
The Association of Nighttime Fasting Duration and Prostate Cancer Risk: Results from the Multicase-Control (MCC) Study in Spain

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
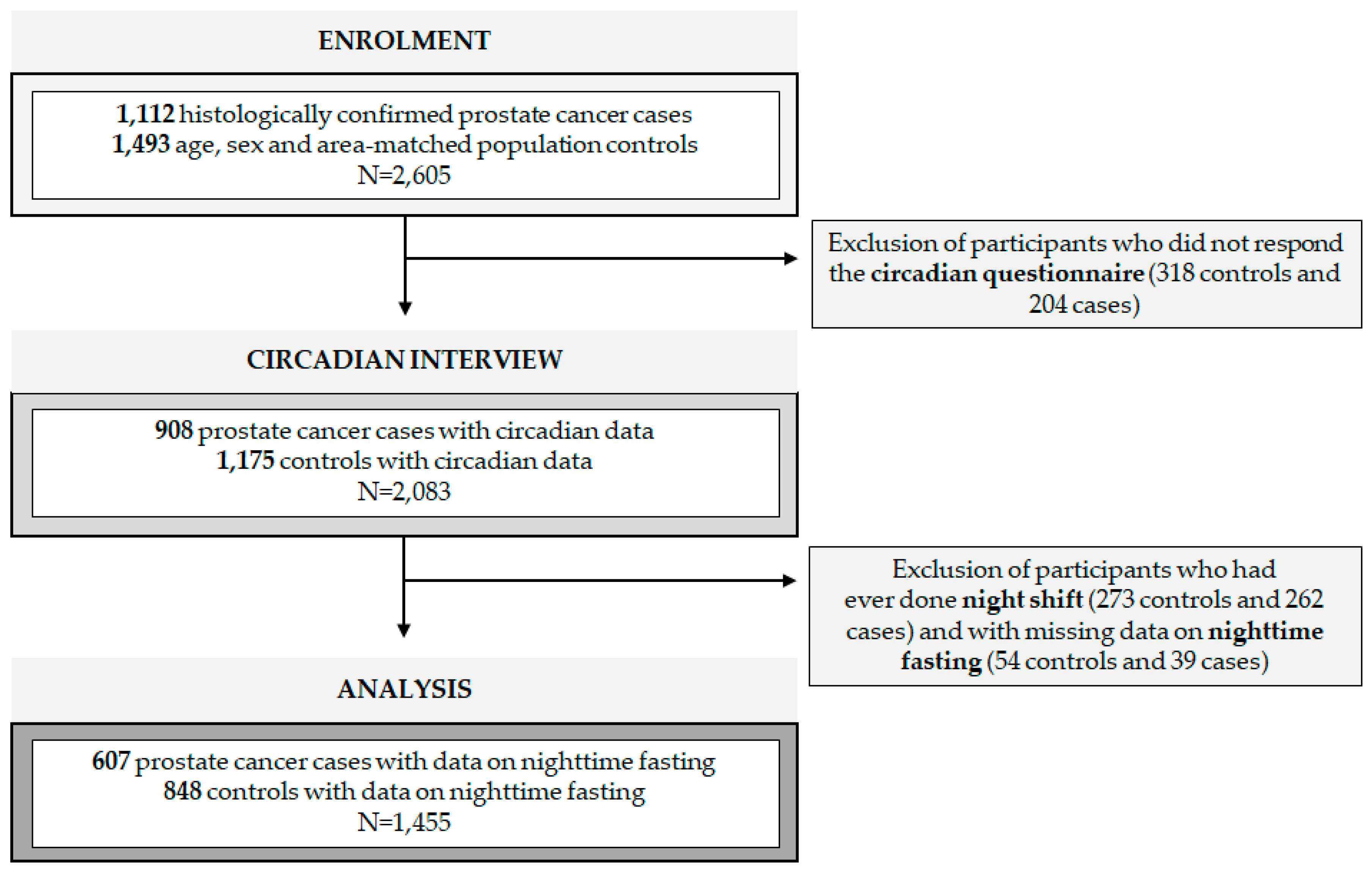
2.1. Study Population
2.2. Data Collection
2.3. Exposure and Outcome Assessment
2.4. Statistical Analyses
2.5. Sensitivity Analyses
3. Results
3.1. Study Population
3.2. Nighttime Fasting and Prostate Cancer Risk
3.3. Prostate Cancer Risk Stratified by Time of First Intake
3.4. Association Combining Nighttime Fasting Duration and Time of Breakfast with Prostate Cancer Risk
3.5. Prostate Cancer Risk Stratified by Chronotype
3.6. Relative Risk among Cancer Subtypes
3.7. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sociedad Española de Oncología Médica (SEOM). Las Cifras del Cáncer en España. 2021. Available online: https://seom.org/images/Cifras_del_cancer_en_Espnaha_2021.pdf (accessed on 4 February 2021).
- Patel, A.R.; Klein, E.A. Risk factors for prostate cancer. Nat. Clin. Pr. Urol. 2009, 6, 87–95. [Google Scholar] [CrossRef]
- Ward, E.; Germolec, D.; Kogevinas, M.; McCormick, D.; Vermeulen, R.; Anisimov, V.; Aronson, K.; Bhatti, P.; Cocco, P.; Costa, G.; et al. Carcinogenicity of night shift work. Lancet Oncol. 2019, 20, 1058–1059. [Google Scholar] [CrossRef]
- Straif, K.; Baan, R.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Bouvard, V.; Altieri, A.; Benbrahim-Tallaa, L.; Cogliano, V.; WHO International Agency For Research on Cancer Monograph Working Group. Carcinogenicity of shift-work, painting, and fire-fighting. Lancet Oncol. 2007, 8, 1065–1066. [Google Scholar] [CrossRef]
- Challet, E. The circadian regulation of food intake. Nat. Rev. Endocrinol. 2019, 15, 393–405. [Google Scholar] [CrossRef]
- Garcia-Saenz, A.; Miguel, A.S. de Espinosa, A.; Valentin, A.; Aragonés, N.; Llorca, J.; Amiano, P.; Sánchez, V.M.; Guevara, M.; Capelo, R.; et al. Evaluating the Association between Artificial Light-at-Night Exposure and Breast and Prostate Cancer Risk in Spain (MCC-Spain Study). Environ. Health Perspect. 2018, 126, 47011. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.Y.; Lee, E.; Kim, Y.J.; Kim, J. The association between artificial light at night and prostate cancer in Gwangju City and South Jeolla Province of South Korea. Chronobiol. Int. 2017, 34, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Gapstur, S.M.; Diver, W.R.; Stevens, V.L.; Carter, B.D.; Teras, L.R.; Jacobs, E.J. Work schedule, sleep duration, insomnia, and risk of fatal prostate cancer. Am. J. Prev. Med. 2014, 46, S26–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigurdardottir, L.G.; Markt, S.C.; Rider, J.R.; Haneuse, S.; Fall, K.; Schernhammer, E.S.; Tamimi, R.M.; Flynn-Evans, E.; Batista, J.L.; Launer, L.; et al. Urinary melatonin levels, sleep disruption, and risk of prostate cancer in elderly men. Eur. Urol. 2015, 67, 191–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigurdardottir, L.G.; Valdimarsdottir, U.A.; Mucci, L.A.; Fall, K.; Rider, J.R.; Schernhammer, E.; Czeisler, C.A.; Launer, L.; Harris, T.; Stampfer, M.J.; et al. Sleep disruption among older men and risk of prostate cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 872–879. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Zheng, T.; Stevens, R.G.; Zhang, Y.; Boyle, P. Does “clock” matter in prostate cancer? Cancer Epidemiol. Biomark. Prev. 2006, 15, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srour, B.; Plancoulaine, S.; Andreeva, V.A.; Fassier, P.; Julia, C.; Galan, P.; Hercberg, S.; Deschasaux, M.; Latino-Martel, P.; Touvier, M. Circadian nutritional behaviours and cancer risk: New insights from the NutriNet-santé prospective cohort study: Disclaimers. Int. J. Cancer 2018, 143, 2369–2379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogevinas, M.; Espinosa, A.; Castelló, A.; Gómez-Acebo, I.; Guevara, M.; Martin, V.; Amiano, P.; Alguacil, J.; Peiro, R.; Moreno, V.; et al. Effect of mistimed eating patterns on breast and prostate cancer risk (MCC-Spain Study). Int. J. Cancer 2018, 143, 2380–2389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Zheng, C.; Xu, C.; Liu, Q.; Wang, J.; Hong, Y.; Zhao, P. Nighttime snacking is associated with risk of obesity and hyperglycemia in adults: A cross-sectional survey from Chinese adult teachers. J. Biomed. Res. 2017, 31, 541–547. [Google Scholar]
- Continuous Update Project: Diet, Nutrition, Physical Activity and the Prevention of Cancer. Summary of Strong Evidence. 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Summary-of-Third-Expert-Report-2018.pdf (accessed on 10 March 2021).
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesztyüs, D.; Cermak, P.; Gulich, M.; Kesztyüs, T. Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre-Post Design. Nutrients 2019, 11, 2854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinac, C.R.; Natarajan, L.; Sears, D.D.; Gallo, L.C.; Hartman, S.J.; Arredondo, E.; Patterson, R.E. Prolonged Nightly Fasting and Breast Cancer Risk: Findings from NHANES (2009–2010). Cancer Epidemiol. Biomark. Prev. 2015, 24, 783–789. [Google Scholar] [CrossRef] [Green Version]
- Marinac, C.R.; Sears, D.D.; Natarajan, L.; Gallo, L.C.; Breen, C.I.; Patterson, R.E. Frequency and Circadian Timing of Eating May Influence Biomarkers of Inflammation and Insulin Resistance Associated with Breast Cancer Risk. PLoS ONE 2015, 10, e0136240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinac, C.R.; Nelson, S.H.; Breen, C.I.; Hartman, S.J.; Natarajan, L.; Pierce, J.P.; Flatt, S.W.; Sears, D.D.; Patterson, R.E. Prolonged Nightly Fasting and Breast Cancer Prognosis. JAMA Oncol. 2016, 2, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Nas, A.; Mirza, N.; Hägele, F.; Kahlhöfer, J.; Keller, J.; Rising, R.; Kufer, T.A.; Bosy-Westphal, A. Impact of breakfast skipping compared with dinner skipping on regulation of energy balance and metabolic risk. Am. J. Clin. Nutr. 2017, 105, 1351–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaño-Vinyals, G.; Aragonés, N.; Pérez-Gómez, B.; Martín, V.; Llorca, J.; Moreno, V.; Altzibar, J.M.; Ardanaz, E.; de Sanjosé, S.; Jiménez-Moleón, J.J.; et al. Population-based multicase-control study in common tumors in Spain (MCC-Spain): Rationale and study design. Gac. Sanit. 2015, 29, 308–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreiras, O.; Cabrera, L.; Cuadrado, C.; Carbajal, A. Tablas de Composición de Alimentos; Pirámide: Madrid, Spain, 2003. [Google Scholar]
- Romaguera, D.; Gracia-Lavedan, E.; Molinuevo, A.; de Batlle, J.; Mendez, M.; Moreno, V.; Vidal, C.; Castelló, A.; Pérez-Gómez, B.; Martín, V.; et al. Adherence to nutrition-based cancer prevention guidelines and breast, prostate and colorectal cancer risk in the MCC-Spain case-control study. Int. J. Cancer 2017, 141, 83–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, F.; Rome, S.; Mery, F.; Dawson, E.; Montagne, J.; Biro, P.A.; Beckmann, C.; Renaud, F.; Poulin, R.; Raymond, M.; et al. Changes in diet associated with cancer: An evolutionary perspective. Evol. Appl. 2017, 10, 651–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Neuzillet, Y.; Raynaud, J.-P.; Dreyfus, J.-F.; Radulescu, C.; Rouanne, M.; Schneider, M.; Krish, S.; Rouprêt, M.; Drouin, S.J.; Comperat, E.; et al. Aggressiveness of Localized Prostate Cancer: The Key Value of Testosterone Deficiency Evaluated by Both Total and Bioavailable Testosterone: AndroCan Study Results. Horm. Cancer 2019, 10, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liśkiewicz, M.; Ellison, G.T.H. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2017, 45, 1887–1894. [Google Scholar] [CrossRef] [Green Version]
- Weitzer, J.; Castaño-Vinyals, G.; Aragonés, N.; Gómez-Acebo, I.; Guevara, M.; Amiano, P.; Martín, V.; Molina-Barceló, A.; Alguacil, J.; Moreno, V.; et al. Effect of time of day of recreational and household physical activity on prostate and breast cancer risk (MCC-Spain study). Int. J. Cancer 2021, 148, 1360–1371. [Google Scholar] [CrossRef] [PubMed]
- De Nunzio, C.; Tubaro, A. Prostate cancer: Diabetes and prostate cancer--an open debate. Nat. Rev. Urol. 2013, 10, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Kasper, J.S.; Giovannucci, E. A meta-analysis of diabetes mellitus and the risk of prostate cancer. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2056–2062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Jiang, H.W.; Ding, G.X.; Zhang, H.; Zhang, L.M.; Mao, S.H.; Ding, Q. Diabetes mellitus and prostate cancer risk of different grade or stage: A systematic review and meta-analysis. Diabetes Res. Clin. Pr. 2013, 99, 241–249. [Google Scholar] [CrossRef]
- Patterson, R.E.; Laughlin, G.A.; LaCroix, A.Z.; Hartman, S.J.; Natarajan, L.; Senger, C.M.; Martínez, M.E.; Villaseñor, A.; Sears, D.D.; Marinac, C.R.; et al. Intermittent Fasting and Human Metabolic Health. J. Acad. Nutr. Diet. 2015, 115, 1203–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamshed, H.; Beyl, R.A.; Della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queiroz, J.D.N.; Macedo, R.C.O.; Tinsley, G.M.; Reischak-Oliveira, A. Time-restricted eating and circadian rhythms: The biological clock is ticking. Crit. Rev. Food Sci. Nutr. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mazri, F.H.; Manaf, Z.A.; Shahar, S.; Mat Ludin, A.F. The Association between Chronotype and Dietary Pattern among Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 17, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Controls (N = 848) | Cases (N = 607) | p-Value | |
|---|---|---|---|
| Mean (SD) or N (%) | Mean (SD) or N (%) | ||
| Age | 66.0 (8.4) | 65.6 (7.0) | 0.372 |
| BMI | 27.5 (3.6) | 27.5 (3.6) | 0.967 |
| Normal weight (<25 kg/m2) | 225 (26.5) | 153 (25.2) | 0.850 |
| Overweight (≥25 to <30 kg/m2) | 439 (51.8) | 320 (52.7) | |
| Obese (≥30 kg/m2) | 184 (21.7) | 134 (22.1) | |
| Educational level | |||
| Less than primary school | 115 (13.6) | 104 (17.1) | <0.001 |
| Primary school | 247 (29.1) | 244 (40.2) | |
| Secondary school | 264 (31.1) | 142 (23.4) | |
| University | 222 (26.2) | 117 (19.3) | |
| Family history of prostate cancer | |||
| No | 793 (93.5) | 506 (83.4) | <0.001 |
| Yes | 55 (6.5) | 101 (16.6) | |
| Smoking | |||
| Never | 242 (28.5) | 171 (28.2) | 0.571 |
| Ex-smoker | 434 (51.2) | 325 (53.5) | |
| Current smoker | 172 (20.3) | 111 (18.3) | |
| Chronotype | |||
| Morning | 419 (50.5) | 306 (50.5) | 0.974 |
| Intermediate | 303 (36.6) | 224 (37.0) | |
| Evening | 107 (12.9) | 76 (12.5) | |
| Unknown | 19 | 1 | |
| WCRF/AICR score | |||
| Low adherence a | 307 (40.1) | 203 (37.3) | 0.004 |
| Medium adherence b | 262 (34.2) | 232 (42.6) | |
| High adherence c | 196 (25.6) | 109 (20.0) | |
| Unknown | 83 | 63 | |
| Diabetes | |||
| No | 671 (79.3) | 518 (85.6) | 0.003 |
| Yes | 175 (20.7) | 87 (14.4) | |
| Unknown | 2 | 2 | |
| Indoor ALAN exposure | |||
| Total darkness | 147 (17.4) | 87 (14.4) | 0.001 |
| Almost dark | 348 (41.2) | 211 (34.9) | |
| Dim light | 261 (30.9) | 204 (33.7) | |
| Quite illuminated | 88 (10.4) | 103 (17.0) | |
| Unknown | 4 | 2 | |
| Breakfast | |||
| No | 17 (2.0) | 3 (0.5) | 0.001 |
| Only weekends | 3 (0.4) | 12 (2.0) | |
| Only weekdays | 15 (1.8) | 16 (2.6) | |
| Always | 809 (95.9) | 575 (94.9) | |
| Unknown | 4 | 1 | |
| Time of breakfast | |||
| 8:30 AM or before | 466 (55.0) | 314 (51.7) | 0.227 |
| After 8:30 AM or skip breakfast | 382 (45.0) | 293 (48.3) | |
| Time of last intake | |||
| 10 PM or later | 294 (34.7) | 227 (37.4) | 0.350 |
| 9:00 to <10 PM | 439 (51.8) | 311 (51.2) | |
| Before 9 PM | 115 (13.6) | 69 (11.4) | |
| Supper/sleep interval | |||
| 1 h or less | 186 (22.2) | 169 (28.1) | 0.034 |
| From >1 to ≤2 h | 327 (39.0) | 223 (37.0) | |
| More than 2 h | 326 (38.9) | 210 (34.9) | |
| Unknown | 9 | 5 | |
| ≤11 h of Fast (N = 474) | >11 h of Fast (N = 374) | p-Value | |
|---|---|---|---|
| Mean (SD) or N (%) | Mean (SD) or N (%) | ||
| Age | 65.5 (8.5) | 66.5 (8.2) | 0.070 |
| BMI | 27.4 (3.5) | 27.6 (3.8) | 0.384 |
| Normal weight (<25 kg/m2) | 121 (25.5) | 104 (27.8) | 0.198 |
| Overweight (≥25 to <30 kg/m2) | 258 (54.4) | 181 (48.4) | |
| Obese (≥30 kg/m2) | 95 (20.0) | 89 (23.8) | |
| Educational level | |||
| Less than primary school | 50 (10.5) | 65 (17.4) | <0.001 |
| Primary school | 115 (24.3) | 132 (35.3) | |
| Secondary school | 161 (34.0) | 103 (27.5) | |
| University | 148 (31.2) | 74 (19.8) | |
| Family history of prostate cancer | |||
| No | 445 (93.9) | 348 (93.0) | 0.727 |
| Yes | 29 (6.1) | 26 (7.0) | |
| Smoking | |||
| Never | 140 (29.5) | 102 (27.3) | 0.191 |
| Ex-smoker | 230 (48.5) | 204 (54.5) | |
| Current smoker | 104 (21.9) | 68 (18.2) | |
| Chronotype | |||
| Morning | 219 (47.1) | 200 (54.9) | 0.080 |
| Intermediate | 181 (38.9) | 122 (33.5) | |
| Evening | 65 (14.0) | 42 (11.5) | |
| Unknown | 9 | 10 | |
| WCRF/AICR score | |||
| Low adherence a | 164 (38.2) | 143 (42.6) | 0.432 |
| Medium adherence b | 154 (35.9) | 108 (32.1) | |
| High adherence c | 111 (25.9) | 85 (25.3) | |
| Unknown | 45 | 38 | |
| Diabetes | |||
| No | 387 (81.8) | 284 (76.1) | 0.052 |
| Yes | 86 (18.2) | 89 (23.9) | |
| Unknown | 1 | 1 | |
| Indoor ALAN exposure | |||
| Total darkness | 63 (13.3) | 84 (22.6) | 0.005 |
| Almost dark | 203 (43.0 | 145 (39.0) | |
| Dim light | 151 (32.0) | 110 (29.6) | |
| Quite illuminated | 55 (11.7) | 33 (8.9) | |
| Unknown | 2 | 2 | |
| Breakfast | |||
| No | 1 (0.2) | 16 (4.3) | <0.001 |
| Only weekends | NA | 3 (0.8) | |
| Only weekdays | 8 (1.7) | 7 (1.9) | |
| Always | 465 (98.1) | 344 (93.0) | |
| Unknown | NA | 4 | |
| Time of breakfast | |||
| 8:30 AM or before | 417 (88.0) | 49 (13.1) | <0.001 |
| After 8:30 AM or skip breakfast | 57 (12.0) | 325 (86.9) | |
| Time of last intake | |||
| 10 PM or later | 215 (45.4) | 79 (21.1) | <0.001 |
| 9:00 to <10 PM | 233 (49.2) | 206 (55.1) | |
| Before 9 PM | 26 (5.5) | 89 (23.8) | |
| Supper/sleep interval | |||
| 1 h or less | 110 (23.6) | 76 (20.4) | 0.553 |
| From >1 to ≤2 h | 178 (38.1) | 149 (40.1) | |
| More than 2 h | 179 (38.3) | 147 (39.5) | |
| Unknown | 7 | 2 | |
| Nighttime Fasting | Controls N (%) | Cases N (%) | OR (95% CI) a | OR (95% CI) b |
|---|---|---|---|---|
| ≤11 h | 474 (55.9) | 342 (56.3) | Ref | Ref |
| >11 h | 374 (44.1) | 265 (43.7) | 0.92 (0.73–1.16) | 0.77 (0.54–1.07) |
| Nighttime Fasting | Controls N (%) | Cases N (%) | OR (95% CI) a | OR (95% CI) b |
|---|---|---|---|---|
| Breakfast at 8:30 AM or before | ||||
| ≤11 h | 417 (89.5) | 293 (93.3) | Ref | Ref |
| >11 h | 49 (10.5) | 21 (6.7) | 0.66 (0.37–1.13) | 0.60 (0.33–1.04) |
| Breakfast after 8:30 AM or skip breakfast | ||||
| ≤11 h | 57 (14.9) | 49 (16.7) | Ref | Ref |
| >11 h | 325 (85.1) | 245 (83.3) | 0.87 (0.57–1.33) | 0.90 (0.58–1.39) |
| Controls N (%) | Cases N (%) | OR (95% CI) a | OR (95% CI) b | |
|---|---|---|---|---|
| Short nighttime fasting (≤11 h) and late breakfast (>8:30 AM) | 56 (6.6) | 49 (8.1) | Ref | Ref |
| Short nighttime fasting (≤11 h) and early breakfast (≤8:30 AM) | 418 (49.3) | 293 (48.3) | 0.88 (0.57–1.36) | 0.89 (0.57–1.39) |
| Long nighttime fasting (>11 h) and late breakfast (>8:30 AM) | 325 (38.3) | 244 (40.2) | 0.87 (0.57–1.33) | 0.88 (0.57–1.36) |
| Long nighttime fasting (>11 h) and early breakfast (≤8:30 AM) | 49 (5.8) | 21 (3.5) | 0.58 (0.30–1.11) | 0.54 (0.27–1.04) |
| Nighttime Fasting | Controls N (%) | Cases N (%) | OR (95% CI) a | OR (95% CI) b |
|---|---|---|---|---|
| Morning chronotype | ||||
| ≤11 h | 219 (52.3) | 170 (55.5) | Ref | Ref |
| >11 h | 200 (47.7) | 136 (44.5) | 0.84 (0.61–1.15) | 0.70 (0.47–1.04) |
| Intermediate chronotype | ||||
| ≤11 h | 181 (59.7) | 130 (58.0) | Ref | Ref |
| >11 h | 122 (40.3) | 94 (42.0) | 0.97 (0.67–1.41) | 0.80 (0.50–1.27) |
| Evening chronotype | ||||
| ≤11 h | 65 (60.7) | 41 (53.9) | Ref | Ref |
| >11 h | 42 (39.3) | 35 (46.1) | 1.17 (0.63–2.18) | 0.99 (0.51–1.92) |
| Nighttime Fasting | Controls N (%) | Cases N (%) | RRR (95% CI) a | RRR (95% CI) b |
|---|---|---|---|---|
| Low aggressiveness | ||||
| ≤11 h | 474 (55.9) | 246 (56.7) | Ref | Ref |
| >11 h | 374 (44.1) | 188 (43.3) | 0.91 (0.71–1.18) | 0.78 (0.53–1.14) |
| High aggressiveness | ||||
| ≤11 h | 474 (55.9) | 86 (55.1) | Ref | Ref |
| >11 h | 374 (44.1) | 70 (44.9) | 0.92 (0.63–1.33) | 0.71 (0.42–1.19) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomar-Cros, A.; Espinosa, A.; Straif, K.; Pérez-Gómez, B.; Papantoniou, K.; Gómez-Acebo, I.; Molina-Barceló, A.; Olmedo-Requena, R.; Alguacil, J.; Fernández-Tardón, G.; et al. The Association of Nighttime Fasting Duration and Prostate Cancer Risk: Results from the Multicase-Control (MCC) Study in Spain. Nutrients 2021, 13, 2662. https://doi.org/10.3390/nu13082662
Palomar-Cros A, Espinosa A, Straif K, Pérez-Gómez B, Papantoniou K, Gómez-Acebo I, Molina-Barceló A, Olmedo-Requena R, Alguacil J, Fernández-Tardón G, et al. The Association of Nighttime Fasting Duration and Prostate Cancer Risk: Results from the Multicase-Control (MCC) Study in Spain. Nutrients. 2021; 13(8):2662. https://doi.org/10.3390/nu13082662
Chicago/Turabian StylePalomar-Cros, Anna, Ana Espinosa, Kurt Straif, Beatriz Pérez-Gómez, Kyriaki Papantoniou, Inés Gómez-Acebo, Ana Molina-Barceló, Rocío Olmedo-Requena, Juan Alguacil, Guillermo Fernández-Tardón, and et al. 2021. "The Association of Nighttime Fasting Duration and Prostate Cancer Risk: Results from the Multicase-Control (MCC) Study in Spain" Nutrients 13, no. 8: 2662. https://doi.org/10.3390/nu13082662
APA StylePalomar-Cros, A., Espinosa, A., Straif, K., Pérez-Gómez, B., Papantoniou, K., Gómez-Acebo, I., Molina-Barceló, A., Olmedo-Requena, R., Alguacil, J., Fernández-Tardón, G., Casabonne, D., Aragonés, N., Castaño-Vinyals, G., Pollán, M., Romaguera, D., & Kogevinas, M. (2021). The Association of Nighttime Fasting Duration and Prostate Cancer Risk: Results from the Multicase-Control (MCC) Study in Spain. Nutrients, 13(8), 2662. https://doi.org/10.3390/nu13082662