The Impact of Whole Grain Intake on Gastrointestinal Tumors: A Focus on Colorectal, Gastric, and Esophageal Cancers


Abstract
:1. Introduction
2. Whole Grains: An Overview
2.1. Definition
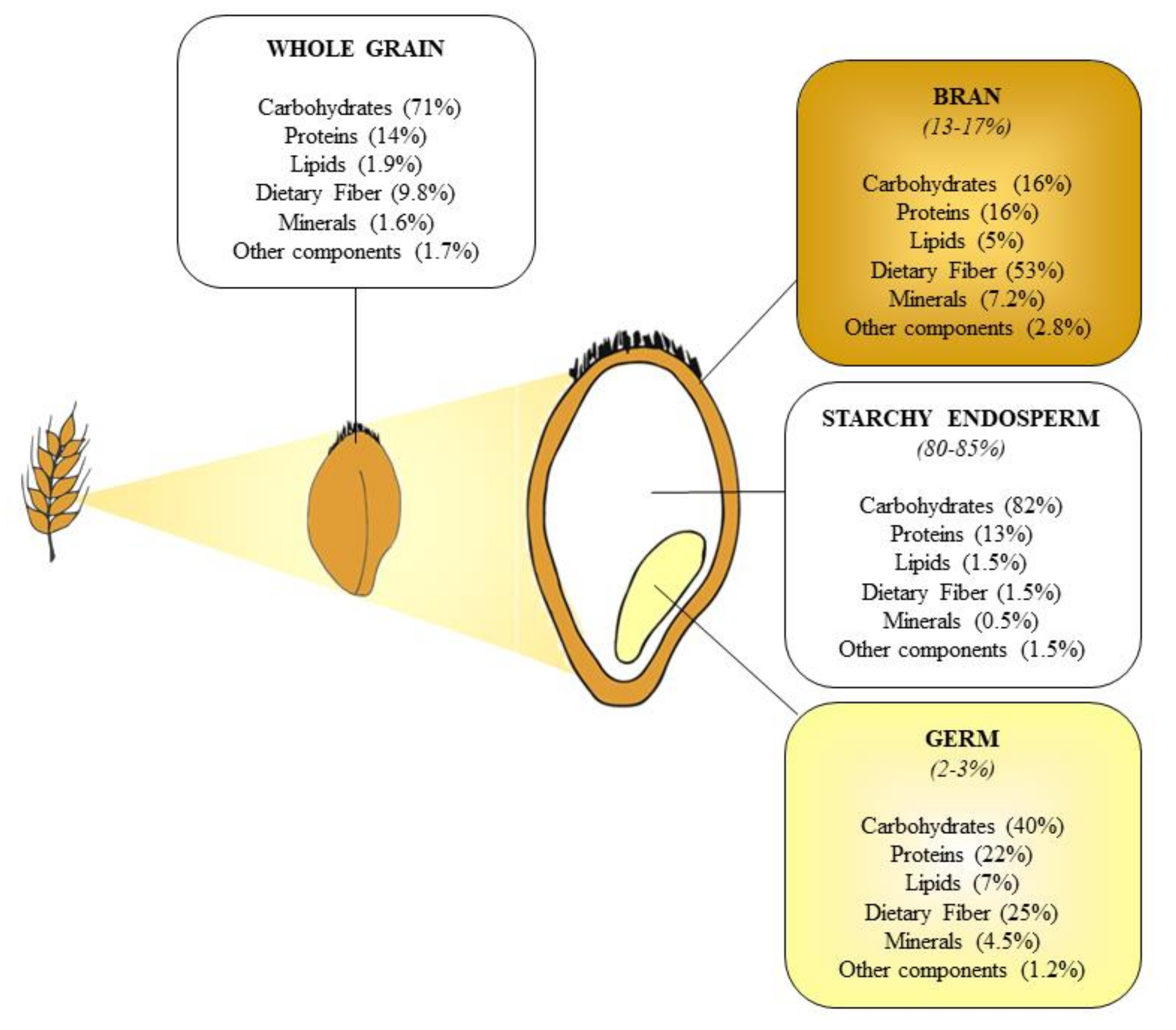
2.2. Chemical Composition of Cereal Kernels
2.3. Whole Grains and Health
3. Dietary Fiber and Polyphenols as Functional Compounds in Whole Grains
4. Whole Grains and Gastrointestinal Cancers: An Overview
5. Whole Grains and Colorectal Cancer
6. Whole Grains and Gastric Cancer
7. Whole Grains in Esophageal Cancer
8. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Ross, A.B.; van der Kamp, J.W.; King, R.; Lê, K.A.; Mejborn, H.; Seal, C.J.; Thielecke, F. Perspective: A definition for whole-grain food products—Recommendations from the Healthgrain Forum. Adv. Nutr. 2017, 8, 525–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferruzzi, M.G.; Jonnalagadda, S.S.; Liu, S.; Marquart, L.; McKeown, N.; Reicks, M.; Riccardi, G.; Seal, C.; Slavin, J.; Thielecke, F.; et al. Developing a Standard Definition of Whole-Grain Foods for Dietary Recommendations: Summary Report of a Multidisciplinary Expert Roundtable Discussion. Adv. Nutr. 2014, 5, 164–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carcea, M. Nutritional Value of Grain-Based Foods. Foods 2020, 9, 504. [Google Scholar] [CrossRef] [PubMed]
- Nugent, A.P.; Thielecke, F. Wholegrains and health: Many benefits but do contaminants pose any risk? Nutr. Bull. 2019, 44, 107–115. [Google Scholar] [CrossRef]
- Cummings, J.H.; Engineer, A. Nutr. Res. Rev. 2018, 31, 1–15. [CrossRef] [PubMed] [Green Version]
- Huang, T.; Xu, M.; Lee, A.; Cho, S.; Qi, L. Consumption of whole grains and cereal fiber and total and cause-specific mortality: Prospective analysis of 367,442 individuals. BMC Med. 2015, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [Green Version]
- Mellen, P.B.; Walsh, T.F.; Herrington, D.M. Whole grain intake and cardiovascular disease: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 283–290. [Google Scholar] [CrossRef]
- Larsson, S.C.; Giovannucci, E.; Bergkvist, L.; Wolk, A. Whole grain consumption and risk of colorectal cancer: A population-based cohort of 60,000 women. Br. J. Cancer 2005, 92, 1803–1807. [Google Scholar] [CrossRef]
- Wu, H.; Flint, A.J.; Qi, Q.; Van Dam, R.M.; Sampson, L.A.; Rimm, E.B.; Holmes, M.D.; Willett, W.C.; Hu, F.B.; Sun, Q. Association between dietary whole grain intake and risk of mortality: Two large prospective studies in US Men and Women. JAMA Intern. Med. 2015, 175, 373–384. [Google Scholar] [CrossRef]
- Zong, G.; Gao, A.; Hu, F.B.; Sun, Q. Whole grain intake and mortality from all causes, cardiovascular disease, and cancer. Circulation 2016, 133, 2370–2380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacco, R.; Costabile, G.; Fatati, G.; Frittitta, L.; Maiorino, M.I.; Marelli, G.; Parillo, M.; Pistis, D.; Tubili, C.; Vetrani, C.; et al. Effects of polyphenols on cardio-metabolic risk factors and risk of type 2 diabetes. A joint position statement of the Diabetes and Nutrition Study Group of the Italian Society of Diabetology (SID), the Italian Association of Dietetics and Clinical Nutrit. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Polito, R.; Costabile, G.; Nigro, E.; Giacco, R.; Vetrani, C.; Anniballi, G.; Luongo, D.; Riccardi, G.; Daniele, A.; Annuzzi, G. Nutritional factors influencing plasma adiponectin levels: Results from a randomised controlled study with whole-grain cereals. Int. J. Food Sci. Nutr. 2020, 71, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Vetrani, C.; Costabile, G.; Luongo, D.; Naviglio, D.; Rivellese, A.A.; Riccardi, G.; Giacco, R. Effects of whole-grain cereal foods on plasma short chain fatty acid concentrations in individuals with the metabolic syndrome. Nutrition 2016, 32, 217–221. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. US Department of Agriculture 2015–2020 Dietary Guidelines for Americans, 8th ed. Available online: https://health.gov/sites/default/files/2019-09/2015-2020_Dietary_Guidelines.pdf (accessed on 26 November 2020).
- ALTOMKOST. Danish Veterinary and Food Administration The Official Dietary Guidelines. Available online: https://altomkost.dk/raad-og-anbefalinger/de-officielle-kostraad/ (accessed on 26 November 2020).
- Helsedirektoratet. Norwegian Directorate of Health Recommendations about Diet, Nutrition and Physical Activity. Available online: https://www.helsedirektoratet.no/brosjyrer/helsedirektoratets-kostrad-brosjyre-og-plakat/Helsedirektoratets%20kostr%C3%A5d%20-%20engelsk.pdf/_/attachment/inline/80f68126-68af-4cec-b2aa-d04069d02471:dcb8efdbe6b6129470ec4969f6639be21a8afd82/Helsedirektoratets%20kostr%C3%A5d%20-%20engelsk.pdf (accessed on 26 November 2020).
- Sweden Countries Swedish Food Agency Find Your Way to Eat Greener, not too much and Be Active. Available online: https://www.livsmedelsverket.se/globalassets/publikationsdatabas/rapporter/2015/rapp-hanteringsrapport-engelska-omslag--inlaga--bilagor-eng-version.pdf (accessed on 26 November 2020).
- Division of Nutrition National Food Institute Technical University of Denmark. Wholegrain Intake of Danes 2011–2012. Available online: https://www.food.dtu.dk/english/-/media/Institutter/Foedevareinstituttet/Publikationer/Pub-2013/Rapport_Fuldkornsindtag_11-12_UK.ashx?la=da&hash=8B2A20C3ED33A0B8564E5403DFD8225CB25EE42D (accessed on 27 November 2020).
- Albertson, A.M.; Reicks, M.; Joshi, N.; Gugger, C.K. Whole grain consumption trends and associations with body weight measures in the United States: Results from the cross sectional National Health and Nutrition Examination Survey 2001–2012. Nutr. J. 2016, 15, 8. [Google Scholar] [CrossRef] [Green Version]
- O’Donovan, C.B.; Devlin, N.F.; Buffini, M.; Walton, J.; Flynn, A.; Gibney, M.J.; Nugent, A.P.; McNulty, B.A. Whole grain intakes in Irish adults: Findings from the National Adults Nutrition Survey (NANS). Eur. J. Nutr. 2019, 58, 541–550. [Google Scholar] [CrossRef] [Green Version]
- Devlin, N.F.C.; McNulty, B.A.; Gibney, M.J.; Thielecke, F.; Smith, H.; Nugent, A.P. Whole grain intakes in the diets of Irish children and teenagers. Br. J. Nutr. 2013, 110, 354–362. [Google Scholar] [CrossRef] [Green Version]
- Galea, L.M.; Beck, E.J.; Probst, Y.C.; Cashman, C.J. Whole grain intake of Australians estimated from a cross-sectional analysis of dietary intake data from the 2011–13 Australian Health Survey. Public Health Nutr. 2017, 20, 2166–2172. [Google Scholar] [CrossRef] [Green Version]
- Mann, K.D.; Pearce, M.S.; McKevith, B.; Thielecke, F.; Seal, C.J. Low whole grain intake in the UK: Results from the National Diet and Nutrition Survey rolling programme 2008–11. Br. J. Nutr. 2015, 113, 1643–1651. [Google Scholar] [CrossRef] [Green Version]
- Bellisle, F.; Hébel, P.; Colin, J.; Reyé, B.; Hopkins, S. Consumption of whole grains in French children, adolescents and adults. Br. J. Nutr. 2014, 112, 1674–1684. [Google Scholar] [CrossRef] [Green Version]
- Sette, S.; D’Addezio, L.; Piccinelli, R.; Hopkins, S.; Le Donne, C.; Ferrari, M.; Mistura, L.; Turrini, A. Intakes of whole grain in an Italian sample of children, adolescents and adults. Eur. J. Nutr. 2017, 56, 521–533. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, E.; Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; Persichillo, M.; Bracone, F.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; et al. Consumption of whole grain food and its determinants in a general Italian population: Results from the INHES study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Watson, R.R.; Preedy, V.; Zibadi, S. Wheat and Rice in Disease Prevention and Health; Elsevier Inc.: Amsterdam, The Netherlands, 2014; ISBN 9780124017160. [Google Scholar] [CrossRef]
- van der Kamp, J.W.; Poutanen, K.; Seal, C.J.; Richardson, D.P. The Healthgrain definition of ‘whole grain’. Food Nutr. Res. 2014, 58, 22100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathews, R.; Chu, Y.F. Global review of whole grain definitions and health claims. Nutr. Rev. 2020, 78, 98–106. [Google Scholar] [CrossRef]
- Khan, K.; Shrewry, P.R. Wheat: Chemistry and Technology, 4th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2009; ISBN 9780128104545. [Google Scholar]
- Carcea, M.; Turfani, V.; Narducci, V.; Melloni, S.; Galli, V.; Tullio, V. Stone Milling versus Roller Milling in Soft Wheat: Influence on Products Composition. Foods 2019, 9, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apprich, S.; Tirpanalan, Ö.; Hell, J.; Reisinger, M.; Böhmdorfer, S.; Siebenhandl-Ehn, S.; Novalin, S.; Kneifel, W. Wheat bran-based biorefinery 2: Valorization of products. LWT Food Sci. Technol. 2014, 56, 222–231. [Google Scholar] [CrossRef]
- Onipe, O.O.; Jideani, A.I.O.; Beswa, D. Composition and functionality of wheat bran and its application in some cereal food products. Int. J. Food Sci. Technol. 2015, 50, 2509–2518. [Google Scholar] [CrossRef]
- Oghbaei, M.; Prakash, J. Effect of primary processing of cereals and legumes on its nutritional quality: A comprehensive review. Cogent Food Agric. 2016, 2, 1136015. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.L.; Dodd, K.W.; Gahche, J.J.; Dwyer, J.T.; McDowell, M.A.; Yetley, E.A.; Sempos, C.A.; Burt, V.L.; Radimer, K.L.; Picciano, M.F. Total folate and folic acid intake from foods and dietary supplements in the United States: 2003–2006. Am. J. Clin. Nutr. 2010, 91, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, M.; Jensen, M.G.; Riboldi, G.; Petronio, M.; Bügel, S.; Toubro, S.; Tetens, I.; Astrup, A. Wholegrain vs. refined wheat bread and pasta. Effect on postprandial glycemia, appetite, and subsequent ad libitum energy intake in young healthy adults. Appetite 2010, 54, 163–169. [Google Scholar] [CrossRef]
- Cioffi, I.; Ibrugger, S.; Bache, J.; Thomassen, M.T.; Contaldo, F.; Pasanisi, F.; Kristensen, M. Effects on satiation, satiety and food intake of wholegrain and refined grain pasta. Appetite 2016, 107, 152–158. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, M.; Piccolo, M.; Vannini, L.; Siragusa, S.; de Giacomo, A.; Serrazzanetti, D.I.; Cristofori, F.; Guerzoni, M.E.; Gobbetti, M.; Francavilla, R. Fecal Microbiota and Metabolome of Children with Autism and Pervasive Developmental Disorder Not Otherwise Specified. PLoS ONE 2013, 8, e76993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G.D.; Chen, J.; Hoffmann, C.; Bittinger, K.; Chen, Y.-Y.; Keilbaugh, S.A.; Bewtra, M.; Knights, D.; Walters, W.A.; Knight, R.; et al. Linking Long-Term Dietary Patterns with. Science 2011, 334, 105–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuohy, K.M.; Conterno, L.; Gasperotti, M.; Viola, R. Up-regulating the human intestinal microbiome using whole plant foods, polyphenols, and/or fiber. J. Agric. Food Chem. 2012, 60, 8776–8782. [Google Scholar] [CrossRef]
- Claesson, M.J.; Jeffery, I.B.; Conde, S.; Power, S.E.; O’connor, E.M.; Cusack, S.; Harris, H.M.B.; Coakley, M.; Lakshminarayanan, B.; O’sullivan, O.; et al. Gut microbiota composition correlates with diet and health in the elderly. Nature 2012, 488, 178–184. [Google Scholar] [CrossRef] [PubMed]
- De Filippis, F.; Pellegrini, N.; Vannini, L.; Jeffery, I.B.; La Storia, A.; Laghi, L.; Serrazanetti, I.D.; Di Cagno, R.; Ferrocino, I.; Lazzi, C.; et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut 2016, 65, 1812–1821. [Google Scholar] [CrossRef]
- D’Alessandro, A.; Lampignano, L.; De Pergola, G. Mediterranean Diet Pyramid: A Proposal for Italian People. A Systematic Review of Prospective Studies to Derive Serving Sizes. Nutrients 2019, 11, 1296. [Google Scholar] [CrossRef] [Green Version]
- Vitiello, V.; Germani, A.; Capuzzo Dolcetta, E.; Donini, L.M.; del Balzo, V. The new modern mediterranean diet italian pyramid. Ann. Ig 2016, 28, 179–186. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Vanegas, S.M.; Meydani, M.; Barnett, J.B.; Goldin, B.; Kane, A.; Rasmussen, H.; Brown, C.; Vangay, P.; Knights, D.; Jonnalagadda, S.; et al. Substituting whole grains for refined grains in a 6-wk randomized trial has a modest effect on gut microbiota and immune and inflammatory markers of healthy adults. Am. J. Clin. Nutr. 2017, 105, 635–650. [Google Scholar] [CrossRef] [Green Version]
- Saura-Calixto, F. Dietary fiber as a carrier of dietary antioxidants: An essential physiological function. J. Agric. Food Chem. 2011, 59, 43–49. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Salvatori, T.; Dallagiacoma, G.; Fatigoni, C.; Moretti, M.; Realdon, S. Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1579. [Google Scholar] [CrossRef] [Green Version]
- AACC. The definition of dietary fiber. In Cereal Foods World; AACC (the American Association of Cereal Chemists): Eagan, MN, USA, 2001; Volume 46, pp. 112–129. [Google Scholar]
- Jones, J.M. Dietary fiber methods in Codex Alimentarius: Current status and ongoing discussions. Cereal Foods World 2013, 58, 148–152. [Google Scholar] [CrossRef] [Green Version]
- Caprita, R.; Caprita, A.; Cretescu, I. Effect of extraction conditions on the solubility of non-starch polysaccharides of wheat and barley. J. Food Agric. Environ. 2011, 9, 41–43. [Google Scholar]
- Ain, H.B.U.; Saeed, F.; Ahmad, N.; Imran, A.; Niaz, B.; Afzaal, M.; Imran, M.; Tufail, T.; Javed, A. Functional and health-endorsing properties of wheat and barley cell wall’s non-starch polysaccharides. Int. J. Food Prop. 2018, 21, 1463–1480. [Google Scholar] [CrossRef] [Green Version]
- Chotinsky, D. The use of enzymes to improve utilization of nutrient in poultry diets. Bulg. J. Agric. Sci. 2015, 21, 429–435. [Google Scholar]
- Terry, P.; Lagergren, J.; Ye, W.; Wolk, A.; Nyrén, O. Inverse association between intake of cereal fiber and risk of gastric cardia cancer. Gastroenterology 2001, 120, 387–391. [Google Scholar] [CrossRef]
- Mirmiran, P.; Bahadoran, Z.; Moghadam, S.K.; Vakili, A.Z.; Azizi, F. A prospective study of different types of dietary fiber and risk of cardiovascular disease: Tehran lipid and glucose study. Nutrients 2016, 8, 686. [Google Scholar] [CrossRef] [Green Version]
- CREA Tabelle di composizione degli alimenti. Available online: https://www.crea.gov.it/en/-/tabella-di-composizione-degli-alimenti (accessed on 12 November 2020).
- USDA National Nutrient Database. Available online: https://data.nal.usda.gov/dataset/composition-foods-raw-processed-prepared-usda-national-nutrient-database-standard-reference-release-27 (accessed on 7 November 2020).
- Carcea, M.; Narducci, V.; Turfani, V.; Giannini, V. Polyphenols in Raw and Cooked Cereals/Pseudocereals/Legume Pasta and Couscous. Foods 2017, 6, 80. [Google Scholar] [CrossRef] [Green Version]
- Dykes, L.; Rooney, L.W. Phenolic Compounds in Cereal Grains and Their Health Benefits. Cereal Foods World 2007, 52, 105–111. [Google Scholar] [CrossRef]
- Adom, K.K.; Liu, R.H. Antioxidant Activity of Grains. J. Agric. Food Chem. 2002, 50, 6182–6187. [Google Scholar] [CrossRef] [PubMed]
- Oliver Chen, C.; Costa, S.M.; Carolo, K. Phenolic Acids. In Whole Grains and Their Bioactives; Wiley Online Library: Hoboken, NJ, USA, 2019; pp. 357–382. [Google Scholar]
- Liu, Z.; Liu, Y.; Pu, Z.; Wang, J.; Zheng, Y.; Li, Y.; Wei, Y. Regulation, evolution, and functionality of flavonoids in cereal crops. Biotechnol. Lett. 2013, 35, 1765–1780. [Google Scholar] [CrossRef]
- Quirós-Sauceda, A.E.; Palafox-Carlos, H.; Sáyago-Ayerdi, S.G.; Ayala-Zavala, J.F.; Bello-Perez, L.A.; Álvarez-Parrilla, E.; De La Rosa, L.A.; González-Córdova, A.F.; González-Aguilar, G.A. Dietary fiber and phenolic compounds as functional ingredients: Interaction and possible effect after ingestion. Food Funct. 2014, 5, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, J.S.; Kabir, Y.; Huffman, F.G. Functional foods from cereal grains. Int. J. Food Prop. 2007, 10, 231–244. [Google Scholar] [CrossRef]
- Kaur, P.; Purewal, S.S.; Sandhu, K.S.; Kaur, M.; Salar, R.K. Millets: A cereal grain with potent antioxidants and health benefits. J. Food Meas. Charact. 2019, 13, 793–806. [Google Scholar] [CrossRef]
- Parada, J.; Aguilera, J.M. Food Microstructure Affects the Bioavailability of Several Nutrients. J. Food Sci. 2007, 72, R21–R32. [Google Scholar] [CrossRef]
- Okarter, N.; Liu, C.S.; Sorrells, M.E.; Liu, R.H. Phytochemical content and antioxidant activity of six diverse varieties of whole wheat. Food Chem. 2010, 119, 249–257. [Google Scholar] [CrossRef]
- Xu, Z.; Godber, J.S. Purification and identification of components of γ-oryzanol in rice bran oil. J. Agric. Food Chem. 1999. [Google Scholar] [CrossRef]
- Collins, F.W. Oat Phenolics: Avenanthramides, Novel Substituted N-Cinnamoylanthranilate Alkaloids from Oat Groats and Hulls. J. Agric. Food Chem. 1989. [Google Scholar] [CrossRef]
- McCarty, M.F.; Assanga, S.B.I. Ferulic acid may target MyD88-mediated pro-inflammatory signaling—Implications for the health protection afforded by whole grains, anthocyanins, and coffee. Med. Hypotheses 2018, 118, 114–120. [Google Scholar] [CrossRef]
- Abdel-Aal, E.-S.M.; Young, J.C.; Rabalski, I. Anthocyanin Composition in Black, Blue, Pink, Purple, and Red Cereal Grains. J. Agric. Food Chem. 2006, 54, 4696–4704. [Google Scholar] [CrossRef] [PubMed]
- Durazzo, A.; Zaccaria, M.; Polito, A.; Maiani, G.; Carcea, M. Lignan Content in Cereals, Buckwheat and Derived Foods. Foods 2013, 2, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Cai, C.; Wang, Y.; Zheng, X. The inactivation kinetics of polyphenol oxidase and peroxidase in bayberry juice during thermal and ultrasound treatments. Innov. Food Sci. Emerg. Technol. 2018, 45, 169–178. [Google Scholar] [CrossRef]
- Zhang, H.; Tsao, R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Curr. Opin. Food Sci. 2016, 8, 33–42. [Google Scholar] [CrossRef]
- Gani, A.; Wani, S.M.; Masoodi, F.A.; Hameed, G. Whole-Grain Cereal Bioactive Compounds and Their Health Benefits: A Review. J. Food Process. Technol. 2012, 3, 146–156. [Google Scholar] [CrossRef] [Green Version]
- Vitaglione, P.; Napolitano, A.; Fogliano, V. Cereal dietary fibre: A natural functional ingredient to deliver phenolic compounds into the gut. Trends Food Sci. Technol. 2008, 19, 451–463. [Google Scholar] [CrossRef]
- Ribas-Agustí, A.; Seda, M.; Sarraga, C.; Montero, J.I.; Castellari, M.; Muñoz, P. Municipal solid waste composting: Application as a tomato fertilizer and its effect on crop yield, fruit quality and phenolic content. Renew. Agric. Food Syst. 2017, 32, 358–365. [Google Scholar] [CrossRef]
- Vitaglione, P.; Mennella, I.; Ferracane, R.; Rivellese, A.A.; Giacco, R.; Ercolini, D.; Gibbons, S.M.; La Storia, A.; Gilbert, J.A.; Jonnalagadda, S.; et al. Whole-grain wheat consumption reduces inflammation in a randomized controlled trial on overweight and obese subjects with unhealthy dietary and lifestyle behaviors: Role of polyphenols bound to cereal dietary fiber. Am. J. Clin. Nutr. 2015, 101, 251–261. [Google Scholar] [CrossRef] [Green Version]
- González-Aguilar, G.A.; Blancas-Benítez, F.J.; Sáyago-Ayerdi, S.G. Polyphenols associated with dietary fibers in plant foods: Molecular interactions and bioaccessibility. Curr. Opin. Food Sci. 2017, 13, 84–88. [Google Scholar] [CrossRef]
- Bishehsari, F.; Engen, P.; Preite, N.; Tuncil, Y.; Naqib, A.; Shaikh, M.; Rossi, M.; Wilber, S.; Green, S.; Hamaker, B.; et al. Dietary Fiber Treatment Corrects the Composition of Gut Microbiota, Promotes SCFA Production, and Suppresses Colon Carcinogenesis. Genes 2018, 9, 102. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.; Chen, Y.; Jiang, H.; Nie, D. The role of short-chain fatty acids in orchestrating two types of programmed cell death in colon cancer. Autophagy 2011, 7, 235–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lizarraga, D.; Vinardell, M.P.; Noé, V.; van Delft, J.H.; Alcarraz-Vizán, G.; van Breda, S.G.; Staal, Y.; Günther, U.L.; Reed, M.A.; Ciudad, C.J.; et al. A Lyophilized red grape pomace containing proanthocyanidin-rich dietary fiber induces genetic and metabolic alterations in colon mucosa of female C57Bl/6J mice. J. Nutr. 2011, 141, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.B.F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France; Available online: https://gco.iarc.fr/today (accessed on 13 November 2020).
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Mereiter, S.; Balmaña, M.; Gomes, J.; Magalhães, A.; Reis, C.A. Glycomic approaches for the discovery of targets in gastrointestinal cancer. Front. Oncol. 2016, 6, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology 2020, 159, 335–349.e15. [Google Scholar] [CrossRef]
- Yang, W.; Ma, Y.; Liu, Y.; Smith-Warner, S.A.; Simon, T.G.; Chong, D.Q.; Qi, Q.; Meyerhardt, J.A.; Giovannucci, E.L.; Chan, A.T.; et al. Association of Intake of Whole Grains and Dietary Fiber with Risk of Hepatocellular Carcinoma in US Adults. JAMA Oncol. 2019, 5, 879–886. [Google Scholar] [CrossRef] [Green Version]
- Lei, Q.; Zheng, H.; Bi, J.; Wang, X.; Jiang, T.; Gao, X.; Tian, F.; Xu, M.; Wu, C.; Zhang, L.; et al. Whole Grain Intake Reduces Pancreatic Cancer Risk. Medicine 2016, 95, e2747. [Google Scholar] [CrossRef]
- Winn, D.M.; Ziegler, R.G.; Pickle, L.W.; Gridley, G.; Blot, W.J.; Hoover, R.N. Diet in the Etiology of Oral and Pharyngeal Cancer among Women from the Southern United States. Cancer Res. 1984, 44, 1216–1222. [Google Scholar]
- Levi, F.; Pasche, C.; Lucchini, F.; Chatenoud, L.; Jacobs, D.; La Vecchia, C. Refined and whole grain cereals and the risk of oral, oesophageal and laryngeal cancer. Eur. J. Clin. Nutr. 2000, 54, 487–489. [Google Scholar] [CrossRef] [Green Version]
- Chatenoud, L.; La Vecchia, C.; Franceschi, S.; Tavani, A.; Jacobs, D.R.; Parpinel, M.T.; Soler, M.; Negri, E. Refined-cereal intake and risk of selected cancers in Italy. Am. J. Clin. Nutr. 1999, 70, 1107–1110. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, S.; Favero, A.; Conti, E.; Talamini, R.; Volpe, R.; Negri, E.; Barzan, L.; Vecchia, C. La Food groups, oils and butter, and cancer of the oral cavity and pharynx. Br. J. Cancer 1999, 80, 614–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uzcudun, A.E.; Retolaza, I.R.; Fernández, P.B.; Sánchez Hernández, J.J.; Grande, A.G.; García, A.G.; Olivar, L.M.; de Diego Sastre, I.; Barón, M.G.; Bouzas, J.G. Nutrition and pharyngeal cancer: Results from a case-control study in Spain. Head Neck 2002, 24, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Kasum, C.M.; Jacobs, D.R.; Nicodemus, K.; Folsom, A.R. Dietary risk factors for upper aerodigestive tract cancers. Int. J. Cancer 2002, 99, 267–272. [Google Scholar] [CrossRef] [PubMed]
- De Stefani, E.; Ronco, A.; Mendilaharsu, M.; Deneo-Pellegrini, H. Diet and risk of cancer of the upper aerodigestive tract—II. Nutrients. Oral Oncol. 1999, 35, 22–26. [Google Scholar] [CrossRef]
- Toporcov, T.N.; Antunes, J.L.F.; Tavares, M.R. Fat food habitual intake and risk of oral cancer. Oral Oncol. 2004, 40, 925–931. [Google Scholar] [CrossRef]
- Zheng, T.; Boyle, P.; Willett, W.C.; Hu, H.; Dan, J.; Evstifeeva, T.V.; Niu, S.; MacMahon, B. A case-control study of oral cancer in Beijing, People’s Republic of China. Associations with nutrient intakes, foods and food groups. Eur. J. Cancer. Part B Oral Oncol. 1993, 29, 45–55. [Google Scholar] [CrossRef]
- Sánchez, M.J.; Martínez, C.; Nieto, A.; Castellsagué, X.; Quintana, M.J.; Bosch, F.X.; Muñoz, N.; Herrero, R.; Franceschi, S. Oral and oropharyngeal cancer in Spain: Influence of dietary patterns. Eur. J. Cancer Prev. 2003, 12, 49–56. [Google Scholar] [CrossRef]
- Franceschi, S.; Bidoli, E.; Barón, A.E.; Barra, S.; Talamini, R.; Serraino, D.; La Vecchia, C. Nutrition and cancer of the oral cavity and pharynx in north-east italy. Int. J. Cancer 1991, 47, 20–25. [Google Scholar] [CrossRef]
- Nandakumar, A.; Thimmasetty, K.T.; Sreeramareddy, N.M.; Venugopal, T.C.; Rajanna; Vinutha, A.T.; Srinivas; Bhargava, M.K. A population-based case-control investigation on cancers of the oral cavity in Bangalore, India. Br. J. Cancer 1990, 62, 847–851. [Google Scholar] [CrossRef] [Green Version]
- Garrote, L.F.; Herrero, R.; Reyes, R.M.O.; Vaccarella, S.; Anta, J.L.; Ferbeye, L.; Muoz, N.; Franceschi, S. Risk factors for cancer of the oral cavity and oro-pharynx in Cuba. Br. J. Cancer 2001, 85, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Schatzkin, A.; Park, Y.; Leitzmann, M.F.; Hollenbeck, A.R.; Cross, A.J. Prospective Study of Dietary Fiber, Whole Grain Foods, and Small Intestinal Cancer. Gastroenterology 2008, 135, 1163–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Lo, C.-H.; He, X.; Hang, D.; Wang, M.; Wu, K.; Chan, A.T.; Ogino, S.; Giovannucci, E.L.; Song, M. Risk Factor Profiles Differ for Cancers of Different Regions of the Colorectum. Gastroenterology 2020, 159, 241–256.e13. [Google Scholar] [CrossRef] [PubMed]
- Lakatos, L.; Mester, G.; Erdelyi, Z.; David, G.; Pandur, T.; Balogh, M.; Fischer, S.; Vargha, P.; Lakatos, P.L. Risk factors for ulcerative colitis-associated colorectal cancer in a Hungarian cohort of patients with ulcerative colitis: Results of a population-based study. Inflamm. Bowel Dis. 2006, 12, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Center, M.M.; Jemal, A.; Ward, E. International trends in colorectal cancer incidence rates. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1688–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Vecchia, C.; Chatenoud, L.; Negri, E.; Franceschi, S. Session: Whole cereal grains, fibre and human cancer wholegrain cereals and cancer in Italy. Proc. Nutr. Soc. 2003, 62, 45–49. [Google Scholar] [CrossRef]
- Um, C.Y.; Campbell, P.T.; Carter, B.; Wang, Y.; Gapstur, S.M.; McCullough, M.L. Association between grains, gluten and the risk of colorectal cancer in the Cancer Prevention Study-II Nutrition Cohort. Eur. J. Nutr. 2020, 59, 1739–1749. [Google Scholar] [CrossRef]
- Vieira, A.R.; Abar, L.; Chan, D.S.M.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef]
- Tieri, M.; Ghelfi, F.; Vitale, M.; Vetrani, C.; Marventano, S.; Lafranconi, A.; Godos, J.; Titta, L.; Gambera, A.; Alonzo, E.; et al. Whole grain consumption and human health: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2020, 71, 668–677. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Laure Preterre, A.; Iqbal, K.; Bechthold, A.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; et al. Food groups and risk of colorectal cancer. Int. J. Cancer 2018, 142, 1748–1758. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.-F.; Wang, X.-K.; Tang, Y.-J.; Guan, X.-X.; Guo, Y.; Fan, J.-M.; Cui, L.-L. Association of whole grains intake and the risk of digestive tract cancer: A systematic review and meta-analysis. Nutr. J. 2020, 19, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Liu, Y.; Huang, H.; Li, D.; Zhao, Y. Diet quality score and survival rate in patients with colorectal cancer. Asia Pac. J. Clin. Nutr. 2019, 28, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Alegria-Lertxundi, I.; Aguirre, C.; Bujanda, L.; Fernández, F.J.; Polo, F.; Ordovás, J.M.; Etxezarraga, M.C.; Zabalza, I.; Larzabal, M.; Portillo, I.; et al. Food groups, diet quality and colorectal cancer risk in the Basque Country. World J. Gastroenterol. 2020, 26, 4108–4125. [Google Scholar] [CrossRef]
- Hullings, A.G.; Sinha, R.; Liao, L.M.; Freedman, N.D.; Graubard, B.I.; Loftfield, E. Whole grain and dietary fiber intake and risk of colorectal cancer in the NIH-AARP Diet and Health Study cohort. Am. J. Clin. Nutr. 2020, 112, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Wu, K.; Meyerhardt, J.A.; Ogino, S.; Wang, M.; Fuchs, C.S.; Giovannucci, E.L.; Chan, A.T. Fiber Intake and Survival After Colorectal Cancer Diagnosis. JAMA Oncol. 2018, 4, 71–79. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Wu, K.; Zhang, X.; Nishihara, R.; Cao, Y.; Fuchs, C.S.; Giovannucci, E.L.; Ogino, S.; Chan, A.T.; Song, M. Dietary intake of fiber, whole grains and risk of colorectal cancer: An updated analysis according to food sources, tumor location and molecular subtypes in two large US cohorts. Int. J. Cancer 2019, 145, 3040–3051. [Google Scholar] [CrossRef] [PubMed]
- WCRF/AICR. Diet, Nutrition, Physical Activity and Colorectal Cancer; Word Cancer Research Fund International: London, UK, 2018; pp. 1–111. ISBN 9781912259007. [Google Scholar]
- Pan, P.; Yu, J.; Wang, L.-S. Colon Cancer. Surg. Oncol. Clin. N. Am. 2018, 27, 243–267. [Google Scholar] [CrossRef]
- Nogacka, A.M.; Gómez-Martín, M.; Suárez, A.; González-Bernardo, O.; de los Reyes-Gavilán, C.G.; González, S. Xenobiotics Formed during Food Processing: Their Relation with the Intestinal Microbiota and Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 2051. [Google Scholar] [CrossRef] [Green Version]
- Bingham, S.A.; Day, N.E.; Luben, R.; Ferrari, P.; Slimani, N.; Norat, T.; Clavel-Chapelon, F.; Kesse, E.; Nieters, A.; Boeing, H.; et al. Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC): An observational study. Lancet 2003, 361, 1496–1501. [Google Scholar] [CrossRef]
- Bingham, S.A.; Day, N.E.; Luben, R. DEPARTMENT OF ERROR. Lancet 2003, 362, 1000. [Google Scholar] [CrossRef]
- Kranz, S.; Dodd, K.W.; Juan, W.Y.; Johnson, L.A.K.; Jahns, L. Whole grains contribute only a small proportion of dietary fiber to the U.S. diet. Nutrients 2017, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Janicke, B.; Hegardt, C.; Krogh, M.; Onning, G.; Åkesson, B.; Cirenajwis, H.M.; Oredsson, S.M. The antiproliferative effect of dietary fiber phenolic compounds ferulic acid and p-coumaric acid on the cell cycle of Caco-2 cells. Nutr. Cancer 2011, 63, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Hammond, W.A.; Swaika, A.; Mody, K. Pharmacologic resistance in colorectal cancer: A review. Ther. Adv. Med. Oncol. 2016, 8, 57–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pabla, B.; Bissonnette, M.; Konda, V.J. Colon cancer and the epidermal growth factor receptor: Current treatment paradigms, the importance of diet, and the role of chemoprevention. World J. Clin. Oncol. 2015, 6, 133–141. [Google Scholar] [CrossRef]
- Roy, N.; Narayanankutty, A.; Nazeem, P.; Valsalan, R.; Babu, T.; Mathew, D. Plant phenolics ferulic acid and P-coumaric acid inhibit colorectal cancer cell proliferation through EGFR down- regulation. Asian Pacific J. Cancer Prev. 2016, 17, 4017–4021. [Google Scholar]
- Qu, H.; Madl, R.L.; Takemoto, D.J.; Baybutt, R.C.; Wang, W. Lignans Are Involved in the Antitumor Activity of Wheat Bran in Colon Cancer SW480 Cells. J. Nutr. 2005, 135, 598–602. [Google Scholar] [CrossRef]
- Ayella, A.; Lim, S.; Jiang, Y.; Iwamoto, T.; Lin, D.; Tomich, J.; Wang, W. Cytostatic inhibition of cancer cell growth by lignan secoisolariciresinol diglucoside. Nutr. Res. 2010, 30, 762–769. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.R.; Patel, B.M. Secoisolariciresinol diglucoside rich extract of L. usitatissimum prevents diabetic colon cancer through inhibition of CDK4. Biomed. Pharmacother. 2016, 83, 733–739. [Google Scholar] [CrossRef]
- Yang, L.; Allred, K.F.; Dykes, L.; Allred, C.D.; Awika, J.M. Enhanced action of apigenin and naringenin combination on estrogen receptor activation in non-malignant colonocytes: Implications on sorghum-derived phytoestrogens. Food Funct. 2015, 6, 749–755. [Google Scholar] [CrossRef]
- Turktekin, M.; Konac, E.; Onen, H.I.; Alp, E.; Yilmaz, A.; Menevse, S. Evaluation of the effects of the flavonoid apigenin on apoptotic pathway gene expression on the colon cancer cell line (HT29). J. Med. Food 2011, 14, 1107–1117. [Google Scholar] [CrossRef]
- Takagaki, N.; Sowa, Y.; Oki, T.; Nakanishi, R.; Yogosawa, S.; Sakai, T. Apigenin induces cell cycle arrest and p21/WAF1 expression in a p53-independent pathway. Int. J. Oncol. 2005, 26, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; VanAlstyne, P.C.; Irons, K.A.; Chen, S.; Stewart, J.W.; Birt, D.F. Individual and interactive effects of apigenin analogs on G2/M cell-cycle arrest in human colon carcinoma cell lines. Nutr. Cancer 2004, 48, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Rao, C.; Zheng, G.; Wang, S. Luteolin suppresses colorectal cancer cell metastasis via regulation of the miR-384/pleiotrophin axis. Oncol. Rep. 2019, 42, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Hadi, L.A.; Di Vito, C.; Marfia, G.; Ferraretto, A.; Tringali, C.; Viani, P.; Riboni, L. Sphingosine kinase 2 and ceramide transport as key targets of the natural flavonoid luteolin to induce apoptosis in colon cancer cells. PLoS ONE 2015, 10, e0143384. [Google Scholar] [CrossRef] [Green Version]
- Kang, K.A.; Piao, M.J.; Ryu, Y.S.; Hyun, Y.J.; Park, J.E.; Shilnikova, K.; Zhen, A.X.; Kang, H.K.; Koh, Y.S.; Jeong, Y.J.; et al. Luteolin induces apoptotic cell death via antioxidant activity in human colon cancer cells. Int. J. Oncol. 2017, 51, 1169–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celesia, A.; Morana, O.; Fiore, T.; Pellerito, C.; D’Anneo, A.; Lauricella, M.; Carlisi, D.; De Blasio, A.; Calvaruso, G.; Giuliano, M.; et al. ROS-Dependent ER Stress and Autophagy Mediate the Anti-Tumor Effects of Tributyltin (IV) Ferulate in Colon Cancer Cells. Int. J. Mol. Sci. 2020, 21, 8135. [Google Scholar] [CrossRef] [PubMed]
- Hassani, A.; Azarian, M.M.S.; Ibrahim, W.N.; Hussain, S.A. Preparation, characterization and therapeutic properties of gum arabic-stabilized gallic acid nanoparticles. Sci. Rep. 2020, 10, 1–18. [Google Scholar] [CrossRef]
- Colquhoun, A.; Arnold, M.; Ferlay, J.; Goodman, K.J.; Forman, D.; Soerjomataram, I. Global patterns of cardia and non-cardia gastric cancer incidence in 2012. Gut 2015, 64, 1881–1888. [Google Scholar] [CrossRef]
- Cook, M.B. Editorial: Non-Acid reflux: The missing link between gastric atrophy and esophageal squamous cell carcinoma. Am. J. Gastroenterol. 2011, 106, 1930–1932. [Google Scholar] [CrossRef]
- Freedman, N.D.; Abnet, C.C.; Leitzmann, M.F.; Mouw, T.; Subar, A.F.; Hollenbeck, A.R.; Schatzkin, A. A prospective study of tobacco, alcohol, and the risk of esophageal and gastric cancer subtypes. Am. J. Epidemiol. 2007, 165, 1424–1433. [Google Scholar] [CrossRef]
- Hoyo, C.; Cook, M.B.; Kamangar, F.; Freedman, N.D.; Whiteman, D.C.; Bernstein, L.; Brown, L.M.; Risch, H.A.; Ye, W.; Sharp, L.; et al. Body mass index in relation to oesophageal and oesophagogastric junction adenocarcinomas: A pooled analysis from the international BEACON consortium. Int. J. Epidemiol. 2012, 41, 1706–1718. [Google Scholar] [CrossRef] [PubMed]
- Whiteman, D.C.; Sadeghi, S.; Pandeya, N.; Smithers, B.M.; Gotley, D.C.; Bain, C.J.; Webb, P.M.; Green, A.C. Combined effects of obesity, acid reflux and smoking on the risk of adenocarcinomas of the oesophagus. Gut 2008, 57, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, W.; Chow, W.H.; Lagergren, J.; Yin, L.; Nyrén, O. Risk of adenocarcinomas of the esophagus and gastric cardia in patients with gastroesophageal reflux diseases and after antireflux surgery. Gastroenterology 2001, 121, 1286–1293. [Google Scholar] [CrossRef]
- Binh, T.T.; Tuan, V.P.; Dung, H.D.Q.; Tung, P.H.; Tri, T.D.; Thuan, N.P.M.; Van Khien, V.; Hoan, P.Q.; Suzuki, R.; Uchida, T.; et al. Advanced non-cardia gastric cancer and Helicobacter pylori infection in Vietnam. Gut Pathog. 2017, 9, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamangar, F.; Dawsey, S.M.; Blaser, M.J.; Perez-Perez, G.I.; Pietinen, P.; Newschaffer, C.J.; Abnet, C.C.; Albanes, D.; Virtamo, J.; Taylor, P.R. Opposing risks of gastric cardia and noncardia gastric adenocarcinomas associated with Helicobacter pylori seropositivity. J. Natl. Cancer Inst. 2006, 98, 1445–1452. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Cai, H.; Sasazuki, S.; Tsugane, S.; Zheng, W.; Cho, E.R.; Jee, S.H.; Michel, A.; Pawlita, M.; Xiang, Y.B.; et al. Fruit and vegetable consumption, Helicobacter pylori antibodies, and gastric cancer risk: A pooled analysis of prospective studies in China, Japan, and Korea. Int. J. Cancer 2017, 140, 591–599. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.J.; Wu, D.C.; Lin, J.M.; Wu, M.T.; Sung, F.C. Etiologic factors of gastric cardiac adenocarcinoma among men in Taiwan. World J. Gastroenterol. 2009, 15, 5472–5480. [Google Scholar] [CrossRef]
- Yamaji, Y.; Watabe, H.; Yoshida, H.; Kawabe, T.; Wada, R.; Mitsushima, T.; Omata, M. High-risk population for gastric cancer development based on serum pepsinogen status and lifestyle factors. Helicobacter 2009, 14, 81–86. [Google Scholar] [CrossRef]
- Flores-Luna, L.; Bravo, M.M.; Kasamatsu, E.; Lazcano Ponce, E.C.; Martinez, T.; Torres, J.; Camorlinga-Ponce, M.; Kato, I. Risk factors for gastric precancerous and cancers lesions in Latin American counties with difference gastric cancer risk. Cancer Epidemiol. 2020, 64, 101630. [Google Scholar] [CrossRef]
- Gaddy, J.A.; Radin, J.N.; Loh, J.T.; Zhang, F.; Kay Washington, M.; Peek, R.M.; Scott Algood, H.M.; Cover, T.L. High dietary salt intake exacerbates Helicobacter pylori-induced gastric carcinogenesis. Infect. Immun. 2013, 81, 2258–2267. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, S.F.; Ahmed, K.; Saeed, S.A.; Khan, U.; Sugiyama, T. Can Diet Modulate Helicobacter pylori-associated Gastric Pathogenesis? An Evidence-Based Analysis. Nutr. Cancer 2017, 69, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz. Gastroenterol. 2019, 14, 26. [Google Scholar] [CrossRef]
- McCullough, M.L.; Robertson, A.S.; Jacobs, E.J.; Chao, A.; Calle, E.E.; Thun, M.J. A prospective study of diet and stomach cancer mortality in United States men and women. Cancer Epidemiol. Biomark. Prev. 2001, 10, 1201–1205. [Google Scholar]
- Li, K.; Zhang, B. The association of dietary β-carotene and vitamin A intake on the risk of esophageal cancer: A meta-analysis. Rev. Esp. Enferm. Dig. 2020, 112. [Google Scholar] [CrossRef]
- Xu, Y.; Yang, J.; Du, L.; Li, K.; Zhou, Y. Association of whole grain, refined grain, and cereal consumption with gastric cancer risk: A meta-analysis of observational studies. Food Sci. Nutr. 2019, 7, 256–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Zhan, R.; Lu, J.; Zhong, L.; Peng, X.; Wang, M.; Tang, S. Grain consumption and risk of gastric cancer: A meta-analysis. Int. J. Food Sci. Nutr. 2020, 71, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Frentzel-Beyme, R.; Berger, M.; Berndt, V.; Göres, W.; Körner, M.; Lohmeier, R.; Menarcher, A.; Männl, H.F.K.; Meinhardt, M.; et al. Case-control study on stomach cancer in Germany. Int. J. Cancer 1991, 47, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.A.; Pera, G.; Agudo, A.; Bas Bueno-de-Mesquita, H.; Palli, D.; Boeing, H.; Carneiro, F.; Berrino, F.; Sacerdote, C.; Tumino, R.; et al. Cereal fiber intake may reduce risk of gastric adenocarcinomas: The EPIC-EURGAST study. Int. J. Cancer 2007, 121, 1618–1623. [Google Scholar] [CrossRef]
- Bravi, F.; Scotti, L.; Bosetti, C.; Bertuccio, P.; Negri, E.; La Vecchia, C. Dietary fiber and stomach cancer risk: A case–control study from Italy. Cancer Causes Control 2009, 20, 847–853. [Google Scholar] [CrossRef]
- Gaesser, G.A. Whole Grains, Refined Grains, and Cancer Risk: A Systematic Review of Meta-Analyses of Observational Studies. Nutrients 2020, 12, 3756. [Google Scholar] [CrossRef]
- Díaz-Gómez, R.; López-Solís, R.; Obreque-Slier, E.; Toledo-Araya, H. Comparative antibacterial effect of gallic acid and catechin against Helicobacter pylori. LWT Food Sci. Technol. 2013, 54, 331–335. [Google Scholar] [CrossRef]
- Ho, H.H.; Chang, C.-S.; Ho, W.C.; Liao, S.Y.; Lin, W.L.; Wang, C.J. Gallic acid inhibits gastric cancer cells metastasis and invasive growth via increased expression of RhoB, downregulation of AKT/small GTPase signals and inhibition of NF-κB activity. Toxicol. Appl. Pharmacol. 2013, 266, 76–85. [Google Scholar] [CrossRef]
- Chang, H.T.; Chen, I.L.; Chou, C.T.; Liang, W.Z.; Kuo, D.H.; Shieh, P.; Jan, C.R. Effect of caffeic acid on Ca2+ homeostasis and apoptosis in SCM1 human gastric cancer cells. Arch. Toxicol. 2013, 87, 2141–2150. [Google Scholar] [CrossRef]
- Chen, J.; Chen, J.; Li, Z.; Liu, C.; Yin, L. The apoptotic effect of apigenin on human gastric carcinoma cells through mitochondrial signal pathway. Tumor Biol. 2014, 35, 7719–7726. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Yuan, L.H.; Xia, W. Inhibitory effects of apigenin on the growth of gastric carcinoma SGC-7901 cells. World J. Gastroenterol. 2005, 11, 4461–4464. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Ding, B.Z.; Lin, Y.P.; Wang, H.B. MiR-34a, as a suppressor, enhance the susceptibility of gastric cancer cell to luteolin by directly targeting HK1. Gene 2018, 644, 56–65. [Google Scholar] [CrossRef]
- Hu, L.; Fan, Z.Y.; Wang, H.X.; Zhu, Z.L.; Cao, S.; Wu, X.Y.; Li, J.F.; Su, L.P.; Li, C.; Zhu, Z.G.; et al. Luteolin suppresses gastric cancer progression by reversing epithelial-mesenchymal transition via suppression of the Notch signaling pathway. J. Transl. Med. 2017, 15, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Jang, M.G.; Ko, H.C.; Kim, S.J. Effects of p-coumaric acid on microRNA expression profiles in SNU-16 human gastric cancer cells. Genes Genom. 2020, 42, 817–825. [Google Scholar] [CrossRef]
- Wu, H.; Huang, M.; Liu, Y.; Shu, Y.; Liu, P. Luteolin Induces Apoptosis by Up-regulating miR-34a in Human Gastric Cancer Cells. Technol. Cancer Res. Treat. 2015, 14, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Pennathur, A.; Gibson, M.K.; Jobe, B.A.; Luketich, J.D. Oesophageal carcinoma. Lancet 2013, 381, 400–412. [Google Scholar] [CrossRef] [Green Version]
- Chevallay, M.; Bollschweiler, E.; Chandramohan, S.M.; Schmidt, T.; Koch, O.; Demanzoni, G.; Mönig, S.; Allum, W. Cancer of the gastroesophageal junction: A diagnosis, classification, and management review. Ann. N. Y. Acad. Sci. 2018, 1434, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, G.K.; Yanala, U.; Ravipati, A.; Follet, M.; Vijayakumar, M.; Are, C. Global trends in esophageal cancer. J. Surg. Oncol. 2017, 115, 564–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnal, M.J.D.; Arenas, Á.F.; Arbeloa, Á.L. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J. Gastroenterol. 2015, 21, 7933. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.-P.; Yan, L.-B.; Liu, Z.-Z.; Zhao, W.-J.; Zhang, C.-X.; Chen, Y.-M.; Lao, X.Q.; Liu, X. Dietary factors and risk of mortality among patients with esophageal cancer: A systematic review. BMC Cancer 2020, 20, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Xuan, F.; Li, W.; Guo, X.; Liu, C. Dietary carbohydrate intake and the risk of esophageal cancer: A meta-analysis. Biosci. Rep. 2020, 40. [Google Scholar] [CrossRef] [Green Version]
- Levi, F.; Pasche, C.; Lucchini, F.; Bosetti, C.; Franceschi, S.; Monnier, P.; Vecchia La, C. Food groups and oesophageal cancer risk in Vaud, Switzerland. Eur. J. Cancer Prev. 2000, 9, 257–264. [Google Scholar] [CrossRef]
- Kubo, A.; Block, G.; Quesenberry, C.P.; Buffler, P.; Corley, D.A. Effects of dietary fiber, fats, and meat intakes on the risk of barrett’s esophagus. Nutr. Cancer 2009, 61, 607–616. [Google Scholar] [CrossRef] [Green Version]
- Skeie, G.; Braaten, T.; Olsen, A.; Kyrø, C.; Tjønneland, A.; Landberg, R.; Nilsson, L.M.; Wennberg, M.; Overvad, K.; Åsli, L.A.; et al. Intake of whole grains and incidence of oesophageal cancer in the HELGA Cohort. Eur. J. Epidemiol. 2016, 31, 405–414. [Google Scholar] [CrossRef]
- Slavin, J.L. Mechanisms for the Impact of Whole Grain Foods on Cancer Risk. J. Am. Coll. Nutr. 2000, 19, 300S–307S. [Google Scholar] [CrossRef]
- Frølich, W.; Åman, P.; Tetens, I. Whole grain foods and health—A Scandinavian perspective. Food Nutr. Res. 2013, 57, 18503. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Zhang, Z.; Xu, J.; Xu, G.; Liu, X. Dietary fiber intake reduces risk for Barrett’s esophagus and esophageal cancer. Crit. Rev. Food Sci. Nutr. 2017, 57, 2749–2757. [Google Scholar] [CrossRef] [PubMed]
- Mayne, S.T.; Navarro, S.A. Diet, Obesity and Reflux in the Etiology of Adenocarcinomas of the Esophagus and Gastric Cardia in Humans. J. Nutr. 2002, 132, 3467S–3470S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulholland, H.G.; Cantwell, M.M.; Anderson, L.A.; Johnston, B.T.; Watson, R.G.P.; Murphy, S.J.; Ferguson, H.R.; McGuigan, J.; Reynolds, J.V.; Comber, H.; et al. Glycemic index, carbohydrate and fiber intakes and risk of reflux esophagitis, Barrett’s esophagus, and esophageal adenocarcinoma. Cancer Causes Control 2009, 20, 279–288. [Google Scholar] [CrossRef]
- McFadden, D.; Riggs, D.; Jackson, B.; Cunningham, C. Corn-derived carbohydrate inositol hexaphosphate inhibits Barrett’s adenocarcinoma growth by pro-apoptotic mechanisms. Oncol. Rep. 2008, 19, 563–566. [Google Scholar] [CrossRef] [Green Version]
- Nobel, Y.R.; Snider, E.J.; Compres, G.; Freedberg, D.E.; Khiabanian, H.; Lightdale, C.J.; Toussaint, N.C.; Abrams, J.A. Increasing Dietary Fiber Intake Is Associated with a Distinct Esophageal Microbiome. Clin. Transl. Gastroenterol. 2018, 9, e199. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.-W.; Lee, S.-M. Protective Effects of Chlorogenic Acid against Experimental Reflux Esophagitis in Rats. Biomol. Ther. 2014, 22, 420–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, Y.; Li, R.; Feng, C.; Li, X.; Huang, S.; Wang, L.; Liu, Z.; Jiang, J.; Han, Y. Chlorogenic acid inhibits esophageal squamous cell carcinoma growth in vitro and in vivo by downregulating the expression of BMI1 and SOX2. Biomed. Pharmacother. 2020, 121, 109602. [Google Scholar] [CrossRef]
- Faried, A.; Kurnia, D.; Faried, L.S.; Usman, N.; Miyazaki, T.; Kato, H.; Kuwano, H. Anticancer effects of gallic acid isolated from Indonesian herbal medicine, Phaleria macrocarpa (Scheff.) Boerl, on human cancer cell lines. Int. J. Oncol. 2007, 30, 605–613. [Google Scholar] [CrossRef]
- Qiu, J.G.; Wang, L.; Liu, W.J.; Wang, J.F.; Zhao, E.J.; Zhou, F.M.; Ji, X.B.; Wang, L.H.; Xia, Z.K.; Wang, W.; et al. Apigenin inhibits IL-6 transcription and suppresses esophageal carcinogenesis. Front. Pharmacol. 2019, 10, 1002. [Google Scholar] [CrossRef] [Green Version]
- Shioga, T.; Matsushima, S.; Yamada, E.; Uchiyama, T.; Noto, H.; Suzuki, D.; Nonaka, T.; Miyazawa, S.; Komatsu, T.; Yamamoto, Y.; et al. Esophageal carcinosarcoma that was diagnosed as a granulocyte-colony stimulating factor and interleukin-6-producing tumor with a tumor fever. Intern. Med. 2018, 57, 2819–2825. [Google Scholar] [CrossRef] [Green Version]
- SACN. Carbohydrates and Health; The Stationery Office: London, UK, 2015; ISBN 9780117082847. [Google Scholar]
- CREA. Linee Guida per una sana Alimentazione; CREA: Rome, Italy, 2018; pp. 1689–1699. [Google Scholar]
- Joint WHO/FAO Expert Consultation. Diet, nutrition and the prevention of chronic diseases. In World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- PHE. Government Dietary Recommendations; Public Health England: London, UK, 2016. [Google Scholar]
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Compound 1 | Wheat | Oat | Corn | Rice | Refs |
|---|---|---|---|---|---|
| Dietary fiber | 9.7–13.1 | 7.6–10.6 | 2–7.3 | 1.4–3.75 | [57,58] |
| Total polyphenols | 538 | 471.7 | 497.1 | 421.8 | [59] |
| Total phenolic acids | 1342 (75%) 2 | 472 (75%) 2 | 601 (85%) 2 | 197–376 (62%) 2 | [60,61] |
| Ferulic acid | 11.6–870 | 249.4–1044.9 | 97–584.0 | 68.2–301.7 | [62] |
| p-coumaric acid | 3.5–293.0 | 607.3 | 97.0–584.0 | 22.8–85.0 | [62] |
| Gallic acid | 6.5–195.0 | 1.7–241.2 | 0.5–116.5 | 5.5–115.6 | [62] |
| Caffeic acid | 0.5–51.9 | 3.6–9.2 | 5.7–24.4 | 1.0–3.5 | [62] |
| Total flavonoids | 95.8–212 | n.r. | 607.1–1277 | 94–3274 | [63] |
| Study Type and Design | Main Findings * | Refs | |
|---|---|---|---|
| Whole grains | 14-year US prospective population-based case-control study (112,149 participants (1742 CRC) from the Cancer Prevention Study-II Nutrition Cohort 1999–2013) Quintiles of WG intake (g/day):
| Similar WG intake in women (mean: 72.8 g/day; 10th–90th percentile distribution: 10.6–168 g/day) and men (mean: 74.5 g/day; 10th–90th percentile distribution: 9.2–174 g/day) High WG intake associated with low CRC risk among older men, but not women (HR = 0.77, 95% CI 0.61–0.97; p = 0.03 for men; HR = 1.10, 95% CI 0.88–1.36; p = 0.14 for women; p interaction by sex = 0.01) Men in the highest quintile: 43% reduced risk (HR = 0.57, 95% CI 0.35–0.93, p = 0.04) No association of RG with CRC risk | [109] |
| 10-year prospective population study (369 CRC patients, 154 deaths during the follow-up) Quartiles of WG intake (g/day)
| High WG intake associated with risk of mortality (HRQ4 vs. Q1 = 0.56, 95% CI 0.35–0.89; p for trend 0.05) | [114] | |
| Meta-analysis of 11 prospective studies for WG consumption and 3 reports for RG consumption | Inverse association between CRC risk and WG intake (RR = 0.88, 95% CI 0.83–0.94, I2 = 35%, p = 0.13) (10 studies with 9223 CRC cases; overall intake range: 0–374 g/day) Each additional daily 30 g of WGs inversely associated with CRC risk (RR = 0.95, 95% CI 0.93–0.97, I2 = 58%, p = 0.02); 20% decreased risk with WG intake up to 120 g/day No association for RG intake (RR = 1.46, 95% CI 0.80–2.67, I2 = 71%, p = 0.06) (900 CRC cases, overall intake range: 15–585 g/day) | [112] | |
| Meta-analysis of 34 studies of WG intake and risk of digestive tract cancer [CRC: 7 case-control and 10 cohort studies (1,489,581 participants and 19,424 cases)] | Inverse association between CRC risk and WG intake (RR = 0.89, 95% CI 0.84–0.93; p < 0.001; I2 = 38.2%, p = 0.029). Positive effects of WGs only in studies with sample size ≥500 (RR = 0.91, 95% CI 0.88–0.94, p < 0.001) No statistically significant heterogeneity in women (I2 = 0%, p = 0.619), European (I2 = 0%, p = 0.732), before 2010 publication year (I2 = 0%, p = 0.622) and adjustment for energy (I2 = 4.6%, p = 0.399) studies | [113] | |
| Whole grains/whole grain fiber | Spanish observational case-control study (308 CRC and 308 controls)
| WG intake lower in CRC patients than controls (14.4 ± 19.9 vs. 18.8 ± 23.4 g/day, p = 0.012). Inverse association between WG intake and CRC risk (ORT3 vs. T1 = 0.62, 95% CI 0.39–0.98) Consumption of fiber-containing foods, especially WG, associated with lower CRC risk (ORT3 vs. T1 = 0.65, 95% CI 0.35–1.21). | [115] |
| US Prospective NIH-AARP Diet and Health Study (1995–2011) including 478,994 subjects (285,456 men and 193,538 women) cancer free at the beginning; 10,200 incident cases (6712 men and 3488 women) at the end. Quintiles of WG intake (servings/1000 kcal/day)
| Positive association for both WGs (HRQ5 vs. Q1 = 0.69, 95% CI 0.64–0.73; p < 0.001) and dietary fiber (HRQ5 vs. Q1 = 0.70, 95% CI 0.66–0.75; p < 0.0001) After adjustment for potential confounders: HRQ5 vs. Q1 = 0.83 (95% CI 0.78–0.89; p < 0.001) for WGs and HRQ5 vs. Q1 = 0.92 (95% CI 0.86–0.99; p < 0.03) for dietary fiber intake. The association remained statistically significant after adjustment for folate (HRQ5 vs. Q1 = 0.84, 95% CI 0.79–0.90; p < 0.001) and dietary fiber intake (HRQ5 vs. Q1 = 0.84, 95% CI 0.78–0.90; p < 0.001) Only fiber from grains was inversely associated with CRC (HRQ5 vs. Q1 = 0.89, 95% CI 0.83–0.96; p < 0.001) No sex-dependence (p = 0.13 for interaction) | [116] | |
| 963 US females from Nurses’ Health Study cohort (NHS; 1980–2010) and 612 US males from Health Professionals Follow-up Study cohort (HPFS; 1986–2010) diagnosed stage I to III CRC throughout follow-up. Quintiles of WG fiber intake (g/1000 kcal/day)
| WG intake associated with low CRC-specific mortality (HR per 20 g/day increment = 0.72, 95% CI 0.59–0.88; p = 0.002), also after adjusting for fiber intake (HR = 0.77, 95% CI 0.62–0.96; p = 0.02), and all-cause mortality (HR = 0.88, 95% CI 0.80–0.97; p = 0.008 for trend). Cereal fiber intake associated with low CRC-specific mortality (HR per 5 g/day increment = 0.67, 95% CI 0.50–0.90; p = 0.007) and all-cause mortality (HR = 0.78, 95% CI 0.68–0.90; p < 0.001). Vegetable fiber associated with low all-cause mortality (HR = 0.83, 95% CI 0.72–0.96; p = 0.009), but not CRC-specific mortality (HR = 0.82, 95% CI 0.60–1.13; p = 0.22); no association for fruit fiber. Patients with increased fiber intake after diagnosis: lower mortality rate [each 5 g/day increase associated with 18% decrease in CRC-specific mortality (95% CI 7–28%; p = 0.002) and 14% decrease in all-cause mortality (95% CI 8–19%; p = 0.001)]. | [117] | |
| 1902 US females from Nurses’ Health Study cohort (NHS; 1980–2012) and 1276 US males from Health Professionals Follow-up Study cohort (HPFS; 1986–2012) diagnosed CRC throughout follow-up. Deciles of total fiber intake (g/day):
| No association between total fiber and CRC risk. No association for fruit or vegetable fiber. Inverse association between cereal fiber intake and CRC risk only in men (HRD10 vs. D1 = 0.75, 95% CI 0.57–1.00). Inverse association between intake of WG fiber and risk of CRC only in men (HRD10 vs. D1 = 0.72, 95% CI 0.54–0.96). | [118] |
| Study Type and Design | Main Findings * | Refs | |
|---|---|---|---|
| Whole grains | Prospective 14-year population-based case-control Cancer Prevention Study [533,391 women (439 deaths for GC) and 436,654 men (910 deaths for GC)] Tertiles of WG intake (days/week):
| Men: high WG consumption associated with decreased risk only in age-adjusted model (RRT2 vs. T1 = 0.87, 95% CI 0.74–1.03; RRT3 vs. T1 = 0.77, 95% CI 0.66–0.90; p < 0.001), but not in multivariate-adjusted model (RRT2 vs. T1 = 0.94, 95% CI 0.79–1.11; RRT3 vs. T1 = 0.90, 95% CI 0.77–1.06; p = 0.17). More than 4 times/week cold cereal intake related to lower risk with respect to low (<once/week) intake (RR = 0.83, 95% CI 0.68–1.00; p = 0.03 for trend). Men with positive family GC history, consuming WG products >4 days/week, showed lower risk (RR = 0.31, 95% CI 0.15–0.64) with respect to men with no family GC history. Women: no association between WGs and GC risk. Women consuming brown rice, whole wheat or barley 6 to 7 times/week were at greater risk of fatal stomach cancer with respect to women with no intake (RR T3 vs. T1 = 1.41, 95% CI 1.04–1.91; p for trend = 0.05). | [156] |
| Retrospective 10-year hospital-based case-control study (745 GC patients and 3526 controls) Tertiles of WG food intake (simple score of consumption):
| Whole meal consumption negatively correlated with GC risk For WG foods: ORT3 vs. T1 = 0.5, 95% CI 0.4–0.7 For RG foods: ORT2 vs. T1 = 1.24, 95% CI 1.0–1.5 and ORT3 vs. T1 = 1.54, 95% CI 1.2–2.0 | [92] | |
| Retrospective 3-year hospital-based case-control study (143 GC patients and 328 controls) Tertiles of whole-meal bread intake (simple score of consumption):
| Whole meal consumption negatively correlated with GC risk RRT2 vs. T1 = 1.26, 95% CI 0.79–2.01 RRT3 vs. T1 = 0.48, 95% CI 0.28–0.82 | [160] | |
| Meta-analysis of 5 hospital-based case-control, 4 population-based case-control and 2 prospective cohort studies (2920 GC cases and 527,256 controls) | WG consumption inversely related to GC in Europe (OR = 0.72, 95% CI 0.19–1.24) and America (OR = 0.61, 95% CI 0.38–0.85), both in hospital-based case-control (OR = 0.50, 95% CI 0.35–0.65) and cohort (OR = 0.61, 95% CI 0.38–0.85) studies | [158] | |
| Meta-analysis of 34 studies of WG intake and risk of digestive tract cancer [GC: 9 case-control and 2 cohort studies (1,021,955 participants and 8274 GC cases)] | WG consumption: 36% decrease in GC risk (RR = 0.64, 95% CI 0.53–0.79; p < 0.001), with a significant heterogeneity (I2 = 78.2%, p = 0.001) WG intake was a protective factor for case-control (RR = 0.55, 95% CI 0.41–0.74; p < 0.001) and European (RR = 0.64, 95% CI 0.53–0.79; p < 0.001) studies No significant association in cohort (RR = 0.89, 95% CI 0.78–1.01; p = 0.070) and American (RR = 0.70, 95% CI 0.50–1.00; p = 0.051) studies | [113] | |
| Meta-analysis of 19 studies (17 case-control and 2 cohort studies; 994,258 participants) Consumption of WGs or RGs:
| WG consumption: 13% decrease in GC risk (OR = 0.87, 95% CI 0.79–0.95; p = 0.003) High consumption: 44% reduced risk (OR high vs. low = 0.56, 95% CI 0.45–0.69; p < 0.001) No significant correlation for moderate consumption RG consumption: 36% increase in GC risk (OR = 1.36, 95% CI 1.21–1.54; p < 0.001) 63% increased GC risk in high consumers (OR = 1.63, 95% CI 1.49–1.79; p < 0.001) 28% increased GC risk in moderate consumers (OR = 1.28, 95% CI 1.18–1.39; p < 0.001) 53% increased GC risk in rice consumers (OR = 1.53, 95% CI 1.31–1.79; p < 0.001) 28% increased GC risk in RG, not-rice consumers (OR = 1.28, 95% CI 1.11–1.49; p = 001) No correlation between small amounts of RG intake and GC risk | [159] | |
| Whole grain fiber | Prospective 14-year cohort Iowa Women’s Health Study (34,651 initially free-cancer women; 56 GC) Tertiles of WG fiber intake (g/day):
| WG fiber intake inversely related to GC risk (HRRT3 vs. T1 = 0.53) No association for RG fiber intake | [95] |
| Study Type and Design | Main Findings * | Refs | |
|---|---|---|---|
| Whole grains | Swiss 7-year retrospective hospital-based case-control study (349 controls and 101 EC patients). Whole (whole wheat bread and cereals) and refined (white bread and biscuits, pizza, pasta and rice) grain foods Tertiles for WG intake (times/week):
| EC risk inversely correlated to WG intakes (ORT3 vs. T1 = 0.30, CI 95% 0.1–0.6) and directly correlated to RG intakes (ORT2 vs. T1 = 2.6, CI 95% 1.1–6.2; ORT3 vs. T1 = 3.7, CI 95% 1.8–7.9) | [91] |
| Italian 14-year hospital-based case-control studies (1983–1997) 10058 controls and 11.990 cancer patients (410 EC cases). Tertiles for WG food intake (day/week):
| WG consumption associated with reduced risk (OR T3 vs. T1 = 0.4, 95% CI 0.2–0.7 and ORT2 vs. T1 = 0.4, 95% CI 0.3–0.7) | [108] | |
| Meta-analysis of 34 studies of WG intake and risk of digestive tract cancer (EC: 4 case-control studies and 2 cohort studies (151,742 participants and 1223 EC cases)) | WG consumption associated with reduced risk (RR = 0.54, 95% CI 0.44–0.67, p < 0.001) No statistically significant heterogeneity (I2 = 27.7%, p = 0.217) | [113] | |
| Scandinavian 11-year prospective population-based case-control study (113,993 members from HELGA cohort including 56 EAC patients and 54 ESCC patients; 73.2% male and 33.8% women) Sex-specific tertiles of total WG intake (g/day):
| Inverse correlation between EC risk and total WGs (HR T3 vs. T1 = 0.55, 95% CI 0.31–0.97) and WG products (HR T3 vs. T1 = 0.51, 95% CI 0.30–0.88 per 25 g) Only wheat showed significant associations in adjusted models (adjusted HRT3 vs. T1 = 0.32, 95% CI 0.16–0.63) Only WG bread showed significant associations in adjusted model (adjusted HR T3 vs. T1 = 0.88, 95% CI 0.80–0.96 per 25 g WG bread) EAC: adjusted HR = 0.81, 95% CI 0.65–1.02 per 50 g WG products and HR = 0.85, 95% CI 0.66–1.09 per 20 g WGs ECCS: adjusted HR = 0.66, 95% CI 0.51–0.86 per 50 g WG products and adjusted HR = 0.75, 95% CI 0.56–1.00 per 20 g WGs | [181] | |
| Whole grains/whole grain fiber | Prospective 14-year cohort Iowa Women’s Health Study (34,651 initially free-cancer women; 21 EC and 56 GC) Tertiles of WG intake (servings/week):
| Inverse correlation between EC risk and WG (HRR T3 vs. T1 = 0.47) or WG fiber (HRR T3 vs. T1 = 0.35) intake | [95] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tullio, V.; Gasperi, V.; Catani, M.V.; Savini, I. The Impact of Whole Grain Intake on Gastrointestinal Tumors: A Focus on Colorectal, Gastric, and Esophageal Cancers. Nutrients 2021, 13, 81. https://doi.org/10.3390/nu13010081
Tullio V, Gasperi V, Catani MV, Savini I. The Impact of Whole Grain Intake on Gastrointestinal Tumors: A Focus on Colorectal, Gastric, and Esophageal Cancers. Nutrients. 2021; 13(1):81. https://doi.org/10.3390/nu13010081
Chicago/Turabian StyleTullio, Valentina, Valeria Gasperi, Maria Valeria Catani, and Isabella Savini. 2021. "The Impact of Whole Grain Intake on Gastrointestinal Tumors: A Focus on Colorectal, Gastric, and Esophageal Cancers" Nutrients 13, no. 1: 81. https://doi.org/10.3390/nu13010081
APA StyleTullio, V., Gasperi, V., Catani, M. V., & Savini, I. (2021). The Impact of Whole Grain Intake on Gastrointestinal Tumors: A Focus on Colorectal, Gastric, and Esophageal Cancers. Nutrients, 13(1), 81. https://doi.org/10.3390/nu13010081