
Protein Quality in Infant Formulas Marketed in Brazil: Assessments on Biodigestibility, Essential Amino Acid Content and Proteins of Biological Importance

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Sample Selection
2.2. Total Protein Contents
2.3. Protein Fraction Analysis
Sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE)
2.4. High-Performance Liquid Chromatography (HPLC)
2.5. Essential Amino Acid Identification
2.6. In Vitro Gastrointestinal Digestion Simulation
2.7. Gastric Phase Digestion (GPD)
2.8. Intestinal Phase Digestion (IPD)
2.9. In Vitro Protein Digestibility (IVPD) Assay
2.10. Amino Acid Score (AAS) and Protein Digestibility Corrected Amino Acid Score (PDCAAS)
2.11. Statistical Analyses
3. Results
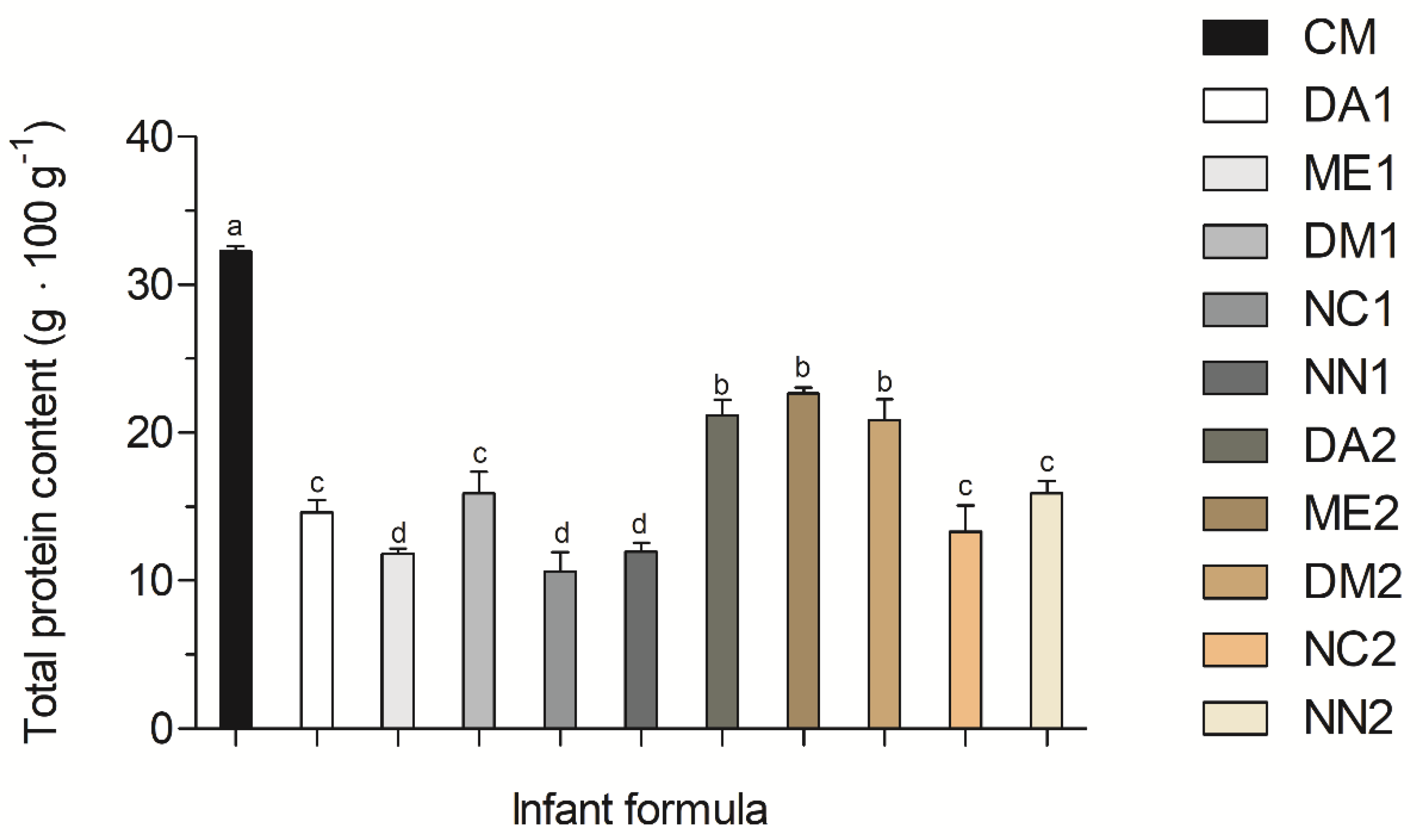
3.1. Crude Protein Contents
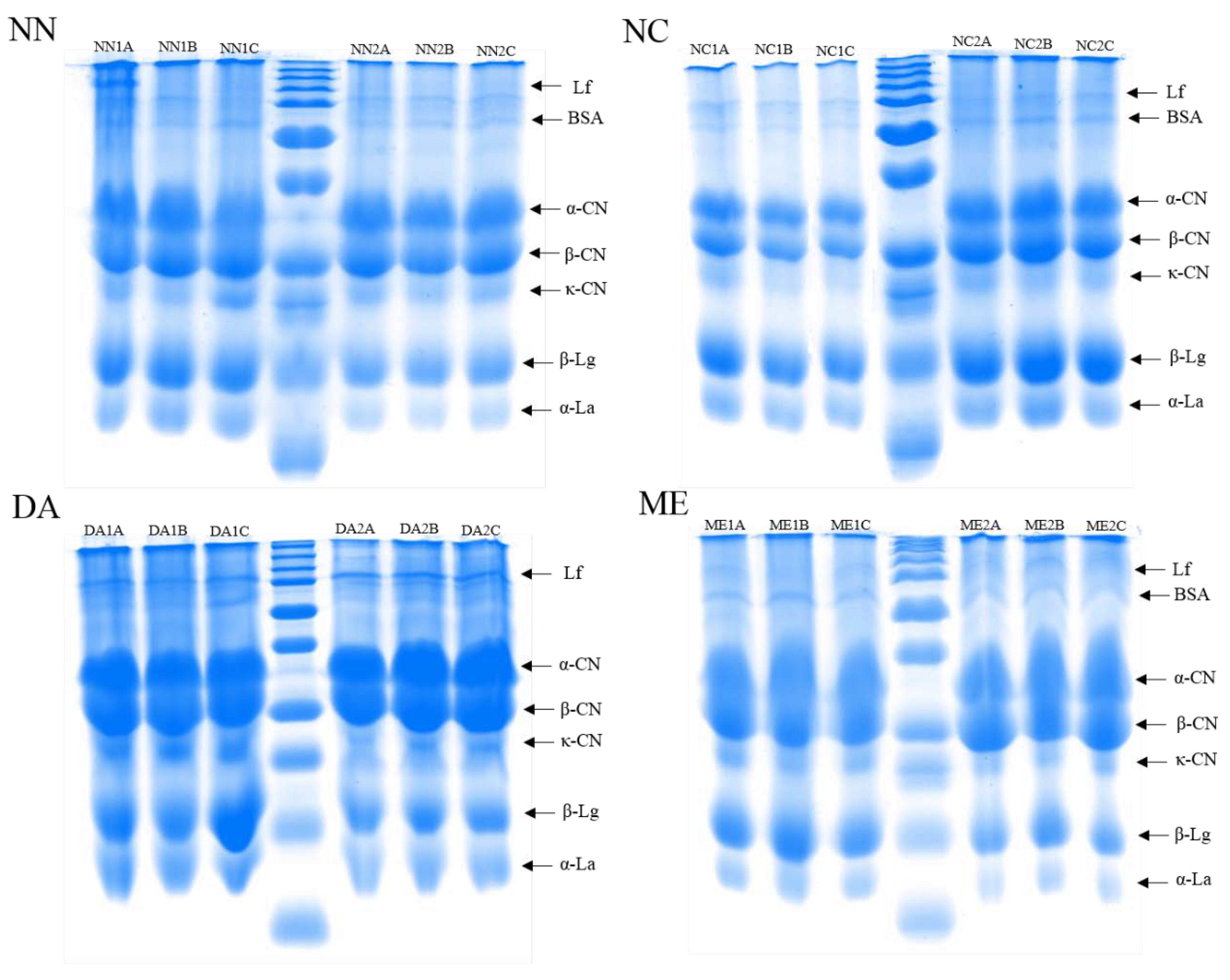
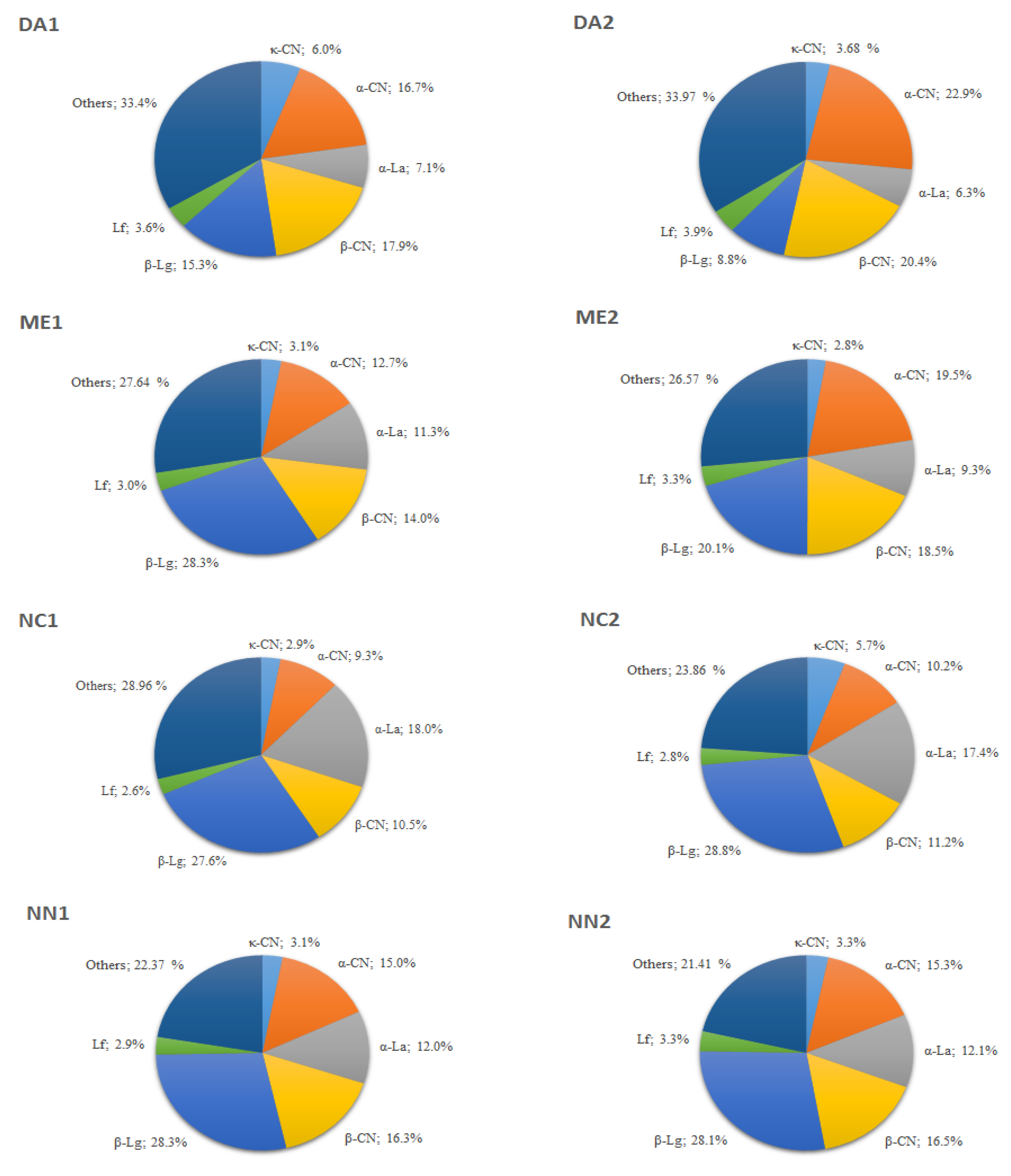
3.2. Protein Fractions Analysis
Protein Profiles and Relative Protein Abundance
3.3. Amino Acid Quantification in Phase 1 and Phase 2 IFs
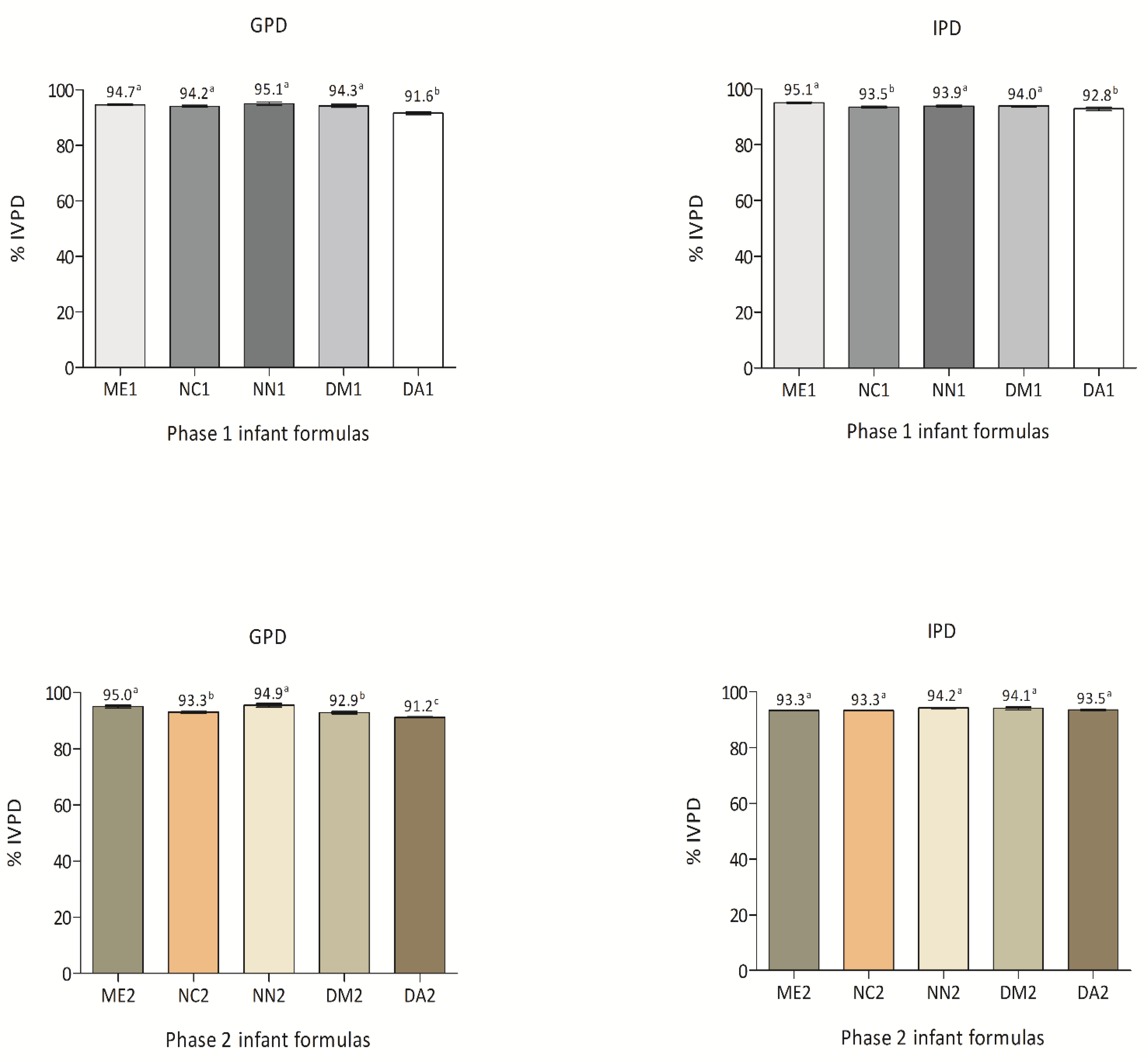
3.4. Phase 1 and Phase 2 IFs %IVPD
3.5. Phase 1 and Phase 2 IFs AAS and PDCAAS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koletzko, B.; Brands, B.; Chourdakis, M.; Cramer, S.; Grote, V.; Hellmuth, C.; Kirchberg, F.; Prell, C.; Rzehak, P.; Uhl, O.; et al. The power of programming and the early nutrition project: Opportunities for health promotion by nutrition during the first thousand days of life and beyond. Ann. Nutr. Metab. 2014, 64, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Uauy, R.; Kurpad, A.; Tano-Debrah, K.; Otoo, G.E.; Aaron, G.A.; Toride, Y.; Ghosh, S. Role of protein and amino acids in infant and young child nutrition: Protein and amino acid needs and relationship with child growth. J. Nutr. Sci. Vitaminol. 2015, 61, S192–S194. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization and United Nations Foundation. Global Strategy for Infant and Young Children; WHO: Geneva, Switzerland, 2003; Available online: https://apps.who.int/iris/bitstream/handle/10665/42590/9241562218.pdf?sequence=1 (accessed on 10 August 2021).
- American Dietetic Association. Position of the American ietetic Association: Breaking the barriers to breastfeeding. J. Am. Diet. Assoc. 2001, 101, 1213–1220. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Policy Statement: Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Sociedade Brasileira de Pediatria. Nutrição do lactente. In Manual de Alimentação: Orientações para Alimentação do Lactente ao Adolescente, na Escola, na Gestante, na Prevenção de Doenças e Segurança Alimentar, 4th ed.; Weffort, V.R.S., Oliveira, F.L.C., Ricco, R.C., Rocha, H.F., Mattos, A.P., Lopez, F.A., Eds.; SBP: São Paulo, Brasil, 2018; pp. 13–49. [Google Scholar]
- CODEX Alimentarius. Standard for Infant Formula and Formulas for Special Medical Purposes Intended for Infants; Amendment: 1983, 1985, 1987, 2011, 2015 and 2016. Revision: 2007; CODEX STAN 72-1981; Codex-Alimentarius-Commission: Rome, Italy; Available online: http://www.fao.org/fao-who-codexalimentarius/sh-proxy/en/?lnk=1&url=https%253A%252F%252Fworkspace.fao.org%252Fsites%252Fcodex%252FStandards%252FCXS%2B72-1981%252FCXS_072e.pdf (accessed on 13 September 2021).
- Martin, C.R.; Ling, P.R.; Blackburn, G.L. Review of infant feeding: Key features of breast milk and infant formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.; Grote, V.; Closa-Monasterolo, R.; Escribano, J.; Langhendries, J.P.; Dain, E.; Giovannini, M.; Verduci, E.; Gruszfeld, D.; Socha, P.; et al. European Childhood Obesity Trial Study Group. Lower protein content in infant formula reduces BMI and obesity risk at school age: Follow-up of a randomized trial. Am. J. Clin. Nutr. 2014, 99, 1041–1051. [Google Scholar] [CrossRef]
- Agostoni, C.; Decsi, T.; Fewtrell, M.; Goulet, O.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Moreno, L.; Puntis, J.; Rigo, J.; et al. ESPGHAN Committee on Nutrition. Complementary feeding: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Michaelsen, K.F.; Greer, F. Protein needs early in life and long-term health. Am. J. Clin. Nutr. 2014, 99, 718S–722S. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S. Protein quality in the first thousand days of life. Food Nutr. Bull. 2016, 37, S14–S21. [Google Scholar] [CrossRef] [Green Version]
- Oropeza-Ceja, L.G.; Rosado, J.L.; Ronquillo, D.; García, O.P.; Caamaño, M.; García-Ugalde, C.; Viveros-Contreras, R.; Duarte-Vázquez, M.Á. Lower protein intake supports normal growth of full-term infants fed formula: A randomized controlled trial. Nutrients 2018, 10, 886. [Google Scholar] [CrossRef] [Green Version]
- AOAC. Association of Official Analytical Chemists. In Official Methods of Analysis of the Association of Official Analytical Chemist, 19th ed.; AOAC International: Gaithersburg, MD, USA, 2012; Volume 12. [Google Scholar]
- Conte-Junior, C.A.; Golinelli, L.P.; Paschoalin, V.M.; Silva, J.T. Desarrollo de la Tecnica de Fraccionamiento de Proteinas Presentes en el Suero del Calostro por Electroforesis Bidimensional para su Identificacion por Espectrometria de Masa (MALDI-TOF). Alimentaria 2006, 373, 120–121. Available online: https://www.scielo.br/j/babt/a/YTyws7brhQc7LtNdgqjr9bf/?format=pdf&lang=en (accessed on 3 August 2021).
- Almeida, C.C.; Alvares, T.S.; Costa, M.P.; Conte-Junior, C.A. Protein and amino acid profiles of different whey protein supplements. J. Diet. Suppl. 2015, 13, 313–323. [Google Scholar] [CrossRef]
- Bobe, G.; Beitz, D.C.; Freeman, A.E.; Lindberg, G.L. Separation and quantification of bovine milk proteins by reversed-phase high performance liquid chromatography. J. Agric. Food Chem. 1998, 46, 458–463. [Google Scholar] [CrossRef]
- Bonfatti, V.; Grigoletto, L.; Cecchinato, A.; Gallo, L.; Carnier, P. Validation of a new reversed-phase high-performance liquid chromatography method for separation and quantification of bovine milk protein genetic variants. J. Chromatogr. A. 2008, 1195, 101–106. [Google Scholar] [CrossRef]
- Duchén, K.; Casas, R.; Fagerås-böttcher, M.; Yu, G.; Björkstén, B. Human milk polyunsaturated long-chain fatty acids and secretory immunoglobulin A antibodies and early childhood allergy. Pediatr. Allergy Immunol. 2000, 11, 29–39. [Google Scholar] [CrossRef]
- Furota, S.; Ogawa, N.O.; Takano, Y.; Yoshimura, T.; Ohkouchi, N. Quantitative analysis of underivatized amino acids in the sub- to several-nanomolar range by ion-pair HPLC using a corona-charged aerosol detector (HPLC–CAD). J. Chromatogr. B. 2018, 1095, 191–197. [Google Scholar] [CrossRef]
- Oomen, A.G.; Rompelberg, C.J.; Bruil, M.A.; Dobbe, C.J.; Pereboom, D.P.; Sips, A.J. Development of an in vitro digestion model for estimating the bioaccessibility of soil contaminants. Arch. Environ. Contam. Toxicol. 2003, 44, 281–287. [Google Scholar] [CrossRef]
- Sagratini, G.; Caprioli, G.; Maggi, F.; Font, G.; Giardinà, D.; Mañes, J.; Meca, G.; Ricciutelli, M.; Sirocchi, V.; Torregiani, E.; et al. Determination of soya saponins I and βg in raw and cooked legumes by solid phase extraction (SPE) coupled to liquid chromatography (LC)-mass spectrometry (MS) and assessment of their bioaccessibility by an in vitro digestion model. J. Agric. Food Chem. 2013, 61, 1702–1709. [Google Scholar] [CrossRef]
- World Health Organization. Joint WHO/FAO/UNU Expert Consultation on Protein and Amino Acid Requirements in Human Nutrition. In World Health Organization Technical Report Series; World Health Organization: Geneva, Switzerland, 2007; Volume 935, 265p, Available online: https://apps.who.int/iris/handle/10665/43411 (accessed on 11 September 2021).
- Prentice, P.; Ong, K.K.; Schoemaker, M.H.; Tol, E.A.; Vervoort, J.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Breast milk nutrient content and infancy growth. Acta Paediatr. 2016, 105, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Rêgo, C.; Pereira-da-silva, L.; Ferreira, R. Consenso sobre fórmulas infantis: A opinião dos especialistas portugueses sobre sua composição e suas indicações. Acta Pediatr. 2018, 31, 754–765. [Google Scholar] [CrossRef]
- Donovan, S.M. Human milk proteins: Composition and physiological significance. In Human Milk: Composition, Clinical Benefits and Future Opportunities, 90th Nestlé Nutrition Institute Workshop; Donovan, S.M., German, J.B., Lönnerdal, B., Lucas, A., Eds.; Karger: Lausanne, Switzerland, 2019; Volume 90, pp. 93–101. [Google Scholar] [CrossRef] [Green Version]
- BRASIL. Agência Nacional de Vigilância Sanitária. Resolução RDC n° 43, de 19 de Setembro de 2011. Dispõe Sobre o Regulamento Técnico para Fórmulas Infantis para Lactentes. 2011. Available online: http://www.ibfan.org.br/site/wp-content/uploads/2014/06/Resolucao_RDC_n_43_de_19_de_setembro_de_2011.pdf (accessed on 26 July 2021).
- BRASIL. Agência Nacional de Vigilância Sanitária. Resolução RDC n° 44, de 19 de Setembro de 2011. Dispõe Sobre o Regulamento Técnico para Fórmulas Infantis de Seguimento para Lactentes e Crianças de Primeira Infância. 2011. Available online: https://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2011/res0042_19_09_2011.html (accessed on 26 July 2021).
- U.S. Food and Drug Administration Guidance for Industry. Demonstration of the Quality Factor Reguirements under 21 CFR 106.96 (i) for “Eligible Infant Formulas”. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=106.96 (accessed on 27 July 2021).
- Gonçalves, N.A.; Cecchi, P.P.; Vieira, R.M.; Santos, M.D.A.; Almeida, T.C. Rotulagem de alimentos e consumidor. Nutr. Brasil. 2015, 14, 1–8. [Google Scholar] [CrossRef]
- BRASIL. Agência Nacional de Vigilância Sanitária. Aprova o Regulamento Técnico sobre Rotulagem Nutricional de Alimentos Embalados, Tornando Obrigatória a Rotulagem; RDC n° 360, de 23 de Dezembro de 2003; Diário Oficial [da] República Federativa do Brasil: Brasília, Brasil, 2003; pp. 33–34. Available online: https://www.gov.br/agricultura/pt-br/assuntos/inspecao/produtos-vegetal/legislacao-1/biblioteca-de-normas-vinhos-e-bebidas/resolucao-rdc-no-360-de-23-de-dezembro-de-2003.pdf (accessed on 26 July 2021).
- Escribano, J.; Luque, V.; Ferre, N.; Zaragoza-Jordana, M.; Grote, V.; Koletzko, B.; Gruszfeld, D.; Socha, P.; Dain, E.; Van Hees, J.N.; et al. Increased protein intake augments kidney volume and function in healthy infants. Kidney Int. 2011, 79, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, I.M.; Main, K.M.; Damgaard, I.N.; Mau, C.; Haavisto, A.M.; Chellakooty, M.; Boisen, K.A.; Petersen, J.H.; Scheike, T.; Olgaard, K. Kidney growth in 717 healthy children aged 0–18 months: A longitudinal cohort study. Pediatr. Nephrol. 2004, 19, 992–1003. [Google Scholar] [CrossRef]
- Lifschitz, C. Early life factors influencing the risk of obesity. Pediatr. Gastroenterol. Hepatol. Nutr. 2015, 8, 217–223. [Google Scholar] [CrossRef] [Green Version]
- Koletzko, B.; von Kries, R.; Closa, R.; Escribano, J.; Scaglioni, S.; Giovannini, M.; Beyer, J.; Demmelmair, H.; Gruszfeld, D.; Dobrzanska, A.; et al. Lower protein in infant formula is associated with lower weight up to age 2 years: A randomized clinical trial. Am. J. Clin. Nutr. 2009, 89, 1836–1845. [Google Scholar] [CrossRef] [Green Version]
- Michaelsen, K.; Hoppe, C.; Mølgaard, C. Effect of early protein intake on linear growth velocity and development of adiposity. Monatsschrift Kinderheilkunde 2003, 151, S78–S83. [Google Scholar] [CrossRef]
- Gruszfeld, D.; Socha, P. Early nutrition and health: Short- and long-term outcomes. World Rev. Nutr. Diet. 2013, 108, 32–39. [Google Scholar] [CrossRef]
- Alexander, B.T. Fetal programming of hypertension. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 290, R1–R10. [Google Scholar] [CrossRef]
- Drougia, A.; Giapros, V.; Hotoura, E.; Papadopoulou, F.; Argyropoulou, M.; Andronikou, S. The effects of gestational age and growth restriction on compensatory kidney growth. Nephrol. Dial. Transplant. 2009, 24, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.J.; O’Mara, F. Nutritional manipulation of milk protein concentration and its impact on the dairy industry. Livest. Prod. Sci. 1993, 35, 117–134. [Google Scholar] [CrossRef]
- Walstra, P.; Wouters, J.T.M.; Geurts, T.J. Dairy Science and Technology, 2nd ed.; CRC: New York, NY, USA, 2005; pp. 166–167. [Google Scholar]
- Onwulata, C.I.; Konstance, R.P.; Tomasula, P.M. Minimizing variations in functionality of whey protein concentrates from different sources. J. Dairy Sci. 2004, 87, 749–756. [Google Scholar] [CrossRef] [Green Version]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M.; Food and Nutrition Board of the Institute of Medicine, The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Cavaletto, M.; Giuffrida, M.G.; Conti, A. Milk fat globule membrane components: A proteomic approach. In Bioactive Components of Milk, 2008th ed.; Springer: New York, NY, USA, 2008; Volume 606, pp. 129–141. [Google Scholar]
- Cao, X.; Han, Y.; Li, F.; Li, Z.; McClements, D.J.; He, L.; Decker, E.A.; Xing, B.; Xiao, H. Impact of protein-nanoparticle interactions on gastrointestinal fate of ingested nanoparticles: Not just simple protein corona effects. NanoImpact 2019, 13, 37–43. [Google Scholar] [CrossRef]
- Manoni, M.; DI Lorenzo, C.; Ottoboni, M.; Tretola, M.; Pinotti, L. Comparative proteomics of milk fat globule membrane (MFGM) proteome across species and lactation stages and the potentials of MFGM fractions in infant formula preparation. Foods 2020, 9, 1251. [Google Scholar] [CrossRef]
- Sousa, R.; Portmann, R.; Dubois, S.; Recio, I.; Egger, L. Protein digestion of different protein sources using the INFOGEST static digestion model. Food Res. Int. 2020, 130, 108996. [Google Scholar] [CrossRef]
- Nucci, A.M.; Virtanen, S.M.; Becker, D.J. Infant feeding and timing of complementary foods in the development of type 1 diabetes. Curr. Diab. Rep. 2015, 15, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gridneva, Z.; Kugananthan, S.; Hepworth, A.; Tie, W.; Lai, C.; Ward, L.; Hartmann, P.E.; Geddes, D. Effect of Human Milk Appetite Hormones, Macronutrients, and Infant Characteristics on Gastric Emptying and Breastfeeding Patterns of Term Fully Breastfed Infants. Nutrients 2016, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Livney, Y.D. Milk proteins as vehicles for bioactives. Curr. Opin. Colloid In. 2010, 15, 73–83. [Google Scholar] [CrossRef]
- Guo, M. Manufacturing Technology. In Human Milk Biochemistry and Infant Formula; Elsevier: Cambrdige, UK, 2014. [Google Scholar]
- Vincenzetti, S.; Pucciarelli, S.; Polzonetti, V.; Polidori, P. Role of Proteins and of some bioactive peptides on the nutritional quality of donkey milk and their impact on human health. Beverages 2017, 3, 34. [Google Scholar] [CrossRef]
- Le, T.T.; Deeth, H.C.; Larsen, L.B. Proteomics of major bovine milk proteins: Novel insights. Int. Dairy J. 2017, 67, 2–15. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Adelman, A.S.; Rai, D.; Boettcher, J.; Lönnerdal, B. Amino acid profiles in term and preterm human milk through lactation: A systematic review. Nutrients 2013, 5, 4800–4821. [Google Scholar] [CrossRef] [Green Version]
- Echarri, P.P.; Bermudez, C.A.G.; Morillas, V.M.M.I.; Santaella, M.; Ros, G.; Saseta, F.C.; Graciá, C.M. α-Lactalbumin as an ingredient of infant formula. Arch. Latinoam. Nutr. 2012, 62, 6–14. Available online: http://ve.scielo.org/pdf/alan/v62n1/art02.pdf (accessed on 10 September 2021).
- Crowley, S.V.; Dowling, A.P.; Caldeo, V.; Kelly, A.L.; O’Mahony, A. Impact of α-lactalbumin: β-lactoglobulin ratio on the heat stability of model infant milk formula protein systems. Food Chem. 2016, 194, 184–190. [Google Scholar] [CrossRef]
- Kaiser, G.G.; Mucci, N.C.; González, V.; Sánchez, L.; Parrón, J.A.; Pérez, M.D.; Calvo, M.; Aller, J.F.; Hozbor, F.A.; Mutto, A.A. Detection of recombinant human lactoferrin and lysozyme produced in a bitransgenic cow. J. Dairy Sci. 2017, 100, 1605–1617. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Sharma, R.; Rajput, Y.S.; Mann, B.; Gandhi, K. Distinction between glycomacropeptide and β-lactoglobulin with “stains all” dye on Tricine SDS-PAGE gels. Food Chem. 2020, 340, 127923. [Google Scholar] [CrossRef]
- Keith, J.N. Lactose intolerance and milk protein allergy. Curr. Treat. Options Gastro. 2020, 18, 1–14. [Google Scholar] [CrossRef]
- Rangel, A.H.N.; Sales, D.C.; Urbano, S.A.; Galvão Júnior, J.G.B.; Andrade Neto, J.C.; Macêdo, C.S. Lactose intolerance and cow’s milk protein allergy. Food Sci. Technol. 2016, 36, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Chia, J.S.J.; McRae, J.L.; Kukuljan, S.; Woodford, K.; Elliott, R.B.; Swinburn, B.; Dwyer, K.M. A1 beta-casein milk protein and other environmental pre-disposing factors for type 1 diabetes. Nutr. Diabetes 2017, 7, e274. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority. Review of the potential health impact of β-casomorphins and related peptides: Review of the potential health impact of β-casomorphins and related peptides. EFSA Sci. Rep. 2009, 231, 1–107. [Google Scholar] [CrossRef]
- Sharma, N.; Sharma, R.; Rajput, Y.S.; Mann, B.; Singh, R.; Gandhi, K. Separation methods for milk proteins on polyacrylamide gel electrophoresis: Critical analysis and options for better resolution. Int. Dairy. J. 2021, 114, 104920. [Google Scholar] [CrossRef]
- Qian, F.; Sun, J.; Cao, D.; Tuo, Y.; Jiang, S.; Mu, G. Experimental and modelling study of the denaturation of milk protein by heat treatment. Korean J. Food Sci. Anim. Resour. 2017, 37, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Lönnerdal, B. Bioactive proteins in human milk: Health, nutrition, and implications for infant formulas. J. Pediatr. 2016, 173, S4–S9. [Google Scholar] [CrossRef] [Green Version]
- Golkar, A.; Milani, J.M.; Vasiljevic, T. Altering allergenicity of cow’s milk by food processing for applications in infant formula. Crit. Rev. Food Sci. Nutr. 2019, 59, 159–172. [Google Scholar] [CrossRef]
- Golinelli, L.P.; Del-Aguiar, E.M.; Paschoalin, V.M.F.; Silva, J.T.; Conte-Junior, C.A. Functional aspect of colostrum and whey proteins in human milk. J. Hum. Nutr. Food Sci. 2014, 2, 1–9. Available online: https://www.jscimedcentral.com/Nutrition/nutrition-2-1035.pdf (accessed on 16 August 2021).
- Alegría, A.; Barberá, R.; Farré, R.; Lagarda, M.J.; López, J.C. Amino acid contents of infant formulas. J. Food Compos. Anal. 1999, 12, 137–146. [Google Scholar] [CrossRef]
- Hall, W.L.; Millward, D.J.; Long, S.J.; Morgan, L.M. Casein and whey exert different effects on plasma amino acid profiles, gastrointestinal hormone secretion and appetite. Br. J. Nutr. 2003, 89, 239–248. [Google Scholar] [CrossRef]
- Lönnerdal, B. Infant formula and infant nutrition: Bioactive proteins of human milk and implications for composition of infant formulas. Am. J. Clin. Nutr. 2014, 99, 712S–717S. [Google Scholar] [CrossRef] [Green Version]
- Carbonell-Capella, J.M.; Buniowska, M.; Barba, F.J.; Esteve, M.J.; Frígola, A. Analytical methods for determining bioavailability and bioaccessibility of bioactive compounds from fruits and vegetables: A Review. Compreh. Rev. Food Sci. Food Saf. 2014, 13, 154–171. [Google Scholar] [CrossRef] [PubMed]
- Butts, C.A.; Monro, J.A.; Moughan, P.J. In vitro determination of dietary protein and amino acid digestibility for humans. Br. J. Nutr. 2012, 108, S282–S287. [Google Scholar] [CrossRef] [Green Version]
- Balthazar, C.F.; Pimentel, T.C.; Ferrao, L.L.; Almada, C.N.; Santillo, A.; Albenzio, M.; Mollakhalili, N.; Mortazavian, A.M.; Nascimento, J.S.; Silva, M.C.; et al. Sheep Milk: Physicochemical characteristics and relevance for functional food development. Compreh. Rev. Food Sci. Food Saf. 2017, 16, 247–262. [Google Scholar] [CrossRef]
- Lacroix, M.; Bos, C.; Léonil, J.; Airinei, G.; Luengo, C.; Daré, S.; Benamouzig, R.; Fouillet, H.; Fauquant, J.; Tomé, D.; et al. Compared with casein or total milk protein, digestion of milk soluble proteins is too rapid to sustain the anabolic postprandial amino acid requirement. Am. J. Clin. Nutr. 2006, 84, 1070–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maathuis, A.; Havenaar, R.; He, T.; Bellmann, S. Digestão de proteínas e qualidade de fórmulas infantis de leite de cabra e vaca e leite humano em condições simuladas de bebês. J. Ped. Gastroenterol. Nutr. 2017, 65, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Millward, D.J.; Layman, D.K.; Tomé, D.; Schaafsma, G. Protein quality assessment: Impact of expanding understanding of protein and amino acid needs for optimal health. Am. J. Clin. Nut. 2008, 87, 1576–1581. [Google Scholar] [CrossRef] [PubMed]
- Lien, E.L. Infant formulas with increased concentrations of α-lactalbumin. Am. J. Clin. Nutr. 2003, 77, 1555S–1558S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandström, O.; Lönnerdal, B.; Graverholt, G.; Hernell, O. Effects of alpha-lactalbumin enriched formula containing different concentrations of glycomacropeptide on infant nutrition. Am. J. Clin. Nutr. 2008, 87, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Trabulsi, J.; Capeding, R.; Lebumfacil, J.; Ramanujam, K.; Feng, P.; McSweeney, S.; Harris, B.; DeRusso, P. Effect of an α-lactalbumin-enriched infant formula with lower protein on growth. Eur. J. Clin. Nutr. 2011, 65, 167–174. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infant Formulas | Major Proteins (mg·g−1) | |||||
|---|---|---|---|---|---|---|
| Lf | α-CN | β-CN | κ-CN | β-Lg | α-La | |
| CM | 0.31 ± 0.02 e | 43.26 ± 0.30 a | 57.95 ± 0.50 a | 125.14 ± 0.39 a | 56.62 ± 0.41 a | 3.53 ± 0.13 c |
| Phase 1 | ||||||
| ME1 | 1.37 ± 0.15 b | 14.77 ± 2.02 d,e | 7.96 ± 0.55 f | 100.50 ± 0.37 d | 22.20 ± 1.35 d,e | 0.33 ± 0.05 f |
| NC1 | 0.57 ± 0.27 d | 21.17 ± 2.74 b | 11.13 ± 0.90 d | 89.90 ± 4.08 e | 19.37 ± 1.76 e | 12.10 ± 1.21 a |
| NN1 | 0.85 ± 0.04 c | 7.60 ± 0.17 g | 11.61 ± 0.01 d | 124.50 ± 3.37 a | 39.83 ± 1.79 b | 13.23 ± 0.41 a |
| DM1 | 1.37 ± 0.10 b | 11.17 ± 0.57 f | 25.16 ± 3.37 b,c | 100.23 ± 0.37 d | 15.77 ± 1.66 f | 3.93 ± 0.89 c,d |
| DA1 | 1.13 ± 0.15 b | 12.57 ± 1.53 e,f | 7.76 ± 0.31 f | 106.53 ± 2.72 c | 14.10 ± 2.30 f | 3.40 ± 1.82 c,d |
| Phase 2 | ||||||
| ME2 | 0.87 ± 0.07 c | 18.50 ± 0.81 c | 5.63 ± 1.06 g | 127.1 ± 3.90 a | 26.27 ± 3.17 c,d | 0.57 ± 0.11 f |
| NC2 | 0.40 ± 0.11 e | 13.37 ± 1.12 d,e | 10.6 ± 0.11 e | 88.17 ± 7.85 e | 17.7 ± 1.75 e,f | 7.57 ± 0.45 b |
| NN2 | 0.67 ± 0.15 c,d | 7.23 ± 0.21 g | 22.23 ± 3.62 c | 115.53 ± 2.21 b | 32.61 ± 3.91 c | 11.97 ± 0.87 a |
| DM2 | 0.71 ± 0.20 c,d | 13.51 ± 0.88 d,e | 28.7 ± 3.96 b | 103.47 ± 3.03 c,d | 18.70 ± 2.66 e,f | 2.10 ± 1.12 d |
| DA2 | 3.80 ± 3.01 a | 14.71 ± 2.55 d,e | 9.03 ± 1.10 f | 107.17 ± 1.14 c | 17.90 ± 2.08 e,f | 1.07 ± 0.11 e |
| Infant Formulas | Major Proteins (mg·g−1) | |||||
|---|---|---|---|---|---|---|
| Lf | α-CN | β-CN | κ-CN | β-Lg | α-La | |
| Phase 1 | ||||||
| ME1A | 1.51 ± 0.15 a | 16.62 ± 0.11 a | 7.62 ± 0.11 b | 100.21 ± 0.27 b | 20.61 ± 0.15 b | 0.31 ± 0.21 a |
| ME1B | 1.45 ± 0.11 a,b | 12.62 ± 0.22 c | 8.63 ± 0.21 a | 100.36 ± 0.27 b | 22.92 ± 0.15 a | 0.41 ± 0.11 a |
| ME1C | 1.21 ± 0.21 b | 15.11 ± 0.13 b | 7.75 ± 0.17 b | 100.95 ± 0.17 a | 23.02 ± 0.34 a | 0.39 ± 0.11 a |
| NC1A | 0.19 ± 0.17 a | 22.83 ± 0.15 a | 10.14 ± 0.27 b | 94.87 ± 0.29 a | 21.43 ± 0.11 a | 13.41 ± 0.23 a |
| NC1B | 0.22 ± 0.15 a | 18.02 ± 0.45 b | 11.57 ± 0.65 a | 86.07 ± 0.19 c | 18.45 ± 0.31 b | 11.42 ± 0.43 b |
| NC1C | 0.41 ± 0.26 a | 22.72 ± 0.54 a | 11.84 ± 0.46 a | 88.94 ± 0.48 b | 18.35 ± 0.41 b | 11.29 ± 0.22 b |
| NN1A | 0.73 ± 0.21 a | 7.82 ± 0.10 a | 11.65 ± 0.43 a | 121.25 ± 0.72 c | 41.94 ± 0.42 a | 13.18 ± 0.12 b |
| NN1B | 0.88 ± 0.32 a | 7.51 ± 0.12 b | 11.56 ± 0.22 a | 129.85 ± 0.42 a | 38.76 ± 0.21 b | 13.76 ± 0.32 a |
| NN1C | 0.99 ± 0.12 a | 7.54 ± 0.12 b | 11.76 ± 0.49 a | 122.55 ± 0.83 b | 38.97 ± 0.12 b | 12.95 ± 0.11 b |
| DM1A | 1.42 ± 0.15 a | 10.57 ± 0.53 b | 27.38 ± 0.34 b | 99.87 ± 0.11 b | 14.08 ± 0.42 c | 4.41 ± 0.19 a |
| DM1B | 1.43 ± 0.11 a | 11.56 ± 0.14 a | 29.19 ± 0.55 a | 100.57 ± 0.11 a | 16.09 ± 0.12 b | 4.51 ± 0.39 a |
| DM1C | 1.39 ± 0.13 a | 11.53 ± 0.23 a | 19.19 ± 0.91 c | 100.44 ± 0.31 a | 17.39 ± 0.83 a | 2.93 ± 0.26 b |
| DA1A | 1.33 ± 0.21 a | 13.55 ± 0.11 a | 7.54 ± 0.43 a | 108.33 ± 0.21 a | 13.25 ± 0.12 b | 2.21 ± 0.25 b |
| DA1B | 1.15 ± 0.12 a | 13.41 ± 0.21 a | 8.15 ± 0.25 a | 103.42 ± 0.21 b | 15.66 ± 0.13 a | 2.54 ± 0.15 b |
| DA1C | 1.01 ± 0.28 a | 10.81 ± 0.11 b | 7.74 ± 0.21 a | 107.98 ± 0.13 a | 13.52 ± 0.33 b | 5.54 ± 0.14 a |
| Phase 2 | ||||||
| ME2A | 1.06 ± 0.11 a | 19.22 ± 0.14 a | 6.81 ± 0.21 a | 129.09 ± 0.14 b | 22.63 ± 0.27 b | 0.58 ± 0.15 a |
| ME2B | 0.88 ± 0.22 a | 17.63 ± 0.12 c | 4.72 ± 0.11 c | 129.59 ± 0.14 a | 28.03 ± 0.18 a | 0.51 ± 0.15 a |
| ME2C | 0.87 ± 0.28 a | 18.77 ± 0.28 b | 5.42 ± 0.18 b | 122.56 ± 0.25 c | 28.24 ± 0.18 a | 0.76 ± 0.13 a |
| NC2A | 0.57 ± 0.19 a | 13.36 ± 0.26 b | 10.76 ± 0.14 a | 82.97 ± 0.41 c | 17.74 ± 0.29 b | 8.06 ± 0.24 a |
| NC2B | 0.39 ± 0.37 a | 12.45 ± 0.17 c | 10.54 ± 0.45 a | 97.25 ± 0.22 a | 19.35 ± 0.15 a | 7.66 ± 0.23 a |
| NC2C | 0.42 ± 0.14 a | 14.46 ± 0.63 a | 10.71 ± 0.15 a | 84.47 ± 0.23 b | 15.86 ± 0.16 c | 7.15 ± 0.24 b |
| NN2A | 0.61 ± 0.16 a | 7.09 ± 0.24 b | 25.61 ± 0.17 a | 113.17 ± 0.21 c | 28.54 ± 0.54 c | 12.57 ± 0.11 a |
| NN2B | 0.71 ± 0.15 a | 7.39 ± 0.25 a,b | 22.71 ± 0.28 b | 116.12 ± 0.43 b | 33.01 ± 0.11 b | 11.68 ± 0.21 b |
| NN2C | 0.73 ± 0.19 a | 7.47 ± 0.14 a | 18.41 ± 0.63 c | 117.43 ± 0.33 a | 36.32 ± 0.72 a | 11.83 ± 0.11 b |
| DM2A | 0.92 ± 0.17 a | 14.24 ± 0.26 a | 25.40 ± 0.23 c | 109.33 ± 0.15 a | 21.53 ± 0.51 a | 2.82 ± 0.22 a |
| DM2B | 0.94 ± 0.77 a | 13.81 ± 0.56 b | 27.62 ± 0.36 b | 100.96 ± 0.35 b | 18.46 ± 0.14 b | 2.71 ± 0.33 a |
| DM2C | 0.28 ± 0.21 b | 12.53 ± 0.14 c | 33.10 ± 0.39 a | 100.25 ± 0.14 c | 16.26 ± 0.24 c | 0.82 ± 0.52 b |
| DA2A | 8.55 ± 0.41 a | 12.51 ± 0.18 b | 7.93 ± 0.11 c | 108.54 ± 0.24 a | 19.37 ± 0.13 a | 1.02 ± 0.21 a |
| DA2B | 1.54 ± 0.21 b | 17.52 ± 0.25 a | 9.15 ± 0.12 b | 107.34 ± 0.11 b | 18.98 ± 0.15 b | 1.29 ± 0.11 a |
| DA2C | 1.44 ± 0.21 b | 14.11 ± 0.22 c | 10.13 ± 0.22 a | 105.74 ± 0.32 c | 15.59 ± 0.36 c | 1.09 ± 0.11 a |
| Reference | Infant Formulas | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Phase 1 (mg·g−1) | Phase 2 (mg·g−1) | ||||||||||
| Amino Acids | FAO/WHO (mg·g of Protein−1) * | ME1 | NC1 | NN1 | DM1 | DA1 | ME2 | NC2 | NN2 | DM2 | DA2 |
| Threonine | 31 | 3.93 ± 0.02 c,E | 3.08 ± 0.03 e,I | 3.18 ± 0.01 d,H | 4.19 ± 0.02 b,C | 4.34 ± 0.01 a,B | 4.07 ± 0.02 b,D | 3.24 ± 0.01 d,G | 3.04 ± 0.02 e,I | 4.70 ± 0.02 a,A | 3.72 ± 0.02 c,F |
| Lysine | 57 | 0.20 ± 0.04 a,A,B | 0.20 ± 0.03 a,A,B | 0.26 ± 0.03 a,A | 0.15 ± 0.01 b,C | 0.14 ± 0.01 b,C | 0.16 ± 0.01 b,C | 0.19 ± 0.01 a,B | 0.10 ± 0.01 c,D | 0.19 ± 0.01 a,B | 0.15 ± 0.01 b,C |
| Histidine | 20 | 0.15 ± 0.01 a,A | 0.14 ± 0.01 a,A | 0.13 ± 0.01 a,A | 0.14 ± 0.03 a,A | 0.14 ± 0.04 a,A | 0.12 ± 0.02 a,A | 0.14 ± 0.01 a,A | 0.16 ± 0.02 a,A | 0.16 ± 0.02 a,A | 0.11 ± 0.03 a,A |
| Valine | 43 | 0.33 ± 0.01 c,C | 1.23 ± 0.03 b,B | 1.27 ± 0.01 b,B | 1.34 ± 0.02 a,A | 0.27 ± 0.05 c,D | 0.35 ± 0.01 b,C | 1.29 ± 0.03 a,B | 1.27 ± 0.01 a,B | 1.25 ± 0.01 a,B | 0.26 ± 0.02 c,D |
| Methionine | 28 | 0.95 ± 0.01 e,F | 1.34 ± 0.01 c,D | 1.40 ± 0.02 b,C | 1.99 ± 0.01 a,B | 1.19 ± 0.01 d,E | 0.97 ± 0.01 d,F | 1.41 ± 0.01 b,C | 1.36 ± 0.01 c,D | 2.13 ± 0.02 a,A | 0.87 ± 0.02 e,G |
| Isoleucine | 32 | 0.94 ± 0.02 c,D | 0.90 ± 0.03 c,D | 0.90 ± 0.04 c,D | 1.69 ± 0.01 a,B | 1.32 ± 0.02 b,C | 0.96 ± 0.03 b,D | 0.90 ± 0.03 b,D | 0.81 ± 0.01 c,E | 1.99 ± 0.01 a,A | 0.91 ± 0.02 b,D |
| Leucine | 66 | 0.75 ± 0.04 d,G | 2.66 ± 0.04 c,E | 2.69 ± 0.01 c,E | 3.96 ± 0.02 b,C | 4.14 ± 0.02 a,B | 3.29 ± 0.02 b,D | 2.72 ± 0.02 c,E | 2.56 ± 0.01 d,F | 4.56 ± 0.01 a,A | 3.24 ± 0.03 b,D |
| Phenylalanine | 52 | 2.61 ± 0.01 b,C | 2.39 ± 0.01 c,E | 2.60 ± 0.03 b,C | 3.24 ± 0.04 a,A | 2.60 ± 0.03 b,C | 2.92 ± 0.01 b,B | 2.52 ± 0.01 d,D | 2.63 ± 0.02 c,C | 3.28 ± 0.02 a,A | 2.50 ± 0.02 d,D |
| Tryptophan | 8.5 | 0.14 ± 0.09 a,A | 0.13 ± 0.07 a,A | 0.12 ± 0.07 a,A | 0.13 ± 0.09 a,A | 0.11 ± 0.08 a,A | 0.11 ± 0.09 a,A | 0.10 ± 0.07 a,A | 0.14 ± 0.01 a,A | 0.12 ± 0.06 a,A | 0.14 ± 0.06 a,A |
| Amino Acids | Phase 1 (mg·g−1) | Phase 2 (mg·g−1) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ME1 | NC1 | NN1 | DM1 | DA1 | ME2 | NC2 | NN2 | DM2 | DA2 | |
| Threonine | 1.011 ± 0.005 b,B | 1.019 ± 0.010 b,B | 0.970 ± 0.014 c,C | 1.008 ± 0.007 b,B | 1.169 ± 0.002 a,A | 0.655 ± 0.007 c,D | 0.595 ± 0.021 d,E | 0.644 ± 0.012 c,D | 0.890 ± 0.014 a,C | 0.665 ± 0.017 b,D |
| Lysine | 0.025 ± 0.003 a,A | 0.040 ± 0.003 a,A | 0.035 ± 0.007 a,A | 0.030 ± 0.014 a,b,A | 0.029 ± 0.002 b,B | 0.016 ± 0.003 b,C | 0.026 ± 0.001 a,B | 0.017 ± 0.002 b,C | 0.032 ± 0.008 a,B | 0.025 ± 0.005 a,B |
| Histidine | 0.058 ± 0.005 a,b,A | 0.065 ± 0.002 a,A | 0.045 ± 0.007 c,C | 0.050 ± 0.009 b,B | 0.059 ± 0.005 a,b,A | 0.030 ± 0.004 b,D | 0.035 ± 0.003 b,D | 0.020 ± 0.015 b,D | 0.050 ± 0.001 a,B | 0.032 ± 0.004 b,D |
| Valine | 0.065 ± 0.002 c,E | 0.261 ± 0.001 a,A | 0.215 ± 0.007 b,B | 0.205 ± 0.008 b,B | 0.053 ± 0.007 c,E | 0.040 ± 0.008 c,E | 0.145 ± 0.007 b,D | 0.185 ± 0.010 a,C | 0.170 ± 0.008 a,C | 0.039 ± 0.006 c,E |
| Methionine | 0.263 ± 0.001 c,D | 0.436 ± 0.013 a,A | 0.365 ± 0.007 b,B | 0.445 ± 0.008 a,A | 0.357 ± 0.003 b,B | 0.170 ± 0.001 d,F | 0.240 ± 0.007 c,E | 0.306 ± 0.019 b,C | 0.450 ± 0.001 a,A | 0.170 ± 0.001 d,F |
| Isoleucine | 0.228 ± 0.001 c,D | 0.255 ± 0.001 b,C | 0.210 ± 0.011 d,E | 0.340 ± 0.021 a,B | 0.345 ± 0.001 a,B | 0.140 ± 0.017 b,F | 0.135 ± 0.015 b,F | 0.159 ± 0.015 b,F | 0.370 ± 0.003 a,A | 0.160 ± 0.013 b,F |
| Leucine | 0.088 ± 0.001 d,G | 0.368 ± 0.001 b,C | 0.285 ± 0.008 c,D | 0.375 ± 0.020 b,C | 0.523 ± 0.003 a,A | 0.235 ± 0.010 d,E | 0.200 ± 0.007 e,F | 0.243 ± 0.001 c,E | 0.410 ± 0.003 a,B | 0.270 ± 0.008 b,D |
| Phenylalanine | 0.387 ± 0.007 b,B | 0.419 ± 0.023 a,A | 0.370 ± 0.010 b,B | 0.380 ± 0.007 b,B | 0.418 ± 0.001 a,A | 0.265 ± 0.006 c,D | 0.230 ± 0.001 d,E | 0.317 ± 0.029 b,C | 0.375 ± 0.011 a,B | 0.265 ± 0.008 c,D |
| Tryptophan | 0.133 ± 0.009 a,A | 0.145 ± 0.001 a,A | 0.105 ± 0.009 b,B | 0.115 ± 0.003 b,B | 0.112 ± 0.06 b,B | 0.070 ± 0.002 c,D | 0.067 ± 0.011 c,D | 0.111 ± 0.011 a,B | 0.082 ± 0.008 b,C | 0.091 ± 0.001 b,C |
| Amino Acids | Phase 1 (mg·g−1) | Phase 2 (mg·g−1) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ME1 | NC1 | NN1 | DM1 | DA1 | ME2 | NC2 | NN2 | DM2 | DA2 | |
| Threonine | 1.010 ± 0.007 b,B | 0.965 ± 0.007 c,C | 0.967 ± 0.010 c,C | 0.995 ± 0.009 c,C | 1.115 ± 0.007 a,A | 0.595 ± 0.005 c,F | 0.575 ± 0.020 d,F | 0.580 ± 0.014 c,F | 0.850 ± 0.014 a,D | 0.635 ± 0.009 b,E |
| Lysine | 0.024 ± 0.007 b,B | 0.030 ± 0.005 a,A | 0.031 ± 0.002 a,A | 0.025 ± 0.004 b,A | 0.025 ± 0.003 b,B | 0.016 ± 0.004 b,B | 0.024 ± 0.003 b,B | 0.015 ± 0.005 b,B | 0.030 ± 0.003 a,A | 0.018 ± 0.004 b,B |
| Histidine | 0.055 ± 0.013 a,A | 0.063 ± 0.010 a,A | 0.044 ± 0.010 a,A | 0.045 ± 0.010 a,A | 0.055 ± 0.012 a,A | 0.027 ± 0.005 b,B | 0.030 ± 0.001 b,B | 0.015 ± 0.007 c,C | 0.045 ± 0.008 a,A | 0.030 ± 0.001 b,B |
| Valine | 0.061 ± 0.018 d,E | 0.255 ± 0.013 a,A | 0.210 ± 0.07 b,B | 0.180 ± 0.005 c,C | 0.051 ± 0.012 d,E | 0.038 ± 0.008 c,E | 0.135 ± 0.001 b,D | 0.175 ± 0.007 a,C | 0.165 ± 0.011 a,C | 0.035 ± 0.015 c,E |
| Methionine | 0.255 ± 0.011 c,D | 0.415 ± 0.010 a,B | 0.350 ± 0.07 b,C | 0.425 ± 0.007 a,A | 0.345 ± 0.001 b,C | 0.160 ± 0.002 d,E | 0.230 ± 0.015 c,D | 0.290 ± 0.010 b,D | 0.430 ± 0.004 a,A | 0.165 ± 0.005 d,E |
| Isoleucine | 0.225 ± 0.012 b,B | 0.245 ± 0.010 b,B | 0.180 ± 0.012 c,C | 0.319 ± 0.015 a,A | 0.325 ± 0.011 a,A | 0.137 ± 0.011 b,D | 0.133 ± 0.011 c,D | 0.150 ± 0.011 b,D | 0.350 ± 0.018 a,A | 0.150 ± 0.009 b,D |
| Leucine | 0.085 ± 0.001 d,G | 0.340 ± 0.008 b,C | 0.275 ± 0.011 c,D | 0.355 ± 0.011 b,C | 0.505 ± 0.005 a,A | 0.225 ± 0.008 b,E | 0.190 ± 0.14 c,F | 0.230 ± 0.001 b,E | 0.390 ± 0.005 a,B | 0.255 ± 0.015 b,D |
| Phenylalanine | 0.369 ± 0.014 c,B | 0.395 ± 0.013 b,B | 0.335 ± 0.011 d,C | 0.370 ± 0.009 b,B | 0.415 ± 0.003 a,A | 0.255 ± 0.013 c,D | 0.227 ± 0.017 d,D | 0.315 ± 0.018 b,C | 0.373 ± 0.011 a,B | 0.250 ± 0.007 c,D |
| Tryptophan | 0.125 ± 0.004 b,B | 0.142 ± 0.008 a,A | 0.101 ± 0.010 c,C | 0.080 ± 0.010 d,D | 0.105 ± 0.003 c,C | 0.069 ± 0.09 c,D | 0.065 ± 0.011 c,D | 0.105 ± 0.015 a,C | 0.080 ± 0.006 b,D | 0.085 ± 0.012 b,D |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, C.C.d.; Baião, D.d.S.; Leandro, K.C.; Paschoalin, V.M.F.; Costa, M.P.d.; Conte-Junior, C.A. Protein Quality in Infant Formulas Marketed in Brazil: Assessments on Biodigestibility, Essential Amino Acid Content and Proteins of Biological Importance. Nutrients 2021, 13, 3933. https://doi.org/10.3390/nu13113933
Almeida CCd, Baião DdS, Leandro KC, Paschoalin VMF, Costa MPd, Conte-Junior CA. Protein Quality in Infant Formulas Marketed in Brazil: Assessments on Biodigestibility, Essential Amino Acid Content and Proteins of Biological Importance. Nutrients. 2021; 13(11):3933. https://doi.org/10.3390/nu13113933
Chicago/Turabian StyleAlmeida, Cristine Couto de, Diego dos Santos Baião, Katia Christina Leandro, Vania Margaret Flosi Paschoalin, Marion Pereira da Costa, and Carlos Adam Conte-Junior. 2021. "Protein Quality in Infant Formulas Marketed in Brazil: Assessments on Biodigestibility, Essential Amino Acid Content and Proteins of Biological Importance" Nutrients 13, no. 11: 3933. https://doi.org/10.3390/nu13113933
APA StyleAlmeida, C. C. d., Baião, D. d. S., Leandro, K. C., Paschoalin, V. M. F., Costa, M. P. d., & Conte-Junior, C. A. (2021). Protein Quality in Infant Formulas Marketed in Brazil: Assessments on Biodigestibility, Essential Amino Acid Content and Proteins of Biological Importance. Nutrients, 13(11), 3933. https://doi.org/10.3390/nu13113933