
Milk Fat Globule Membrane Supplementation in Children: Systematic Review with Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
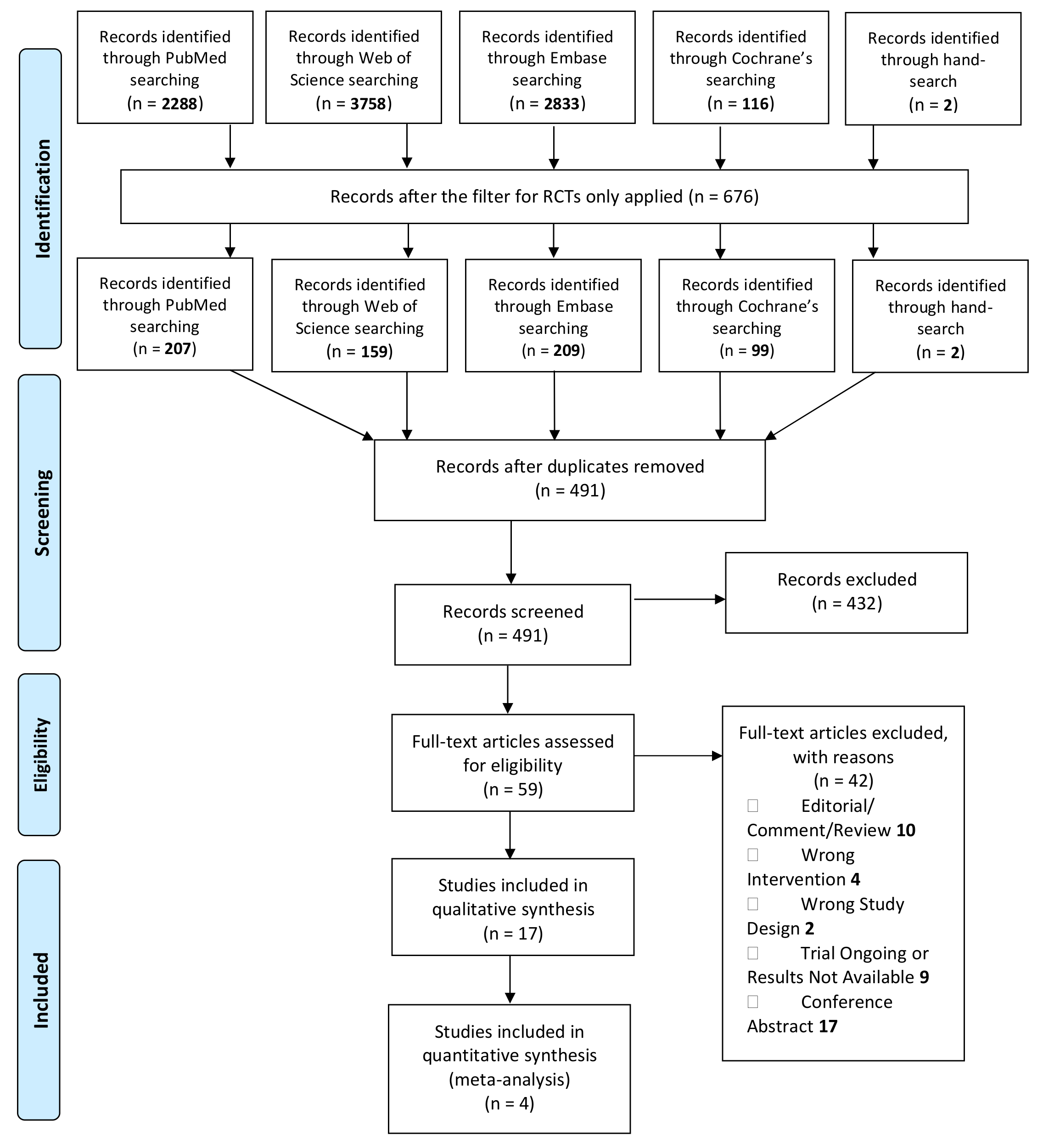
2.1. Search Strategy
2.2. Study Selection
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Risk of Bias Assessment
2.7. Data Synthesis
3. Results
3.1. Description of the Studies
3.2. Populations
3.3. Interventions
3.4. Outcomes
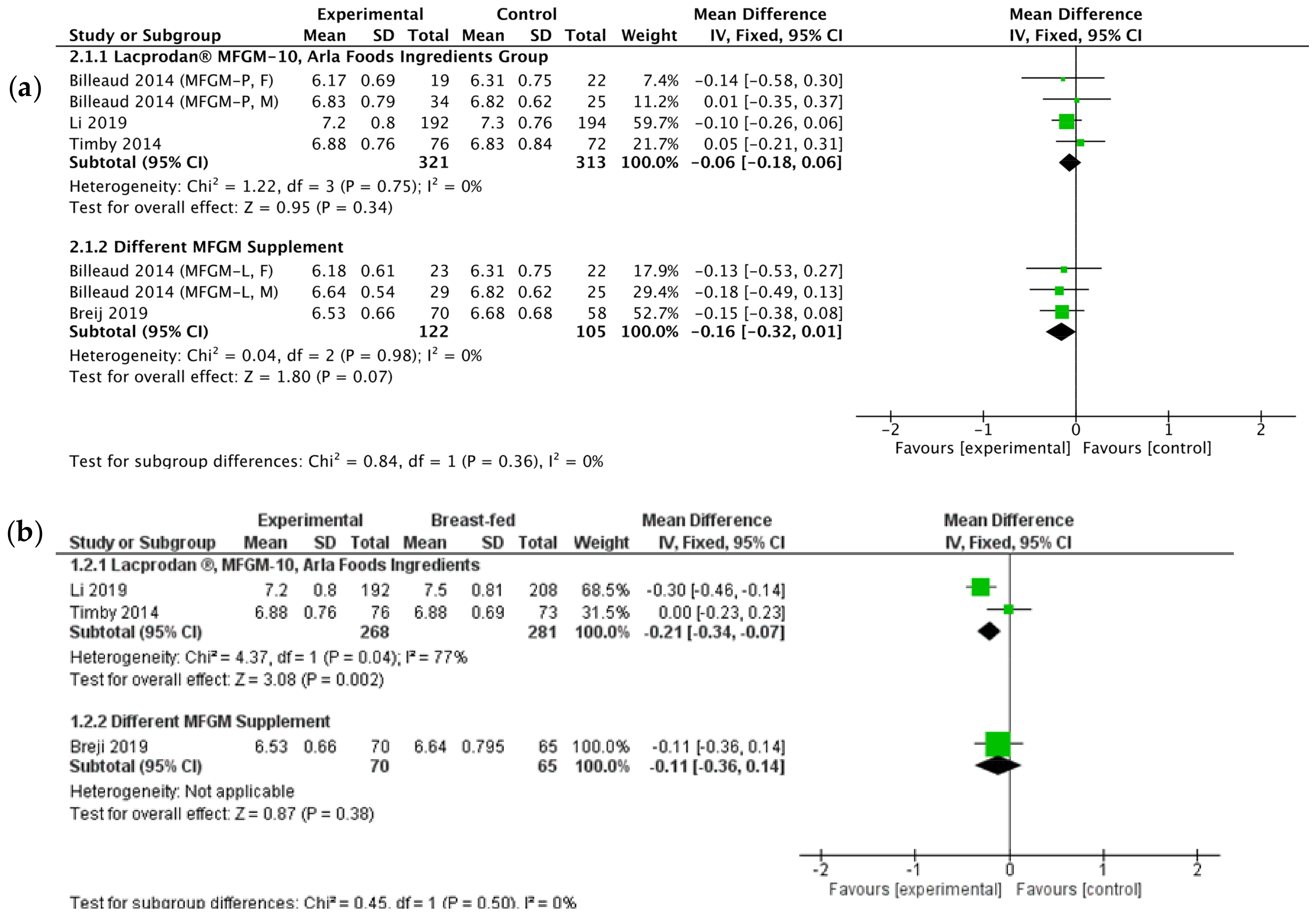
3.4.1. Anthropometric Measurements
- Experimental formula compared to a standard formula
- Experimental Formula Compared to Breastfeeding
3.4.2. Psychomotor Development
3.4.3. Risk of Infections
3.4.4. Prevention of Diarrhea in Developing Countries
3.4.5. Metabolic Effects
3.4.6. Microbiome
3.4.7. Adverse Events

{kind=link}
{kind=link}
{kind=link}
| Study ID | Study Design and Analysis Method | Population | Sample size + FU (%) at the End of Intervention or Specific Assessment Point | Intervention and Duration | Comparison | Measurement Points | Primary Outcomes | Secondary Outcomes | Results |
|---|---|---|---|---|---|---|---|---|---|
| Zavaleta et al. [24] (Peru) 2011 | Double-blind RCT ITT analysis | Healthy children, aged 6 to 11 months old, born at term with a birth weight >2500 g, primarily breast-fed | Inclusion: 550 infants - 277 EF - 273 SF Completed: 91% of infants - 91% EF - 90% SF | Intervention: Complementary daily food (40 g/day) with the protein source being the MFGM protein fraction (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: 6 months | Complementary daily food (40 g/day) with the protein source being skim milk proteins | (1) Monthly assessment by healthcare professional (2) Twice per week assessment of dietary intake (3) Blood samples collection—beginning and end of intervention | Differences between groups with regard to diarrhea morbidity | (1) Anthropometric evaluation (2) Dietary assessment (3) Hematological and biochemical assessment (hemoglobin, serum ferritin, zinc and folate). | (1) No significant difference in severe diarrhea incidence between groups—reduction of bloody diarrhea incidence in EF group (p = 0.025) (2) No differences in biochemical serum parameters between groups (3) Lower Hb level in EF group in 9–10 months of age |
| Gurnida et al. [25] (Indonesia) 2012 | Double-blind RCT PP analysis | Healthy, term infants between 2 and 8 weeks of age with birth weight ≥2.5 kg | Inclusion: 110 infants - 35 EF - 35 SF - 40 BF Completed: 83% of infants - 83% EF - 86% SF - 80% BF | Intervention: Standard formula with added complex milk lipid to increase the ganglioside GD3 (Anmum Infacare, Fonterra) Duration: From enrollment (2–8 weeks) until 6 months (24 weeks) | (1) Standard formula (2) Breastfeeding (reference group) | (1) At baseline and at monthly intervals until 6 months old (2) GMDS before and after intervention | Cognitive development using the GMDS | (1)Anthropometric measurements (2) Serum laboratory measurements | (1) Significant increase in scores for Hand and Eye Coordination (p = 0.006) and Performance (p < 0.001) and also for Total Score (General IQ) (p = 0.041) in the EF group but no differences between EF and BF group (2) No significant differences in anthropometric measurements between EF and SF groups (3) Significantly higher serum level of ganglioside G3 in EF compared to SF (p < 0.01) with no difference between EF and BF groups |
| Veereman-Wauters et al. [23] (Belgium, France, the Netherlands) 2012 | Double-blind RCT PP analysis | Healthy, pre-school children aged 2.5–6 years old | Inclusion: 253 children Completed: 72% of children - 67.5% intervention group - 76.4% control group | Intervention: 200-mL chocolate formula milk enriched with 500 mg of phospholipids with the addition of 2.5% of MFGM (INPULSE, Büllinger SA) Duration: 4 months | 200-mL chocolate formula milk | (1) Diaries with daily reports collected every 2 weeks by study coordinator (2) ASEBA assessment at day 120 of study | Number of days with fever, diarrhea, coughing, and/or constipation | (1) Number of doctor visits (2) Medication intake (3) Number of missed schooldays (4) Acceptability of the study product | (1) No difference between groups for diarrhea, constipation, cough, doctor visits, and days of school absence, medication intake (2) The number of days with fever (>38.5 °C) and the number of short (<3 day) febrile periods were significantly (p < 0.03) decreased in the intervention group |
| Billeaud et al. [12] (France, Italy) 2014 | Double-blind RCT ITT analysis | Healthy, full-term infants, ≤14 days of age, with a birthweight 2500–4500g | Inclusion: 199 infants - 72 EF (MFGM–P) - 70 EF (MFGM–L) - 57 SF Completed: 72.3% of infants - 72.2% EF (MFGM–P) - 67.1 EF (MFGM–L) - 78.9% SF | Interventions: - Lipid-rich MFGM (Anmum Infacare, Fonterra), - Protein-rich MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: Intervention from 14 (±3) days of age to 4 months (day 112) ≈14 weeks | Standard formula | Baseline visit (0–13 day), day 14 ± 3, 56 ± 5, 84 ± 7, 112 ± 7 plus 3 additional follow-up visits at 6, 9, and 12 months of age in France | Mean weight gain (g/day) from baseline (age 0–13 days) to age 112 days (≈age 4 months), with a non-inferiority margin of −3.0 g/day | (1) Anthropometric measurements (2) Plasma laboratory measurements (3) Immune response to Polio and Hib vaccines | (1) No significant differences in anthropometric measurements ) No differences in plasma phospholipid, cardiolipin, cholesterol, IGF-1, leptin levels (3) Lower C-peptide levels in MFGM-L and P group compared to control formula (p = 0.03) (4) Lower mean polio virus type 1 IgG level in the MFGM-P group in Italy (p = 0.04) |
| Poppitt et al. [26] (India) 2014 | Double-blind RCT ITT analysis | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Inclusion: 450 of infants Completed: 93% - 94% EF - 91% SF | Intervention: High ganglioside complex milk lipid supplement (Anmum Infacare, Fonterra) added to fresh milk Duration: For 12 weeks | Control supplement added to fresh milk | Baseline, assessment by fieldworker twice a week (24 visits), after 12-week intervention | Total number of days with RVD during the intervention | (1) Total number of days with diarrhea of any type (ACD) (2) Number of episodes, duration, and severity of RVD and ACD (3) RV load in stool samples at baseline and 12-week | (1) Mean duration that RVD persisted was lower in the EF group (p = 0.03) (2) The reported prevalence of major illness during the period of 12 weeks was lower in the EF group (OR 3.5, 95% CI 0.9–20.4, p = 0.05) |
| Timby et al.* [11] (Sweden) 2014 | Double-blind RCT ITT analysis | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Inclusion: 240 infants -80 EF -80 SF -80 BF Completed (6 months of age): 92% of infants - 95% EF - 90% SF - 90% BF | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: From enrollment <2 months to 6 months of age, follow-up until 12 months of age | (1) Standard formula (2) Breastfeeding (reference group) | At inclusion, 4, 6, 12 months of age | (1) Cognitive level at 12 month using Bayley-III (2) Weight at 6 months | (1) Anthropometric measurements (2) Plasma inulin | (1) Significantly higher cognitive development in EF group than in SF (p = 0.008) but not different from BFR group (2) When groups were divided into BFR compared with formula-fed groups (EF + SF), significant interactions were found between group and time on z-scores for weight (p = 0.025) and length (p = 0.003) (3) Formula (EF + SF) fed infants had higher insulin plasma concentrations at baseline and 4, 6 months compared to BF group |
| Timby et al.* [14] (Sweden) 2014 | Double-blind RCT ITT analysis | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Inclusion: 240 infants -80 EF -80 SF -80 BF Analysis at: - 4 months of age: 92.5% - 6 months of age: 92% - 12 months of age: 92% | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: From enrollment <2 months to 6 months of age, follow-up until 12 months of age | (1) Standard formula (2) Breastfeeding (reference group) | At inclusion, 4, 6, 12 months of age | Serum lipids, adipokines, homocysteine, inflammatory biomarkers, and blood pressure | NA | (1) Until 6 mo, the EF group had higher total serum cholesterol concentration than the SF group, reaching the level of the BF group (2) Blood pressure did not differ significantly between groups |
| Timby et al.* [15] (Sweden) 2015 | Double-blind RCT ITT analysis | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Inclusion: 240 infants - 80 EF - 80 SF - 80 BF Analysis at: - 6 months of age: 93% - 12 months of age: 75% | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: From enrollment <2 months to 6 months of age, follow-up until 12 months of age | (1) Standard formula (2) Breastfeeding (reference group) | (1) Diaries filled by parent until 6 and 12 months of age (2) IgG level to pneumococci at 12 month of age | (1) Incidence of infections throughout 12 months (2) Infection-related medication intake (2) Serum concentration of IgG to pneumococci | NA | (1) Fewer acute otitis media episodes in EF compared to the SF group (p = 0.034) (2) The incidence (p = 0.021) and longitudinal prevalence (p = 0.012) of antipyretic use were significantly lower in the EF group (3) EF group had lower s-IgG concentrations for S. Pneumoniae serotypes 1, 5, and 14 compared with the SF group |
| Timby et al.* [16] (Sweden) 2017 | Double-blind RCT Analysis of randomly selected infants | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Inclusion: 240 infants - 80 EF - 80 SF - 80 BF Analysis at: - 4 months of age 52% - 12 months of age: 69% | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: From enrollment <2 months to 6 months of age, follow-up until 12 months of age | (1) Standard formula (2) Breastfeeding (reference group) | Control visits at 4 and 12 months of age | Oral microbiota composition | NA | (1) The species richness did not differ between the EF and SF group at 4 or 12 months of age (2) BF group had significantly lower species richness in oral microbiota than the formula-fed groups at 4 and 12 month of age |
| Grip et al.* [17] (Sweden) 2018 | Double-blind RCT Analysis of the serum of randomly selected infants from each group | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Inclusion: 240 infants - 80 EF - 80 SF - 80 BF Analysis at: - 4 month of age: 90 randomly chosen infants - 6 months of age: 89% of infants - 12 months of age: 90 randomly chosen infants | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: From enrollment: <2 months to 6 months of age, follow-up until 12 months of age | (1) Standard formula (2) Breastfeeding (reference group) | Blood samples were collected at 4, 6, and 12 months of age and were obtained >2 h after the latest meal in randomly selected infants | (1) Plasma lipidome and erythrocyte membrane lipidome (6 months) (2) Serum lipidome (4 and 12 months) | NA | There were significant differences in the serum/plasma lipidome at 4 and 6 months of age in infants fed the EF compared to infants fed SF. This separation was also detected in erythrocyte membranes at 6 months, but it did not remain in sera collected at 12 months of age, 6 months after the end of the intervention |
| He X. et al.* [18] (Sweden) 2019 | Double-blind RCT Analysis of the serum and plasma of randomly selected infants from each group | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Longitudinal assessment: 90 randomly selected infants out of 240 Cross-sectional assessment: 212 infants out of 240 | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: From enrollment: <2 months to 6 months of age, follow-up until 12 months of age | (1) Standard formula (2) Breastfeeding (reference group) | At enrollment, 4, 6, 12 months of age: serum for longitudinal assessment 6 month of age- plasma for cross-sectional assessment | Metabolome | NA | (1) Formula-fed infants had higher levels of amino acid catabolism by-products and a low efficiency of amino acid clearance (preference for protein metabolism) (2) BF infants had higher levels of fatty acid oxidation products (preference for fat metabolism) |
| He X. et al.* [19] (Sweden) 2019 | Double-blind RCT Analysis of fecal microbiome and metabolome of randomly selected infants from each group | Healthy infants <2 months of age, gestational age 37–42 weeks, birth weight 2500–4500 g | Randomly selected subset of 90 infants (15 females and 15 males from each group: BF, SF, and BF) out of 240 infants | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) Duration: From enrollment: <2 months to 6 months of age, follow-up until 12 months of age | (1) Standard formula (2) Breastfeeding (reference group) | At enrollment, 4, 6, 12 months of age | Fecal microbiome and metabolome | NA | (1) Fecal metabolome of EF-fed infants showed a significant reduction of lactate, succinate, amino acids, and their derivatives compared to SF-fed infants (2) Introduction of weaning food with either human milk or infant formula reduces the distinct characteristics of breastfed or formula-fed infant fecal microbiome and metabolome profiles |
| Breij et al. [22] (Belgium, France, the Netherlands, Singapore) 2019 | Double-blind RCT PP analysis | Healthy, term infants (gestational age 37–42), postnatal age ≤35 d, at birth weight between 10th and 90th percentiles | Inclusion: 313 infants - 115 EF - 108 SF - 88 BF Completed: 76% of infants - 76% EF - 75% SF - 78% BF | Intervention: Experimental formula comprising large, milk phospholipid-coated dairy lipid droplets Duration: From enrollment: ≤35 days of age to 17 weeks of age | (1) Standard formula with small lipid droplets containing vegetable oils (2) Breastfeeding (reference group) | Baseline visit (≤35 day of age), 5, 8, 13, 17 weeks of age | Daily weight gain until 17 weeks of age | (1) Anthropometric measurements (2) Formula intake (3) Tolerance (4) Stool characteristics (5) Fat-soluble vitamins in plasma (6) Adverse events | (1) No relevant differences were observed in growth in all groups (2) Lower percentage of subjects with the atopic eczema in the EF compared with the SF group (p = 0.03) (3) No differences in plasma A and E vitamins concentration (p = 0.423, p = 0.62 respectively) |
| Li X et al. [13] (China) 2019 | Double-blind RCT ITT analysis | Healthy infants aged 21 ± 7 days with gestational age of 37–42 weeks at birth, birth weight >2500 g and <4000 g | Inclusion: 789 infants: - 192 EF - 195 PF - 194 SF - 208 BF Completed: 87% of infants - 87% EF - 88% PF - 86% SF - 86% BF | Intervention: (1) Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) (2) Milk formula supplemented with L. paracasei strain F19 (Chr. Hansen) Duration: From enrollment (21 ± 7 days) until 4 months of age | (1) Standard formula (2) Breastfeeding (reference group) | At baseline and at 1, 2, 3, 4, 5, 6, 9, and 12 month of age | Incidence of infections, diarrhea episodes and days with fever | (1) Anthropometric measurements (2) Safety and tolerability | (1) Mean weight for the breastfed group was significantly higher than for the F19 group until age 2 months (p = 0.015 and 0.028 at 1 and 2 months, respectively) and for the SF and MFGM groups until age 4 months (all p < 0.041). After these ages’ infants showed no significant differences (2) Compared to the breastfed group, the SF infants had significantly more fever episodes (p = 0.021) and days with fever (p = 0.036), but not episodes of diarrhoea (3) Neither the MFGM nor the F19 groups had significantly more episodes of fever or number of days with fever than the breastfed group |
| Li F et al. [27] (China) 2019 | Double-blind RCT ITT analysis | Healthy, full-term infants, 10–14 days of age at randomization, exclusively formula fed for at least 3 days before randomization, birth weight of 2500–4000 g, singleton birth | Inclusion: 451 infants - 223 EF - 228 SF Completed: 65% - 65% EF - 65% SF | Intervention: Experimental formula supplemented with protein-rich bovine MFGM (Lacprodan MFGM-10, Arla Foods Ingredients) and bovine lactoferrin Duration: From 10–14 day of age until 365 day of age | Standard formula | (1) Bayley-III at day 365 and 545, (2) Anthropometric measurements at day 30, 42, 60, 90, and 120 | Cognitive level at day 365 (age of infant) | (1) Anthropometric measurements (2) Medically confirmed adverse events (3) Cognitive level at day 545 (4) Other instruments for child’s development at various time points | (1) Higher scores in cognitive (p < 0.01), motor (p < 0.01), and language functions (p < 0.01) in MFGM group at day 365 (2) No group differences were detected (adjusted or unadjusted) in any Bayley-III domain in participants tested at day 545 (3) Lower rate of respiratory and gastrointestinal AEs in MFGM + lactoferrin group; no differences in eczema occurrence |
| Nieto-Ruiz et al. [20] (Spain) 2019 | Double-blind RCT PP analysis | Healthy 0–2-month-old full-term infants w/adequate birth weight for gestational age, normal Apgar score | Inclusion: 220 infants: - 85 EF - 85 SF - 50 BF Completed: 64% of infants - 66% EF - 56% SF - 76% BF | Intervention: EF containing LCPUFAs AA, DHA, MFGM, symbiotics, gangliosides, nucleotides, and sialic acid Duration: From 0–2 month up to 18 months of age | (1) Standard formula (2) Breastfeeding (reference group) | (1) Baseline, 2, 3, 4, 6, 12, 18 months of age for anthropometric evaluation (2) Neurological development assessment at 2, 3, 4, and 12 months of age | (1) Weight, length, and subsequent body mass index (BMI) (2) Neurological Development (3) Visual Function | NA | (1) All infants presented an adequate neurological development up to 4 months of life, and no statistically significant differences were found between all the groups at any point in time |
| Nieto-Ruiz et al. [21] (Spain) 2020z | Double-blind RCT PP analysis | Healthy 0–2-month-old full-term infants w/adequate birth weight for gestational age, normal Apgar score | Inclusion: 220 infants: - 85 EF - 85 SF - 50 BF Completed: 55% of infants - 50% EF - 54% SF - 66% BF | Intervention: EF containing LCPUFAs AA, DHA, MFGM, symbiotics, gangliosides, nucleotides and sialic acid Duration: From 0–2 months old up to 18 months of age | (1) Standard formula (2) Breastfeeding (reference group) | At 4 years of age | Assessments of oral language development in kindergarten children | NA | (1) Children who received EF seemed to show higher scores in the use of language (p = 0.033) and oral spontaneous expression (p = 0.024) than children who received SF (2) SF children presented lower scores in language content (p = 0.026) and total score of PLON-R test (p = 0.029) compared to BF children in an unadjusted model. After adjustment for selected confounding variables differences disappeared |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gila-Diaz, A.; Arribas, S.M.; Algara, A.; Martín-Cabrejas, M.A.; López de Pablo, Á.L.; Sáenz de Pipaón, M.; Ramiro-Cortijo, D. A Review of Bioactive Factors in Human Breastmilk: A Focus on Prematurity. Nutrients 2019, 11, 1307. [Google Scholar] [CrossRef] [Green Version]
- Howie, P.W.; Forsyth, J.S.; Ogston, S.A.; Clark, A.; Florey, C.D. Protective effect of breast feeding against infection. BMJ 1990, 300, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Saarinen, U.M.; Kajosaari, M. Breastfeeding as prophylaxis against atopic disease: Prospective follow-up study until 17 years old. Lancet 1995, 346, 1065–1069. [Google Scholar] [CrossRef]
- German, J.B. Dietary lipids from an evolutionary perspective: Sources, structures and functions. Matern. Child Nutr. 2011, 7 (Suppl. 2), 2–16. [Google Scholar] [CrossRef] [PubMed]
- Demmelmair, H.; Koletzko, B. Lipids in human milk. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 57–68. [Google Scholar] [CrossRef]
- Manoni, M.; Di Lorenzo, C.; Ottoboni, M.; Tretola, M.; Pinotti, L. Comparative Proteomics of Milk Fat Globule Membrane (MFGM) Proteome across Species and Lactation Stages and the Potentials of MFGM Fractions in Infant Formula Preparation. Foods 2020, 9, 1251. [Google Scholar] [CrossRef] [PubMed]
- Norris, G.H.; Milard, M.; Michalski, M.-C.; Blesso, C.N. Protective properties of milk sphingomyelin against dysfunctional lipid metabolism, gut dysbiosis, and inflammation. J. Nutr. Biochem. 2019, 73, 108224. [Google Scholar] [CrossRef] [PubMed]
- Hernell, O.; Timby, N.; Domellöf, M.; Lönnerdal, B. Clinical Benefits of Milk Fat Globule Membranes for Infants and Children. J. Pediatr. 2016, 173, S60–S65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Timby, N.; Domellöf, E.; Hernell, O.; Lönnerdal, B.; Domellöf, M. Neurodevelopment, nutrition, and growth until 12 mo of age in infants fed a low-energy, low-protein formula supplemented with bovine milk fat globule membranes: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 860–868. [Google Scholar] [CrossRef] [Green Version]
- Billeaud, C.; Puccio, G.; Saliba, E.; Guillois, B.; Vaysse, C.; Pecquet, S.; Steenhout, P. Safety and tolerance evaluation of milk fat globule membrane-enriched infant formulas: A randomized controlled multicenter non-inferiority trial in healthy term infants. Clin. Med. Insights Pediatr. 2014, 8, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Peng, Y.; Li, Z.; Christensen, B.; Heckmann, A.B.; Stenlund, H.; Lönnerdal, B.; Hernell, O. Feeding Infants Formula with Probiotics or Milk Fat Globule Membrane: A Double-Blind, Randomized Controlled Trial. Front. Pediatr. 2019, 7, 347. [Google Scholar] [CrossRef] [PubMed]
- Timby, N.; Lönnerdal, B.; Hernell, O.; Domellöf, M. Cardiovascular risk markers until 12 mo of age in infants fed a formula supplemented with bovine milk fat globule membranes. Pediatr. Res. 2014, 76, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timby, N.; Hernell, O.; Vaarala, O.; Melin, M.; Lönnerdal, B.; Domellöf, M. Infections in infants fed formula supplemented with bovine milk fat globule membranes. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Timby, N.; Domellöf, M.; Holgerson, P.L.; West, C.E.; Lönnerdal, B.; Hernell, O.; Johansson, I. Oral Microbiota in Infants Fed a Formula Supplemented with Bovine Milk Fat Globule Membranes—A Randomized Controlled Trial. PLoS ONE 2017, 12, e0169831. [Google Scholar] [CrossRef]
- Grip, T.; Dyrlund, T.S.; Ahonen, L.; Domellöf, M.; Hernell, O.; Hyötyläinen, T.; Knip, M.; Lönnerdal, B.; Orešič, M.; Timby, N. Serum, plasma and erythrocyte membrane lipidomes in infants fed formula supplemented with bovine milk fat globule membranes. Pediatr. Res. 2018, 84, 726–732. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Parenti, M.; Grip, T.; Domellöf, M.; Lönnerdal, B.; Hernell, O.; Timby, N.; Slupsky, C.M. Metabolic phenotype of breast-fed infants, and infants fed standard formula or bovine MFGM supplemented formula: A randomized controlled trial. Sci. Rep. 2019, 9, 339. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Parenti, M.; Grip, T.; Lönnerdal, B.; Timby, N.; Domellöf, M.; Hernell, O.; Slupsky, C.M. Fecal microbiome and metabolome of infants fed bovine MFGM supplemented formula or standard formula with breast-fed infants as reference: A randomized controlled trial. Sci. Rep. 2019, 9, 11589. [Google Scholar] [CrossRef] [Green Version]
- Nieto-Ruiz, A.; García-Santos, J.A.; Bermúdez, M.G.; Herrmann, F.; Diéguez, E.; Sepúlveda-Valbuena, N.; García, S.; Miranda, M.T.; De-Castellar, R.; Rodríguez-Palmero, M.; et al. Cortical Visual Evoked Potentials and Growth in Infants Fed with Bioactive Compounds-Enriched Infant Formula: Results from COGNIS Randomized Clinical Trial. Nutrients 2019, 11, 2456. [Google Scholar] [CrossRef] [Green Version]
- Nieto-Ruiz, A.; Diéguez, E.; Sepúlveda-Valbuena, N.; Catena, E.; Jiménez, J.; Rodríguez-Palmero, M.; Catena, A.; Miranda, M.T.; García-Santos, J.A.; Bermúdez, M.G.; et al. Influence of a Functional Nutrients-Enriched Infant Formula on Language Development in Healthy Children at Four Years Old. Nutrients 2020, 12, 535. [Google Scholar] [CrossRef] [Green Version]
- Breij, L.M.; Abrahamse-Berkeveld, M.; Vandenplas, Y.; Jespers, S.N.J.; de Mol, A.C.; Khoo, P.C.; Kalenga, M.; Peeters, S.; van Beek, R.H.T.; Norbruis, O.F.; et al. An infant formula with large, milk phospholipid-coated lipid droplets containing a mixture of dairy and vegetable lipids supports adequate growth and is well tolerated in healthy, term infants. Am. J. Clin. Nutr. 2019, 109, 586–596. [Google Scholar] [CrossRef] [PubMed]
- Veereman-Wauters, G.; Staelens, S.; Rombaut, R.; Dewettinck, K.; Deboutte, D.; Brummer, R.-J.; Boone, M.; Le Ruyet, P. Milk fat globule membrane (INPULSE) enriched formula milk decreases febrile episodes and may improve behavioral regulation in young children. Nutrition 2012, 28, 749–752. [Google Scholar] [CrossRef]
- Zavaleta, N.; Kvistgaard, A.S.; Graverholt, G.; Respicio, G.; Guija, H.; Valencia, N.; Lönnerdal, B. Efficacy of an MFGM-enriched complementary food in diarrhea, anemia, and micronutrient status in infants. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Gurnida, D.A.; Rowan, A.M.; Idjradinata, P.; Muchtadi, D.; Sekarwana, N. Association of complex lipids containing gangliosides with cognitive development of 6-month-old infants. Early Hum. Dev. 2012, 88, 595–601. [Google Scholar] [CrossRef]
- Poppitt, S.D.; McGregor, R.A.; Wiessing, K.R.; Goyal, V.K.; Chitkara, A.J.; Gupta, S.; Palmano, K.; Kuhn-Sherlock, B.; McConnell, M.A. Bovine complex milk lipid containing gangliosides for prevention of rotavirus infection and diarrhoea in northern Indian infants. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 167–171. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Wu, S.S.; Berseth, C.L.; Harris, C.L.; Richards, J.D.; Wampler, J.L.; Zhuang, W.; Cleghorn, G.; Rudolph, C.D.; Liu, B.; et al. Improved Neurodevelopmental Outcomes Associated with Bovine Milk Fat Globule Membrane and Lactoferrin in Infant Formula: A Randomized, Controlled Trial. J. Pediatr. 2019, 215, 24–31. [Google Scholar] [CrossRef]
- Fung, T.C.; Olson, C.A.; Hsiao, E.Y. Interactions between the microbiota, immune and nervous systems in health and disease. Nat. Neurosci. 2017, 20, 145–155. [Google Scholar] [CrossRef]
- Budden, K.F.; Gellatly, S.L.; Wood, D.L.A.; Cooper, M.A.; Morrison, M.; Hugenholtz, P.; Hansbro, P.M. Emerging pathogenic links between microbiota and the gut–lung axis. Nat. Rev. Microbiol. 2017, 15, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Sprong, R.C.; Hulstein, M.F.; Lambers, T.T.; van der Meer, R. Sweet buttermilk intake reduces colonisation and translocation of Listeria monocytogenes in rats by inhibiting mucosal pathogen adherence. Br. J. Nutr. 2012, 108. [Google Scholar] [CrossRef] [Green Version]
- Snow, D.R.; Ward, R.E.; Olsen, A.; Jimenez-Flores, R.; Hintze, K.J. Membrane-rich milk fat diet provides protection against gastrointestinal leakiness in mice treated with lipopolysaccharide. J. Dairy Sci. 2011, 94, 2201–2212. [Google Scholar] [CrossRef] [Green Version]
- Moukarzel, S.; Dyer, R.A.; Garcia, C.; Wiedeman, A.M.; Boyce, G.; Weinberg, J.; Keller, B.O.; Elango, R.; Innis, S.M. Milk Fat Globule Membrane Supplementation in Formula-Fed Rat Pups Improves Reflex Development and May Alter Brain Lipid Composition. Sci. Rep. 2018, 8, 15277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Z.; Li, Y.; Niu, Y.; Tang, Q.; Wu, J. Milk Fat Globule Membrane Enhances Colonic–Mucus-Barrier Function in a Rat Model of Short-Bowel Syndrome. J. Parenter. Enter. Nutr. 2020, jpen.1956. [Google Scholar] [CrossRef] [PubMed]
- Bhinder, G.; Allaire, J.M.; Garcia, C.; Lau, J.T.; Chan, J.M.; Ryz, N.R.; Bosman, E.S.; Graef, F.A.; Crowley, S.M.; Celiberto, L.S.; et al. Milk Fat Globule Membrane Supplementation in Formula Modulates the Neonatal Gut Microbiome and Normalizes Intestinal Development. Sci. Rep. 2017, 7, 45274. [Google Scholar] [CrossRef] [PubMed]
- Neu, J.; Walker, W.A. Necrotizing Enterocolitis. N. Engl. J. Med. 2011, 364, 255–264. [Google Scholar] [CrossRef] [Green Version]
- Sammons, J.S.; Toltzis, P.; Zaoutis, T.E. Clostridium difficile Infection in Children. JAMA Pediatr. 2013, 167, 567. [Google Scholar] [CrossRef] [Green Version]
- Na, J.Y.; Park, J.M.; Lee, K.S.; Kang, J.O.; Oh, S.H.; Kim, Y.J. Clinical Characteristics of Symptomatic Clostridium difficile Infection in Children: Conditions as Infection Risks and Whether Probiotics Is Effective. Pediatr. Gastroenterol. Hepatol. Nutr. 2014, 17, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appleton, J.; Russell, C.G.; Laws, R.; Fowler, C.; Campbell, K.; Denney-Wilson, E. Infant formula feeding practices associated with rapid weight gain: A systematic review. Matern. Child Nutr. 2018, 14, e12602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azad, M.B.; Vehling, L.; Chan, D.; Klopp, A.; Nickel, N.C.; McGavock, J.M.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; Moraes, T.J.; et al. Infant Feeding and Weight Gain: Separating Breast Milk from Breastfeeding and Formula from Food. Pediatrics 2018, 142, e20181092. [Google Scholar] [CrossRef] [Green Version]
- Dziechciarz, P.; Horvath, A.; Szajewska, H. Effects of n-3 long-chain polyunsaturated fatty acid supplementation during pregnancy and/or lactation on neurodevelopment and visual function in children: A systematic review of randomized controlled trials. J. Am. Coll. Nutr. 2010, 29, 443–454. [Google Scholar] [CrossRef]
- Taylor, R.M.; Fealy, S.M.; Bisquera, A.; Smith, R.; Collins, C.E.; Evans, T.-J.; Hure, A.J. Effects of Nutritional Interventions during Pregnancy on Infant and Child Cognitive Outcomes: A Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Y.; Cao, L.; Yu, J. Prophylactic lactoferrin for preventing late-onset sepsis and necrotizing enterocolitis in preterm infants: A PRISMA-compliant systematic review and meta-analysis. Medicine 2018, 97, e11976. [Google Scholar] [CrossRef] [PubMed]
- Toro-Campos, R.; Algarín, C.; Peirano, P.; Peña, M.; Murguia-Peniche, T.; Wu, S.S.; Uauy, R. Effect of feeding mode on infant growth and cognitive function: Study protocol of the Chilean infant Nutrition randomized controlled Trial (ChiNuT). BMC Pediatr. 2020, 20, 225. [Google Scholar] [CrossRef] [PubMed]



| Protocol ID, Trial Registry | Location | Title | Recruitment Status | Estimated Completion Date |
|---|---|---|---|---|
| NCT04508257, ClinicalTrials.gov | China, Zhejiang | The Effect of a New Infant Formula on Growth and Cognition in Healthy Term Infants | Currently Recruiting | 28 February 2023 |
| ACTRN12620000552987, ANZCTR.org.au | Australia | Infant nutrition with milk fat globule membrane for infant cognition in early life | Not Yet Recruiting/Currently Recruiting | 23 March 2024 |
| NCT02626143, ClinicalTrials.gov, BMC Pediatrics [43] | Chile | Effect of feeding mode on infant growth and cognitive function: study protocol of the Chilean infant Nutrition randomized controlled Trial (ChiNuT) | Recruitment Completed | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ambrożej, D.; Dumycz, K.; Dziechciarz, P.; Ruszczyński, M. Milk Fat Globule Membrane Supplementation in Children: Systematic Review with Meta-Analysis. Nutrients 2021, 13, 714. https://doi.org/10.3390/nu13030714
Ambrożej D, Dumycz K, Dziechciarz P, Ruszczyński M. Milk Fat Globule Membrane Supplementation in Children: Systematic Review with Meta-Analysis. Nutrients. 2021; 13(3):714. https://doi.org/10.3390/nu13030714
Chicago/Turabian StyleAmbrożej, Dominika, Karolina Dumycz, Piotr Dziechciarz, and Marek Ruszczyński. 2021. "Milk Fat Globule Membrane Supplementation in Children: Systematic Review with Meta-Analysis" Nutrients 13, no. 3: 714. https://doi.org/10.3390/nu13030714
APA StyleAmbrożej, D., Dumycz, K., Dziechciarz, P., & Ruszczyński, M. (2021). Milk Fat Globule Membrane Supplementation in Children: Systematic Review with Meta-Analysis. Nutrients, 13(3), 714. https://doi.org/10.3390/nu13030714