
Assessment of Foods Associated with Sodium and Potassium Intake in Japanese Youths Using the Brief-Type Self-Administered Diet History Questionnaire


Abstract
:
1. Introduction
2. Materials and Methods
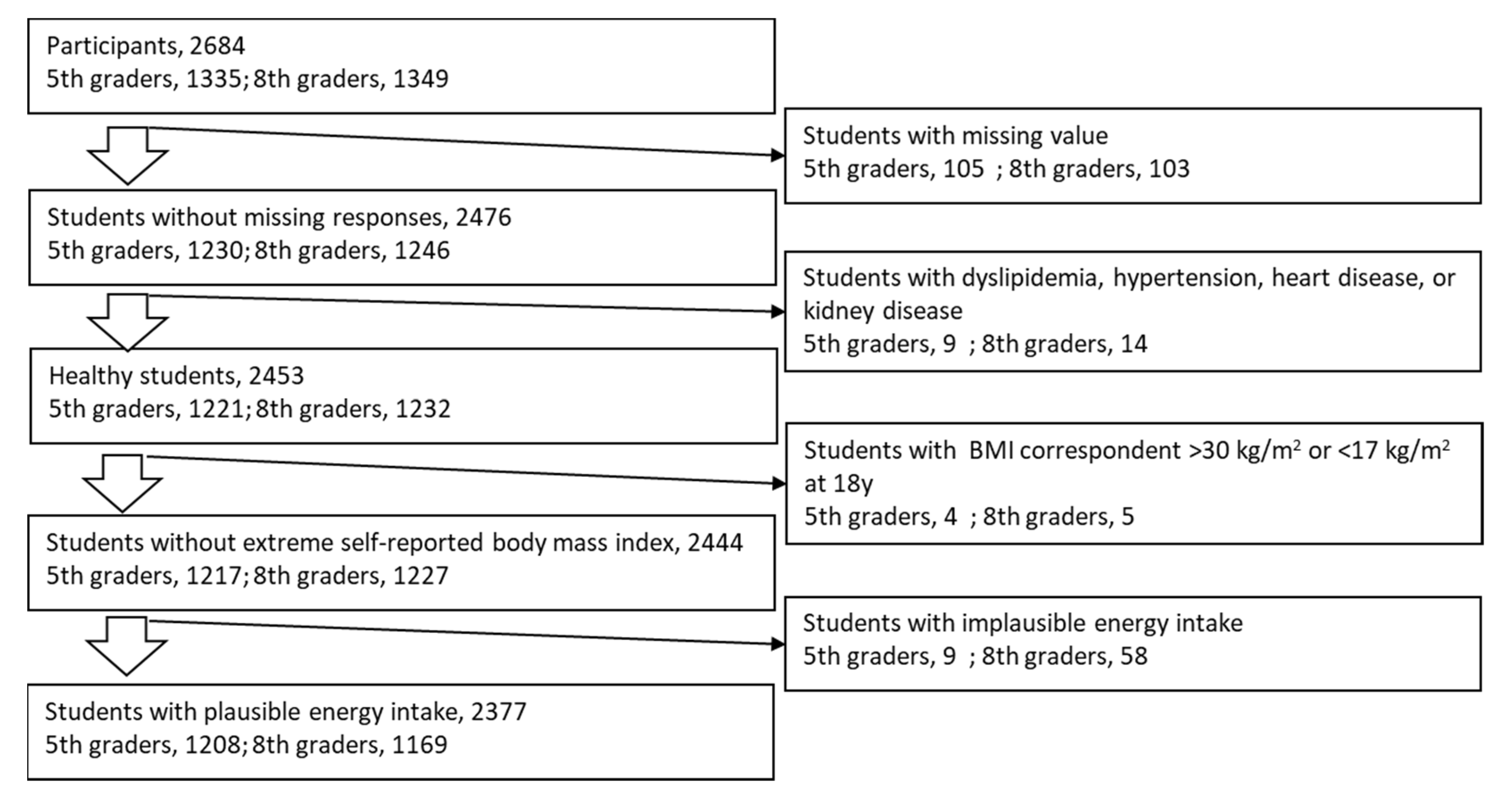
2.1. Subjects
2.2. Dietary Assessment
2.3. Urinalysis
2.4. Confounders
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Foods Associated with Sodium, Potassium, and Sodium-to-Potassium Ratio
4.2. Sodium Intake
4.3. Potassium Intake
4.4. Simple Questionnaires
4.5. Meeting the References
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Aparicio, A.; Rodríguez-Rodríguez, E.; Cuadrado-Soto, E.; Navia, B.; López-Sobaler, A.M.; Ortega, R.M. Estimation of salt intake assessed by urinary excretion of sodium over 24 h in Spanish subjects aged 7–11 years. Eur. J. Nutr. 2015, 56, 171–178. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Marrero, N.M.; MacGregor, G.A. Salt and blood pressure in children and adolescents. J. Hum. Hypertens. 2007, 22, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leyvraz, M.; Chatelan, A.; Da Costa, B.R.; Taffé, P.; Paradis, G.; Bovet, P.; Bochud, M.; Chiolero, A. Sodium intake and blood pressure in children and adolescents: A systematic review and meta-analysis of experimental and observational studies. Int. J. Epidemiol. 2018, 47, 1796–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rios-Leyvraz, M.; Bloetzer, C.; Chatelan, A.; Bochud, M.; Burnier, M.; Santschi, V.; Paradis, G.; Tabin, R.; Bovet, P.; Chiolero, A. Sodium intake and blood pressure in children with clinical conditions: A systematic review with meta-analysis. J. Clin. Hypertens. 2018, 21, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Y. Tracking of Blood Pressure from Childhood to Adulthood. Circulation 2008, 117, 3171–3180. [Google Scholar] [CrossRef] [Green Version]
- Toschke, A.M.; Kohl, L.; Mansmann, U.; Von Kries, R. Meta-analysis of blood pressure tracking from childhood to adulthood and implications for the design of intervention trials. Acta Paediatr. 2009, 99, 24–29. [Google Scholar] [CrossRef]
- WHO. Guideline: Sodium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012; ISBN 978-92-4-150483-6. [Google Scholar]
- Binia, A.; Jaeger, J.; Hu, Y.; Singh, A.; Zimmermann, D. Daily potassium intake and sodium-to-potassium ratio in the reduction of blood pressure: A meta-analysis of randomized controlled trials. J. Hypertens. 2015, 33, 1509–1520. [Google Scholar] [CrossRef]
- Perez, V.; Chang, E.T. Sodium-to-Potassium Ratio and Blood Pressure, Hypertension, and Related Factors. Adv. Nutr. 2014, 5, 712–741. [Google Scholar] [CrossRef]
- Geleijnse, J.M.; Grobbee, D.; Hofman, A. Sodium and potassium intake and blood pressure change in childhood. BMJ 1990, 300, 899–902. [Google Scholar] [CrossRef] [Green Version]
- Buendia, J.R.; Bradlee, M.L.; Daniels, S.R.; Singer, M.R.; Moore, L.L. Longitudinal Effects of Dietary Sodium and Potassium on Blood Pressure in Adolescent Girls. JAMA Pediatr. 2015, 169, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Aguayo, A.G.; Campino, C.; Rodriguez-Fernandez, M.; Poggi, H.; D’Apremont, I.; Moore, R.; Garcia, H.; Solari, S.; Allende, F.; Peredo, S.; et al. Urinary sodium-to-potassium ratio and plasma renin and aldosterone concentrations in normotensive children: Implications for the interpretation of results. J. Hypertens. 2020, 38, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Trieu, K.; Neal, B.; Hawkes, C.; Dunford, E.; Campbell, N.R.C.; Rodriguez-Fernandez, R.; Legetic, B.; McLaren, L.; Barberio, A.; Webster, J. Salt Reduction Initiatives around the World—A Systematic Review of Progress towards the Global Target. PLoS ONE 2015, 10, e0130247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, C.A.; Appel, L.J.; Okuda, N.; Brown, I.J.; Chan, Q.; Zhao, L.; Ueshima, H.; Kesteloot, H.; Miura, K.; Curb, J.D.; et al. Dietary Sources of Sodium in China, Japan, the United Kingdom, and the United States, Women and Men Aged 40 to 59 Years: The INTERMAP Study. J. Am. Diet. Assoc. 2010, 110, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyseni, L.; Elliot-Green, A.; Lloyd-Williams, F.; Kypridemos, C.; O’Flaherty, M.; McGill, R.; Orton, L.; Bromley, H.; Cappuccio, F.P.; Capewell, S. Systematic review of dietary salt reduction policies: Evidence for an effectiveness hierarchy? PLoS ONE 2017, 12, e0177535. [Google Scholar] [CrossRef] [Green Version]
- Asakura, K.; Uechi, K.; Masayasu, S.; Sasaki, S. Sodium sources in the Japanese diet: Difference between generations and sexes. Public Health Nutr. 2016, 19, 2011–2023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimes, C.A.; Campbell, K.J.; Riddell, L.J.; Nowson, C.A. Sources of sodium in Australian children’s diets and the effect of the application of sodium targets to food products to reduce sodium intake. Br. J. Nutr. 2010, 105, 468–477. [Google Scholar] [CrossRef] [Green Version]
- Blanco-Metzler, A.; Núñez-Rivas, H.; Vega-Solano, J.; Montero-Campos, M.; Benavides-Aguilar, K.; Cubillo-Rodríguez, N. Household Cooking and Eating out: Food Practices and Perceptions of Salt/Sodium Consumption in Costa Rica. Int. J. Environ. Res. Public Health 2021, 18, 1208. [Google Scholar] [CrossRef]
- Uechi, K.; Kobayashi, S.; Sugimoto, M.; Sasaki, S. Urine 24-Hour Sodium Excretion Decreased between 1953 and 2014 in Japan, but Estimated Intake Still Exceeds the WHO Recommendation. J. Nutr. 2017, 147, 390–397. [Google Scholar] [CrossRef] [Green Version]
- Yasutake, K.; Miyoshi, E.; Kajiyama, T.; Umeki, Y.; Misumi, Y.; Horita, N.; Murata, Y.; Ohe, K.; Enjoji, M.; Tsuchihashi, T. Comparison of a salt check sheet with 24-h urinary salt excretion measurement in local residents. Hypertens. Res. 2016, 39, 879–885. [Google Scholar] [CrossRef]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both Comprehensive and Brief Self-Administered Diet History Questionnaires Satisfactorily Rank Nutrient Intakes in Japanese Adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, S.; Tsuchihashi, T.; Oniki, H.; Tominaga, M.; Arakawa, K.; Sakaki, M.; Kitazono, T. Relationship between salt intake as estimated by a brief self-administered diet-history questionnaire (BDHQ) and 24-h urinary salt excretion in hypertensive patients. Hypertens. Res. 2015, 38, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Okuda, M.; Sasaki, S.; Bando, N.; Hashimoto, M.; Kunitsugu, I.; Sugiyama, S.; Terao, J.; Hobara, T. Carotenoid, Tocopherol, and Fatty Acid Biomarkers and Dietary Intake Estimated by Using a Brief Self-Administered Diet History Questionnaire for Older Japanese Children and Adolescents. J. Nutr. Sci. Vitaminol. 2009, 55, 231–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okuda, M.; Asakura, K.; Sasaki, S. Protein Intake Estimated from Brief-Type Self-Administered Diet History Questionnaire and Urinary Urea Nitrogen Level in Adolescents. Nutrients 2019, 11, 319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okuda, M.; Sugiyama, S.; Kunitsugu, I.; Hinoda, Y.; Okuda, Y.; Shirabe, K.; Yoshitake, N.; Hobara, T. Use of Body Mass Index and Percentage Overweight Cutoffs to Screen Japanese Children and Adolescents for Obesity-Related Risk Factors. J. Epidemiol. 2010, 20, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinozaki, K.; Okuda, M.; Kunitsugu, I.; Shigeta, M.; Sasaki, S. Dietary Fiber Consumption Decreases the Risks of Overweight and Hypercholesterolemia in Japanese Children. Ann. Nutr. Metab. 2015, 67, 58–64. [Google Scholar] [CrossRef]
- Ito, S.; Sasaki, S. Dietary Reference Intakes for Japanese; Daiichi-Shuppan: Tokyo, Japan, 2020; ISBN 978-4-8041-1408-8. [Google Scholar]
- Okuda, M.; Asakura, K.; Sasaki, S. Estimation of daily sodium and potassium excretion from overnight urine of Japanese children and adolescents. Environ. Health Prev. Med. 2020, 25, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, J.T.; Patterson, K.Y.; Bodner, J.; Douglas, L.W.; Veillon, C.; Kelsay, J.L.; Mertz, W.; Smith, J.C. Sodium and potassium intake and balance in adults consuming self-selected diets. Am. J. Clin. Nutr. 1984, 40, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Okuda, N.; Okayama, A.; Miura, K.; Yoshita, K.; Saito, S.; Nakagawa, H.; Sakata, K.; Miyagawa, N.; Chan, Q.; Elliott, P.; et al. Food sources of dietary sodium in the Japanese adult population: The international study of macro-/micronutrients and blood pressure (INTERMAP). Eur. J. Nutr. 2016, 56, 1269–1280. [Google Scholar] [CrossRef]
- Yoshitake, N.; Okuda, M.; Sasaki, S.; Kunitsugu, I.; Hobara, T. Validity of self-reported body mass index of Japanese children and adolescents. Pediatr. Int. 2012, 54, 397–401. [Google Scholar] [CrossRef]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The lms method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef]
- Kato, N.; Takimoto, H.; Sudo, N. The Cubic Functions for Spline Smoothed L, S and M Values for BMI Reference Data of Japanese Children. Clin. Pediatr. Endocrinol. 2011, 20, 47–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, K.; Miyata, K.; Mohri, M.; Origuchi, H.; Yamamoto, H. The Effects of the Habitual Consumption of Miso Soup on the Blood Pressure and Heart Rate of Japanese Adults: A Cross-sectional Study of a Health Examination. Intern. Med. 2017, 56, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakasugi, M.; Kazama, J.J.; Narita, I. Associations between the Intake of Miso Soup and Japanese Pickles and the Estimated 24-hour Urinary Sodium Excretion: A Population-based Cross-sectional Study. Intern. Med. 2015, 54, 903–910. [Google Scholar] [CrossRef] [Green Version]
- Iwahori, T.; Miura, K.; Ueshima, H. Time to Consider Use of the Sodium-to-Potassium Ratio for Practical Sodium Reduction and Potassium Increase. Nutrients 2017, 9, 700. [Google Scholar] [CrossRef]
- Rauber, F.; Louzada, M.L.D.C.; Steele, E.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okuda, M.; Asakura, K.; Sasaki, S. Placing Salt/Soy Sauce at Dining Tables and Out-of-Home Behavior Are Related to Urinary Sodium Excretion in Japanese Secondary School Students. Nutrients 2017, 9, 1290. [Google Scholar] [CrossRef] [Green Version]
- Stewart, C.P. Loss of Nutrients in Cooking. Proc. Nutr. Soc. 1946, 4, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Eaton, S.; Konner, M. Review Paleolithic nutrition revisited: A twelve-year retrospective on its nature and implications. Eur. J. Clin. Nutr. 1997, 51, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Kimura, M.; Itokawa, Y. Cooking losses of minerals in foods and its nutritional significance. J. Nutr. Sci. Vitaminol. 1990, 36 (Suppl. S1), S25. [Google Scholar] [CrossRef]
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; Beckford, K.; Baxter, J.R.; He, F.J.; Nowson, C. Dietary intake and sources of sodium and potassium among Australian schoolchildren: Results from the cross-sectional Salt and Other Nutrients in Children (SONIC) study. BMJ Open 2017, 7, e016639. [Google Scholar] [CrossRef] [Green Version]
- Okuda, N.; Okayama, A.; Miura, K.; Yoshita, K.; Miyagawa, N.; Saitoh, S.; Nakagawa, H.; Sakata, K.; Chan, Q.; Elliott, P.; et al. Food Sources of Dietary Potassium in the Adult Japanese Population: The International Study of Macro-/Micronutrients and Blood Pressure (INTERMAP). Nutrients 2020, 12, 787. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, S.; Yanagibori, R.; Amano, K. Self-Administered Diet History Questionnaire Developed for Health Education: A Relative Validation of the Test-Version by Comparison with 3-Day Diet Record in Women. J. Epidemiol. 1998, 8, 203–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, K.; Masuda, A.; Uezono, K.; Kawasaki, T. Assessment of Dietary Intake Estimation Using a Simple Questionnaire Method. Nippon. Eiyo Shokuryo Gakkaishi 1992, 45, 535–543. [Google Scholar] [CrossRef]
- Tsuchihashi, T.; Masuda, K.; Oniki, H.; Sakaki, M.; Arakawa, H.; Kameda, W.; Fukui, H. Validity of salt check sheet in hepertesive patients: Assessment of salt intake by using a simple check sheet in hypertensive patients. J. Blood Press. 2013, 20, 1239–1243. [Google Scholar]
- Seko, C.; Odani, K.; Wada, S.; Yoshii, K.; Segawa, H.; Kitaoka, K.; Masumoto, T.; Higashi, A. Characteristic dietary habits associated with high values of estimated 24-hours urinary sodium excretion and sodium-to-potassium ratio assessed by age group among the residents of a rural town in Japan. Clin. Exp. Hypertens. 2019, 42, 449–459. [Google Scholar] [CrossRef]
- Fujiwara, T.; Kikuchi, K.; Hoshide, S.; Tsuchihashi, T.; Kario, K. Usefulness of a salt check sheet for elementary school and junior high school children. J. Clin. Hypertens. 2019, 21, 722–729. [Google Scholar] [CrossRef] [Green Version]
- Morimoto, A.; Takase, S.; Hada, K.; Hosoya, N. Evaluation of a Covinient Method for the estimation of dietary food consumption. Jap. J. Nutr. 1977, 35, 235–245. [Google Scholar] [CrossRef]
- Sougawa, Y.; Miyai, N.; Morioka, I.; Utsumi, M.; Takeda, S.; Miyashita, K.; Arita, M. The combination of obesity and high salt intake are associated with blood pressure elevation among healthy Japanese adolescents. J. Hum. Hypertens. 2020, 34, 117–124. [Google Scholar] [CrossRef]
- Armstrong, B.K.; White, E.; Saracci, R. Principles of Exposure Measurement in Epidemiology: Monographs in Epidemiology and Biostatistics; Oxford University Press: New York, NY, USA, 1992; ISBN 978-0192617057. [Google Scholar]
- Willet, W. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 2013; ISBN 978-0-19-975403-8. [Google Scholar]


{kind=link}
{kind=link}
| Food Groups | Food Items |
|---|---|
| Meat | Poultry, meat, processed meat, liver |
| Fish | Squid and octopus, shellfish, fish with bone, tuna, oily fish, dried fish, lean fish, fish paste |
| Vegetables | Raw vegetables used in salad, green leafy vegetables, broccoli, cabbage, Chinese cabbage, carrots, pumpkins, radishes and turnips, other root vegetables (onions, burdock, lotus root), tomato sauce, boiled tomato and stewed tomato, salted vegetable pickles |
| Fruits | Citrus fruits, strawberries, persimmons, kiwi fruit, other fruits |
| Cereals | Bread: including white bread and sweet Japanese bread Noodles: buckwheat noodles, Japanese wheat noodles; instant noodles, Chinese noodles, spaghetti, macaroni |
| Seasonings/condiments | Butter, margarine, jams, mayonnaise, ketchup, soy, and other sauces |
| Fermented soybean paste (miso) | |
| Noodle soup | |
| Confectionaries | Cookies, biscuits, Japanese sweets, rice crackers, rice cakes, Japanese-style pancakes, snack confectionaries |
| Beverages | Green tea, black tea, oolong tea, coffee, fruits and vegetable juice, sugar-sweetened beverages |
| Sugar-sweetened beverages | Cola, sweetened soft drink, coffee with milk, lactobacillus beverage |
| Dairy products | Milk, low-fat milk, yogurt, cheese |
| n = 2377 | |
|---|---|
| Age, years | 12.05 ± 1.54 |
| Male: female | 1207: 1170 |
| Height, cm | 147.4 ± 11.2 |
| Weight, kg | 39.9 ± 9.9 |
| Body mass index, kg/m2 | 18.10 ± 2.59 |
| zBMI | 0.02 ± 1.03 |
| BDHQ | |
| Energy | 2005 ± 570 |
| NaBDHQ, mg/day | 4179 ± 1162 |
| NaBDHQ, mg/day·1000 kcal | 2123 ± 402 |
| KBDHQ, mg/day | 2491 ± 777 |
| KBDHQ, mg/day·1000 kcal | 1260 ± 263 |
| Na/KBDHQ ratio, mol/mol | 3.4 ± 1.7 |
| Urinary Excretion | |
| Naex, mg/day | 3394 ± 2071 |
| Naex/weight, mg/day·kg | 86.6 ± 4702 |
| Kex, mg/day | 1759 ± 1275 |
| Kex/weight, mg/day·kg | 44.9 ± 31.2 |
| Na/Kex ratio, mol/mol | 2.7 ± 0.6 |
| Urinary Excretion | ||||
|---|---|---|---|---|
| Raw Values, mg/day | Weight Adjusted Values, mg/day·kg | |||
| Rho | p | Rho | p | |
| NaBDHQ, mg/day | 0.048 | 0.031 | 0.037 | 0.074 |
| NaBDHQ, mg/day·1000 kcal | 0.044 | 0.081 | 0.036 | 0.081 |
| KBDHQ, mg/day | 0.091 | <0.001 | 0.108 | <0.001 |
| KBDHQ, mg/day·1000 kcal | 0.110 | <0.001 | 0.130 | <0.001 |
| Na/KBDHQratio, mol/mol | 0.096 | <0.001 | 0.130 | <0.001 |
| Naex (mg/day) | Kex (mg/day) | Na/Kex Ratio | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | ptrend | Q1 | Q2 | Q3 | Q4 | Q5 | ptrend | Q1 | Q2 | Q3 | Q4 | Q5 | ptrend | |
| Cereals | 3376 | 3451 | 3463 | 3371 | 3576 | 0.289 | 1763 | 1832 | 1734 | 1684 | 1784 | 0.573 | 3.3 | 3.3 | 3.4 | 3.4 | 3.5 | 0.065 |
| Bread | 3447 | 3442 | 3495 | 3371 | 3481 | 0.990 | 1870 | 1686 | 1670 | 1806 | 1765 | 0.618 | 3.2 | 3.5 | 3.5 | 3.4 | 3.3 | 0.762 |
| Noodles | 3358 | 3440 | 3495 | 3406 | 3538 | 0.272 | 1743 | 1727 | 1819 | 1777 | 1730 | 0.898 | 3.3 | 3.4 | 3.4 | 3.3 | 3.6 | 0.070 |
| Vegetables | 3375 | 3352 | 3577 | 3531 | 3400 | 0.438 | 1777 | 1692 | 1748 | 1798 | 1782 | 0.517 | 3.4 | 3.4 | 3.5 | 3.4 | 3.3 | 0.308 |
| Pickles | 3281 | 3405 | 3411 | 3579 | 3600 | 0.005 | 1694 | 1680 | 1732 | 1855 | 1831 | 0.012 | 3.3 | 3.4 | 3.4 | 3.4 | 3.5 | 0.129 |
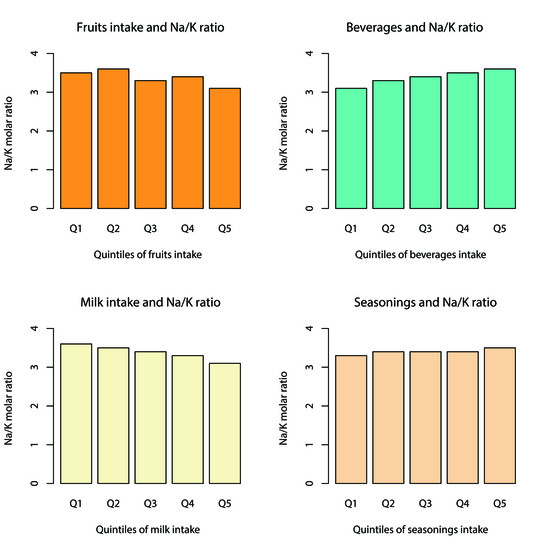
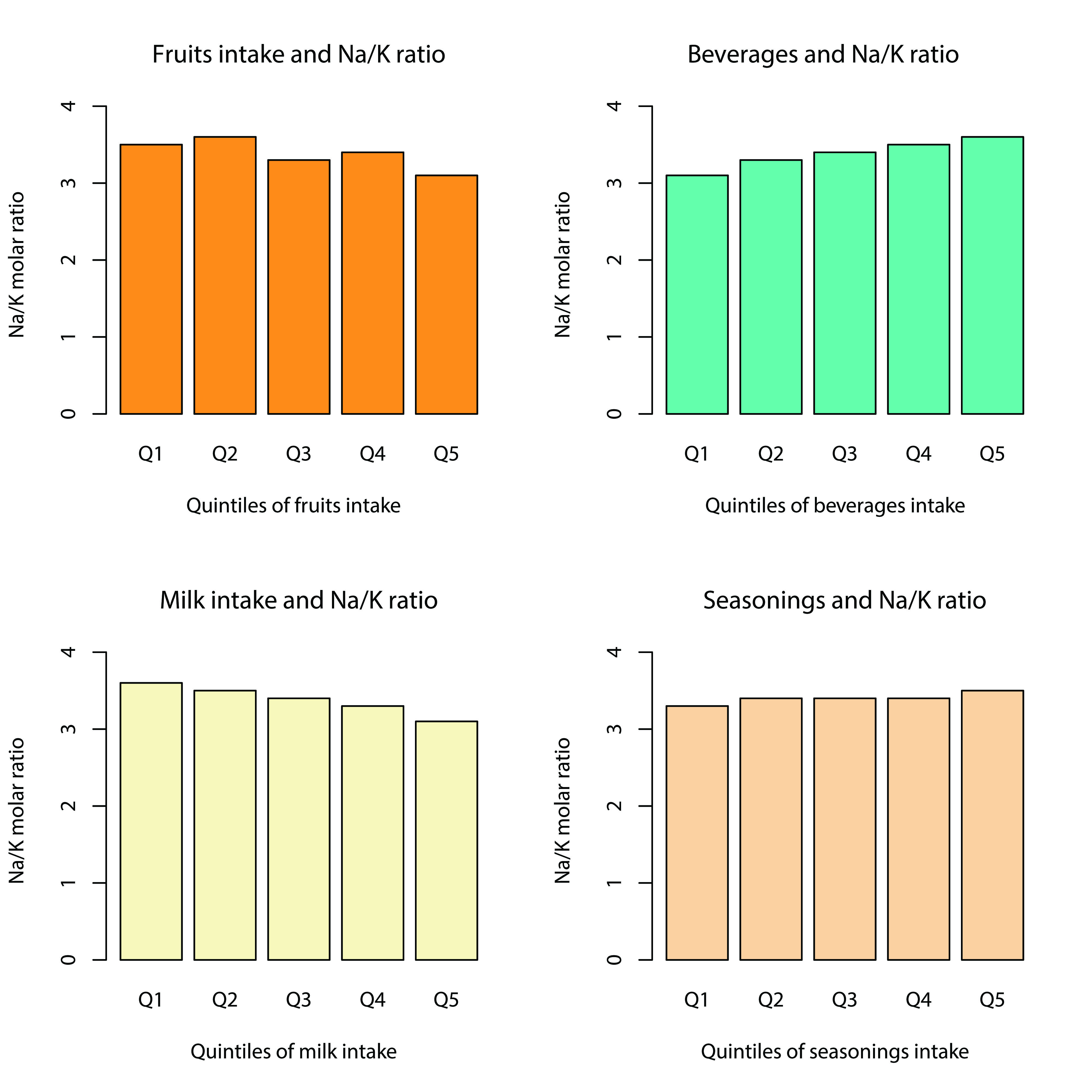
| Fruits | 3408 | 3608 | 3403 | 3490 | 3327 | 0.349 | 1695 | 1726 | 1759 | 1759 | 1858 | 0.048 | 3.5 | 3.6 | 3.3 | 3.4 | 3.1 | <0.001 |
| Fish | 3501 | 3437 | 3444 | 3434 | 3421 | 0.581 | 1727 | 1779 | 1770 | 1812 | 1708 | 0.973 | 3.5 | 3.4 | 3.4 | 3.3 | 3.4 | 0.266 |
| Salty fish | 3455 | 3599 | 3399 | 3409 | 3375 | 0.238 | 1779 | 1714 | 1804 | 1757 | 1742 | 0.861 | 3.3 | 3.6 | 3.3 | 3.4 | 3.3 | 0.184 |
| Meat | 3488 | 3477 | 3360 | 3490 | 3421 | 0.685 | 1754 | 1740 | 1803 | 1772 | 1727 | 0.906 | 3.4 | 3.4 | 3.3 | 3.4 | 3.4 | 0.722 |
| Processed meat | 3378 | 3536 | 3470 | 3362 | 3490 | 0.864 | 1738 | 1812 | 1715 | 1758 | 1772 | 0.939 | 3.4 | 3.4 | 3.5 | 3.3 | 3.4 | 0.875 |
| Dairy product | 3436 | 3528 | 3429 | 3376 | 3467 | 0.279 | 1608 | 1768 | 1690 | 1799 | 1932 | <0.001 | 3.6 | 3.5 | 3.4 | 3.3 | 3.1 | <0.001 |
| Confectionaries | 3518 | 3604 | 3315 | 3376 | 3423 | 0.162 | 1781 | 1856 | 1785 | 1687 | 1688 | 0.053 | 3.4 | 3.3 | 3.3 | 3.5 | 3.5 | 0.226 |
| Japanese conf. | 3576 | 3471 | 3419 | 3461 | 3307 | 0.064 | 1774 | 1745 | 1791 | 1784 | 1701 | 0.558 | 3.4 | 3.5 | 3.4 | 3.3 | 3.3 | 0.213 |
| Beverages | 3423 | 3436 | 3397 | 3498 | 3482 | 0.553 | 1910 | 1783 | 1710 | 1721 | 1673 | 0.004 | 3.1 | 3.3 | 3.4 | 3.5 | 3.6 | <0.001 |
| SSBs | 3540 | 3427 | 3328 | 3461 | 3481 | 0.775 | 1882 | 1687 | 1826 | 1764 | 1639 | 0.024 | 3.3 | 3.5 | 3.3 | 3.3 | 3.5 | 0.218 |
| Seasonings/condiments | 3419 | 3456 | 3455 | 3526 | 3379 | 0.977 | 1767 | 1801 | 1775 | 1751 | 1702 | 0.326 | 3.3 | 3.4 | 3.4 | 3.4 | 3.5 | 0.039 |
| Soy and other sauces | 3343 | 3386 | 3609 | 3495 | 3402 | 0.604 | 1735 | 1751 | 1827 | 1706 | 1777 | 0.828 | 3.3 | 3.4 | 3.4 | 3.3 | 3.6 | 0.099 |
| Noodle soup | 3362 | 3506 | 3428 | 3335 | 3606 | 0.287 | 1728 | 1830 | 1807 | 1731 | 1701 | 0.567 | 3.3 | 3.2 | 3.5 | 3.5 | 3.5 | 0.060 |
| Soybean paste (miso) | 3238 | 3358 | 3436 | 3473 | 3733 | <0.001 | 1650 | 1693 | 1791 | 1760 | 1903 | 0.002 | 3.4 | 3.4 | 3.3 | 3.4 | 3.4 | 0.945 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okuda, M.; Sasaki, S. Assessment of Foods Associated with Sodium and Potassium Intake in Japanese Youths Using the Brief-Type Self-Administered Diet History Questionnaire. Nutrients 2021, 13, 2345. https://doi.org/10.3390/nu13072345
Okuda M, Sasaki S. Assessment of Foods Associated with Sodium and Potassium Intake in Japanese Youths Using the Brief-Type Self-Administered Diet History Questionnaire. Nutrients. 2021; 13(7):2345. https://doi.org/10.3390/nu13072345
Chicago/Turabian StyleOkuda, Masayuki, and Satoshi Sasaki. 2021. "Assessment of Foods Associated with Sodium and Potassium Intake in Japanese Youths Using the Brief-Type Self-Administered Diet History Questionnaire" Nutrients 13, no. 7: 2345. https://doi.org/10.3390/nu13072345
APA StyleOkuda, M., & Sasaki, S. (2021). Assessment of Foods Associated with Sodium and Potassium Intake in Japanese Youths Using the Brief-Type Self-Administered Diet History Questionnaire. Nutrients, 13(7), 2345. https://doi.org/10.3390/nu13072345