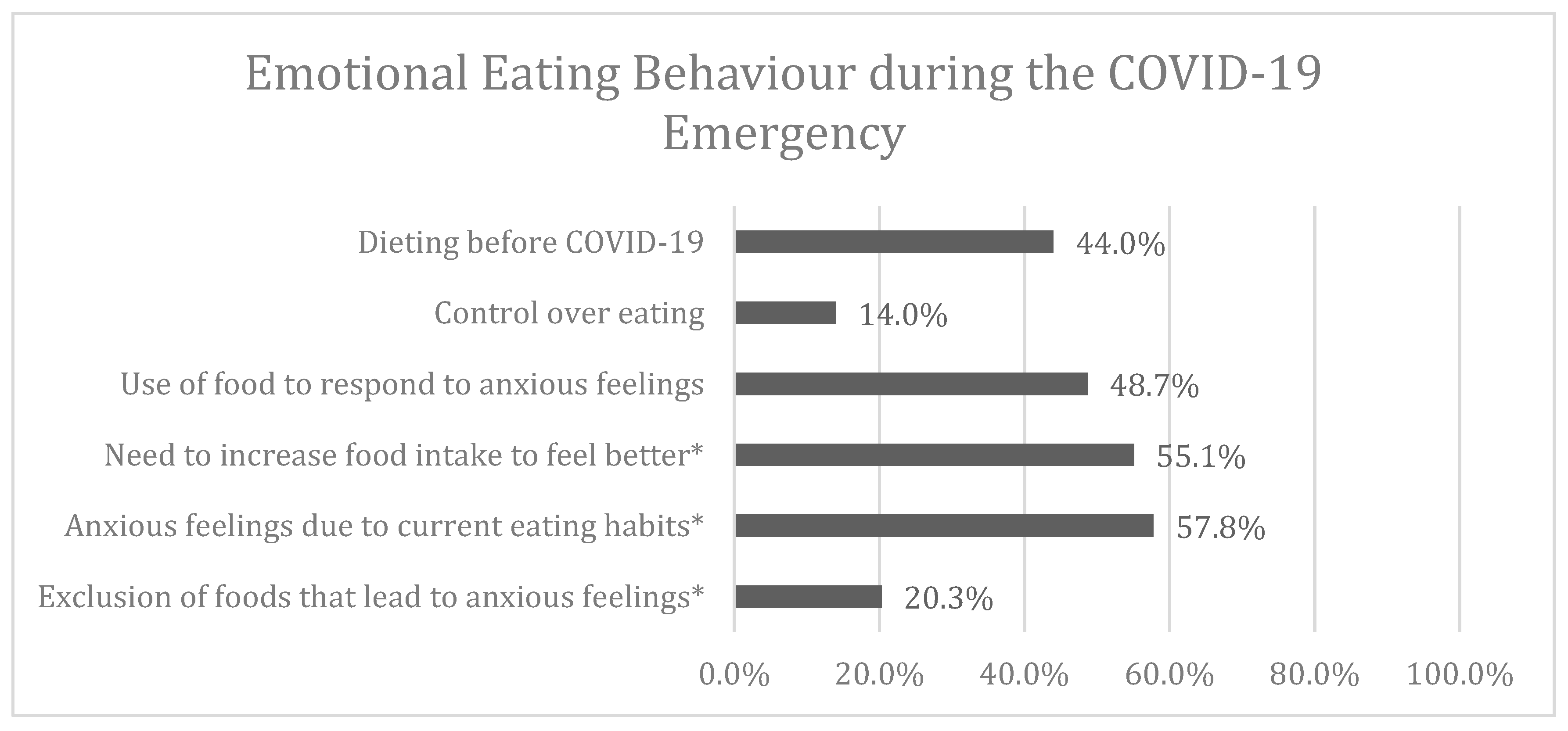
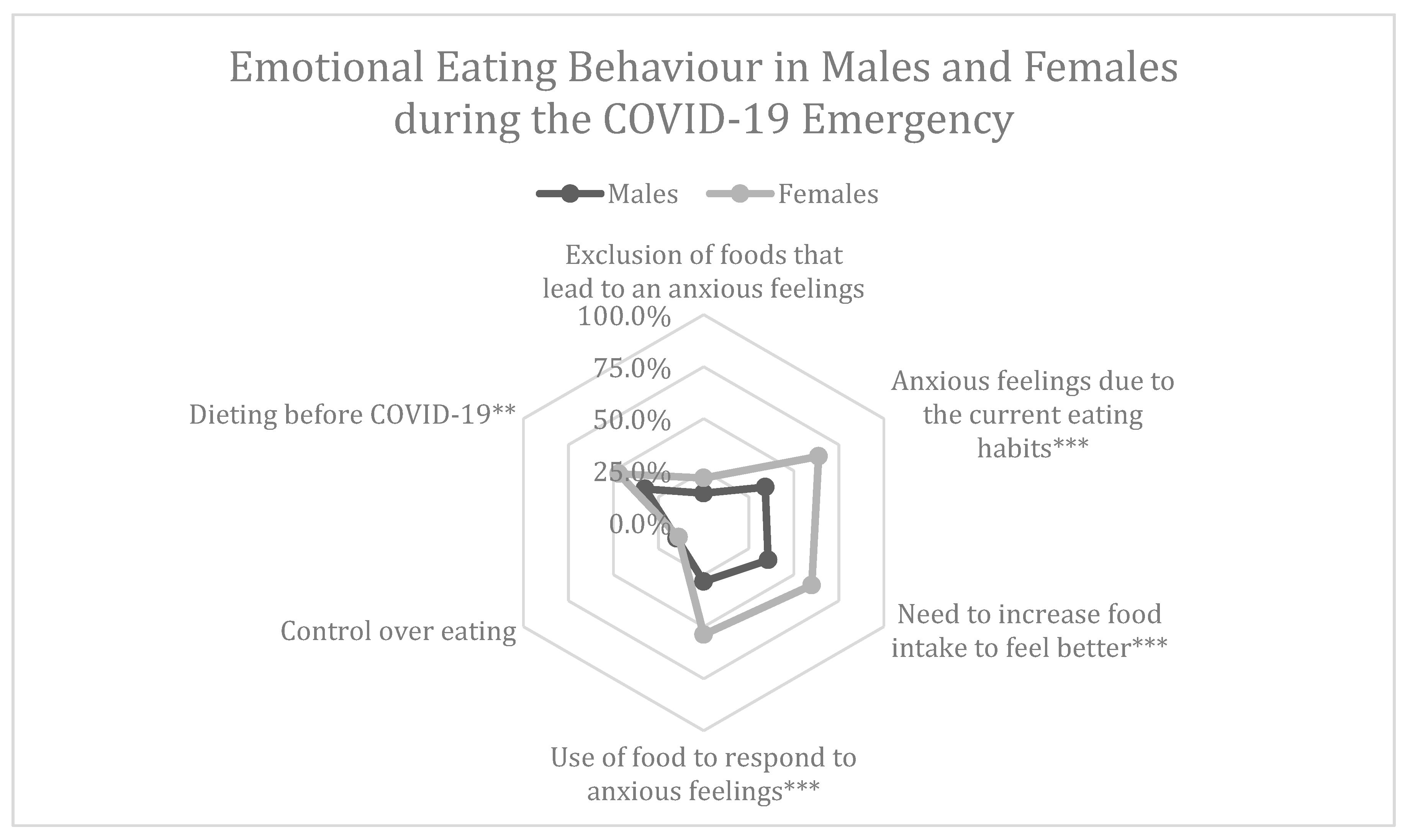
3.3. Emotional Eating Behaviour during the COVID-19 Emergency
3.4. Eating Control and Emotional State
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Answers | |
| Personal Data | 1. Age | Age in number |
| 2. Gender | Female/Male/NS | |
| 3. Place of residence | Region | |
| 4. Hometown | Province | |
| 5. Educational level | Elementary school diploma/Superior school diploma/Master Degree Post degree diploma | |
| 6. Who do you live with? | Alone/With roommates/With friends/With cohabitant/With parents With children/With spouse/cohabitant and children | |
| Anthropometrics Data | 7. Weight | Weight in kg |
| 8. Height | Height in cm | |
| Emotional state, eating habits and emotional eating behaviors | 9. In this social isolation period, is your mood depressed? | Yes/No |
| 10. In this social isolation period are you focused on your work? | Yes/No/At the moment I am not working due to the pandemia | |
| 11. In this social isolation period, are you experiencing anxious feelings? | Yes/No | |
| 12. In this social isolation period, are you feeling “hypochondriac” (afraid of getting sick)? | Yes/No | |
| 13. In this social isolation period, are you experiencing manifestations of anxiety (i.e., headache, sweating)? | Yes/No | |
| 14. In this social isolation period, are you experiencing manifestations of tension, fatigability, on alert, ready to cry, trembling, restless, unable to relax? | Yes/No | |
| 15. In this social isolation period are you experiencing breathing difficulties, choking sensation, chest pressure, dyspnea? | Yes/No | |
| 16. In this social isolation period are you experiencing tachycardia, palpitations, chest pain, feelings of fainting? | Yes/No | |
| 17. In this social isolation period are you taking any supplements (i.e., valerian, passionflower) and/or medications (i.e., benzodiazepines) to treat your manifestations of anxiety? | Yes/No | |
| 18. Have you been diagnosed with medical conditions? | Yes/No | |
| 19. In this social isolation period, are you experiencing insomnia? | Yes/No | |
| 20. In this social isolation period, when you experience manifestations of anxiety, do you comfort yourself with foods? | Yes/No | |
| 21. In this social isolation period, when you experience manifestations of anxiety did you avoid any food? | Yes/No | |
| 22. Before this social isolation period, were you on a diet? | Yes/No | |
| 23. In this social isolation period, do you continue to follow your diet? | Yes/No | |
| 24. In this social isolation period, are you feeling guilty for your eating habits? | Yes/No | |
| 25. In this isolation period, are you eating more to get feeling better, to reduce negative emotions or to increase pleasant feelings? | Yes/No |
Appendix B

References
- Lima, C.K.T.; Carvalho, P.M.D.M.; Lima, I.D.A.A.S.; Nunes, J.V.A.D.O.; Saraiva, J.S.; De Souza, R.I.; Da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Psychiatry Advisor. Mental Health Concerns Aris Amid COVID-19 Epidemic. Available online: https://www.psychiatryadvisor.com/home/topics/general-psychiatry/mental-health-concerns-arise-amid-COVID-19-epidemic (accessed on 4 June 2020).
- Hall, R.C.; Hall, R.C.; Chapman, M.J. The 1995 Kikwit Ebola outbreak: Lessons hospitals and physicians can apply to future viral epidemics. Gen. Hosp. Psychiatry 2008, 30, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, 20. [Google Scholar] [CrossRef]
- Schaller, M. The behavioural immune system and the psychology of human sociality. Philos. Trans. R. Soc. Biol. Sci. 2011, 366, 3418–3426. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Rubin, G.J.; Wessely, S. The psychological effects of quarantining a city. BMJ 2020, 368, 313. [Google Scholar] [CrossRef] [Green Version]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The Psychological Impact of the SARS Epidemic on Hospital Employees in China: Exposure, Risk Perception, and Altruistic Acceptance of Risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 1–15. [Google Scholar] [CrossRef]
- Digital 2020 Global Digital Overview. Available online: https://datareportal.com/reports/digital-2020-global-digital-overview (accessed on 6 June 2020).
- Hamilton, M. The Assessment of Anxiety States by Rating. Br. J. Med Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Thompson, E. Hamilton Rating Scale for Anxiety (HAM-A). Occup. Med. 2015, 65, 601. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef] [Green Version]
- Manzoni, G.M.; Rossi, A.; Pietrabissa, G.; Varallo, G.; Molinari, E.; Poggiogalle, E.; Donini, L.M.; Tarrini, G.; Melchionda, N.; Piccione, C.; et al. Validation of the Italian Yale Food Addiction Scale in postgraduate university students. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 167–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Google Privacy and Terms. Available online: https://policies.google.com/privacy?hl=en (accessed on 12 June 2020).
- Istat. Multiscope on Families: Aspect of Everyday Life—General Part. Available online: https://www.istat.it/it/archivio/91926 (accessed on 10 June 2020).
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Scarmozzino, F.; Visioli, F. COVID-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Inchausti, F.; Macbeth, A.; Hasson-Ohayon, I.; DiMaggio, G. Psychological Intervention and COVID-19: What We Know So Far and What We Can Do. J. Contemp. Psychother. 2020. [Google Scholar] [CrossRef]
- Van Strien, T.; Konttinen, H.M.; Homberg, J.; Engels, R.C.M.E.; Winkens, L.H. Emotional eating as a mediator between depression and weight gain. Appetite 2016, 100, 216–224. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Adhikari, A.; Lee, S.Y.; Marshel, J.H.; Kim, C.; Mallory, C.; Lo, M.; Pak, S.; Mattis, J.; Lim, B.K.; et al. Diverging neural pathways assemble a behavioural state from separable features in anxiety. Nature 2013, 496, 219–223. [Google Scholar] [CrossRef]
- Akiskal, K.K.; Akiskal, H.S. The theoretical underpinnings of affective temperaments: Implications for evolutionary foundations of bipolar disorder and human nature. J. Affect. Disord. 2005, 85, 231–239. [Google Scholar] [CrossRef]
- Litwin, R.; Goldbacher, E.; Cardaciotto, L.; Gambrel, L.E. Negative emotions and emotional eating: The mediating role of experiential avoidance. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2016, 22, 97–104. [Google Scholar] [CrossRef]
- Konttinen, H.M.; Männistö, S.; Sarlio-Lähteenkorva, S.; Silventoinen, K.; Haukkala, A. Emotional eating, depressive symptoms and self-reported food consumption. A population-based study. Appetite 2010, 54, 473–479. [Google Scholar] [CrossRef]
- Ruiz-Roso, M.B.; Padilha, P.D.C.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Peres, W.A.F.; Martorell, M.; Aires, M.T.; Cardoso, L.D.O.; et al. COVID-19 Confinement and Changes of Adolescent’s Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef]
- Halbreich, U.; Kahn, L.S. Atypical depression, somatic depression and anxious depression in women: Are they gender-preferred phenotypes? J. Affect. Disord. 2007, 102, 245–258. [Google Scholar] [CrossRef]
- Off-Label Use of Medicines for COVID-19. WHO. 2020. Available online: https://www.who.int/news-room/commentaries/detail/off-label-use-of-medicines-for-covid-19 (accessed on 12 June 2020).
- Butler, M.J.; Barrientos, R.M. The impact of nutrition on COVID-19 susceptibility and long-term consequences. Brain Behav. Immun. 2020, 87, 53–54. [Google Scholar] [CrossRef]
- Iddir, M.; Brito, A.; Dingeo, G.; Del Campo, S.S.F.; Samouda, H.; La Frano, M.R.; Bohn, T. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during the COVID-19 Crisis. Nutrients 2020, 12, 1562. [Google Scholar] [CrossRef]
- Carter, J.C.; Van Wijk, M.; Rowsell, M. Symptoms of ‘food addiction’ in binge eating disorder using the Yale Food Addiction Scale version 2.0. Appetite 2019, 133, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, P.C.; Kenny, P.J. Food addiction: A valid concept? Neuropsychopharmacology 2018, 43, 2506–2513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parylak, S.L.; Koob, G.F.; Zorrilla, E.P. The dark side of food addiction. Physiol. Behav. 2011, 104, 149–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corwin, R.; Grigson, P.S. Symposium overview—Food addiction: Fact or fiction? J. Nutr. 2009, 139, 617–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Ministry. Available online: http://www.salute.gov.it/imgs/C_17_notizie_4776_0_file.pdf (accessed on 10 June 2020).




| Whole Sample (n = 602) | Northern Italy (n = 94) | Centre Italy (n = 241) | Southern Italy and Islands (n = 267) | |
|---|---|---|---|---|
| Age | 36.0 [20.0] | 36.0 [18.0] | 33.0 [23.0] | 38.0 [17.0] |
| 38.2 ± 12.9 | 38.1 ± 12.5 | 37.3 ± 14.1 | 39.1 ± 11.9 | |
| Age Groups | ||||
| 18–30 years | 212 (35.2%) | 33 (35.1%) | 107 (44.4%) | 72 (27.0%) |
| 31–50 years | 279 (46.3%) | 45 (47.9%) | 86 (35.7%) | 148 (55.4%) |
| 51–65 years | 91 (15.1%) | 13 (13.8%) | 37 (15.4%) | 41 (15.4%) |
| >66 years | 20 (3.3%) | 3 (3.2%) | 11 (4.6%) | 6 (2.2%) |
| Gender | ||||
| Female | 480 (79.7%) | 82 (87.2%) | 182 (75.5%) | 216 (80.9%) |
| Male | 120 (19.9%) | 12 (12.8%) | 58 (24.1%) | 50 (18.5%) |
| Not specified | 2 (0.3%) | 0.0 (0%) | 1 (0.4%) | 1 (0.4%) |
| Educational Level | ||||
| Compulsory school | 44 (7.3%) | 9 (9.6%) | 11 (4.6%) | 24 (9.0%) |
| High school degree | 215 (35.7%) | 23 (24.5%) | 76 (31.5%) | 116 (43.4%) |
| Graduate school degree | 243 (40.4%) | 41 (43.6%) | 107 (44.4%) | 95 (35.6%) |
| Post-graduate school degree | 100 (16.6%) | 21 (22.3%) | 47 (19.5%) | 32 (12.0%) |
| Weight (kg) | 66.0 [21.0] | 64.5 [16.3] | 66.0 [22.0] | 67.0 [21.0] |
| 69.6 ± 16.4 | 67.6 ± 16.8 | 70.3 ± 16.6 | 69.6 ± 16.2 | |
| Height (cm) | 165.0 [11.3] | 165.5 [9.5] | 165.0 [13.0] | 165.0 [10.0] |
| 166.4 ± 8.6 | 166.5 ± 7.6 | 167.2 ± 8.5 | 165.8 ± 8.9 | |
| BMI (kg/m2) | 24.0 [6.4] | 23.1 [5.6] | 24.0 [6.3] | 24.6 [6.7] |
| 25.0 ± 5.2 | 24.3 ± 5.6 | 25.1 ± 5.3 | 25.2 ± 4.9 | |
| Class of BMI | ||||
| Underweight | 13 (2.2%) | 2 (2.1%) | 7 (2.9%) | 4 (1.5%) |
| Normal weight | 344 (57.1%) | 62 (66.0%) | 137 (56.8%) | 145 (54.3%) |
| Overweight | 161 (26.7%) | 20 (21.3%) | 64 (26.6%) | 77 (28.8%) |
| Obesity I | 61 (10.1%) | 7 (7.4%) | 23 (9.5%) | 31 (11.6%) |
| Obesity II | 13 (2.2%) | 1 (1.1%) | 5 (2.1%) | 7 (2.6%) |
| Obesity III | 10 (1.7%) | 2 (2.1%) | 5 (2.1%) | 3 (1.1%) |
| Dependent Variable | Independent Variables | Coefficient (B) | 95% CI | p | OR | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Control over-eating | Age | −0.034 | 0.945 | 0.989 | 0.004 | 0.967 |
| BMI | −0.113 | 0.833 | 0.958 | 0.002 | 0.893 | |
| Dieting before COVID-19 | 0.830 | 1.375 | 3.822 | 0.001 | 2.293 | |
| Depressed mood | −0.549 | 0.314 | 1.062 | 0.077 | 0.577 | |
| Anxious feelings | −0.820 | 0.239 | 0.812 | 0.009 | 0.440 | |
| Need to increase food intake to feel better | −1.036 | 0.206 | 0.611 | <0.001 | 0.355 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, 2152. https://doi.org/10.3390/nu12072152
Di Renzo L, Gualtieri P, Cinelli G, Bigioni G, Soldati L, Attinà A, Bianco FF, Caparello G, Camodeca V, Carrano E, et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients. 2020; 12(7):2152. https://doi.org/10.3390/nu12072152
Chicago/Turabian StyleDi Renzo, Laura, Paola Gualtieri, Giulia Cinelli, Giulia Bigioni, Laura Soldati, Alda Attinà, Francesca Fabiola Bianco, Giovanna Caparello, Vanessa Camodeca, Elena Carrano, and et al. 2020. "Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey" Nutrients 12, no. 7: 2152. https://doi.org/10.3390/nu12072152
APA StyleDi Renzo, L., Gualtieri, P., Cinelli, G., Bigioni, G., Soldati, L., Attinà, A., Bianco, F. F., Caparello, G., Camodeca, V., Carrano, E., Ferraro, S., Giannattasio, S., Leggeri, C., Rampello, T., Lo Presti, L., Tarsitano, M. G., & De Lorenzo, A. (2020). Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients, 12(7), 2152. https://doi.org/10.3390/nu12072152