
The Joint Effects of Diet and Dietary Supplements in Relation to Obesity and Cardiovascular Disease over a 10-Year Follow-Up: A Longitudinal Study of 69,990 Participants in Australia

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
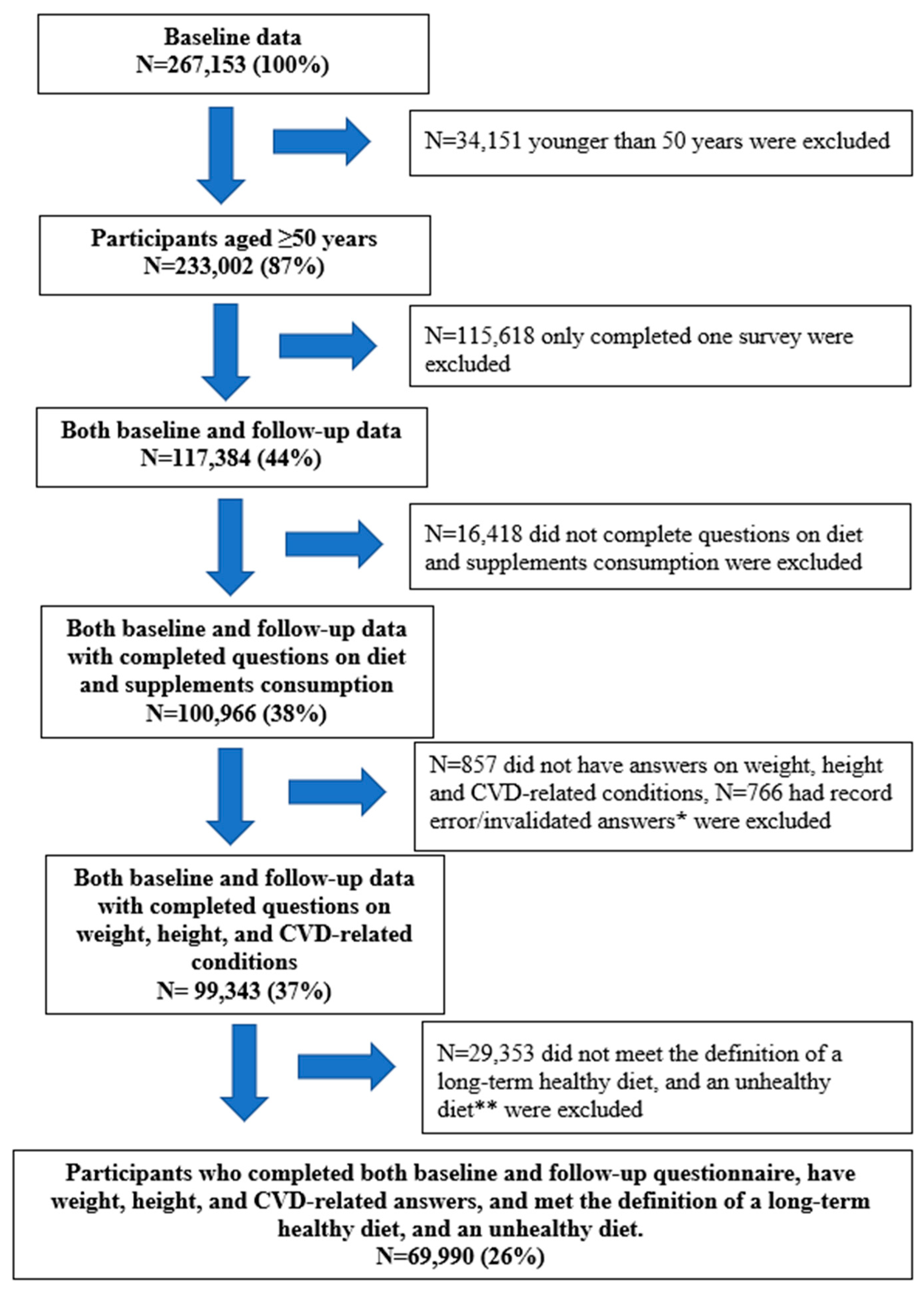
2.1. Study Design
2.2. Outcomes
2.3. Long-Term Dietary Consumption
2.4. Dietary Supplements
2.5. Joint Effects of Diet and Supplements
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Diet, Dietary Supplements, and Obesity and/or CVD
3.3. The Joint Effects of Diet and Supplements in Relation to Obesity and/or CVD
3.4. Sensitivity Analysis
3.5. Post hoc Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Disease: Report of a Joint WHO/FAO Expert Geneva. 2003. Available online: http://www.who.int/dietphysicalactivity/publications/trs916/en/ (accessed on 7 September 2016).
- Nguyen, B.; Bauman, A.; Gale, J.; Banks, E.; Kritharides, L.; Ding, D. Fruit and vegetable consumption and all-cause mortality: Evidence from a large Australian cohort study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 9. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- García-Esquinas, E.; Ortolá, R.; Banegas, J.R.; Lopez-García, E.; Rodríguez-Artalejo, F. Dietary n-3 polyunsaturated fatty acids, fish intake and healthy ageing. Int. J. Epidemiol. 2019, 48, 1914–1924. [Google Scholar] [CrossRef] [PubMed]
- Santesso, N.; Akl, E.A.; Bianchi, M.; Mente, A.; Mustafa, R.; Heels-Ansdell, D.; Schünemann, H.J. Effects of higher-versus lower-protein diets on health outcomes: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Ward, E. Addressing nutritional gaps with multivitamin and mineral supplements. Nutr. J. 2014, 13, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, F.; Dickinson, H.O.; Critchley, J.A.; Ford, G.A.; Bradburn, M. A systematic review of fish-oil supplements for the prevention and treatment of hypertension. Eur. J. Prev. Cardiol. 2013, 20, 107–120. [Google Scholar] [CrossRef]
- Grodstein, F.; O’Brien, J.; Kang, J.H.; Dushkes, R.; Cook, N.R.; Okereke, O.; Manson, J.E.; Glynn, R.J.; Buring, J.E.; Gaziano, J.M.; et al. Long-term multivitamin supplementation and cognitive function in men: A randomized trial. Ann. Intern. Med. 2013, 159, 806–814. [Google Scholar] [CrossRef]
- Rautiainen, S.; Manson, J.E.; Lichtenstein, A.H.; Sesso, H.D. Dietary supplements and disease prevention—A global overview. Nat. Rev. Endocrinol. 2016, 12, 407. [Google Scholar] [CrossRef]
- Blumberg, J.B.; Bailey, R.L.; Sesso, H.D.; Ulrich, C.M. The evolving role of multivitamin/multimineral supplement use among adults in the age of personalized nutrition. Nutrients 2018, 10, 248. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Choi, J.; Kwon, S.Y.; McEvoy, J.W.; Blaha, M.J.; Blumenthal, R.S.; Guallar, E.; Zhao, D.; Michos, E.D. Association of multivitamin and mineral supplementation and risk of cardiovascular disease: A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004224. [Google Scholar] [CrossRef]
- Tankeu, A.T.; Ndip Agbor, V.; Noubiap, J. Calcium supplementation and cardiovascular risk: A rising concern. J. Clin. Hypertens 2017, 19, 640–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, M.; Tang, A.M.; Fu, Z.; Wang, D.D.; Newberry, S.J. Calcium intake and cardiovascular disease risk: An updated systematic review and meta-analysis. Ann. Intern. Med. 2016, 165, 856–866. [Google Scholar] [CrossRef] [Green Version]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H. Obesity and cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss: An update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006, 113, 898–918. [Google Scholar] [PubMed] [Green Version]
- Sax Institute. 45 and Up Study 2015. Available online: https://www.saxinstitute.org.au/our-work/45-up-study/ (accessed on 2 March 2018).
- Up Study Collaborators. Cohort profile: The 45 and up study. Int. J. Epidemiol. 2007, 37, 941–947. [Google Scholar]
- Australian Government. Eat for Health: Australian Dietary Guidelines Providing the Scientific Evidence for Healthier Australian Diets; Commonwealth of Australia, National Health and Medical Research Council: Canberra, Australia, 2013.
- National Health and Medical Research Council. Australian Guidelines to Reduce Health Risks from Drinking Alcohol; National Health and Medical Research Council: Canberra, Australia, 2020.
- Xu, X.; Parker, D.; Inglis, S.; Byles, J. Can regular long-term breakfast cereals consumption benefits lower cardiovascular diseases and diabetes risk? A longitudinal population-based study. Ann. Epidemol. 2019, 37, 43–50. [Google Scholar] [CrossRef]
- Xu, X.; Ling, M.; Inglis, S.; Hickman, L.; Parker, D. Eating and healthy ageing: A longitudinal study on the association between food consumption, memory loss and its comorbidities. Int. J. Public Health 2020, 65, 571–582. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Croteau, K.; Kolt, G.S. Influence of neighbourhood ethnic density, diet and physical activity on ethnic differences in weight status: A study of 214,807 adults in Australia. Soc. Sci. Med. 2013, 93, 70–77. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas 2018. Available online: http://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 15 July 2019).
- Ding, D.; Rogers, K.; van der Ploeg, H.; Stamatakis, E.; Bauman, A.E. Traditional and emerging lifestyle risk behaviors and all-cause mortality in middle-aged and older adults: Evidence from a large population-based Australian cohort. PLoS Med. 2015, 12, e1001917. [Google Scholar] [CrossRef] [PubMed]
- The Department of Health. Australia’s Physical Activity and Sedentary Behaviour Guidelines 2017. Available online: http://www.health.gov.au/internet/main/publishing.nsf/content/health-pubhlth-strateg-phys-act-guidelines (accessed on 5 June 2018).
- Barros, A.J.D.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Rautiainen, S.; Rist, P.M.; Glynn, R.J.; Buring, J.E.; Gaziano, J.M.; Sesso, H.D. Multivitamin use and the risk of cardiovascular disease in men. J. Nutr. 2016, 146, 1235–1240. [Google Scholar] [CrossRef]
- Rautiainen, S.; Lee, I.-M.; Rist, P.M.; Gaziano, J.M.; Manson, J.E.; Buring, J.E.; Sesso, H.D. Multivitamin use and cardiovascular disease in a prospective study of women. Am. J. Clin. Nutr. 2015, 101, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Kromhout, D.; Yasuda, S.; Geleijnse, J.M.; Shimokawa, H. Fish oil and omega-3 fatty acids in cardiovascular disease: Do they really work? Eur. Heart J. 2012, 33, 436–443. [Google Scholar] [CrossRef] [Green Version]
- Weitz, D.; Weintraub, H.; Fisher, E.; Schwartzbard, A.Z. Fish oil for the treatment of cardiovascular disease. Cardiol. Rev. 2010, 18, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.; AlAbdulghafoor, F.K.; Summerbell, C.D.; Worthington, H.V.; et al. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2018, 7, CD003177. [Google Scholar] [CrossRef]
- Clar, C.; Al-Khudairy, L.; Loveman, E.; Kelly, S.A.; Hartley, L.; Flowers, N.; Germanò, R.; Frost, G.; Rees, K. Low glycaemic index diets for the prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2017, 7, CD004467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlesinger, S.; Neuenschwander, M.; Schwedhelm, C.; Hoffmann, G.; Bechthold, A.; Boeing, H.; Schwingshackl, L. Food Groups and Risk of Overweight, Obesity, and Weight Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2019, 10, 205–218. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Alvarez, I.; de Rojas, J.P.; Fernandez-Montero, A.; Zazpe, I.; Ruiz-Canela, M.; Hidalgo-Santamaría, M.; Bes-Rastrollo, M.; Martínez-González, M.Á. Strong inverse associations of Mediterranean diet, physical activity and their combination with cardiovascular disease: The Seguimiento Universidad de Navarra (SUN) cohort. Eur. J. Prev. Cardiol. 2018, 25, 1186–1197. [Google Scholar] [CrossRef]
- Soares, M.; Ping-Delfos, W.C.S.; Ghanbari, M.J. Calcium and vitamin D for obesity: A review of randomized controlled trials. Eur. J. Clin. Nutr. 2011, 65, 994–1004. [Google Scholar] [CrossRef] [Green Version]
- Pereira-Santos, M.; Costa, P.R.; Assis, A.M.; Santos, C.A.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Ye, J.; Zhu, X.; Wang, L.; Gao, P.; Shu, G.; Jiang, Q.; Wang, S. Anti-Obesity Effects of Dietary Calcium: The Evidence and Possible Mechanisms. Int. J. Mol. Sci. 2019, 20, 3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, P.; Fan, C.; Lu, Y.; Qi, K. Effects of calcium supplementation on body weight: A meta-analysis. Am. J. Clin. Nutr. 2016, 104, 1263–1273. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Older Australia at a Glance; Australian Institute of Health and Welfare: Canberra, Australia, 2018.
- Kheiri, B.; Abdalla, A.; Osman, M.; Ahmed, S.; Hassan, M.; Bachuwa, G. Vitamin D deficiency and risk of cardiovascular diseases: A narrative review. Clin. Hypertens 2018, 24, 9. [Google Scholar] [CrossRef] [PubMed]
- Burnett, A.J.; Livingstone, K.M.; Woods, J.L.; McNaughton, S.A. Dietary Supplement Use among Australian Adults: Findings from the 2011–2012 National Nutrition and Physical Activity Survey. Nutrients 2017, 9, 1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Baseline | Follow-Up | p Value |
|---|---|---|---|
| N (%) | |||
| Socio-demographic variables | |||
| Age | |||
| 51–70 years | 53,868 (77.0) | 38,384 (54.8) | <0.001 |
| >70 years | 16,122 (23.0) | 31,605 (45.2) | |
| Marital status | |||
| Married/partner | 54,454 (78.2) | 50,762 (73.2) | <0.001 |
| Single/divorce/separated | 10,014 (14.4) | 10,135 (14.6) | |
| Widowed | 5166 (7.4) | 8480 (12.2) | |
| SEIFA * | |||
| Low | 21,269 (31.3) | 23,128 (34.9) | <0.001 |
| Medium | 22,951 (33.7) | 21,715 (32.8) | |
| High | 23,818 (35.0) | 21,291 (32.2) | |
| Sex | |||
| Men | 30,325 (43.3) | 30,326 (43.3) | NA |
| Women | 39,665 (56.7) | 39,665 (56.7) | |
| Country of birth | |||
| Australia | 54,828 (78.8) | 54,828 (78.8) | NA |
| Other countries | 14,742 (21.2) | 14,742 (21.2) | |
| Education ** | |||
| Low | 21,910 (31.6) | 21,910 (31.6) | NA |
| Medium | 29,098 (42.0) | 29,098 (42.0) | |
| High | 18,272 (26.4) | 18,272 (26.4) | |
| Supplements | |||
| Minerals and multivitamins | |||
| No | 51,809 (74.0) | 50,513 (72.2) | <0.001 |
| Yes | 18,181 (26.0) | 19,477 (27.8) | |
| Fish oil, omega 3 | |||
| No | 42,546 (60.8) | 40,103 (57.3) | <0.001 |
| Yes | 27,444 (39.2) | 29,882 (42.7) | |
| Calcium | |||
| No | 62,126 (88.8) | 60,733 (86.8) | <0.001 |
| Yes | 7863 (11.2) | 9254 (13.2) | |
| Conditions or disease | |||
| Body mass index | |||
| Underweight | 693 (1.0) | 893 (1.3) | <0.001 |
| Normal | 23,814 (34.0) | 21,071 (30.1) | |
| Overweight | 26,627 (38.0) | 23,405 (33.4) | |
| Obesity | 18,856 (26.9) | 24,621 (35.2) | |
| CVD | |||
| No | 59,110 (84.5) | 49,534 (70.8) | <0.001 |
| Yes | 10,880 (15.6) | 20,456 (29.2) | |
| Comorbid obesity and CVD | |||
| No | 43,574 (94.4) | 32,657 (88.0) | <0.001 |
| Yes | 2610 (5.6) | 4443 (12.0) | |
| IRR (95% CI) ¶ | ||||
|---|---|---|---|---|
| Obesity (N = 55,654) * | ||||
| Diet | Crude model | Model 2 | Model 3 | Model 4 |
| Healthy | 1.00 | 1.00 | 1.00 | 1.00 |
| Unhealthy | 1.06 (1.00; 1.14) | 1.15 (1.08; 1.24) | 1.09 (1.01; 1.17) | 1.10 (1.02; 1.18) |
| Minerals and Multivitamins | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.97 (0.91; 1.04) | 0.99 (0.92; 1.06) | 0.99 (0.93; 1.06) | 1.03 (0.96; 1.11) |
| Fish oil, omega 3 | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.96 (0.91; 1.02) | 0.96 (0.90; 1.02) | 0.99 (0.93; 1.05) | 1.01 (0.95; 1.07) |
| Calcium | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.94 (0.86; 1.02) | 0.89 (0.81; 0.98) | 0.88 (0.80; 0.97) | 0.83 (0.75; 0.91) |
| CVD (N = 59,110) ** | ||||
| Diet | ||||
| Healthy | 1.00 | 1.00 | 1.00 | 1.00 |
| Unhealthy | 0.98 (0.94; 1.02) | 1.06 (1.02; 1.11) | 1.05 (1.00; 1.10) | 1.03 (0.98; 1.08) |
| Minerals and Multivitamins | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.81 (0.77; 0.85) | 0.92 (0.88; 0.96) | 0.92 (0.87; 0.96) | 0.94 (0.89; 0.99) |
| Fish oil, omega 3 | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.89 (0.86; 0.93) | 0.92 (0.89; 0.96) | 0.93 (0.88; 0.97) | 0.95 (0.91; 0.99) |
| Calcium | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.07 (1.01; 1.13) | 1.09 (1.02; 1.15) | 1.06 (1.00; 1.13) | 1.03 (0.97; 1.11) |
| Obesity and CVD (N = 29,815) § | ||||
| Diet | ||||
| Healthy | 1.00 | 1.00 | 1.00 | 1.00 |
| Unhealthy | 1.10 (0.91; 1.33) | 1.13 (0.91; 1.39) | 1.03 (0.83; 1.28) | 0.99 (0.79; 1.24) |
| Minerals and Multivitamins | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.69 (0.55; 0.85) | 0.78 (0.62; 0.97) | 0.79 (0.64; 0.99) | 0.84 (0.67; 1.06) |
| Fish oil, omega 3 | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.75 (0.63; 0.91) | 0.80 (0.66; 0.98) | 0.85 (0.70; 1.04) | 0.87 (0.71; 1.07) |
| Calcium | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.94 (0.72; 1.23) | 1.00 (0.74; 1.34) | 0.99 (0.74; 1.34) | 0.89 (0.66; 1.21) |
| Incidence of People with Obesity and CVD * | ||||
|---|---|---|---|---|
| IRR (95% CI) ¶ | ||||
| Crude Model | Model 2 | Model 3 | Model 4 | |
| Minerals and multivitamins (N = 29,813) | ||||
| Healthy diet (+), no MVM (–) | 1.00 | 1.00 | 1.00 | 1.00 |
| Healthy diet (+), new MVM (+) | 0.88 (0.64; 1.23) | 1.05 (0.75; 1.46) | 1.07 (0.77; 1.50) | 1.14 (0.82; 1.59) |
| Healthy diet (+), former MVM (+, –) | 1.11 (0.80; 1.53) | 1.23 (0.87; 1.74) | 1.20 (0.84; 1.71) | 1.28 (0.90; 1.82) |
| Healthy diet (+), long-term MVM (+, +) | 0.49 (0.34; 0.71) | 0.55 (0.37; 0.81) | 0.60 (0.38; 0.83) | 0.61 (0.41; 0.91) |
| Unhealthy diet (–), No MVM (–) | 1.11 (0.88; 1.41) | 1.14 (0.88; 1.47) | 1.04 (0.80; 1.35) | 1.00 (0.77; 1.31) |
| Unhealthy diet (–), new MVM (+) | 0.88 (0.54; 1.45) | 0.97 (0.56; 1.67) | 0.85 (0.48; 1.49) | 0.81 (0.44; 1.48) |
| Unhealthy diet (–), former MVM (+, –) | 1.11 (0.68; 1.81) | 1.31 (0.79; 2.18) | 1.22 (0.73; 2.04) | 1.31 (0.78; 2.20) |
| Unhealthy diet (–), long-term MVM (+, +) | 0.62 (0.38; 1.03) | 0.78 (0.46; 1.32) | 0.74 (0.44; 1.26) | 0.78 (0.45; 1.35) |
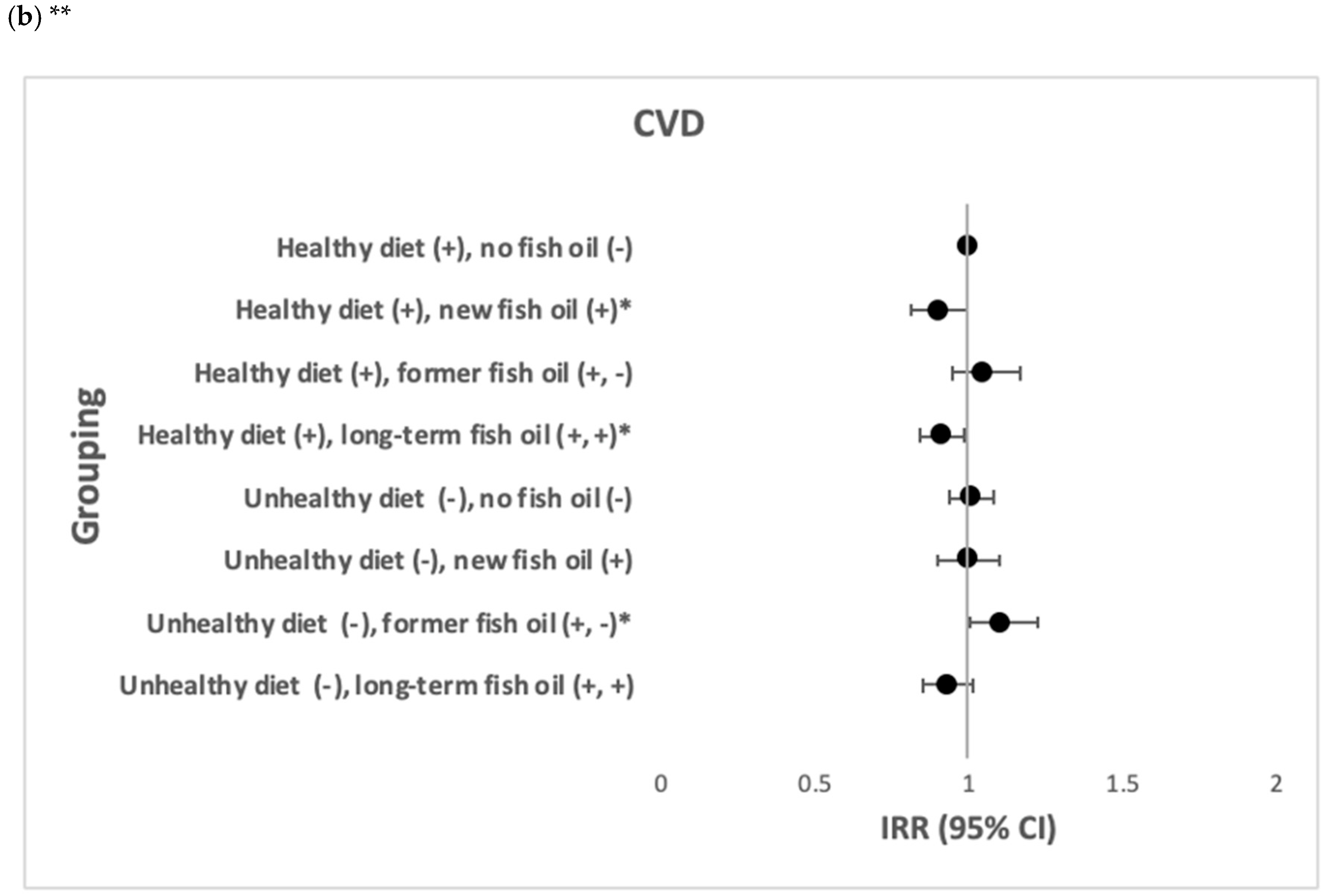
| Fish oil (N = 29,814) | ||||
| Healthy diet (+), no fish oil (–) | 1.00 | 1.00 | 1.00 | 1.00 |
| Healthy diet (+), new fish oil (+) | 0.68 (0.49; 0.94) | 0.70 (0.50; 0.98) | 0.74 (0.53; 1.05) | 0.80 (0.57; 1.13) |
| Healthy diet (+), former fish oil (+, –) | 0.98 (0.71; 1.35) | 0.99 (0.71; 1.39) | 1.06 (0.75; 1.49) | 1.09 (0.77; 1.53) |
| Healthy diet (+), long-term fish oil (+, +) | 0.64 (0.49; 0.84) | 0.68 (0.51; 0.90) | 0.72 (0.54; 0.96) | 0.78 (0.58; 1.03) |
| Unhealthy diet (–), no fish oil (–) | 1.06 (0.81; 1.37) | 1.05 (0.79; 1.40) | 0.96 (0.72; 1.29) | 0.95 (0.71; 1.28) |
| Unhealthy diet (–), new fish oil (+) | 0.91 (0.60; 1.38) | 1.08 (0.70; 1.66) | 1.06 (0.68; 1.64) | 1.07 (0.68; 1.68) |
| Unhealthy diet (–), former fish oil (+, –) | 0.85 (0.51; 1.41) | 0.85 (0.48; 1.51) | 0.82 (0.47; 1.45) | 0.88 (0.50; 1.56) |
| Unhealthy diet (–), long–term fish oil (+, +) | 0.63 (0.40; 0.98) | 0.73 (0.47; 1.16) | 0.73 (0.46; 1.15) | 0.70 (0.43; 1.14) |
| Calcium (N = 29,814) | ||||
| Healthy diet (+), no calcium (–) | 1.00 | 1.00 | 1.00 | 1.00 |
| Healthy diet (+), new calcium (+) | 0.91 (0.60; 1.36) | 0.96 (0.62; 1.47) | 0.94 (0.61; 1.47) | 0.85 (0.55; 1.33) |
| Healthy diet (+), former calcium (+, –) | 0.58 (0.33; 1.04) | 0.68 (0.38; 1.22) | 0.71 (0.39; 1.27) | 0.69 (0.38; 1.23) |
| Healthy diet (+), long-term calcium (+, +) | 0.78 (0.50; 1.20) | 0.76 (0.48; 1.22) | 0.80 (0.50; 1.27) | 0.72 (0.45; 1.14) |
| Unhealthy diet (–), no calcium (–) | 1.08 (0.88; 1.33) | 1.11 (0.89; 1.39) | 1.03 (0.81; 1.29) | 0.99 (0.78; 1.26) |
| Unhealthy diet (–), new calcium (+) | 1.18 (0.63; 2.22) | 1.37 (0.71; 2.66) | 1.14 (0.56; 2.30) | 1.03 (0.49; 2.17) |
| Unhealthy diet (–), former calcium (+, –) | 0.60 (0.19; 1.88) | 0.55 (0.14; 2.19) | 0.51 (0.13; 2.05) | 0.51 (0.13; 2.06) |
| Unhealthy diet (–), long-term calcium (+, +) | 0.61 (0.23; 1.65) | 0.80 (0.30; 2.14) | 0.74 (0.24; 1.24) | 0.71 (0.27; 1.90) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, X.; Shi, Z.; Liu, G.; Chang, D.; Inglis, S.C.; Hall, J.J.; Schutte, A.E.; Byles, J.E.; Parker, D. The Joint Effects of Diet and Dietary Supplements in Relation to Obesity and Cardiovascular Disease over a 10-Year Follow-Up: A Longitudinal Study of 69,990 Participants in Australia. Nutrients 2021, 13, 944. https://doi.org/10.3390/nu13030944
Xu X, Shi Z, Liu G, Chang D, Inglis SC, Hall JJ, Schutte AE, Byles JE, Parker D. The Joint Effects of Diet and Dietary Supplements in Relation to Obesity and Cardiovascular Disease over a 10-Year Follow-Up: A Longitudinal Study of 69,990 Participants in Australia. Nutrients. 2021; 13(3):944. https://doi.org/10.3390/nu13030944
Chicago/Turabian StyleXu, Xiaoyue, Zumin Shi, Gang Liu, Dennis Chang, Sally C. Inglis, John J. Hall, Aletta E. Schutte, Julie E. Byles, and Deborah Parker. 2021. "The Joint Effects of Diet and Dietary Supplements in Relation to Obesity and Cardiovascular Disease over a 10-Year Follow-Up: A Longitudinal Study of 69,990 Participants in Australia" Nutrients 13, no. 3: 944. https://doi.org/10.3390/nu13030944
APA StyleXu, X., Shi, Z., Liu, G., Chang, D., Inglis, S. C., Hall, J. J., Schutte, A. E., Byles, J. E., & Parker, D. (2021). The Joint Effects of Diet and Dietary Supplements in Relation to Obesity and Cardiovascular Disease over a 10-Year Follow-Up: A Longitudinal Study of 69,990 Participants in Australia. Nutrients, 13(3), 944. https://doi.org/10.3390/nu13030944