
Micronutrients in Multiple Pregnancies—The Knowns and Unknowns: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
3. Results
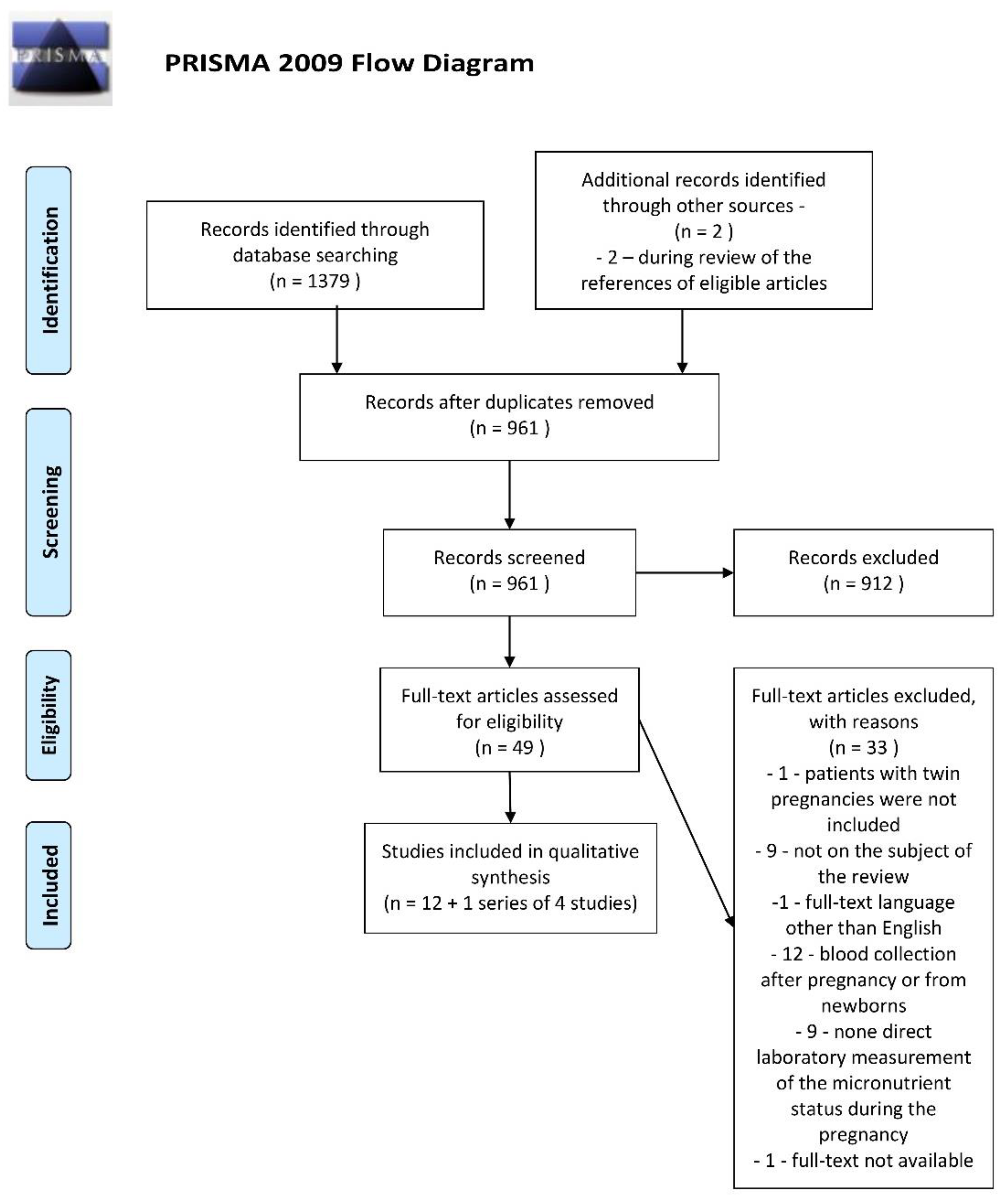
3.1. Characteristics of the Retrieved Studies
3.2. Vitamin D, Calcium and Phosphorus
3.3. Iron
3.4. Folic Acid and Vitamin B12
3.5. Other Studied Micronutrients
3.6. Risk of Bias Assessment
4. Discussion
4.1. Main Discussion
4.2. Implications and Future Research Directions
4.3. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Koletzko, B.; Godfrey, K.M.; Poston, L.; Szajewska, H.; van Goudoever, J.B.; de Waard, M.; Brands, B.; Grivell, R.M.; Deussen, A.R.; Dodd, J.M.; et al. Nutrition During Pregnancy, Lactation and Early Childhood and its Implications for Maternal and Long-Term Child Health: The Early Nutrition Project Recommendations. Ann. Nutr. Metab. 2019, 74, 93–106. [Google Scholar] [CrossRef] [PubMed]
- King, J.C. A Summary of Pathways or Mechanisms Linking Preconception Maternal Nutrition with Birth Outcomes. J. Nutr. 2016, 146, 1437S–1444S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todd, C.S.; Chowdhury, Z.; Mahmud, Z.; Islam, N.; Shabnam, S.; Parvin, M.; Bernholc, A.; Martinez, A.; Aktar, B.; Afsana, K.; et al. Maternal nutrition intervention and maternal complications in 4 districts of Bangladesh: A nested cross-sectional study. PLoS Med. 2019, 16, e1002927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hambidge, K.M.; Krebs, N.F. Strategies for optimizing maternal nutrition to promote infant development. Reprod. Health 2018, 15, 87. [Google Scholar] [CrossRef]
- Keats, E.C.; Haider, B.A.; Tam, E.; Bhutta, Z.A. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 3, CD004905. [Google Scholar] [CrossRef]
- Mousa, A.; Naqash, A.; Lim, S. Macronutrient and Micronutrient Intake during Pregnancy: An Overview of Recent Evidence. Nutrients 2019, 11, 443. [Google Scholar] [CrossRef] [Green Version]
- Marleen, S.; Dias, C.; MacGregor, R.; Allotey, J.; Aquilina, J.; Khalil, A.; Thangaratinam, S. Biochemical predictors of preterm birth in twin pregnancies: A systematic review involving 6077 twin pregnancies. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 130–142. [Google Scholar] [CrossRef]
- van Gool, J.D.; Hirche, H.; Lax, H.; De Schaepdrijver, L. Folic acid and primary prevention of neural tube defects: A review. Reprod. Toxicol. 2018, 80, 73–84. [Google Scholar] [CrossRef]
- Hsu, C.N.; Tain, Y.L. The Good, the Bad, and the Ugly of Pregnancy Nutrients and Developmental Programming of Adult Disease. Nutrients 2019, 11, 894. [Google Scholar] [CrossRef] [Green Version]
- Castro-Rodríguez, D.C.; Rodríguez-González, G.L.; Menjivar, M.; Zambrano, E. Maternal interventions to prevent adverse fetal programming outcomes due to maternal malnutrition: Evidence in animal models. Placenta 2020, 102, 49–54. [Google Scholar] [CrossRef]
- Rodriguez-Caro, H.; Williams, S.A. Strategies to reduce non-communicable diseases in the offspring: Negative and positive in utero programming. J. Dev. Orig. Heal. Dis. 2018, 9, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Cetin, I.; Bühling, K.; Demir, C.; Kortam, A.; Prescott, S.L.; Yamashiro, Y.; Yarmolinskaya, M.; Koletzko, B. Impact of Micronutrient Status during Pregnancy on Early Nutrition Programming. Ann. Nutr. Metab. 2019, 74, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Luke, B. Nutrition for Multiples. Clin. Obstet. Gynecol. 2015, 58, 585–610. [Google Scholar] [CrossRef] [PubMed]
- Shinagawa, S.; Suzuki, S.; Chihara, H.; Otsubo, Y.; Takeshita, T.; Araki, T. Maternal basal metabolic rate in twin pregnancy. Gynecol. Obstet. Investig. 2005, 60, 145–148. [Google Scholar] [CrossRef]
- Casele, H.L.; Dooley, S.L.; Metzger, B.E. Metabolic response to meal eating and extended overnight fast in twin gestation. Am. J. Obstet. Gynecol. 1996, 175, 917–921. [Google Scholar] [CrossRef]
- MacGibbon, K.W. Hyperemesis Gravidarum: Strategies to Improve Outcomes. J. Infus. Nurs. 2020, 43, 78–96. [Google Scholar] [CrossRef]
- Austin, K.; Wilson, K.; Saha, S. Hyperemesis Gravidarum. Nutr. Clin. Pract. 2019, 34, 226–241. [Google Scholar] [CrossRef]
- Rissanen, A.S.; Jernman, R.M.; Gissler, M.; Nupponen, I.; Nuutila, M.E. Maternal complications in twin pregnancies in Finland during 1987–2014: A retrospective study. BMC Pregnancy Childbirth 2019, 19, 337. [Google Scholar] [CrossRef]
- Rissanen, A.S.; Jernman, R.M.; Gissler, M.; Nupponen, I.K.; Nuutila, M.E. Perinatal outcomes in Finnish twins: A retrospective study. BMC Pregnancy Childbirth 2019, 20, 2. [Google Scholar] [CrossRef] [Green Version]
- Rissanen, A.S.; Jernman, R.M.; Gissler, M.; Nupponen, I.K.; Nuutila, M.E. Correction to: Perinatal outcomes in Finnish twins: A retrospective study. BMC Pregnancy Childbirth 2020, 20, 438. [Google Scholar] [CrossRef]
- Rothman, K.J.; Moore, L.L.; Singer, M.R.; Nguyen, U.S.; Mannino, S.; Milunsky, A. Teratogenicity of high vitamin A intake. N. Engl. J. Med. 1995, 333, 1369–1373. [Google Scholar] [CrossRef]
- Jirakittidul, P.; Sirichotiyakul, S.; Ruengorn, C.; Techatraisak, K.; Wiriyasirivaj, B. Effect of iron supplementation during early pregnancy on the development of gestational hypertension and pre-eclampsia. Arch. Gynecol. Obstet. 2018, 298, 545–550. [Google Scholar] [CrossRef]
- Cheng, Y.; Li, T.; He, M.; Liu, J.; Wu, K.; Liu, S.; Ma, Z.; Lu, J.; Zhang, Q.; Cheng, H. The association of elevated serum ferritin concentration in early pregnancy with gestational diabetes mellitus: A prospective observational study. Eur. J. Clin. Nutr. 2020, 74, 741–748. [Google Scholar] [CrossRef]
- Kataria, Y.; Wu, Y.; Horskjaer, P.H.; Mandrup-Poulsen, T.; Ellervik, C. Iron Status and Gestational Diabetes-A Meta-Analysis. Nutrients 2018, 10, 621. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.; Lian, J.; Tian, J.; Shen, Y.; Ping, Z.; Fang, X.; Min, J.; Wang, F. Dietary intake of heme iron and body iron status are associated with the risk of gestational diabetes mellitus: A systematic review and meta-analysis. Asia Pac. J. Clin. Nutr. 2017, 26, 1092–1106. [Google Scholar] [CrossRef]
- Shaji Geetha, N.; Bobby, Z.; Dorairajan, G.; Jacob, S.E. Increased hepcidin levels in preeclampsia: A protective mechanism against iron overload mediated oxidative stress? J. Matern. Fetal Neonatal Med. 2020, 10, 1–6. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence: Twin and Triplet Pregnancy NICE Guideline [NG137]. 2019. Available online: https://www.nice.org.uk/guidance/ng137 (accessed on 19 October 2020).
- Medicine, I.O. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; The National Academies Press: Washington, DC, USA, 2006; p. 1344. [Google Scholar] [CrossRef]
- Goodnight, W.; Newman, R.; Society of Maternal-Fetal, M. Optimal nutrition for improved twin pregnancy outcome. Obstet. Gynecol. 2009, 114, 1121–1134. [Google Scholar] [CrossRef] [Green Version]
- Nutrition Guideline Pregnancy: Multiples. Available online: https://www.albertahealthservices.ca/assets/info/nutrition/if-nfs-ng-pregnancy-multiples.pdf (accessed on 17 November 2020).
- Obstetrical Health Promotion, Nutritional Guidelines for a Multiple Pregnancy. Available online: https://www.ottawahospital.on.ca/en/documents/2017/01/p334english.pdf/ (accessed on 17 November 2020).
- Healthy Eating When You’re Pregnant with Twins. Available online: https://thewomens.r.worldssl.net/images/uploads/fact-sheets/Healthy-eating-when-pregnant-with-twins-2018.pdf (accessed on 17 November 2020).
- Luke, B.; Brown, M.B.; Misiunas, R.; Anderson, E.; Nugent, C.; van de Ven, C.; Burpee, B.; Gogliotti, S. Specialized prenatal care and maternal and infant outcomes in twin pregnancy. Am. J. Obstet. Gynecol. 2003, 189, 934–938. [Google Scholar] [CrossRef]
- Luke, B. Improving multiple pregnancy outcomes with nutritional interventions. Clin. Obstet. Gynecol. 2004, 47, 146–162. [Google Scholar] [CrossRef]
- Bricker, L.; Reed, K.; Wood, L.; Neilson, J.P. Nutritional advice for improving outcomes in multiple pregnancies. Cochrane Database Syst. Rev. 2015, 2015, CD008867. [Google Scholar] [CrossRef]
- Committee, S.R.; Grantz, K.L.; Kawakita, T.; Lu, Y.L.; Newman, R.; Berghella, V.; Caughey, A. SMFM Special Statement: State of the science on multifetal gestations: Unique considerations and importance. Am. J. Obstet. Gynecol. 2019, 221, B2–B12. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- McFadyen, M.; Farquharson, J.; Cockburn, F. Maternal and umbilical cord erythrocyte omega-3 and omega-6 fatty acids and haemorheology in singleton and twin pregnancies. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F134–F138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben Miled, S.; Bibi, D.; Khalfi, N.; Blibech, R.; Gharbi, Y.; Castalli, R.; Khrouf, N. Iron stocks and risk of anemia in twins. Arch. Inst. Pasteur Tunis 1989, 66, 221–241. [Google Scholar] [PubMed]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Nwosu, B.U.; Soyka, L.A.; Angelescu, A.; Hardy, O.T.; Lee, M.M. Multifetal pregnancy may increase the risk for severe maternal and neonatal vitamin D deficiency. Endocrinologist 2008, 18, 172–175. [Google Scholar] [CrossRef]
- Delaney, K.M.; Guillet, R.; Pressman, E.K.; Caulfield, L.E.; Zavaleta, N.; Abrams, S.A.; O’Brien, K.O. Iron absorption during pregnancy is underestimated when iron utilization by the placenta and fetus is ignored. Am. J. Clin. Nutr. 2020, 112, 576–585. [Google Scholar] [CrossRef]
- Nakayama, S.; Yasui, T.; Suto, M.; Sato, M.; Kaji, T.; Uemura, H.; Maeda, K.; Irahara, M. Differences in bone metabolism between singleton pregnancy and twin pregnancy. Bone 2011, 49, 513–519. [Google Scholar] [CrossRef]
- de la Calle, M.; Garcia, S.; Duque, M.; Bartha, J.L. Vitamin D concentrations are decreased in singleton and twin pregnancies. Med. Clin. 2016, 147, 371–372. [Google Scholar] [CrossRef]
- Bajoria, R.; Lazda, E.; Ward, S.; Sooranna, S. Iron metabolism in monochorionic twin pregnancies in relation to twin–twin transfusion syndrome. Hum. Reprod. 2001, 16, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Blarduni, E.; Arrospide, A.; Galar, M.; Castano, L.; Mar, J.; Grupo, G. Factors associated with the prevalence of hypovitaminosis D in pregnant women and their newborns. An. Pediatr 2019, 91, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Ball, E.W.; Giles, C. Folic Acid and Vitamin B12 Levels in Pregnancy and Their Relation to Megaloblastic Anaemia. J. Clin. Pathol. 1964, 17, 165–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, J.M.; Sommerville, J.W. Practical Evaluation of the Figlu Test in Pregnancy with Special Reference to the White Cell Changes. J. Clin. Pathol. 1965, 18, 322–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, G.S.; Norman, A.W.; Willis, D.M.; Goltzman, D.; Guyda, H.; Solomon, S.; Philips, D.R.; Bishop, J.E.; Mayer, E. Regulation of vitamin D metabolism in normal human pregnancy. J. Clin. Endocrinol. Metab. 1983, 56, 363–370. [Google Scholar] [CrossRef]
- Okah, F.A.; Tsang, R.C.; Sierra, R.; Brady, K.K.; Specker, B.L. Bone turnover and mineral metabolism in the last trimester of pregnancy: Effect of multiple gestation. Obstet. Gynecol. 1996, 88, 168–173. [Google Scholar] [CrossRef]
- Goswami, D.; Rani, R.; Saxena, A.; Arora, M.S.; Batra, S.; Sreenivas, V. Maternal and neonatal vitamin-D status in twin versus singleton pregnancies. J. Obstet. Gynaecol. Res. 2016, 42, 1250–1257. [Google Scholar] [CrossRef]
- Ru, Y.; Pressman, E.K.; Cooper, E.M.; Guillet, R.; Katzman, P.J.; Kent, T.R.; Bacak, S.J.; O’Brien, K.O. Iron deficiency and anemia are prevalent in women with multiple gestations. Am. J. Clin. Nutr. 2016, 104, 1052–1060. [Google Scholar] [CrossRef]
- Ru, Y.; Pressman, E.K.; Guillet, R.; Katzman, P.J.; Bacak, S.J.; O’Brien, K.O. Predictors of anemia and iron status at birth in neonates born to women carrying multiple fetuses. Pediatr. Res. 2018, 84, 199–204. [Google Scholar] [CrossRef]
- Ru, Y.; Pressman, E.K.; Guillet, R.; Katzman, P.J.; Vermeylen, F.; O’Brien, K.O. Umbilical Cord Hepcidin Concentrations Are Positively Associated with the Variance in Iron Status among Multiple Birth Neonates. J. Nutr. 2018, 148, 1716–1722. [Google Scholar] [CrossRef]
- Delaney, K.M.; Guillet, R.; Fleming, R.E.; Ru, Y.; Pressman, E.K.; Vermeylen, F.; Nemeth, E.; O’Brien, K.O. Umbilical Cord Serum Ferritin Concentration is Inversely Associated with Umbilical Cord Hemoglobin in Neonates Born to Adolescents Carrying Singletons and Women Carrying Multiples. J. Nutr. 2019, 149, 406–415. [Google Scholar] [CrossRef]
- Shinar, S.; Shapira, U.; Maslovitz, S. Redefining normal hemoglobin and anemia in singleton and twin pregnancies. Int. J. Gynaecol. Obstet. 2018, 142, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Jantsch, L.B.; de Lucca, L.; Dorneles, B.N.; Konopka, C.K.; Gonçalves, T.D.L. Evaluation of oxidative stress and δ-aminolevulinate dehydratase activity in twin pregnancies. J. Matern. Fetal Neonatal Med. 2020, 33, 3071–3076. [Google Scholar] [CrossRef]
- Santana, D.S.; Surita, F.G.; Cecatti, J.G. Multiple Pregnancy: Epidemiology and Association with Maternal and Perinatal Morbidity. Rev. Bras. Ginecol. Obstet. 2018, 40, 554–562. [Google Scholar] [CrossRef] [Green Version]
- Luke, B.; Gopal, D.; Cabral, H.; Stern, J.E.; Diop, H. Adverse pregnancy, birth, and infant outcomes in twins: Effects of maternal fertility status and infant gender combinations; the Massachusetts Outcomes Study of Assisted Reproductive Technology. Am. J. Obstet. Gynecol. 2017, 217, 330.e331–330.e335. [Google Scholar] [CrossRef]
- Gür, S.; Türk, G.; Demirci, E.; Yüce, A.; Sönmez, M.; Ozer, S.; Aksu, E. Effect of pregnancy and foetal number on diameter of corpus luteum, maternal progesterone concentration and oxidant/antioxidant balance in ewes. Reprod. Domest. Anim. 2011, 46, 289–295. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.; Ward, T.; Stolfi, A.; Ayoub, D. Overrepresentation of multiple birth pregnancies in young infants with four metabolic bone disorders: Further evidence that fetal bone loading is a critical determinant of fetal and young infant bone strength. Osteoporos. Int. 2014, 25, 1861–1873. [Google Scholar] [CrossRef]
- Katz, J.; Tielsch, J.M.; Thulasiraj, R.D.; Coles, C.; Sheeladevi, S.; Yanik, E.L.; Rahmathullah, L. Risk factors for maternal night blindness in rural South India. Ophthalmic Epidemiol. 2009, 16, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Ju, R.; Wu, R.; Li, J.-X.; Zhang, P.-B. Astigmatism in twin infants is related to pregnant nutrition. Biomed. Res. 2014, 25, 528–532. [Google Scholar]
- Hediger, M.L.; Luke, B. Hemodynamics and Maternal Weight Gain in Twin Pregnancies; American Public Health Association: Chicago, IL, USA, 1999; pp. 9–11. [Google Scholar]
- Blickstein, I.; Goldschmit, R.; Lurie, S. Hemoglobin levels during twin vs. singleton pregnancies. Parity makes the difference. J. Reprod. Med. 1995, 40, 47–50. [Google Scholar]
- Spellacy, W.N.; Handler, A.; Ferre, C.D. A case-control study of 1253 twin pregnancies from a 1982-1987 perinatal data base. Obstet. Gynecol. 1990, 75, 168–171. [Google Scholar]
- Dubois, S.; Dougherty, C.; Duquette, M.P.; Hanley, J.A.; Moutquin, J.M. Twin pregnancy: The impact of the Higgins Nutrition Intervention Program on maternal and neonatal outcomes. Am. J. Clin. Nutr. 1991, 53, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Kamiloglu, S.; Tomas, M.; Ozdal, T.; Capanoglu, E. Effect of food matrix on the content and bioavailability of flavonoids. Trends Food Sci. Technol. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search Strategy | Number of Results |
|---|---|---|
| PubMed/MEDLINE | (“pregnancy, multiple”(MeSH Terms) OR “twin pregnanc *”(Title/Abstract) OR “twin gestation *”(Title/Abstract) OR “twins”(Title/Abstract) OR “triplet *”(Title/Abstract) OR “quadruplet *”(Title/Abstract) OR “quintuplet *”(Title/Abstract) OR “multiple pregnanc *”(Title/Abstract) OR “multiples”(Title/Abstract) OR “multifetal *”(Title/Abstract)) AND (“Nutrients”(MeSH Terms) OR “nutrient *”(Title/Abstract) OR “Micronutrients”(MeSH Terms) OR “micronutrient *”(Title/Abstract) OR “Trace Elements”(MeSH Terms) OR “trace element *”(Title/Abstract) OR “Vitamins”(MeSH Terms) OR “vitamin *”(Title/Abstract)) | 542 |
| Embase | (‘twin pregnanc *’:ab OR ‘twin gestation *’:ab OR twins:ab OR triplet *:ab OR quadruplet *:ab OR quintuplet *:ab OR ‘multiple pregnanc *’:ab OR ‘multiple gestation *’:ab OR multiples:ab OR ‘multifetal *’:ab) AND (nutrient *:ab OR micronutrient *:ab OR ‘trace element *’:ab OR vitamin *:ab) AND [embase]/lim | 612 |
| Scopus | (TITLE-ABS-KEY ((“twin pregnanc *” OR “twin gestation *” OR twins: OR triplet * OR quadruplet *: ab OR quintuplet * OR “multiple pregnanc *” OR “multiple gestation *” OR multiples OR multifetal *)) AND TITLE-ABS-KEY ((nutrient * OR micronutrient * OR “trace element *” OR vitamin *))) | 225 |
| 3 databases | 1379 |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| All types of original articles including case reports, case series and scientific letters, concerning the nutritional status of selected microelements in women with multiple pregnancies | Reviews, editorials, conference papers or abstracts |
| Published in a peer-reviewed scientific journal | Published in a journal other than a peer-reviewed scientific one |
| At least one laboratory measurement of the micronutrient level in women during the multiple gestation or at birth with available direct results | Post-pregnancy measurements |
| Presumption of nutritional status based only on such factors as symptoms, not confirmed with a laboratory examination | |
| Full-text available in English | Language other than English; only abstract available in English |
| Unrestricted publication time | |
| Human studies | Animal studies |
| Study | Year and Country of Publication | Micronutrient(s) of Interest | Main Aim | Number of Women and Type of Multiple Pregnancy Included in the Study Results | Mean * Maternal Age at Examination (Years) | Mean * Gestational Age at Examination (Gestational Weeks) |
|---|---|---|---|---|---|---|
| Ball & Giles [47] | 1964 UK | Folic acid Vitamin B12 | To analyze folic acid and vitamin B12 levels in pregnancy and their relation to megaloblastic anemia | 13 ** twin | 26.7 ** ± 6.3 | 33.3 ** ± 5.6 |
| Scott & Sommerville [48] | 1965 UK | Folic acid | To perform a practical evaluation of the Figlu test in pregnancy | 33 twin | LoD | LoD |
| Reddy et al. [49] | 1983 Canada | Vitamin D | To establish the relationship of vitamin D metabolites with each other and their dependency on pregnancy-related hormones | 27 twin | 27 ± 4.3 | Range 37–41 |
| Okah et al. [50] | 1996 USA | Vitamin D Calcium Phosphorus | To check if maternal bone turnover and mineral stress are greater in multiple pregnancy than in singleton pregnancy | 15 twin 2 triplet | 29.2 ± 1.5 | 30.6 ± 0.9 |
| Bajoria et al. [45] | 2001 UK | Iron | To investigate fetal iron metabolism in MC twin pregnancies in relation to TTTS | 22 twin | LoD | TTTS 23 (Range 19–31) Control 30 (Range 21–34) |
| Nakayama et al. [43] | 2011 Japan | Vitamin D Calcium Phosphorus | To examine the influence of twin pregnancy on calcium metabolism by comparison to singleton pregnancy | C-S study: 131 twin L study: 11 twin | L study: 30.8 ±4.8 | Time points: 10, 25, 30 and 36 weeks |
| de la Calle et al. [44] | 2016 Spain | Vitamin D | To answer if women pregnant with twins have lower serum levels of vitamin D | 97 twin | LoD | Range: 12–14 |
| Goswami et al. [51] | 2016 India | Vitamin D Calcium Phosphorus | To compare maternal and neonatal vitamin D status in twin versus singleton pregnancies | 50 twin | 27.4 ± 4.2 | 35.8 ± 1.9 |
| Ru et al. [52] and related studies: [53,54,55] | 2016 USA | Iron Folic acid Vitamin B12 | To characterize longitudinal changes in iron status across the pregnancy in a cohort of healthy women with multiple gestations and identify the determinants of maternal iron deficiency and anemia | 64 twin 18 triplet 1 quadruplet | 30.3 ± 5.1 | Samples obtained during pregnancy 24.4 ± 5.4 at delivery 35.3 ± 2.3 |
| Shinar et al. [56] | 2018 Israel | Iron | To assess the benefit of the hemoglobin cutoff of 10.5 g/dL as a trigger for anemia evaluation during the second trimester of pregnancy | 300 twin | 25.8 ± 5.0 | 17.0 ± 0.9 |
| Blarduni et al. [46] | 2019 Spain | Vitamin D | To measure the prevalence of hypovitaminosis D in mothers and newborns | 11 type unknown | LoD | LoD |
| Delaney et al. [42] | 2020 USA | Iron Folic Acid Vitamin B12 | To evaluate maternal iron absorption and identify factors associated with iron partitioning between the maternal, neonatal, and placental compartments | 4 twin 1 triplet | 31.0 ± 2.3 | 33.8 ± 2.5 |
| Jantsch et al. [57] | 2020 Brazil | Vitamin C | To assess maternal oxidative stress in twin pregnancies | 30 twin | 28.0 (interquartile range 23–33) | 31.5 ± 0.5 |
| Study | Data on Supplementation | Serum Calcium [Mean ± SD; mg/dL] * | Serum Phosphorus [Mean ± SD; mg/dL] * | Serum 25(OH)D [Mean ± SD; ng/mL] * | Comparison: Multiple vs. Singleton Pregnancies | |
|---|---|---|---|---|---|---|
| Reddy et al. [49] | Women were advised to take 400 IU of vitamin D2 | 2nd trimester | 2nd trimester | 2nd trimester |
| |
| 8.96 ± 0.23 | 3.09 ± 0.12 | 15 ± 2.3 | ||||
| 3rd trimester | 3rd trimester | 3rd trimester | ||||
| 8.75 ± 0.14 | 3.16 ± 0.09 | 14 ± 0.9 | ||||
| At delivery | At delivery | At delivery | ||||
| 7.71 ± 0.45 | 2.59 ± 0.24 | 11 ± 1.6 | ||||
| Okah et al. [50] | Average daily dietary intake: Vitamin D: 1181 ± 246 IU Calcium: 1621 ± 346 mg | 3rd trimester | 3rd trimester | 3rd trimester |
| |
| 9.1 ± 0.1 | 3.2 ± 0.2 | 61 ± 5 | ||||
| Nakayama et al. [43] | Average daily dietary intake: Vitamin D: 296 ± 136 IU Calcium: 795 ± 287 mg Phosphate: 1022 ± 204 mg | See Figures 1B and 2B in the original manuscript ** [43] | See Figures 1B and 2B in the original manuscript [43] | C-S study | L study |
|
| 10 weeks | 10 weeks | |||||
| 12.8 ± 5.1 | 14.6 ± 8.7 | |||||
| 25 weeks | 25 weeks | |||||
| 12.5 ± 4.3 | 12.1 ± 4.5 | |||||
| 30 weeks | 30 weeks | |||||
| 15.1 ± 5.5 | 13.8 ± 5.0 | |||||
| 36 weeks | 36 weeks | |||||
| 15.0 ± 6.6 | 14.2 ± 6.4 | |||||
| de la Calle et al. [44] | All participants had taken multivitamin complex including 200 IU of vitamin D3 daily for at least 3 weeks before | NS | NS | 1st trimester |
| |
| 21.4 ± 7.8 | ||||||
| 90% < 30 | ||||||
| Goswami et al. [51] | Average daily dietary intake: Calcium: 1023 ± 275 mg No vitamin D supplementation was prescribed | 3rd trimester 9.9 ± 0.66 ** | 3rd trimester 3.9 ± 0.76 | 3rd trimester 5.7 ± 4.2 90% < 12 |
| |
| Blarduni et al. [46] | LoD | NS | NS | 92.3% < 20 |
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zgliczynska, M.; Kosinska-Kaczynska, K. Micronutrients in Multiple Pregnancies—The Knowns and Unknowns: A Systematic Review. Nutrients 2021, 13, 386. https://doi.org/10.3390/nu13020386
Zgliczynska M, Kosinska-Kaczynska K. Micronutrients in Multiple Pregnancies—The Knowns and Unknowns: A Systematic Review. Nutrients. 2021; 13(2):386. https://doi.org/10.3390/nu13020386
Chicago/Turabian StyleZgliczynska, Magdalena, and Katarzyna Kosinska-Kaczynska. 2021. "Micronutrients in Multiple Pregnancies—The Knowns and Unknowns: A Systematic Review" Nutrients 13, no. 2: 386. https://doi.org/10.3390/nu13020386
APA StyleZgliczynska, M., & Kosinska-Kaczynska, K. (2021). Micronutrients in Multiple Pregnancies—The Knowns and Unknowns: A Systematic Review. Nutrients, 13(2), 386. https://doi.org/10.3390/nu13020386