
Lactobacillus Kefiri LKF01 (Kefibios®) for Prevention of Diarrhoea in Cancer Patients Treated with Chemotherapy: A Prospective Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Treatment
2.3. Study Objectives and Endpoints
- The overall incidence of diarrhoea.
- Drugs used for its treatment.
- The risk of infections/sepsis and severe neutropenia or febrile neutropenia.
- Any dose reductions/interruptions of the current treatment.
- The effects on anti-EGFR-induced acneiform rash (where applicable).
- Any AEs of the treatment.
2.4. Statistical Analysis
3. Results
3.1. Flow of Patients
3.2. Severe Diarrhoea
3.3. Secondary Endpoints
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Milles, S.S.; Muggia, A.L.; Spiro, H.M. Colonic Histologic Changes Induced by 5-Fluorouracil. Gastroenterology 1962, 43, 391–399. [Google Scholar] [CrossRef]
- Ikuno, N.; Soda, H.; Watanabe, M.; Oka, M. Irinotecan (CPT-11) and characteristic mucosal changes in the mouse ileum and cecum. J. Natl. Cancer Inst. 1995, 87, 1876–1883. [Google Scholar] [CrossRef] [PubMed]
- Loupakis, F.; Cremolini, C.; Masi, G.; Lonardi, S.; Zagonel, V.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Ronzoni, M.; Spadi, R.; et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N. Engl. J. Med. 2014, 371, 1609–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dranitsaris, G.; Shah, A.; Spirovski, B.; Vincent, M. Severe diarrhea in patients with advanced-stage colorectal cancer receiving FOLFOX or FOLFIRI chemotherapy: The development of a risk prediction tool. Clin. Colorectal Cancer 2007, 6, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Iacovelli, R.; Pietrantonio, F.; Palazzo, A.; Maggi, C.; Ricchini, F.; de Braud, F.; Di Bartolomeo, M. Incidence and relative risk of grade 3 and 4 diarrhoea in patients treated with capecitabine or 5-fluorouracil: A meta-analysis of published trials. Br. J. Clin. Pharmacol. 2014, 78, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Plaza-Diaz, J.; Ruiz-Ojeda, F.J.; Gil-Campos, M.; Gil, A. Mechanisms of action of probiotics. Adv. Nutr. 2019, 10, S49–S66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suez, J.; Zmora, N.; Segal, E.; Elinav, E. The pros, cons, and many unknowns of probiotics. Nat. Med. 2019, 25, 716–729. [Google Scholar] [CrossRef] [PubMed]
- Wei, D.; Heus, P.; van de Wetering, F.; van Tienhoven, G.; Verleye, L.; Scholten, R.J. Probiotics for the prevention or treatment of chemotherapy- or radiotherapy-related diarrhoea in people with cancer. Cochrane Database Syst. Rev. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Quigley, E.M.M. Prebiotics and probiotics: Their role in the management of gastrointestinal disorders in adults. Nutr. Clin. Pract. 2012, 27, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Bültzingslöwen, I.V.; Adlerberth, I.; Wold, A.E.; Dahlén, G.; Jontell, M. Oral and intestinal microflora in 5-fluorouracil treated rats, translocation to cervical and mesenteric lymph nodes and effects of probiotic bacteria. Oral Microbiol. Immunol. 2003, 18, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Carasi, P.; Racedo, S.M.; Jacquot, C.; Romanin, D.E.; Serradell, M.A.; Urdaci, M.C. Impact of kefir derived Lactobacillus kefiri on the mucosal immune response and gut microbiota. J. Immunol. Res. 2015, 2015, 361604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toscano, M.; De Grandi, R.; Miniello, V.L.; Mattina, R.; Drago, L. Ability of Lactobacillus kefiri LKF01 (DSM32079) to colonize the intestinal environment and modify the gut microbiota composition of healthy individuals. Dig. Liver Dis. 2017, 49, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, D.; Yan, J.; Liu, F.; Ding, P.; Chen, B.; Lu, Y.; Sun, Z. Probiotics in preventing and treating chemotherapy-induced diarrhea: A meta-analysis. Asia Pac. J. Clin. Nutr. 2019, 28, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Ghoneum, M.; Felo, N. Selective induction of apoptosis in human gastric cancer cells by Lactobacillus kefiri (PFT), a novel kefir product. Oncol. Rep. 2015, 34, 1659–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowen, J.M.; Gibson, R.J.; Coller, J.K.; Blijlevens, N.; Bossi, P.; Al-Dasoogi, N.; Bateman, E.H.; Chiang, K.; de Mooij, C.; Mayo, B.; et al. Systematic review of agents for the management of cancer treatment-related gastrointestinal mucositis and clinical practice guidelines. Support. Care Cancer 2019, 27, 4011–4022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demers, M.; Dagnault, A.; Desjardins, J. A randomized double-blind controlled trial: Impact of probiotics on diarrhea in patients treated with pelvic radiation. Clin. Nutr. 2014, 33, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Mego, M.; Chovanec, J.; Vochyanova-Andrezalova, I.; Konkolovsky, P.; Mikulova, M.; Reckova, M.; Miskovska, V.; Bystricky, B.; Beniak, J.; Medvecova, L.; et al. Prevention of irinotecan induced diarrhea by probiotics: A randomized double blind, placebo controlled pilot study. Complement. Ther. Med. 2015, 23, 356–362. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cycle | Incidence of G3–4 Diarrhoea |
|---|---|
| 1 | 3.9% |
| 2 | 3.9% |
| 3 | 1.3% |
| 4 | 1.5% |
| 5 | 0.0% |
| 6 | 0.0% |
| Mean | 1.7% |
| Cycle | Incidence of G1–4 Diarrhoea |
|---|---|
| 1 | 35.5% |
| 2 | 34.0% |
| 3 | 28.0% |
| 4 | 27.6% |
| 5 | 20.0% |
| 6 | 25.0% |
| Mean | 28.35% |
| Cycle | Cisplatin/Oxaliplatin | Doublets and Triplets of Irinotecan | 5-FU | Capecitabine |
|---|---|---|---|---|
| 1 | 1.7% | 11.0% | 4.7% | 2.9% |
| 2 | 1.7% | 11.0% | 4.7% | 2.9% |
| 3 | 1.8% | 0% | 0% | 2.9% |
| 4 | 0% | 0% | 0% | 0% |
| 5 | 0% | 0% | 0% | 0% |
| 6 | 0% | 0% | 0% | 0% |
| Mean | 0.86% | 3.6% | 4.7% | 1.45% |
| Characteristics | Main Findings |
|---|---|
| Type of study | Prospective observational |
| Number of patients | 78 (76 evaluable) |
| Median age | 67 years |
| Treatment duration | 4 months |
| Probiotic used | Lactobacillus kefiri |
| Disease (number): | |
| GASTRO-OESOPHAGEAL | 16 |
| COLORECTAL | 51 |
| PANCREATIC | 5 |
| OTHER | 6 |
| Stage of disease (%): | |
| localised | 55 |
| metastatic | 45 |
| Overall diarrhoea G1–4, mean per patient (%) | 48.7 |
| Overall diarrhoea G3–4, mean per patient (%) | 6.5 |
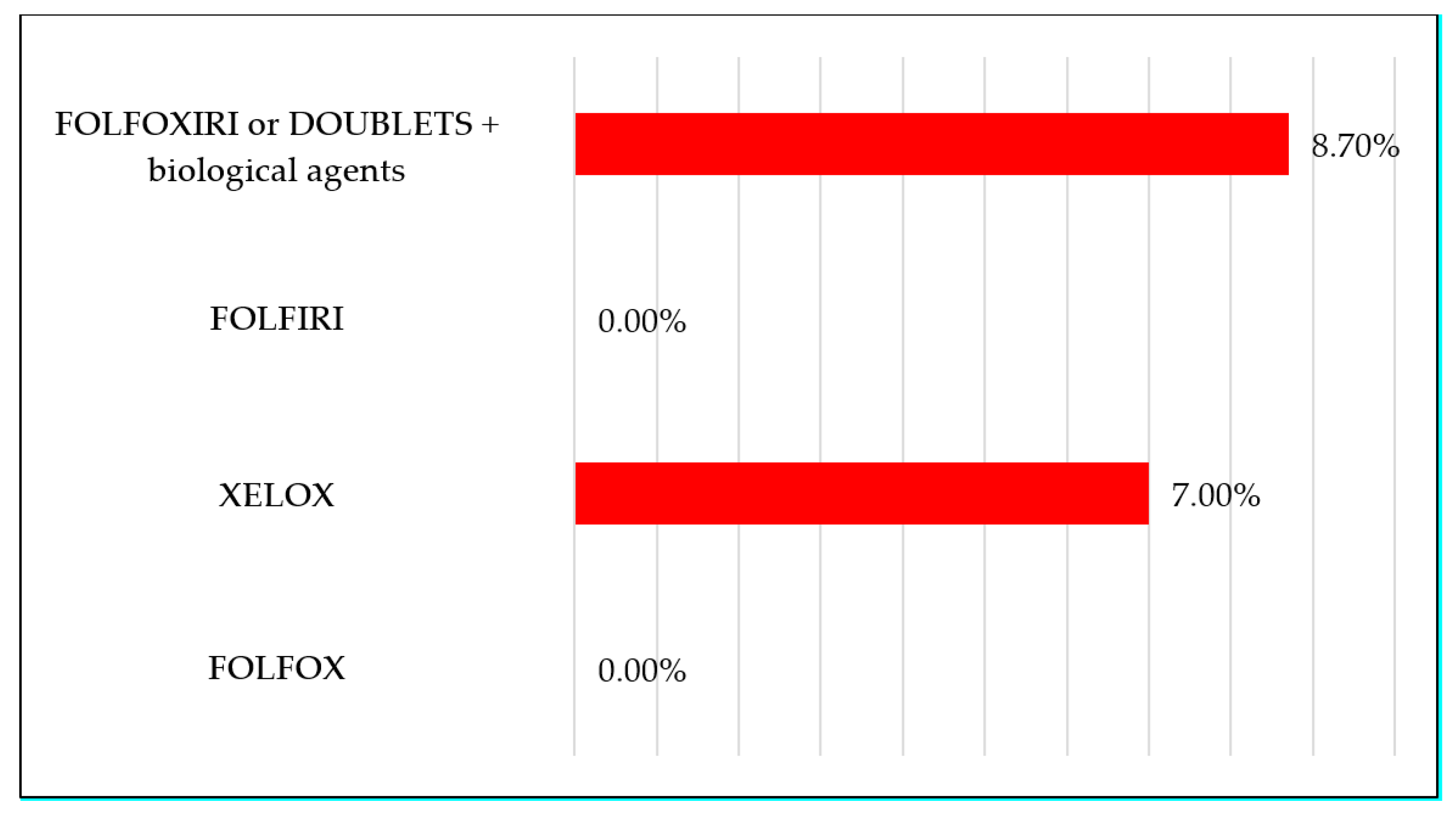
| Diarrhoea G3–4 according to schedule used, mean per patient (%): | |
| FOLFOX | 0 |
| XELOX | 7 |
| FOLFIRI | 0 |
| FOLFOXIRI (or doublets) ± biological agents | 8.7 |
| CAPECITABINE-BASED | 8.5 |
| 5FU-BASED | 4.7 |
| Compliance to treatment (dose assumed, %) | 100 |
| Adverse Events (number) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghidini, M.; Nicoletti, M.; Ratti, M.; Tomasello, G.; Lonati, V.; Ghilardi, M.; Parati, M.C.; Borgonovo, K.; Cabiddu, M.; Petrelli, F. Lactobacillus Kefiri LKF01 (Kefibios®) for Prevention of Diarrhoea in Cancer Patients Treated with Chemotherapy: A Prospective Study. Nutrients 2021, 13, 385. https://doi.org/10.3390/nu13020385
Ghidini M, Nicoletti M, Ratti M, Tomasello G, Lonati V, Ghilardi M, Parati MC, Borgonovo K, Cabiddu M, Petrelli F. Lactobacillus Kefiri LKF01 (Kefibios®) for Prevention of Diarrhoea in Cancer Patients Treated with Chemotherapy: A Prospective Study. Nutrients. 2021; 13(2):385. https://doi.org/10.3390/nu13020385
Chicago/Turabian StyleGhidini, Michele, Mariaceleste Nicoletti, Margherita Ratti, Gianluca Tomasello, Veronica Lonati, Mara Ghilardi, Maria Chiara Parati, Karen Borgonovo, Mary Cabiddu, and Fausto Petrelli. 2021. "Lactobacillus Kefiri LKF01 (Kefibios®) for Prevention of Diarrhoea in Cancer Patients Treated with Chemotherapy: A Prospective Study" Nutrients 13, no. 2: 385. https://doi.org/10.3390/nu13020385
APA StyleGhidini, M., Nicoletti, M., Ratti, M., Tomasello, G., Lonati, V., Ghilardi, M., Parati, M. C., Borgonovo, K., Cabiddu, M., & Petrelli, F. (2021). Lactobacillus Kefiri LKF01 (Kefibios®) for Prevention of Diarrhoea in Cancer Patients Treated with Chemotherapy: A Prospective Study. Nutrients, 13(2), 385. https://doi.org/10.3390/nu13020385