
Correlations between Coffee Consumption and Metabolic Phenotypes, Plasma Folate, and Vitamin B12: NHANES 2003 to 2006

Abstract
:1. Introduction
2. Materials and Methods
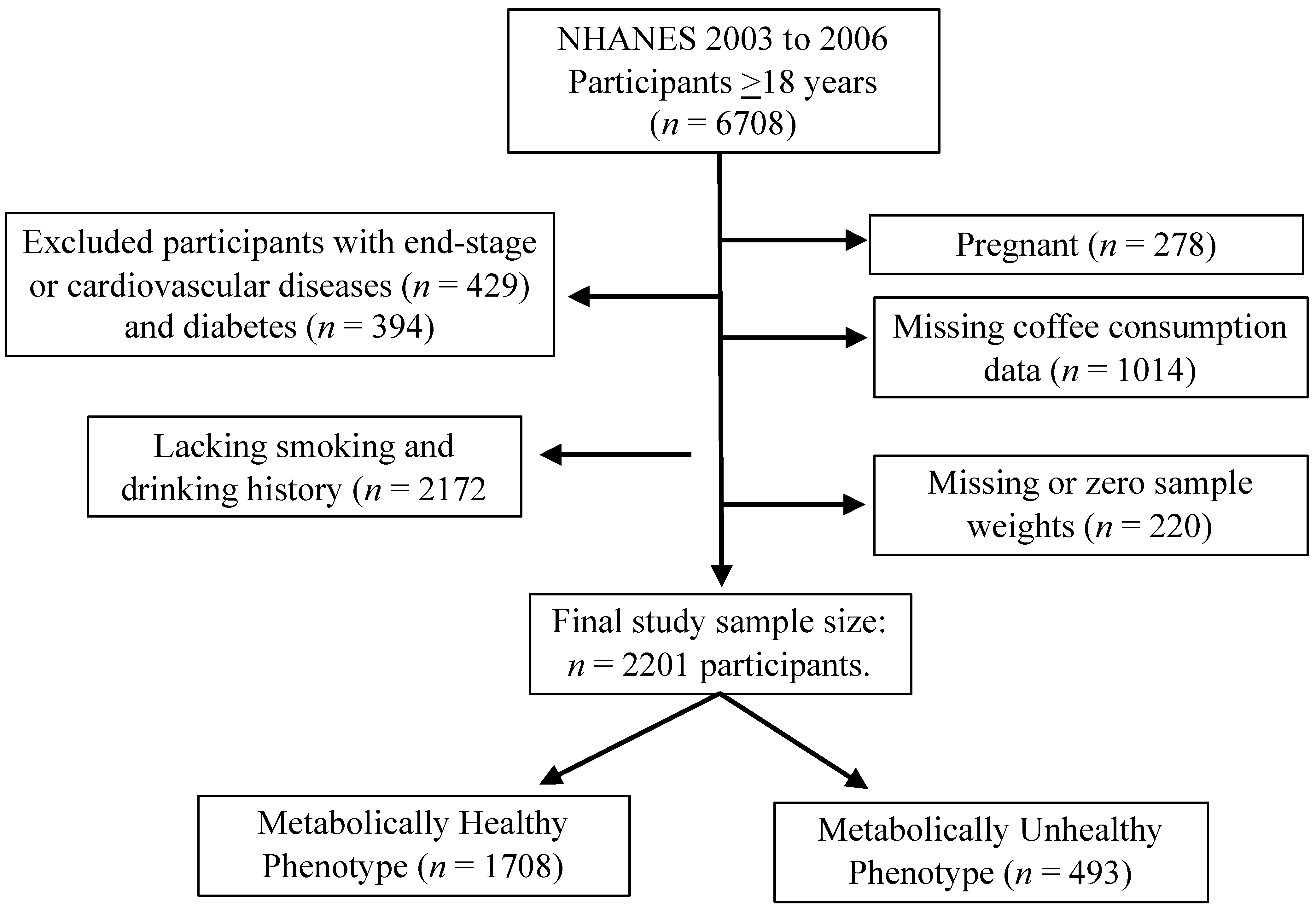
2.1. Study Population
2.2. Data Collection
2.3. Classification of MetS, Metabolically Healthy, and Unhealthy Phenotypes
2.4. Plasma Folate and Vitamin B12
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
3.2. Correlations between Coffee Intake Frequencies and Metabolic Phenotypes and Individual Metabolic Variables
3.3. Correlations between Micronutrients and Coffee Intake and Metabolic Phenotypes
4. Discussion
4.1. Correlation between Coffee Intake Frequencies and Metabolic Phenotypes
4.2. Influence of Coffee Intake on Metabolic Syndrome (MetS) and Its Components
4.3. Correlation between Micronutrients, Coffee Intake, and Metabolic Phenotypes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adult Obesity Facts. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 20 September 2020).
- Managing Overweight and Obesity in Adults: Systematic Evidence Review from the Obesity Expert Panel. Available online: https://www.nhlbi.nih.gov/health-topics/managing-overweight-obesity-in-adults (accessed on 15 September 2020).
- Karelis, A.D.; Rabasa-Lhoret, R. Characterization of metabolically healthy but obese individuals: Should we add vitamin D to the puzzle? Diabetes Metab. 2014, 40, 319–321. [Google Scholar] [CrossRef]
- Karelis, A.D.; Brochu, M.; Rabasa-Lhoret, R.; Garrel, D.; Poehlman, E.T. Clinical markers for the identification of metabolically healthy but obese individuals. Diabetes Obes. Metab. 2004, 6, 456–457. [Google Scholar] [CrossRef]
- Wildman, R.P.; Muntner, P.; Reynolds, K.; McGinn, A.P.; Rajpathak, S.; Wylie-Rosett, J.; Sowers, M.R. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: Prevalence and correlates of 2 phenotypes among the US population (NHANES 1999-2004). Arch. Intern. Med. 2008, 168, 1617–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims, E.A. Are there persons who are obese, but metabolically healthy? Metabolism 2001, 50, 1499–1504. [Google Scholar] [CrossRef]
- Martınez-Larrad, M.T.; Anchuelo, A.C.; Prado, N.D.; Rueda, J.M.I.; Gabriel, R.; Serrano-Ríos, M. Profile of Individuals Who Are Metabolically Healthy Obese Using Different Definition Criteria. A Population-Based Analysis in the Spanish Population. PLoS ONE 2014, 9, e106641. [Google Scholar] [CrossRef] [PubMed]
- Heinzle, S.; Ball, G.D.; Kuk, J.L. Variations in the prevalence and predictors of prevalent metabolically healthy obesity in adolescents. Pediatr. Obes. 2016, 11, 425–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khalidi, B.; Kimball, S.M.; Kuk, J.L.; Ardern, C.I. Metabolically healthy obesity, vitamin D, and all-cause and cardiometabolic mortality risk in NHANES III. Clin. Nutr. 2019, 38, 820–828. [Google Scholar] [CrossRef]
- de Winter, M.; Rioux, B.V.; Boudreau, J.G.; Bouchard, D.R.; Sénéchal, M. Physical Activity and Sedentary Patterns among Metabolically Healthy Individuals Living with Obesity. J. Diabetes Res. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- Esteghamati, A.; Aryan, Z.; Esteghamati, A.; Nakhjavani, M. Differences in vitamin D concentration between metabolically healthy and unhealthy obese adults: Associations with inflammatory and cardiometabolic markers in 4391 subjects. Diabetes Metab. 2014, 40, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Kim do, H.; Roh, Y.K.; Ju, S.Y.; Nam, H.Y.; Nam, G.E.; Kim, D.W.; Lee, S.H.; Lee, C.W.; Han, K.; et al. Serum Ferritin Levels Are Positively Associated With Metabolically Obese Normal Weight: A Nationwide Population-Based Study. Medicine 2015, 94, e2335. [Google Scholar] [CrossRef]
- Goncalves, C.G.; Glade, M.J.; Meguid, M.M. Metabolically healthy obese individuals: Key protective factors. Nutrition 2016, 32, 14–20. [Google Scholar] [CrossRef]
- Mirmiran, P.; Moslehi, N.; Hosseinpanah, F.; Sarbazi, N.; Azizi, F. Dietary determinants of unhealthy metabolic phenotype in normal weight and overweight/obese adults: Results of a prospective study. Int. J. Food Sci. Nutr. 2020, 71, 891–901. [Google Scholar] [CrossRef]
- O’Keefe, J.H.; DiNicolantonio, J.J.; Lavie, C.J. Coffee for Cardioprotection and Longevity. Prog. Cardiovasc. Dis. 2018, 61, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Rehm, C.D.; Ratliff, J.C.; Riedt, C.S.; Drewnowski, A. Coffee Consumption among Adults in the United States by Demographic Variables and Purchase Location: Analyses of NHANES 2011-2016 Data. Nutrients 2020, 12, 2463. [Google Scholar] [CrossRef]
- Nieber, K. The impact of coffee on health. Planta Med. 2017, 83, 1256–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.J.; Jeon, H.J.; Park, S.; Kim, S.A.; Lim, K.; Chung, S.; Chang, P.S.; Lee, J.K.; Kang, D.; Shin, S. Association of Coffee Consumption and Its Types According to Addition of Sugar and Creamer with Metabolic Syndrome Incidence in a Korean Population from the Health Examinees (HEXA) Study. Nutrients 2021, 13, 920. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, E.; Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; De Curtis, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Bonaccio, M.; et al. Daily Coffee Drinking Is Associated with Lower Risks of Cardiovascular and Total Mortality in a General Italian Population: Results from the Moli-sani Study. J. Nutr. 2021, 151, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Sakamaki, T.; Kayaba, K.; Kotani, K.; Namekawa, M.; Hamaguchi, T.; Nakaya, N.; Ishikawa, S. Coffee consumption and mortality in Japan with 18 years of follow-up: The Jichi Medical School Cohort Study. Public Health 2021, 191, 23–30. [Google Scholar] [CrossRef]
- Teramoto, M.; Muraki, I.; Yamagishi, K.; Tamakoshi, A.; Iso, H. Green Tea and Coffee Consumption and All-Cause Mortality Among Persons With and Without Stroke or Myocardial Infarction. Stroke 2021, 52, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.M.; Goulart, A.C.; Bensenor, I.M.; Lotufo, P.A.; Marchioni, D.M. Moderate coffee consumption is associated with lower risk of mortality in prior Acute Coronary Syndrome patients: A prospective analysis in the ERICO cohort. Int. J. Food Sci. Nutr. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Komorita, Y.; Iwase, M.; Fujii, H.; Ohkuma, T.; Ide, H.; Jodai-Kitamura, T.; Yoshinari, M.; Oku, Y.; Higashi, T.; Nakamura, U.; et al. Additive effects of green tea and coffee on all-cause mortality in patients with type 2 diabetes mellitus: The Fukuoka Diabetes Registry. BMJ Open Diabetes Res. Care 2020, 8, e001252. [Google Scholar] [CrossRef] [PubMed]
- Miranda, A.M.; Steluti, J.; Fisberg, R.M.; Marchioni, D.M. Association between Coffee Consumption and Its Polyphenols with Cardiovascular Risk Factors: A Population-Based Study. Nutrients 2017, 9, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.T.; Tabrez, S.; Jabir, N.R.; Ali, M.; Kamal, M.A.; da Silva Araujo, L.; De Oliveira Santos, J.V.; Da Mata, A.; De Aguiar, R.P.S.; de Carvalho Melo Cavalcante, A.A. An Insight into the Therapeutic Potential of Major Coffee Components. Curr. Drug Metab. 2018, 19, 544–556. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Ma, W.; Sun, D.; Heianza, Y.; Wang, T.; Zheng, Y.; Huang, T.; Duan, D.; Bray, J.G.A.; Champagne, C.M.; et al. Genetic variation of habitual coffee consumption and glycemic changes in response to weight-loss diet intervention: The Preventing Overweight Using Novel Dietary Strategies (POUNDS LOST) trial. Am. J. Clin. Nutr. 2017, 106, 1321–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Huang, T.; Kang, J.H.; Zheng, Y.; Jensen, M.K.; Wiggs, J.L.; Pasquale, L.R.; Fuchs, C.S.; Campos, H.; Rimm, E.B.; et al. Habitual coffee consumption and genetic predisposition to obesity: Gene-diet interaction analyses in three US prospective studies. BMC Med. 2017, 15, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.N.; Cho, H.J.; Youn, J.; Jin, T.; Kang, M.; Sung, J.; Lee, J.E. Coffee Consumption, Genetic Polymorphisms, and the Risk of Type 2 Diabetes Mellitus: A Pooled Analysis of Four Prospective Cohort Studies. Int. J. Environ. Res. Public Health 2020, 17, 5379. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T. Coffee consumption and metabolic syndrome: A dose-response relationship. Int. J. Food Sci. Nutr. 2019, 70, 651. [Google Scholar] [CrossRef]
- Kim, H.J.; Cho, S.; Jacobs, D.R., Jr.; Park, K. Instant coffee consumption may be associated with higher risk of metabolic syndrome in Korean adults. Diabetes Res. Clin. Pract. 2014, 106, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Kim, K.; Park, S.M. Association between the Prevalence of Metabolic Syndrome and the Level of Coffee Consumption among Korean Women. PLoS ONE 2016, 11, e0167007. [Google Scholar] [CrossRef]
- Kim, Y.; Je, Y. Moderate coffee consumption is inversely associated with the metabolic syndrome in the Korean adult population. Br. J. Nutr. 2018, 120, 1279–1287. [Google Scholar] [CrossRef] [Green Version]
- Song, F.; Oh, L.; Lee, K.; Cho, M.S. The efect of coffee consumption on food group intake, nutrition intake, and metabolic syndrome of Korean adults-2010 KNHANES. NSF J. 2016, 4, 9–14. [Google Scholar]
- Thomas, D.R.; Hodges, I.D. Dietary Research on Coffee: Improving Adjustment for Confounding. Curr. Dev. Nutr. 2020, 4, nzz142. [Google Scholar] [CrossRef]
- Tian, D.D.; Natesan, S.; White, J.R., Jr.; Paine, M.F. Effects of Common CYP1A2 Genotypes and Other Key Factors on Intraindividual Variation in the Caffeine Metabolic Ratio: An Exploratory Analysis. Clin. Transl. Sci. 2019, 12, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Yoshihara, T.; Zaitsu, M.; Shiraishi, F.; Arima, H.; Takahashi-Yanaga, F.; Arioka, M.; Kajioka, S.; Sasaguri, T. Influence of genetic polymorphisms and habitual caffeine intake on the changes in blood pressure, pulse rate, and calculation speed after caffeine intake: A prospective, double blind, randomized trial in healthy volunteers. J. Pharmacol. Sci. 2019, 139, 209–214. [Google Scholar] [CrossRef]
- Zhou, A.; Hypponen, E. Long-term coffee consumption, caffeine metabolism genetics, and risk of cardiovascular disease: A prospective analysis of up to 347,077 individuals and 8368 cases. Am. J. Clin. Nutr. 2019, 109, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Yamagata, K. Do Coffee Polyphenols Have a Preventive Action on Metabolic Syndrome Associated Endothelial Dysfunctions? An Assessment of the Current Evidence. Antioxidants 2018, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Battram, D.S.; Arthur, R.; Weekes, A.; Graham, T.E. The glucose intolerance induced by caffeinated coffee ingestion is less pronounced than that due to alkaloid caffeine in men. J. Nutr. 2006, 136, 1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, Y.; Kobayashi, M.; Yamauchi, R.; Ojika, M.; Hiramitsu, M.; Inoue, T.; Katagiri, T.; Murai, A.; Horio, F. Coffee and Caffeine Improve Insulin Sensitivity and Glucose Tolerance in C57BL/6J Mice Fed a High-Fat Diet. Biosci. Biotechnol. Biochem. 2011, 75, 2309–2315. [Google Scholar] [CrossRef] [Green Version]
- Panchal, S.K.; Poudyal, H.; Waanders, J.; Brown, L. Coffee extract attenuates changes in cardiovascular and hepatic structure and function without decreasing obesity in high-carbohydrate, high-fat diet-fed male rats. J. Nutr. 2012, 142, 690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, T.M.; Clifford, M.N.; Penson, S.; Chope, G.; Robertson, M.D. A single serving of caffeinated coffee impairs postprandial glucose metabolism in overweight men. Br. J. Nutr. 2015, 114, 1218–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsch, C.A.; Lachance, P.A.; Wasserman, B.P. Dietary phenolic compounds: Inhibition of Na+-dependent D-glucose uptake in rat intestinal brush border membrane vesicles. J. Nutr. 1989, 119, 1698–1704. [Google Scholar] [CrossRef]
- Baspinar, B.; Eskici, G.; Ozcelik, A.O. How coffee affects metabolic syndrome and its components. Food Funct. 2017, 8, 2089–2101. [Google Scholar] [CrossRef]
- Bidel, S.; Tuomilehto, J. The emerging health benefits of coffee with an emphasis on Type 2 diabetes and cardiovascular disease. Eur. Endocrinol. 2013, 9, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Ding, M.; Bhupathiraju, S.N.; Chen, M.; van Dam, R.M.; Hu, F. Caffeinated and decaffeinated coffee consumption and risk of type 2 diabetes: A systematic review and a dose-response meta-analysis. Diabetes Care 2014, 37, 569–586. [Google Scholar] [CrossRef] [Green Version]
- Santos, D.; Lima, D. Coffee consumption, obesity and type 2 diabetes: A mini-review. Eur. J. Nutr. 2016, 55, 1345–1358. [Google Scholar] [CrossRef]
- Calcaterra, V.; Larizza, D.; De Giuseppe, R.; De Liso, F.; Klersy, C.; Albertini, R.; Pozzebon, I.; Princis, M.P.; Montalbano, C.; Madè, A.; et al. Diet and lifestyle role in homocysteine metabolism in Turner’s syndrome. Med. Princ. Pract. 2018. [Google Scholar] [CrossRef]
- Grubben, M.J.; Boers, G.H.; Blom, H.J.; Broekhuizen, R.; de Jong, R.; van Rijt, L.; de Ruijter, E.; Swinkels, D.W.; Nagengast, F.M.; Katan, M.B. Unfiltered coffee increases plasma homocysteine concentrations in healthy volunteers: A randomized trial. Am. J. Clin. Nutr. 2000, 71, 480–484. [Google Scholar] [CrossRef] [Green Version]
- Vollset, S.E.; Nygard, O.; Refsum, H.; Ueland, P.M. Coffee and homocysteine. Am. J. Clin. Nutr. 2000, 71, 403–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducker, G.S.; Rabinowitz, J.D. One-Carbon Metabolism in Health and Disease. Cell Metab. 2017, 25, 27–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhoef, P.; Pasman, W.J.; Van Vliet, T.; Urgert, R.; Katan, M.B. Contribution of caffeine to the homocysteine-raising effect of coffee: A randomized controlled trial in humans. Am. J. Clin. Nutr. 2002, 76, 1244–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, H.G.; Zaveri, M.P.; Antia, F.P. Letter: Increased vitamin B12 absorption after ingestion of coffee. Gastroenterology 1973, 65, 694–695. [Google Scholar] [CrossRef]
- Waskiewicz, A.; Sygnowska, E.; Broda, G. Dietary intake of vitamins B6, B12 and folate in relation to homocysteine serum concentration in the adult Polish population-WOBASZ Project. Kardiol. Pol. 2010, 68, 275–282. [Google Scholar] [PubMed]
- Ulvik, A.; Vollset, S.E.; Hoff, G.; Ueland, P.M. Coffee consumption and circulating B-vitamins in healthy middle-aged men and women. Clin. Chem. 2008, 54, 1489–1496. [Google Scholar] [CrossRef]
- Kanth, V.V.; Golla, J.P.; Sastry, B.K.; Naik, S.; Kabra, N.; Sujatha, M. Genetic interactions between MTHFR (C677T), methionine synthase (A2756G, C2758G) variants with vitamin B12 and folic acid determine susceptibility to premature coronary artery disease in Indian population. J. Cardiovasc. Dis. Res. 2011, 2, 156–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olthof, M.R.; Hollman, P.C.; Zock, P.L.; Katan, M.B. Consumption of high doses of chlorogenic acid, present in coffee, or of black tea increases plasma total homocysteine concentrations in humans. Am. J. Clin. Nutr. 2001, 73, 532–538. [Google Scholar] [CrossRef]
- Loftfield, E.; Freedman, N.D.; Dodd, K.W.; Vogtmann, E.; Xiao, Q.; Sinha, R.; Graubard, B.I. Coffee Drinking Is Widespread in the United States, but Usual Intake Varies by Key Demographic and Lifestyle Factors. J. Nutr. 2016, 146, 1762–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, M.K.; Han, Y.A.; Roh, Y.K. Utility of obesity indicators for metabolically healthy obesity: An observational study using the Korean National Health and Nutrition Examination Survey (2009–2010). BMC Public Health 2014, 14, 1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messier, V.; Karelis, A.D.; Prud’homme, D.; Primeau, V.; Brochu, M.; Rabasa-Lhoret, R. Identifying metabolically healthy but obese individuals in sedentary postmenopausal women. Obesity 2010, 18, 911–917. [Google Scholar] [CrossRef]
- Munoz-Garach, A.; Cornejo-Pareja, I.; Tinahones, F.J. Does Metabolically Healthy Obesity Exist? Nutrients 2016, 8, 320. [Google Scholar] [CrossRef] [Green Version]
- De Lorenzo, A.; Glerian, L.; Amaral, A.C.; Reis, T.B.; Lima, R.S.L. “Metabolically healthy” obesity: Prevalence, clinical features and association with myocardial ischaemia. Obes. Res. Clin. Pract. 2017, 11, 315–323. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, H.; Jee, H. Effects of socioeconomic status, health behavior, and physical activity on the prevalence of metabolic syndrome. J. Exerc. Rehabil. 2018, 14, 183–191. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.Y.; Jung, C.H.; Park, J.S.; Rhee, E.J.; Kim, S.W. Effects of smoking, alcohol, exercise, education, and family history on the metabolic syndrome as defined by the ATP III. Diabetes Res. Clin. Pract. 2005, 67, 70–77. [Google Scholar] [CrossRef]
- Flores-Guerrero, J.L.; Minovic, I.; Groothof, D.; Gruppen, E.G.; Riphagen, I.J.; Kootstra-Ros, J.; Muller Kobold, A.; Hak, E.; Navis, G.; Gansevoort, R.T.; et al. Association of Plasma Concentration of Vitamin B12 With All-Cause Mortality in the General Population in the Netherlands. JAMA Netw. Open 2020, 3, e1919274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes, M.A.; da Silva, I.; Ramires, V.; Reichert, F.; Martins, R.; Ferreira, R.; Tomasi, E. Metabolic equivalent of task (METs) thresholds as an indicator of physical activity intensity. PLoS ONE 2018, 13, e0200701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHANES. National Health and Nutrition Examination Survey NHANES, “Anthropometry Procedures Manual,”. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_07_08/manual_an.pdf (accessed on 20 September 2020).
- Hall, Y.N.; Xu, P.; Chertow, G.M. Relationship of body size and mortality among US Asians and Pacific Islanders on dialysis. Ethn. Dis. 2011, 21, 40–46. [Google Scholar] [PubMed]
- Davis, J.; Juarez, D.; Hodges. Relationship of Ethnicity and Body Mass Index with the Development of Hypertension and Hyperlipidemia. Ethn. Dis. 2013, 23, 65–70. [Google Scholar] [PubMed]
- Paramsothy, P.; Knopp, R.; Bertoni, A.G.; Tsai, M.Y.; Rue, T.; Heckbert, S.R. Combined hyperlipidemia in relation to race/ethnicity, obesity, and insulin resistance in the Multi-Ethnic Study of Atherosclerosis. Metabolism 2009, 58, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Tomiyama, A.J.; Hunger, J.M.; Nguyen-Cuu, J.; Wells, C. Misclassification of cardiometabolic health when using body mass index categories in NHANES 2005–2012. Int. J. Obes. 2016, 40, 883–886. [Google Scholar] [CrossRef] [Green Version]
- Koyama, T.; Maekawa, M.; Ozaki, E.; Kuriyama, N.; Uehara, R. Daily Consumption of Coffee and Eating Bread at Breakfast Time Is Associated with Lower Visceral Adipose Tissue and with Lower Prevalence of Both Visceral Obesity and Metabolic Syndrome in Japanese Populations: A Cross-Sectional Study. Nutrients 2020, 12, 3090. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.Y.; Kim, J. Coffee Consumption and the Risk of Obesity in Korean Women. Nutrients 2017, 9, 1340. [Google Scholar] [CrossRef] [Green Version]
- Harpaz, E.; Tamir, S.; Weinstein, A.; Weinstein, Y. The effect of caffeine on energy balance. J. Basic Clin. Physiol. Pharmacol. 2017, 28, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Kobayashi, S.; Yamaguchi, T.; Hibi, M.; Fukuhara, I.; Osaki, N. Coffee Abundant in Chlorogenic Acids Reduces Abdominal Fat in Overweight Adults: A Randomized, Double-Blind, Controlled Trial. Nutrients 2019, 11, 1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curb, J.D.; Reed, D.M.; Kautz, J.A.; Yano, K. Coffee, caffeine, and serum cholesterol in Japanese men in Hawaii. Am. J. Epidemiol. 1986, 123, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Davis, B.R.; Curb, J.D.; Borhani, N.O.; Prineas, R.J.; Molteni, A. Coffee consumption and serum cholesterol in the hypertension detection and follow-up program. Am. J. Epidemiol. 1988, 128, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Correa, T.A.; Rogero, M.M.; Mioto, B.M.; Tarasoutchi, D.; Tuda, V.L.; Cesar, L.A.; Torres, E.A. Paper-filtered coffee increases cholesterol and inflammation biomarkers independent of roasting degree: A clinical trial. Nutrition 2013, 29, 977–981. [Google Scholar] [CrossRef] [Green Version]
- van Dam, R.M.; Pasman, W.J.; Verhoef, P. Effects of coffee consumption on fasting blood glucose and insulin concentrations: Randomized controlled trials in healthy volunteers. Diabetes Care 2004, 27, 2990–2992. [Google Scholar] [CrossRef] [Green Version]
- Urgert, R.; Katan, M.B. The cholesterol raising factor from coffee beans. Annu. Rev. Nutr. 1997, 17, 305–324. [Google Scholar] [CrossRef] [Green Version]
- Urgert, R.; van Vliet, T.; Zock, P.L.; Katan, M.B. Heavy coffee consumption and plasma homocysteine: A randomized controlled trial in healthy volunteers. Am. J. Clin. Nutr. 2000, 72, 1107–1110. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Zampelas, A.; Zeimbekis, A.; Chrysohoou, C.; Papademetriou, L.; Stefanadis, C. The association between coffee consumption and plasma total homocysteine levels: The “ATTICA” study. Heart Vessel. 2004, 19, 280–286. [Google Scholar]
- Mursu, J.; Voutilainen, S.; Nurmi, T.; Alfthan, G.; Virtanen, J.K.; Rissanen, T.H.; Happonen, P.; Nyyssonen, K.; Kaikkonen, J.; Salonen, R.; et al. The effects of coffee consumption on lipid peroxidation and plasma total homocysteine concentrations: A clinical trial. Free Radic. Biol. Med. 2005, 38, 527–534. [Google Scholar] [CrossRef]
- Esposito, F.; Morisco, F.; Verde, V.; Ritieni, A.; Alezio, A.; Caporaso, N.; Fogliano, V. Moderate coffee consumption increases plasma glutathione but not homocysteine in healthy subjects. Aliment. Pharmacol. Ther. 2003, 17, 595–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nygard, O.; Refsum, H.; Ueland, P.M.; Stensvold, I.; Nordrehaug, J.E.; Kvale, G.; Vollset, S.E. Coffee consumption and plasma total homocysteine: The Hordaland Homocysteine Study. Am. J. Clin. Nutr. 1997, 65, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Bird, J.K.; Ronnenberg, A.G.; Choi, S.W.; Du, F.; Mason, J.B.; Liu, Z. Obesity is associated with increased red blood cell folate despite lower dietary intakes and serum concentrations. J. Nutr. 2015, 145, 79–86. [Google Scholar] [CrossRef]
- Hosseinpanah, F.; Nazeri, P.; Ghareh, S.; Tohidi, M.; Azizi, F. Predictors of the incident metabolic syndrome in healthy obese subjects: A decade of follow-up from the Tehran Lipid and Glucose Study. Eur. J. Clin. Nutr. 2014, 68, 295–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.; Zhang, L.; Zheng, R.; Zheng, Y. The prevalence, metabolic risk and effects of lifestyle intervention for metabolically healthy obesity: A systematic review and meta-analysis: A PRISMA-compliant article. Medicine 2017, 96, e8838. [Google Scholar] [CrossRef]
- Harrington, M.; Gibson, S.; Cottrell, R.C. A review and meta-analysis of the effect of weight loss on all-cause mortality risk. Nutr. Res. Rev. 2009, 22, 93–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Metabolic Phenotypes * | Weighted p-Value | |
|---|---|---|---|
| Metabolic Healthy Phenotype (MHP) (n = 1708) | Metabolic Unhealthy Phenotype (MUHP) (n = 493) | ||
| Demographics | |||
| Age Group, years (n, %) | <0.001 | ||
| 20–34 | 524 (30.9%) | 36 (8.8%) | |
| 35–49 | 507 (36.0%) | 103 (28.6%) | |
| 50–64 | 341 (21.7%) | 166 (37.6%) | |
| 65–79 | 213 (8.2%) | 151 (21.7%) | |
| ≥80 | 123 (3.1%) | 37 (3.3%) | |
| Sex (n, %) | <0.001 | ||
| Male | 790 (43.1%) | 264 (53.8%) | |
| Female | 918 (56.9%) | 229 (46.1%) | |
| Race/Ethnicity (n, %) | <0.001 | ||
| Non-Hispanic White | 924 (73.0%) | 313 (83.0%) | |
| Mexican American or Hispanic | 353 (10.5%) | 90 (5.1%) | |
| Non-Hispanic Black | 353 (11.0%) | 73 (7.1%) | |
| Other | 78 (5.4%) | 17 (4.8%) | |
| Health Behaviors | |||
| Smoker (n, %) | 0.002 | ||
| Never | 917 (52.5%) | 232 (47.5%) | |
| Former | 409 (22.8%) | 169 (32.4%) | |
| Current | 382 (24.8%) | 92 (20.1%) | |
| Alcohol Drinker (n, %) | <0.001 | ||
| Never | 209 (11.3%) | 70 (15.6%) | |
| Former | 252 (14.1%) | 92 (21.6%) | |
| Current: <1 drink/day | 773 (56.5%) | 190 (48.8%) | |
| 1–2 drinks/day | 171 (11.8%) | 28 (6.4%) | |
| >2 drinks/day | 81 (6.3%) | 28 (7.6%) | |
| Physical Activity MET hour/week (n, %) | 0.003 | ||
| <5.0 | 259 (21.4%) | 79 (29.6%) | |
| 5.0–19.9 | 407 (36.3%) | 121 (40.5%) | |
| 20.0–49.9 | 290 (26.9%) | 62 (21.9%) | |
| ≥50.0 | 170 (15.3%) | 25 (8.0%) | |
| MetS Components | |||
| Waist circumference, cm (Mean ± SE) | 92.69 ± 0.36 | 111.46 ± 0.75 | <0.001 |
| Waist circumference, cm (n, %) | <0.001 | ||
| ≥102 | 373 (21.3%) | 378 (81.3%) | |
| <102 | 1294 (78.7%) | 111 (18.7%) | |
| SBP, mm Hg (Mean ± SE) | 119.18 ± 0.61 | 129.13 ± 0.98 | <0.001 |
| DBP, mm Hg (Mean ± SE) | 69.46 ± 0.38 | 73.78 ± 0.72 | <0.001 |
| Elevated blood pressure, mm Hg (n, %) | <0.001 | ||
| ≥130/85 or medication use | 270 (13.0%) | 337 (65.3%) | |
| <130/85 or no medication use | 1438 (87.0%) | 156 (34.7%) | |
| Glucose, mg/dL (Mean ± SE) | 92.99 ± 0.38 | 103.12 ± 0.51 | <0.001 |
| Elevated glucose, mg/dL (n, %) | <0.001 | ||
| ≥100 or medication use | 336 (17.2%) | 356 (69.9%) | |
| <100 or no medication use | 1372 (82.8%) | 137 (30.1%) | |
| HDL-c, mg/dL (Mean ± SE) | 57.73 ± 0.65 | 45.66 ± 1.20 | <0.001 |
| Decreased HDL-c Level, mg/dL (n, %) | <0.001 | ||
| <40 for men or <50 for women or medication use | 215 (12.4%) | 313 (62.7%) | |
| ≥40 for men or ≥50 for women or no medication use | 1493 (87.6%) | 180 (37.3%) | |
| Triglycerides, mg/dL (Mean ± SE) | 115.83 ± 2.20 | 208.60 ± 7.06 | <0.001 |
| Elevated triglycerides, mg/dL (n, %) | <0.001 | ||
| ≥150 | 307 (18.7%) | 335 (69.7%) | |
| <150 | 1381 (81.3%) | 155 (30.3%) | |
| HOMA-IR Components | |||
| Insulin, µU/mL (Mean ± SE) | 7.73 ± 0.22 | 15.92 ± 0.91 | <0.001 |
| HOMA-IR (Mean ± SE) | 11.69 ± 0.32 | 25.06 ± 1.29 | <0.001 |
| HOMA-IR, (n, %) | <0.001 | ||
| Quartile 4 | 271 (14.2%) | 245 (53.1%) | |
| Quartiles 1 to 3 | 1411 (85.8%) | 243 (46.9%) | |
| Other Metabolic Characteristics | |||
| BMI (Kg/m2, Mean ± SE) | 26.86 ± 0.14 | 33.17 ± 0.38 | <0.001 |
| BMI (Kg/m2, n, %) | <0.001 | ||
| Normal weight (<25.0 Kg/m2) | 682 (42.8%) | 40 (7.1%) | |
| Overweight (25.0–29.9 Kg/m2) | 604 (35.5%) | 149 (26.9%) | |
| Obese (≥30.0 Kg/m2) | 399 (21.7%) | 304 (66.1%) | |
| LDL-c, mg/dL (Mean ± SE) | 117.33 ± 1.22 | 120.00 ± 1.81 | 0.219 |
| Total cholesterol, mg/dL (Mean ± SE) | 198.25 ± 1.35 | 207.75 ± 2.09 | <0.001 |
| CRP, mg/dL (Mean ± SE) | 0.40 ± 0.03 | 0.56 ± 0.04 | 0.119 |
| Variables | Metabolic Phenotype * | Weighted p-Value | |
|---|---|---|---|
| Metabolic Healthy Phenotype (MHP) (n = 1708) | Metabolic Unhealthy Phenotype (MUHP) (n = 493) | ||
| Coffee Consumption (n, %) | 0.513 | ||
| None or ≤1 cup/week | 730 (41.3%) | 174 (37.0%) | |
| 2–6 cups/week | 199 (11.4%) | 57 (10.6%) | |
| 1 cup/day | 274 (13.5%) | 84 (14.3%) | |
| ≥2 cups/day | 505 (33.8%) | 178 (38.0%) | |
| Caffeine, mg/day (Mean ± SE) | 180.91 ± 6.47 | 193.38 ± 11.54 | 0.267 |
| Caffeine | 0.153 | ||
| <35.3 mg/day | 435 (22.3%) | 112 (17.8%) | |
| 35.5 mg/day–<106.5 mg/day | 432 (22.1%) | 111 (20.0%) | |
| 106.5 mg/day–<219.5 mg/day | 426 (25.7%) | 136 (28.1%) | |
| ≥219.5 mg/day | 415 (29.8%) | 134 (34.1%) | |
| Metabolic Variables (n, %) | Coffee Consumption * | ||||
|---|---|---|---|---|---|
| None/≤1 cup/week (904, 41.1%) | 2–6 cups/week (256, 11.6%) | 1 cup/day (358, 16.3%) | ≥2 cups/day (683, 31%) | Weighted p-Value | |
| BMI, Kg/m2 (Mean ± SE) | 28.78 ± 0.32 | 28.45 ± 0.43 | 27.79 ± 0.47 | 27.62 ± 0.22 | <0.001 |
| SBP, mm Hg (Mean ± SE) | 119.96 ± 0.93 | 121.39 ± 1.35 | 120.90 ± 1.21 | 122.83 ± 0.87 | 0.027 |
| DBP, mm Hg (Mean ± SE) | 70.64 ± 0.53 | 70.24 ± 0.70 | 69.43 ± 0.89 | 70.44 ± 0.40 | 0.568 |
| Glucose, mg/dL (Mean ± SE) | 94.43 ± 0.53 | 95.82 ± 0.73 | 95.37 ± 0.94 | 95.61 ± 0.44 | 0.020 |
| HDL-c, mg/dL (Mean ± SE) | 53.42 ± 0.99 | 55.47 ± 1.24 | 55.94 ± 1.39 | 55.63 ± 1.14 | 0.166 |
| LDL-c, mg/dL (Mean ± SE) | 114.31 ± 1.56 | 116.43 ± 1.84 | 120.06 ± 2.21 | 121.59 ± 1.62 | <0.001 |
| Total cholesterol, mg/dL (Mean ± SE) | 195.31 ± 1.70 | 199.36 ± 2.68 | 202.05 ± 2.65 | 205.59 ± 1.77 | <0.001 |
| Triglyceride, mg/dL (Mean ± SE) | 137.70 ± 4.46 | 135.24 ± 7.85 | 132.99 ± 5.82 | 133.79 ± 3.81 | 0.522 |
| HOMA-IR (Mean ± SE) | 16.53 ± 0.99 | 14.69 ± 0.75 | 13.96 ± 1.04 | 12.33 ± 0.41 | <0.001 |
| CRP, mg/dL (Mean ± SE) | 0.49 ± 0.05 | 0.47 ± 0.05 | 0.42 ± 0.04 | 0.36 ± 0.04 | 0.021 |
| Number of metabolic abnormalities | 0.871 | ||||
| 0 | 298 (34.4%) | 81 (35.1%) | 102 (35.6%) | 175 (30.5%) | |
| 1 | 259 (28.1%) | 71 (28.0%) | 100 (24.8%) | 173 (25.3%) | |
| 2 | 173 (18.2%) | 47 (17.0%) | 72 (17.7%) | 157 (21.1%) | |
| 3 | 112 (11.6%) | 32 (11.9%) | 49 (13.9%) | 98 (13.4%) | |
| 4 | 51 (6.3%) | 21 (6.6%) | 28 (6.8%) | 64 (7.6%) | |
| 5 | 11 (1.3%) | 4 (1.3%) | 7 (1.3%) | 16 (2.1%) | |
| Folate, ng/mL(Mean± SE) | 12.69 ± 0.39 | 12.38 ± 0.47 | 14.20 ± 0.68 | 14.00 ± 0.49 | 0.009 |
| Folate, ng/mL | 0.009 | ||||
| <8.3 | 244 (25.5%) | 66 (25.0%) | 82 (21.0%) | 146 (22.9%) | |
| 8.3–<11.5 | 244 (28.1%) | 74 (29.8%) | 81 (22.5%) | 146 (21.8%) | |
| 11.5–<16.1 | 206 (23.3%) | 63 (27.5%) | 105 (30.8%) | 176 (25.9%) | |
| ≥16.1 | 200 (23.0%) | 49 (17.7%) | 88 (25.8%) | 211 (29.5%) | |
| Vitamin B12, pg/mL (Mean ± SE) | 560.65 ± 35.69 | 487.32 ± 14.25 | 539.05 ± 19.39 | 509.55 ± 15.32 | 0.218 |
| Vitamin B12, pg/mL | 0.475 | ||||
| <359.0 | 203 (25.7%) | 73 (29.1%) | 83 (25.1%) | 179 (28.3%) | |
| 359.0–<470.5 | 218 (25.6%) | 68 (29.9%) | 77 (22.6%) | 177 (26.0%) | |
| 470.5–<634.5 | 227 (24.0%) | 55 (22.3%) | 96 (26.9%) | 169 (24.2%) | |
| ≥634.5 | 236 (24.7%) | 55 (18.6%) | 97 (25.5%) | 147 (21.5%) | |
| Variable | Total (n = 2201) | BMI Status * | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Normal Weight (n = 722) | Overweight (n = 753) | Obese (n = 703) | ||||||||
| MHP (n = 682) | MUHP (n = 40) | Weighted p-Value | MHP (n = 604) | MUHP (n = 149) | Weighted p-Value | MHP (n = 399) | MUHP (n = 304) | Weighted p-Value | ||
| Coffee Consumption (n, %) | 0.98 | 0.015 | 0.56 | |||||||
| None | 584 (26.6%) | 173 (95.4%) | 10 (4.6%) | 156 (91.6%) | 18 (8.4%) | 134 (57.7%) | 88 (42.3%) | |||
| Ref | Ref | Ref | ||||||||
| ≤1 time/week | 320 (13.8%) | 111 (95.7%) | 6 (4.3%) | 78 (86.2%) | 10 (13.8%) | 67 (59.7%) | 42 (40.3%) | |||
| OR [95% CI] 0.92 [0.27, 3.17] | OR [95% CI] 1.75 [0.67, 4.56] | OR [95% CI] 0.92 [0.52, 1.63] | ||||||||
| 2–6 times/week | 256 (11.2%) | 69 (97.2%) | 4 (2.8%) | 78 (87.2%) | 16 (12.8%) | 50 (57.8%) | 37 (42.2%) | |||
| OR [95% CI] 0.60 [0.15, 2.44] | OR [95% CI] 1.60 [0.63, 4.08] | OR [95% CI] 0.99 [0.55, 1.81] | ||||||||
| 1 time/day | 358 (13.7%) | 108 (95.4%) | 7 (4.6%) | 102 (79.7%) | 31 (20.3%) | 59 (51.1%) | 46 (48.9%) | |||
| OR [95% CI] 1.00 [0.26, 3.77] | OR [95% CI] 2.77 [1.24, 6.20] | OR [95% CI] 1.30 [0.73, 2.34] | ||||||||
| ≥2 times/day | 683 (34.6%) | 221 (95.7%) | 13 (4.3%) | 190 (77.2%) | 74 (22.8%) | 89 (49.9%) | 91 (50.1%) | |||
| OR [95% CI] 0.91 [0.31, 2.72] | OR [95% CI] 3.22 [1.62, 6.39] | OR [95% CI] 1.37 [0.86, 2.19] | ||||||||
| Caffeine, mg/day (Mean ± SE) | 183.53 ± 6.31 | 164.99 ± 9.40 | 147.67 ±40.46 | 0.69 | 204.79 ± 6.53 | 220.39 ± 16.40 | 0.37 | 168.85 ± 13.36 | 187.30 ± 16.30 | 0.40 |
| OR [95% CI] for one SD increase 0.90 [0.50, 1.61] | OR [95% CI] for one SD increase 1.06 [0.90, 1.25] | OR [95% CI] for one SD increase 1.11 [0.92, 1.34] | ||||||||
| Variables | Metabolic Phenotype * | Weighted p-Value | |
|---|---|---|---|
| Metabolic Healthy Phenotype (MHP) (n = 1708) | Metabolic Unhealthy Phenotype (MUHP) (n = 493) | ||
| Folate, ng/mL (Mean ± SE) | 12.97 ± 0.32 | 14.65 ± 0.69 | 0.004 |
| Folate | 0.277 | ||
| <8.3 ng/mL | 433 (24.3%) | 105 (22.3%) | |
| 8.3 ng/ML–<11.5 ng/mL | 433 (25.7%) | 112 (23.9%) | |
| 11.5 ng/mL–<16.1 ng/mL | 422 (25.9%) | 128 (25.0%) | |
| ≥16.1 ng/mL | 406 (24.0%) | 142 (28.8%) | |
| Vitamin B12, pg/mL (Mean ± SE) | 541.64 ± 20.53 | 494.41 ± 13.40 | 0.035 |
| Vitamin B12 | 0.027 | ||
| <359.0 pg/mL | 401 (25.8%) | 137 (31.2%) | |
| 359.0 pg/Ml–<470.5 pg/mL | 415 (25.1%) | 125 (28.5%) | |
| 470.5 pg/mL–<634.5 pg/mL | 431 (25.1%) | 116 (21.1%) | |
| ≥634.5 pg/mL | 430 (24.0%) | 105 (19.3%) | |
| Variable | Total (n = 2201) | BMI Status * | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Normal Weight (n = 722) | Overweight (n = 753) | Obese (n = 703) | ||||||||
| MHP (n = 682) | MUHP (n = 40) | Weighted p-Value | MHP (n = 604) | MUHP (n = 149) | Weighted p-Value | MHP (n = 399) | MUHP (n = 304) | Weighted p-Value | ||
| Folate, ng/mL (Mean ± SE) | 13.32 ± 0.34 | 13.43 ± 0.34 | 16.55 ± 1.81 | 0.11 | 13.44 ± 0.38 | 15.97 ± 1.19 | 0.020 | 11.30 ± 0.49 | 13.91 ± 0.67 | 0.0006 |
| OR [95% CI] for one SD increase 1.27 [0.94, 1.70] | OR [95% CI] for one SD increase 0.27 [0.10, 2.61] | OR [95% CI] for one SD increase 1.47 [1.17, 1.84] | ||||||||
| Vitamin B12, pg/mL (Mean ± SE) | 531.71 ± 17.55 | 548.70 ± 12.96 | 550.92 ± 48.40 | 0.97 | 571.49 ± 53.36 | 506.16 ± 24.85 | 0.25 | 482.22 ± 17.43 | 483.26 ± 18.62 | 0.96 |
| OR [95% CI] for one SD increase 1.04 [0.16, 6.64] | OR [95% CI] for one SD increase 0.67 [0.19, 2.38] | OR [95% CI] for one SD increase 1.02 [0.46, 2.25] | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nerurkar, P.V.; Gandhi, K.; Chen, J.J. Correlations between Coffee Consumption and Metabolic Phenotypes, Plasma Folate, and Vitamin B12: NHANES 2003 to 2006. Nutrients 2021, 13, 1348. https://doi.org/10.3390/nu13041348
Nerurkar PV, Gandhi K, Chen JJ. Correlations between Coffee Consumption and Metabolic Phenotypes, Plasma Folate, and Vitamin B12: NHANES 2003 to 2006. Nutrients. 2021; 13(4):1348. https://doi.org/10.3390/nu13041348
Chicago/Turabian StyleNerurkar, Pratibha V., Krupa Gandhi, and John J. Chen. 2021. "Correlations between Coffee Consumption and Metabolic Phenotypes, Plasma Folate, and Vitamin B12: NHANES 2003 to 2006" Nutrients 13, no. 4: 1348. https://doi.org/10.3390/nu13041348
APA StyleNerurkar, P. V., Gandhi, K., & Chen, J. J. (2021). Correlations between Coffee Consumption and Metabolic Phenotypes, Plasma Folate, and Vitamin B12: NHANES 2003 to 2006. Nutrients, 13(4), 1348. https://doi.org/10.3390/nu13041348