
Relationship between the Gut Microbiome and Osteoarthritis Pain: Review of the Literature

 ,
,  ,
, 
 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.2.1. Type of Studies
2.2.2. Type of Participants
2.2.3. Data Extraction
2.2.4. Quality Assessment
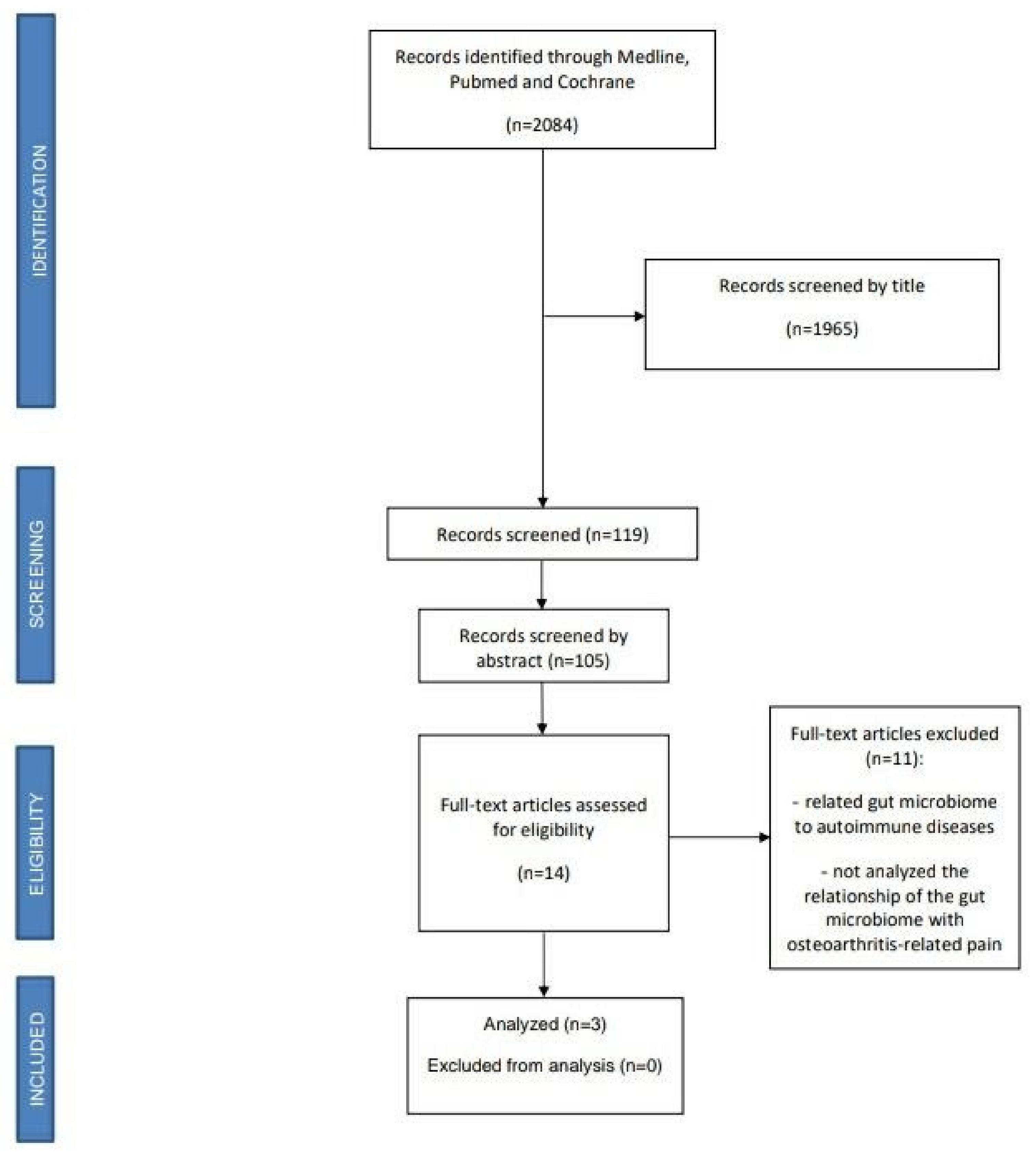
2.2.5. Study Selection
3. Results
3.1. Study Characteristics
3.2. Risk of Bias within Studies
3.3. Data from Studies
3.3.1. Association between Microbiome and OA-Related Pain in Articles with Intervention
3.3.2. Association between Microbiome and OA-Related Pain in Articles without Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287. [Google Scholar] [CrossRef]
- Collins, J.; Katz, J.; Dervan, E.; Losina, E. Trajectories and risk profiles of pain in persons with radiographic, symptomatic knee osteoarthritis: Data from the osteoarthritis initiative. Osteoarthr. Cartil. 2014, 22, 622–630. [Google Scholar] [CrossRef] [Green Version]
- Clauw, D.J.; Hassett, A.L. The role of centralised pain in osteoarthritis. Clin. Exp. Rheumatol. 2017, 107, 79–84. [Google Scholar]
- Villafañe, J.H.; Cleland, J.A.; Fernández-De-Las-Peñas, C. Bilateral Sensory Effects of Unilateral Passive Accessory Mobilization in Patients with Thumb Carpometacarpal Osteoarthritis. J. Manip. Physiol. Ther. 2013, 36, 232–237. [Google Scholar] [CrossRef]
- Villafañe, J.H.; Valdes, K.; Pedersini, P.; Berjano, P. Osteoarthritis: A call for research on central pain mechanism and personalized prevention strategies. Clin. Rheumatol. 2018, 38, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L. Pain sensitisation in osteoarthritis. Clin. Exp. Rheumatol. 2017, 107, 68–74. [Google Scholar]
- Ji, R.R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef] [PubMed]
- Link, T.M.; Steinbach, L.S.; Ghosh, S.; Ries, M.; Lu, Y.; Lane, N.; Majumdar, S. Osteoarthritis: MR Imaging Findings in Different Stages of Disease and Correlation with Clinical Findings. Radiology 2003, 226, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis: Classification of osteoarthritis of the knee. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Biver, E.; Berenbaum, F.; Valdes, A.M.; De Carvalho, I.A.; Bindels, L.B.; Brandi, M.L.; Calder, P.C.; Castronovo, V.; Cavalier, E.; Cherubini, A.; et al. Gut microbiota and osteoarthritis management: An expert consensus of the European society for clinical and economic aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO). Ageing Res. Rev. 2019, 55, 100946. [Google Scholar] [CrossRef]
- Sonnenburg, E.D.; Sonnenburg, J.L. The ancestral and industrialized gut microbiota and implications for human health. Nat. Rev. Genet. 2019, 17, 383–390. [Google Scholar] [CrossRef]
- A Gilbert, J.; Blaser, M.J.; Caporaso, J.G.; Jansson, J.K.; Lynch, S.V.; Knight, R. Current understanding of the human microbiome. Nat. Med. 2018, 24, 392–400. [Google Scholar] [CrossRef]
- Szychlinska, M.A.; di Rosa, M.; Castorina, A.; Mobasheri, A.; Musumeci, G. A correlation between intestinal microbiota dysbiosis and osteoarthritis. Heliyon 2019, 5, e01134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Hunter, D.; Xu, J.; Ding, C. Metabolic triggered inflammation in osteoarthritis. Osteoarthr. Cartil. 2015, 23, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Ding, W.; Wang, H.; Dai, L.; Zong, W.; Wang, Y.; Bi, J.; Han, W.; Dong, G. Gut microbiota and obesity-associated osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1257–1265. [Google Scholar] [CrossRef]
- Wang, J.; Gu, X.; Yang, J.; Wei, Y.; Zhao, Y. Gut Microbiota Dysbiosis and Increased Plasma LPS and TMAO Levels in Patients with Preeclampsia. Front. Cell. Infect. Microbiol. 2019, 9, 409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, S.M.; Surette, M.G.; Bercik, P. The interplay between the intestinal microbiota and the brain. Nat. Rev. Genet. 2012, 10, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Turroni, S.; Pedersini, P.; Villafañe, J.H. The Human Gut Microbiome and Its Relationship with Osteoarthritis Pain. Pain Med. 2020. [Google Scholar] [CrossRef]
- Favazzo, L.J.; Hendesi, H.; Villani, D.A.; Soniwala, S.; Dar, Q.-A.; Schott, E.M.; Gill, S.R.; Zuscik, M.J. The gut microbiome-joint connection: Implications in osteoarthritis. Curr. Opin. Rheumatol. 2020, 32, 92–101. [Google Scholar] [CrossRef]
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; the PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2016, 354, i4086. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 2011. Available online: https://handbook-5-1.cochrane.org/ (accessed on 23 February 2021).
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Coulson, S.; Butt, H.; Vecchio, P.; Gramotnev, H.; Vitetta, L. Green-lipped mussel extract (Perna canaliculus) and glucosamine sulphate in patients with knee osteoarthritis: Therapeutic efficacy and effects on gastrointestinal microbiota profiles. Inflammopharmacology 2013, 21, 79–90. [Google Scholar] [CrossRef]
- Boer, C.G.; Radjabzadeh, D.; Medina-Gomez, C.; Garmaeva, S.; Schiphof, D.; Arp, P.; Koet, T.; Kurilshikov, A.; Fu, J.; Ikram, M.A.; et al. Intestinal microbiome composition and its relation to joint pain and inflammation. Nat. Commun. 2019, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Z.; Stabler, T.; Pei, F.; Kraus, V.B. Both systemic and local lipopolysaccharide (LPS) burden are associated with knee OA severity and inflammation. Osteoarthr. Cartil. 2016, 24, 1769–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepankova, R.; Powrie, F.; Kofronova, O.; Kozakova, H.; Hudcovic, T.; Hrncir, T.; Uhlig, H.; Read, S.; Rehakova, Z.; Benada, O.; et al. Segmented filamentous bacteria in a defined bacterial cocktail induce intestinal inflammation in SCID mice reconstituted with CD45RBhigh CD4+ T cells. Inflamm. Bowel Dis. 2007, 13, 1202–1211. [Google Scholar] [CrossRef]
- Wu, H.-J.; Ivanov, I.I.; Darce, J.; Hattori, K.; Shima, T.; Umesaki, Y.; Littman, D.R.; Benoist, C.; Mathis, D. Gut-Residing Segmented Filamentous Bacteria Drive Autoimmune Arthritis via T Helper 17 Cells. Immunity 2010, 32, 815–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Author, Year | Aim of the Study | Study Design | ParticiPants | Treatment | Outcome Measures | Reported Results |
|---|---|---|---|---|---|---|
| Coulson et al. (2013) [24] | Evaluate how the efficacy of nutraceuticals in treating OA may be altered according to the different microbiota profiles of the gastrointestinal tract and allow the formulation of a hypothesis that partly explains the inconsistent and controversial results of osteoarthritis (OA) clinical studies with green-lipped mussel (GLM) and glucosamine. | Clinical trial | 40 patients (29 women) Mean age: 58.6 ± 8.9 years Inclusion criteria: Patients with knee OA eligible for ACR. | 3000 mg/day green-lipped mussel extract (GLM) or 3000 mg/day glucosamine sulphate for 12 weeks. | - Microbiota analysis in feces (T0 and T12) through viable plate counting and MALDI-TOF mass spectrometry-based colony identification. - WOMAC, Lequesne algofunctional index, SF12 score (quality of life) measure and GSRS (T0, T6 and T12) - Other: BP, height, BMI, WHI and CRP. | Results Significant improvement (p < 0.05) in all WOMAC [pain, stiffness, flexibility and function] and GSRS measures. Although without significant changes in the microbiota, in both groups ↓ Clostridium and Staphylococcus and ↑ Lactobacillus, Streptococcus and Eubacterium. In the GLM group ↑ Bifidobacterium and ↓ Enterococcus and yeasts. In the GS group ↓ Bacteroides and ↑ yeasts and coliforms, most notably Escherichia coli. |
| Boer et al. (2019) [25] | Verify the relationship between joint pain and the composition of the gastrointestinal microbiome, and knee pain related to osteoarthritis in the Rotterdam Study. | Case-Control | 1427 patients (821 women) Mean age: 56.8 ± 5.9 years Inclusion criteria: Patients with knee OA (cases) and without knee OA (controls) from Rotterdam Study. | - | -- 16S rRNA gene-based Illumina sequencing for microbiome profiling. - WOMAC Index. | Results - Microbiome ß-diversity was significantly associated with knee WOMAC scores. - A greater relative abundance of Streptococcus was found in individuals with higher pain values on the WOMAC scale, regardless of tobacco, alcohol consumption and BMI. - There was a significant association between the relative abundance of Streptococcus spp. and knee WOMAC-pain scores (p = 1.4 × 10−4). This association was robust and driven by local inflammation in the knee joint. |
| Huang et al. (2016) [26] | To analyze the relationship of lipopolysaccharide (LPS), a decisive proinflammatory product of the microbiome, with the level of inflammation, symptoms and radiographic alterations in osteoarthritis of the knee. | Cohort study | 25 patients from the Etarfolatide cohort (18 women) Mean age: 62.4.1 ± 15.8 years Inclusion criteria: radiographic knee OA (unilateral or bilateral [K/L] grade 1–4). | - | - LPS was measured using the EndoZyme Assay (recombinant factor C based), carefully optimized for systemic and synovial fluid analyses. - LBP was tested in both serum and synovial fluid for association with OA phenotypic outcomes (commercial sandwich ELISA kit). - Models were adjusted for age, gender and BMI. - WOMAC Index. | Results - Serum LPS and LBP were associated with the abundance of activated macrophages in the knee joint capsule (p = 0.01) and synovium (p = 0.036). - SF LPS and LBP were associated with the abundance of activated macrophages in the synovium (p = 0.001 and p = 0.021, respectively). - Serum LPS, LBP and SF LPS were associated with knee osteophyte severity (p = 0.030, p = 0.017 and p = 0.001, respectively). - SF LPS was positively associated with knee joint space narrowing severity (p < 0.001) and total WOMAC score (p = 0.008). - Serum LBP tended to show a positive association with knee pain score (p = 0.076). - SF LBP was significantly associated with self-reported knee pain score (p = 0.039). - Both LPS and LBP concentrations were significantly lower in SF than in paired serum (p < 0.0001). - Serum LPS and LBP concentrations were highly correlated (p < 0.001) and individually correlated with BMI (p < 0.017) and plasma sCD14 (p < 0.001). |
| Bias AnalysisTtable for RCTs (Cochrane Collaboration) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AUTHORS | Selection bias | Realization bias | Detection bias | Wear bias | Notification bias | Others | OUTCOME | |||||
| Coulson et al. (2012) [24] | Yes | Yes | No | No | No | No | 2 | |||||
| Scale “Physiotherapy Evidence Database (PEDro)” to analyze the methodological quality of clinical studies | ||||||||||||
| AUTHORS | Specified selection criteria | Randomization | Hidden assignment | Similar groups to start | Blinded patients | Blinded therapists | Blinded raters | Outcomes 85% | Treatment or intention to treat | Comparison between groups | Point measures variability | OUTCOME |
| Coulson et al. (2012) [24] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Methodological Index for Nonrandomized Studies (MINORS) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AUTHORS | Clearly stated aim | Inclusion of consecutive patients | Prospective collection of data | Endpoints appropriate to the aim of the study | Unbiased assessment of the study endpoint | Follow-up period appropriate to the aim of the study | Loss to follow up less than 5% | Prospective calculation of the study size | Adequate control group | Contemporary groups | Baseline equivalence of groups | Adequate statistical analyses | OUTCOME |
| Boer et al. (2019) [25] | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 2 | 1 | 2 | 1 | 2 | 18 |
| Huang et al. (2016) [26] | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 2 | 0 | 0 | 0 | 2 | 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez Romero, E.A.; Meléndez Oliva, E.; Alonso Pérez, J.L.; Martín Pérez, S.; Turroni, S.; Marchese, L.; Villafañe, J.H. Relationship between the Gut Microbiome and Osteoarthritis Pain: Review of the Literature. Nutrients 2021, 13, 716. https://doi.org/10.3390/nu13030716
Sánchez Romero EA, Meléndez Oliva E, Alonso Pérez JL, Martín Pérez S, Turroni S, Marchese L, Villafañe JH. Relationship between the Gut Microbiome and Osteoarthritis Pain: Review of the Literature. Nutrients. 2021; 13(3):716. https://doi.org/10.3390/nu13030716
Chicago/Turabian StyleSánchez Romero, Eleuterio A., Erika Meléndez Oliva, José Luis Alonso Pérez, Sebastián Martín Pérez, Silvia Turroni, Lorenzo Marchese, and Jorge Hugo Villafañe. 2021. "Relationship between the Gut Microbiome and Osteoarthritis Pain: Review of the Literature" Nutrients 13, no. 3: 716. https://doi.org/10.3390/nu13030716
APA StyleSánchez Romero, E. A., Meléndez Oliva, E., Alonso Pérez, J. L., Martín Pérez, S., Turroni, S., Marchese, L., & Villafañe, J. H. (2021). Relationship between the Gut Microbiome and Osteoarthritis Pain: Review of the Literature. Nutrients, 13(3), 716. https://doi.org/10.3390/nu13030716