
Adherence to a Plant-Based Diet and Consumption of Specific Plant Foods—Associations with 3-Year Weight-Loss Maintenance and Cardiometabolic Risk Factors: A Secondary Analysis of the PREVIEW Intervention Study

 , ,
, ,  , , ,
, , ,  , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
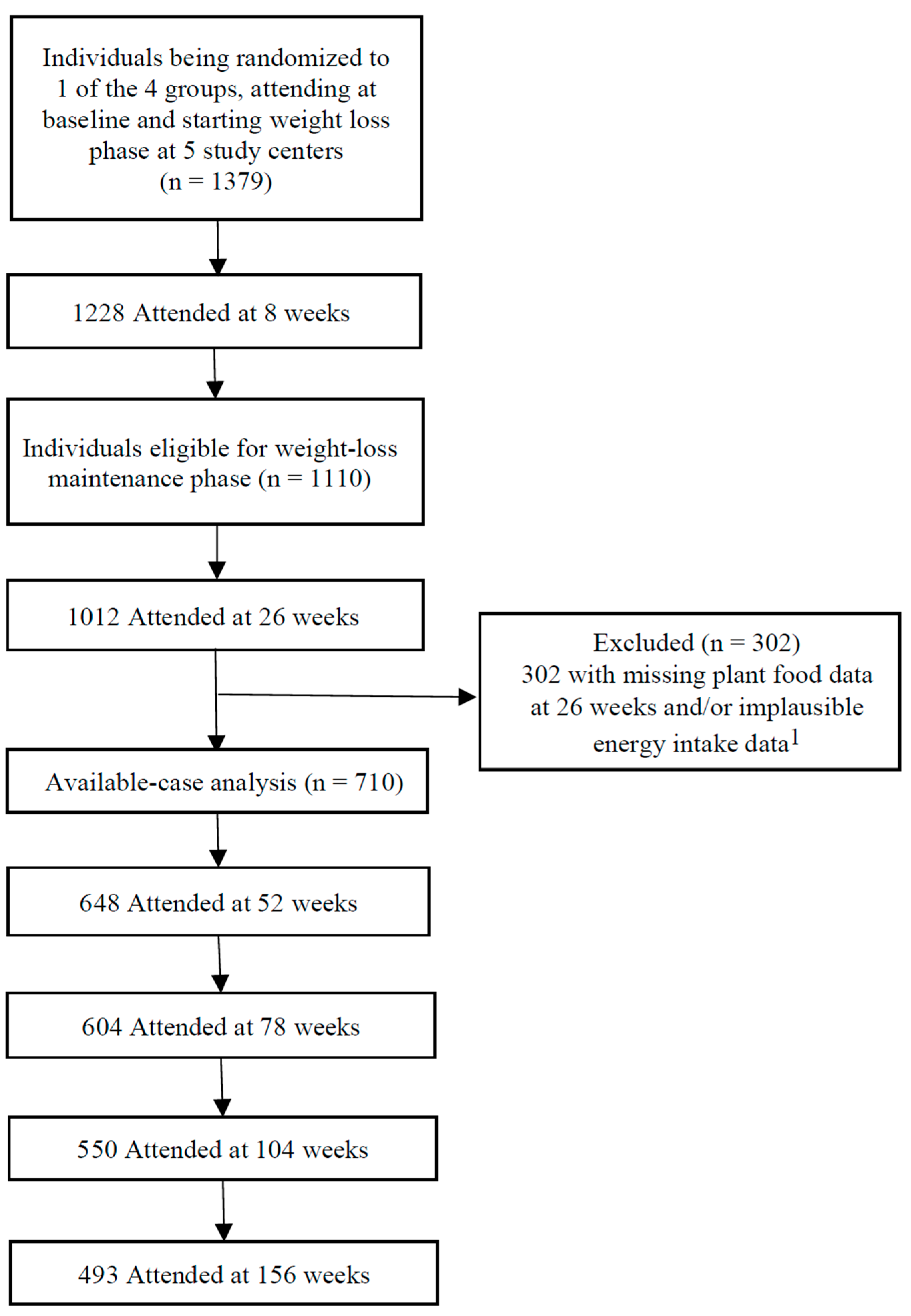
2.2. Study Population
2.3. Assessment of Dietary Intake and Adherence to an Overall Plant-Based Diet
2.4. Assessment of Outcomes
2.5. Assessment of Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]
- Bechthold, A.; Boeing, H.; Tetens, I.; Schwingshackl, L.; Nothlings, U. Perspective: Food-Based Dietary Guidelines in Europe-Scientific Concepts, Current Status, and Perspectives. Adv. Nutr. 2018, 9, 544–560. [Google Scholar] [CrossRef]
- Willett, W.; Rockstrom, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Aune, D. Plant Foods, Antioxidant Biomarkers, and the Risk of Cardiovascular Disease, Cancer, and Mortality: A Review of the Evidence. Adv. Nutr. 2019, 10, S404–S421. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef]
- Choi, Y.; Larson, N.; Gallaher, D.D.; Odegaard, A.O.; Rana, J.S.; Shikany, J.M.; Steffen, L.M.; Jacobs, D.R., Jr. A Shift toward a Plant-Centered Diet from Young to Middle Adulthood and Subsequent Risk of Type 2 Diabetes and Weight Gain: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Diabetes Care 2020, 43, 2796–2803. [Google Scholar] [CrossRef] [PubMed]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Adv. Nutr. 2019, 10, S275–S283. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.Y.; Huang, C.C.; Hu, F.B.; Chavarro, J.E. Vegetarian Diets and Weight Reduction: A Meta-Analysis of Randomized Controlled Trials. J. Gen. Intern. Med. 2016, 31, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant-Based Diets Are Associated With a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All-Cause Mortality in a General Population of Middle-Aged Adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Hu, F.B. Plant-based diets and cardiovascular health. Trends Cardiovasc. Med. 2018, 28, 437–441. [Google Scholar] [CrossRef]
- Bielefeld, D.; Grafenauer, S.; Rangan, A. The Effects of Legume Consumption on Markers of Glycaemic Control in Individuals with and without Diabetes Mellitus: A Systematic Literature Review of Randomised Controlled Trials. Nutrients 2020, 12, 2123. [Google Scholar] [CrossRef]
- Abbaspour, N.; Roberts, T.; Hooshmand, S.; Kern, M.; Hong, M.Y. Mixed nut consumption may improve cardiovascular disease risk factors in overweight and obese adults. Nutrients 2019, 11, 1488. [Google Scholar] [CrossRef] [Green Version]
- Brown, R.C.; Tey, S.L.; Gray, A.R.; Chisholm, A.; Smith, C.; Fleming, E.; Parnell, W. Association of Nut Consumption with Cardiometabolic Risk Factors in the 2008/2009 New Zealand Adult Nutrition Survey. Nutrients 2015, 7, 7523–7542. [Google Scholar] [CrossRef] [Green Version]
- Carter, P.; Gray, L.J.; Talbot, D.; Morris, D.H.; Khunti, K.; Davies, M.J. Fruit and vegetable intake and the association with glucose parameters: A cross-sectional analysis of the Let’s Prevent Diabetes Study. Eur. J. Clin. Nutr. 2013, 67, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Fisk, P.S., II; Middaugh, A.L.; Rhee, Y.S.; Brunt, A.R. Few favorable associations between fruit and vegetable intake and biomarkers for chronic disease risk in American adults. Nutr. Res. 2011, 31, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Toumpanakis, A.; Turnbull, T.; Alba-Barba, I. Effectiveness of plant-based diets in promoting well-being in the management of type 2 diabetes: A systematic review. BMJ Open Diabetes Res. Care 2018, 6, e000534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoyama, Y.; Barnard, N.D.; Levin, S.M.; Watanabe, M. Vegetarian diets and glycemic control in diabetes: A systematic review and meta-analysis. Cardiovasc. Diagn. Ther. 2014, 4, 373–382. [Google Scholar] [CrossRef]
- Fogelholm, M.; Larsen, T.M.; Westerterp-Plantenga, M.; Macdonald, I.; Martinez, J.A.; Boyadjieva, N.; Poppitt, S.; Schlicht, W.; Stratton, G.; Sundvall, J.; et al. PREVIEW: Prevention of diabetes through lifestyle intervention and population studies in Europe and around the world. design, methods, and baseline participant description of an adult cohort enrolled into a three-year randomised clinical trial. Nutrients 2017, 9, 632. [Google Scholar] [CrossRef] [Green Version]
- Christensen, P.; Meinert Larsen, T.; Westerterp-Plantenga, M.; Macdonald, I.; Martinez, J.A.; Handjiev, S.; Poppitt, S.; Hansen, S.; Ritz, C.; Astrup, A.; et al. Men and women respond differently to rapid weight loss: Metabolic outcomes of a multi-centre intervention study after a low-energy diet in 2500 overweight, individuals with pre-diabetes (PREVIEW). Diabetes Obes. Metab. 2018, 20, 2840–2851. [Google Scholar] [CrossRef] [Green Version]
- Raben, A.; Vestentoft, P.S.; Brand-Miller, J.; Jalo, E.; Drummen, M.; Simpson, L.; Martinez, J.; Handjieva-Darlenska, T.; Stratton, G.; Huttunen-Lenz, M.; et al. PREVIEW-Results from a 3-year randomised 2 x 2 factorial multinational trial investigating the role of protein, glycemic index and physical activity for prevention of type-2 diabetes. Diabetes Obes. Metab. 2020, 23, 324–337. [Google Scholar] [CrossRef]
- Kahlert, D.; Unyi-Reicherz, A.; Stratton, G.; Meinert Larsen, T.; Fogelholm, M.; Raben, A.; Schlicht, W. PREVIEW behavior modification intervention toolbox (PREMIT): A study protocol for a psychological element of a multicenter project. Front. Psychol. 2016, 7, 1136. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes. Diabetes Care 2017, 40, S11–S24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, F.J.; Tan, M.; Ma, Y.; MacGregor, G.A. Salt Reduction to Prevent Hypertension and Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol 2020, 75, 632–647. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.E.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef]
- Peters, S.A.; Bots, M.L.; den Ruijter, H.M.; Palmer, M.K.; Grobbee, D.E.; Crouse III, J.R.; O’Leary, D.H.; Evans, G.W.; Raichlen, J.S.; Moons, K.G. Multiple imputation of missing repeated outcome measurements did not add to linear mixed-effects models. J. Clin. Epidemiol. 2012, 65, 686–695. [Google Scholar] [CrossRef]
- Twisk, J.; de Boer, M.; de Vente, W.; Heymans, M. Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J. Clin. Epidemiol. 2013, 66, 1022–1028. [Google Scholar] [CrossRef]
- Wang, F.; Zheng, J.; Yang, B.; Jiang, J.; Fu, Y.; Li, D. Effects of Vegetarian Diets on Blood Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2015, 4, e002408. [Google Scholar] [CrossRef] [Green Version]
- Satija, A.; Malik, V.; Rimm, E.B.; Sacks, F.; Willett, W.; Hu, F.B. Changes in intake of plant-based diets and weight change: Results from 3 prospective cohort studies. Am. J. Clin. Nutr. 2019, 110, 574–582. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Drouin-Chartier, J.P.; Li, Y.; Baden, M.Y.; Manson, J.E.; Willett, W.C.; Voortman, T.; Hu, F.B.; Bhupathiraju, S.N. Changes in Plant-Based Diet Indices and Subsequent Risk of Type 2 Diabetes in Women and Men: Three U.S. Prospective Cohorts. Diabetes Care 2021, 44, 663–671. [Google Scholar] [CrossRef]
- Glenn, A.J.; Lo, K.; Jenkins, D.J.A.; Boucher, B.A.; Hanley, A.J.; Kendall, C.W.C.; Manson, J.E.; Vitolins, M.Z.; Snetselaar, L.G.; Liu, S.; et al. Relationship Between a Plant-Based Dietary Portfolio and Risk of Cardiovascular Disease: Findings From the Women’s Health Initiative Prospective Cohort Study. J. Am. Heart Assoc. 2021, 10, e021515. [Google Scholar] [CrossRef]
- Zhu, R.; Larsen, T.M.; Fogelholm, M.; Poppitt, S.; Vestentoft, P.S.; Silvestre, M.P.; Jalo, E. Dose-dependent associations of dietary glycemic index, glycemic load and fiber with 3-year weight-loss maintenance and glycemic status in a high-risk population: A secondary analysis of the PREVIEW diabetes prevention study. Diabetes Care 2021, 44, 1672–1681. [Google Scholar] [CrossRef]
- Schlesinger, S.; Neuenschwander, M.; Schwedhelm, C.; Hoffmann, G.; Bechthold, A.; Boeing, H.; Schwingshackl, L. Food Groups and Risk of Overweight, Obesity, and Weight Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2019, 10, 205–218. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Li, X.; Yuan, S.; Jin, Y.; Lu, J. Nut consumption and risk of metabolic syndrome and overweight/obesity: A meta-analysis of prospective cohort studies and randomized trials. Nutr. Metab. 2018, 15, 46. [Google Scholar] [CrossRef] [Green Version]
- Eslami, O.; Shidfar, F.; Dehnad, A. Inverse association of long-term nut consumption with weight gain and risk of overweight/obesity: A systematic review. Nutr. Res. 2019, 68, 1–8. [Google Scholar] [CrossRef]
- Tindall, A.M.; Johnston, E.A.; Kris-Etherton, P.M.; Petersen, K.S. The effect of nuts on markers of glycemic control: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2019, 109, 297–314. [Google Scholar] [CrossRef]
- Ibarrola-Jurado, N.; Bulló, M.; Guasch-Ferré, M.; Ros, E.; Martínez-González, M.A.; Corella, D.; Fiol, M.; Wärnberg, J.; Estruch, R.; Román, P. Cross-sectional assessment of nut consumption and obesity, metabolic syndrome and other cardiometabolic risk factors: The PREDIMED study. PLoS ONE 2013, 8, e57367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEvoy, C.T.; Wallace, I.R.; Hamill, L.L.; Hunter, S.J.; Neville, C.E.; Patterson, C.C.; Woodside, J.V.; Young, I.S.; McKinley, M.C. Increasing fruit and vegetable intake has no dose-response effect on conventional cardiovascular risk factors in overweight adults at high risk of developing cardiovascular disease. J. Nutr. 2015, 145, 1464–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, S.; Petocz, P.; Duve, E.; Abbott, K.; Cassettari, T.; Blumfield, M.; Fayet-Moore, F. The Effect of Replacing Refined Grains with Whole Grains on Cardiovascular Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials with GRADE Clinical Recommendation. J. Acad. Nutr. Diet. 2020, 120, 1859–1883.E31. [Google Scholar] [CrossRef] [PubMed]
- Tieri, M.; Ghelfi, F.; Vitale, M.; Vetrani, C.; Marventano, S.; Lafranconi, A.; Godos, J.; Titta, L.; Gambera, A.; Alonzo, E.; et al. Whole grain consumption and human health: An umbArella review of observational studies. Int. J. Food Sci. Nutr. 2020, 71, 668–677. [Google Scholar] [CrossRef]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Musa-Veloso, K.; Poon, T.; Harkness, L.S.; O’Shea, M.; Chu, Y. The effects of whole-grain compared with refined wheat, rice, and rye on the postprandial blood glucose response: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2018, 108, 759–774. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.M.; Knuppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeghi, O.; Sadeghian, M.; Rahmani, S.; Maleki, V.; Larijani, B.; Esmaillzadeh, A. Whole-grain consumption does not affect obesity measures: An updated systematic review and meta-analysis of randomized clinical trials. Adv. Nutr. 2020, 11, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Ye, E.Q.; Chacko, S.A.; Chou, E.L.; Kugizaki, M.; Liu, S. Greater whole-grain intake is associated with lower risk of type 2 diabetes, cardiovascular disease, and weight gain. J. Nutr. 2012, 142, 1304–1313. [Google Scholar] [CrossRef]
- Park, Y.; Dodd, K.W.; Kipnis, V.; Thompson, F.E.; Potischman, N.; Schoeller, D.A.; Baer, D.J.; Midthune, D.; Troiano, R.P.; Bowles, H.; et al. Comparison of self-reported dietary intakes from the Automated Self-Administered 24-h recall, 4-d food records, and food-frequency questionnaires against recovery biomarkers. Am. J. Clin. Nutr. 2018, 107, 80–93. [Google Scholar] [CrossRef] [Green Version]
- Barnett, A.G.; Van Der Pols, J.C.; Dobson, A.J. Regression to the mean: What it is and how to deal with it. Int. J. Epidemiol. 2005, 34, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Capuano, V.; Marchese, F.; Capuano, R.; Torre, S.; Iannone, A.G.; Capuano, E.; Lamaida, N.; Sonderegger, M.; Capuano, E. Hyperuricemia as an independent risk factor for major cardiovascular events: A 10-year cohort study from Southern Italy. J. Cardiovasc. Med. 2017, 18, 159–164. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Groups | Foods | Plant-Based Diet Index |
|---|---|---|
| Plant | ||
| Grains | Bread rolls/baps/bagels, breads, cereal bars, cereal products, cereals, crackers/crispbreads, flours, grains, pastas, pastries/buns, rice, potatoes, potato products, pastry, plain cake, biscuits, and starch-based carbohydrate-rich snacks | Positive scores |
| Legumes | Pulses, beans, peas, lentils, and soy foods | Positive scores |
| Nuts | Nuts and seeds | Positive scores |
| Vegetables | leafy vegetables, dried vegetables, mushrooms, pickles/chutney, roots/tubers/bulbs, sea vegetables/algae, vegetable dishes, and avocado | Positive scores |
| Fruits | Fruits, canned fruit, and dried fruit | Positive scores |
| Animal | ||
| Dairy | Milk products, cow’s milk, cream, creams, drinking yogurts, milkshakes/smoothies, processed milk/powders, yogurts, chilled desserts, and cheeses | Negative scores |
| Eggs | Eggs, egg products, and egg dishes | Negative scores |
| Red meat | Beef, pork, lamb, organ meats, meat dishes, and meat products | Negative scores |
| Processed meat | Frankfurters, bacon, corned beef, sausage, cured ham, and luncheon meat made from beef, pork, and poultry | Negative scores |
| Poultry | Poultry and poultry products, chicken, turkey | Negative scores |
| Fish/seafood | Fatty fish, fish products, low-fat fish, canned fatty fish, canned low-fat fish, seafoods, and crustaceans, including lobster and shrimps | Negative scores |
| Characteristics | |
|---|---|
| n | 710 |
| Socio-demographics 1 | |
| Female, n (%) | 491 (69.2) |
| Age (years) | 57 (46, 63) |
| Height (m) | 1.66 (1.61, 1.73) |
| Ethnicity, n (%) | |
| Caucasian | 617 (86.9) |
| Asian | 24 (3.4) |
| Black | 19 (2.7) |
| Arabic | 4 (0.6) |
| Other | 46 (6.5) |
| Smoking, n (%) | |
| No | 659 (92.8) |
| Yes, but less than weekly | 17 (2.4) |
| Yes, at least daily | 30 (4.2) |
| Missing | 4 (0.6) |
| Anthropometric outcomes and body composition 2 | |
| Body weight (kg) | 86.1 ± 16.6 |
| BMI (kg·m−2) | 29.5 (26.7, 33.5) |
| Fat mass (kg) | 33.5 ± 12.3 |
| Waist circumference (cm) | 100.2 ± 12.6 |
| Cardiometabolic risk factors 2 | |
| Fasting plasma glucose (mmol·L−1) | 5.7 ± 0.6 |
| HbA1c (mmol·mol−1) | 35.0 ± 3.1 |
| HbA1c (%) | 5.4 ± 0.3 |
| Fasting insulin (mU·L−1) | 7.3 (5.3, 9.9) |
| HOMA-IR | 1.8 (1.3, 2.5) |
| Systolic blood pressure (mmHg) | 121.6 ± 15.8 |
| Diastolic blood pressure (mmHg) | 72.1 ± 9.5 |
| Triglycerides (mmol·L−1) | 1.0 (0.8, 1.2) |
| Total cholesterol (mmol·L−1) | 4.1 ± 0.9 |
| HDL cholesterol (mmol·L−1) | 1.1 ± 0.2 |
| LDL cholesterol (mmol·L−1) | 2.4 (1.9, 3.0) |
| Energy and food intake 3 | |
| Energy (kJ·day−1) | 29,491 ± 7731 |
| Grains (g·day−1) | 206.1 (144.7, 276.6) |
| Legumes (g·day−1) | 0.2 (0, 27.5) |
| Nuts (g·day−1) | 3.2 (0, 10.8) |
| Fruits (g·day−1) | 169.5 (83.8, 260.5) |
| Vegetables (g·day−1) | 185.9 (97.1, 310.7) |
| Dairy (g·day−1) | 361.0 (226.4, 501.0) |
| Eggs (g·day−1) | 20.8 (5.1, 41.3) |
| Red meat (g·day−1) | 35.9 (0, 71.9) |
| Processed meat (g·day−1) | 12.0 (0, 29.7) |
| Poultry (g·day−1) | 37.2 (9.6, 70.4) |
| Fish/seafood (g·day−1) | 30.0 (3.6, 62.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, R.; Fogelholm, M.; Poppitt, S.D.; Silvestre, M.P.; Møller, G.; Huttunen-Lenz, M.; Stratton, G.; Sundvall, J.; Råman, L.; Jalo, E.; et al. Adherence to a Plant-Based Diet and Consumption of Specific Plant Foods—Associations with 3-Year Weight-Loss Maintenance and Cardiometabolic Risk Factors: A Secondary Analysis of the PREVIEW Intervention Study. Nutrients 2021, 13, 3916. https://doi.org/10.3390/nu13113916
Zhu R, Fogelholm M, Poppitt SD, Silvestre MP, Møller G, Huttunen-Lenz M, Stratton G, Sundvall J, Råman L, Jalo E, et al. Adherence to a Plant-Based Diet and Consumption of Specific Plant Foods—Associations with 3-Year Weight-Loss Maintenance and Cardiometabolic Risk Factors: A Secondary Analysis of the PREVIEW Intervention Study. Nutrients. 2021; 13(11):3916. https://doi.org/10.3390/nu13113916
Chicago/Turabian StyleZhu, Ruixin, Mikael Fogelholm, Sally D. Poppitt, Marta P. Silvestre, Grith Møller, Maija Huttunen-Lenz, Gareth Stratton, Jouko Sundvall, Laura Råman, Elli Jalo, and et al. 2021. "Adherence to a Plant-Based Diet and Consumption of Specific Plant Foods—Associations with 3-Year Weight-Loss Maintenance and Cardiometabolic Risk Factors: A Secondary Analysis of the PREVIEW Intervention Study" Nutrients 13, no. 11: 3916. https://doi.org/10.3390/nu13113916
APA StyleZhu, R., Fogelholm, M., Poppitt, S. D., Silvestre, M. P., Møller, G., Huttunen-Lenz, M., Stratton, G., Sundvall, J., Råman, L., Jalo, E., Taylor, M. A., Macdonald, I. A., Handjiev, S., Handjieva-Darlenska, T., Martinez, J. A., Muirhead, R., Brand-Miller, J., & Raben, A. (2021). Adherence to a Plant-Based Diet and Consumption of Specific Plant Foods—Associations with 3-Year Weight-Loss Maintenance and Cardiometabolic Risk Factors: A Secondary Analysis of the PREVIEW Intervention Study. Nutrients, 13(11), 3916. https://doi.org/10.3390/nu13113916