
The Effect of a Ketogenic Low-Carbohydrate, High-Fat Diet on Aerobic Capacity and Exercise Performance in Endurance Athletes: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
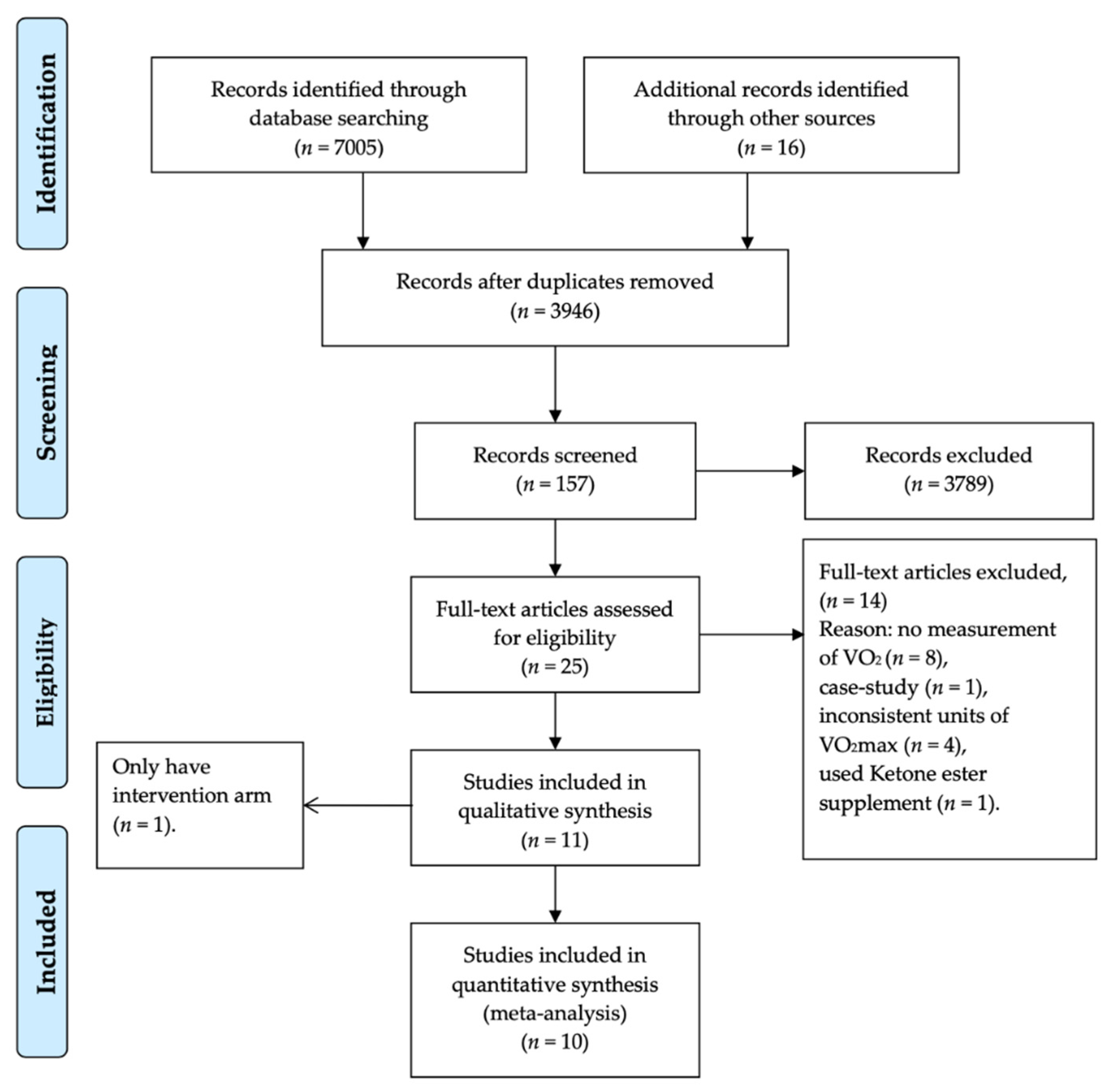
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
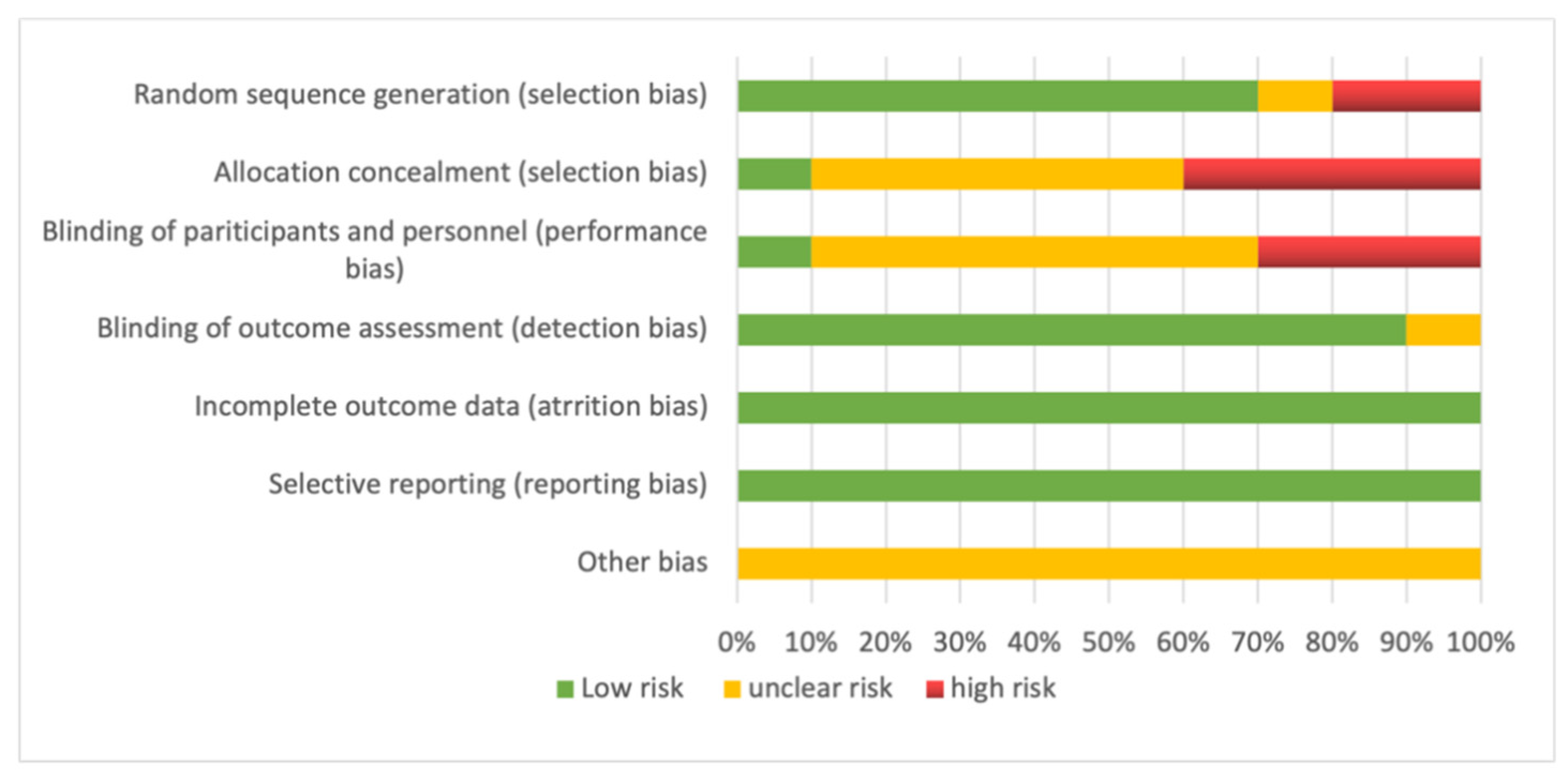
2.4. Risk of Bias and Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Synopsis of Included Studies
3.2. Characteristics of Subjects
3.3. Study Protocol
3.4. Intervention Implementation
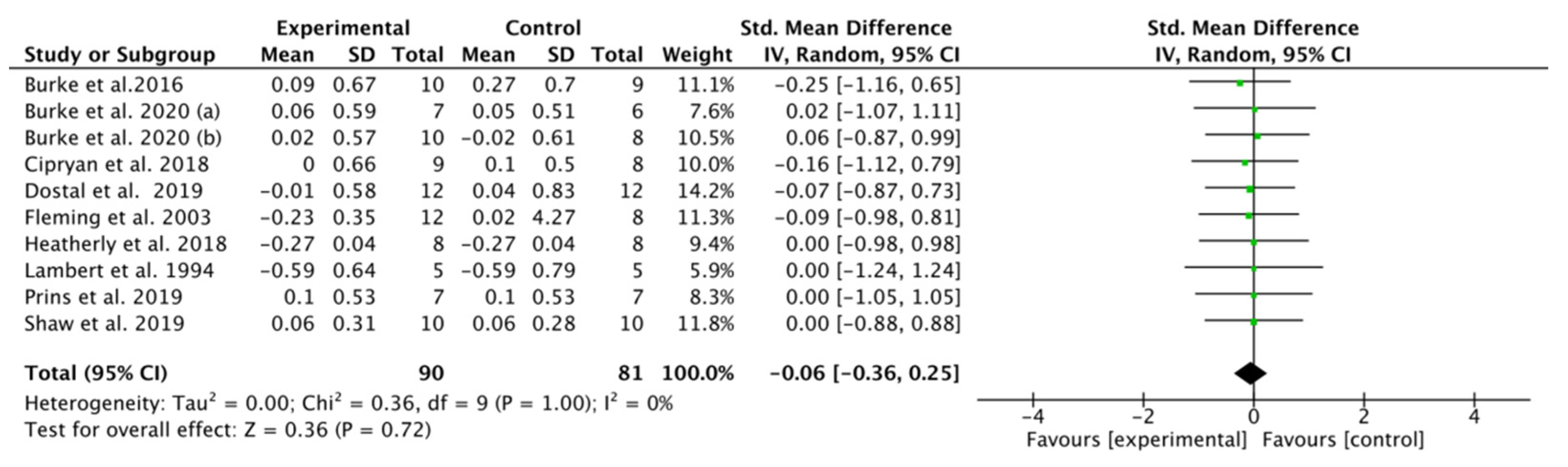
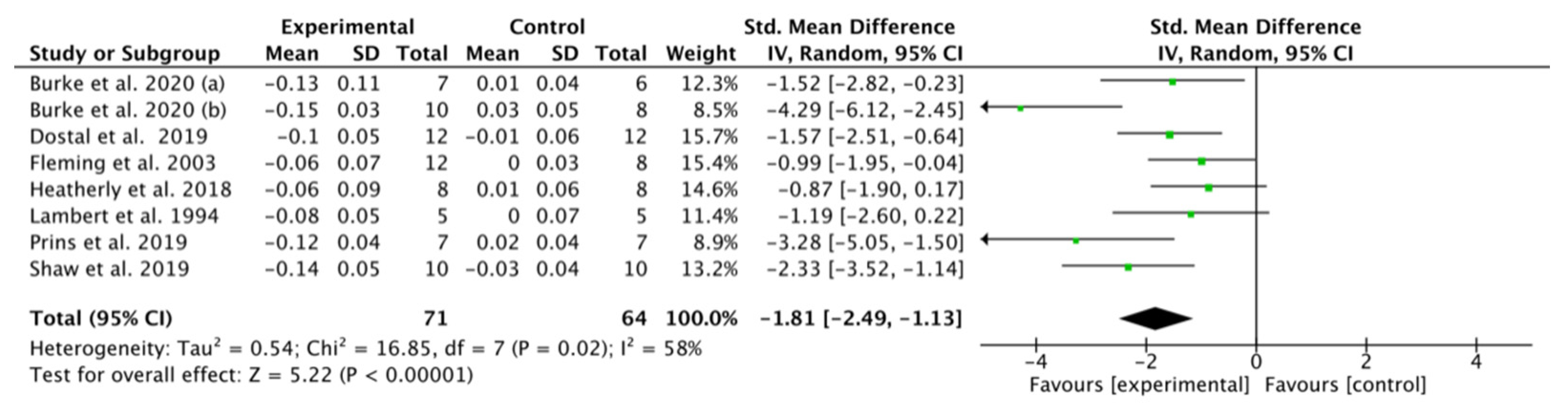
3.5. Effect of K-LCHF Diet on VO2max during a GXT
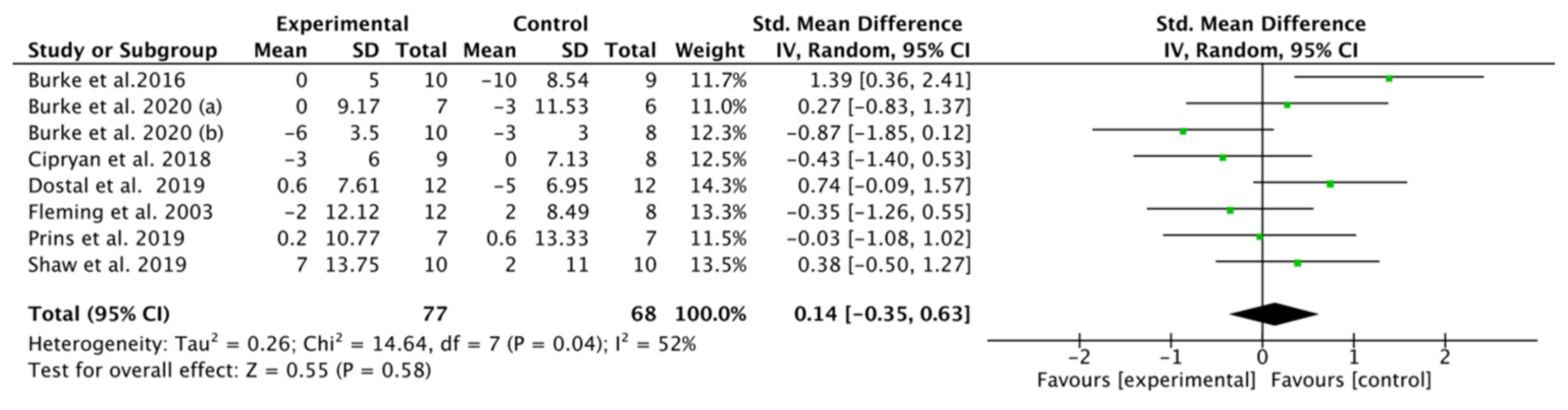
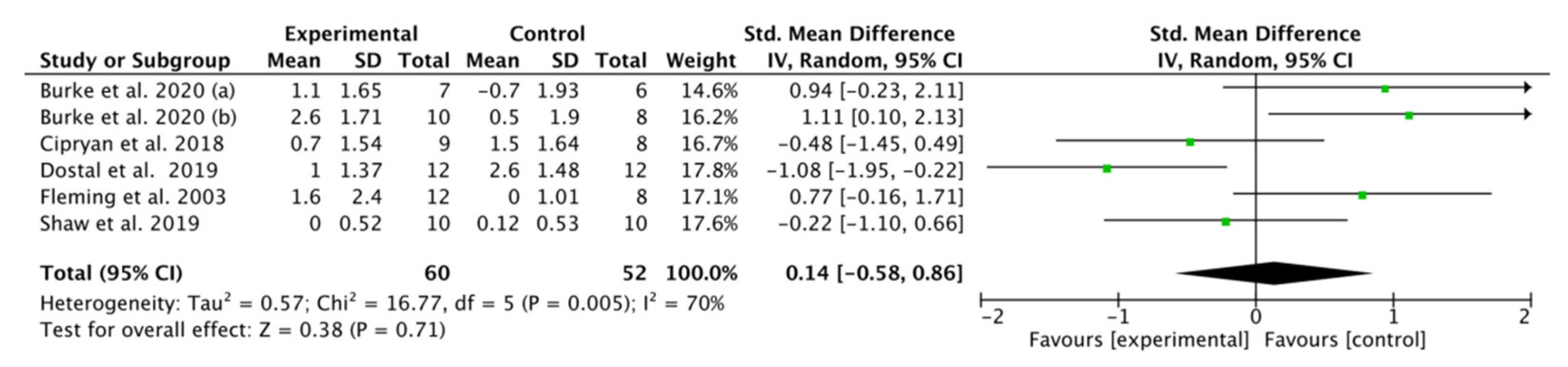
3.6. Effect of K-LCHF Diet on TTE during a GXT
3.7. Effect of K-LCHF Diet on Maximal Heart Rate (HRmax) during GXT
3.8. Effect of K-LCHF Diet on Maximal Respiratory Exchange Ratio (RER) during GXT
3.9. Effect of K-LCHF Diet on RPE during GXT
4. Discussion
4.1. Future Research
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devrim-Lanpir, A.; Hill, L.; Knechtle, B. Efficacy of Popular Diets Applied by Endurance Athletes on Sports Performance: Beneficial or Detrimental? A Narrative Review. Nutrients 2021, 13, 491. [Google Scholar] [CrossRef] [PubMed]
- Valsdottir, T.D.; Øvrebø, B.; Falck, T.M.; Litleskare, S.; Johansen, E.I.; Henriksen, C.; Jensen, J. Low-Carbohydrate High-Fat Diet and Exercise: Effect of a 10-Week Intervention on Body Composition and CVD Risk Factors in Overweight and Obese Women—A Randomized Controlled Trial. Nutrients 2020, 13, 110. [Google Scholar] [CrossRef]
- Phinney, S.; Bistrian, B.; Evans, W.; Gervino, E.; Blackburn, G. The human metabolic response to chronic ketosis without caloric restriction: Preservation of submaximal exercise capability with reduced carbohydrate oxidation. Metabolism 1983, 32, 769–776. [Google Scholar] [CrossRef]
- Burke, L.M.; Kiens, B. “Fat adaptation” for athletic performance: The nail in the coffin? J. Appl. Physiol. 2006, 100, 7–8. [Google Scholar] [CrossRef]
- Kaspar, M.B.; Austin, K.; Huecker, M.; Sarav, M. Ketogenic Diet: From the Historical Records to Use in Elite Athletes. Curr. Nutr. Rep. 2019, 8, 340–346. [Google Scholar] [CrossRef]
- Starling, R.D.; Trappe, T.A.; Parcell, A.C.; Kerr, C.G.; Fink, W.J.; Costill, D.L. Effects of diet on muscle triglyceride and endurance performance. J. Appl. Physiol. 1997, 82, 1185–1189. [Google Scholar] [CrossRef]
- Pitsiladis, Y.P.; Maughan, R.J. The effects of exercise and diet manipulation on the capacity to perform prolonged exercise in the heat and in the cold in trained humans. J. Physiol. 1999, 517, 919–930. [Google Scholar] [CrossRef]
- Volek, J.S.; Noakes, T.D.; Phinney, S. Rethinking fat as a fuel for endurance exercise. Eur. J. Sport Sci. 2015, 15, 13–20. [Google Scholar] [CrossRef]
- Evans, M.; Cogan, K.E.; Egan, B. Metabolism of ketone bodies during exercise and training: Physiological basis for exogenous supplementation. J. Physiol. 2017, 595, 2857–2871. [Google Scholar] [CrossRef] [Green Version]
- Sumithran, P.; Prendergast, L.A.; Delbridge, E.; Purcell, K.; Shulkes, A.; Kriketos, A.D.; Proietto, J. Ketosis and appetite-mediating nutrients and hormones after weight loss. Eur. J. Clin. Nutr. 2013, 67, 759–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidali, S.; Aminzadeh, S.; Lambert, B.; Rutherford, T.; Sperl, W.; Kofler, B.; Feichtinger, R.G. Mitochondria: The ketogenic diet—A metabolism-based therapy. Int. J. Biochem. Cell Biol. 2015, 63, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Puchalska, P.; Crawford, P.A. Multi-dimensional Roles of Ketone Bodies in Fuel Metabolism, Signaling, and Therapeutics. Cell Metab. 2017, 25, 262–284. [Google Scholar] [CrossRef] [Green Version]
- Grabacka, M.; Pierzchalska, M.; Reiss, K. Peroxisome proliferator activated receptor α ligands as anticancer drugs targeting mitochondrial metabolism. Curr. Pharm. Biotechnol. 2013, 14, 342–356. [Google Scholar] [CrossRef] [Green Version]
- Draznin, B.; Wang, C.; Adochio, R.; Leitner, J.W.; Cornier, M.-A. Effect of Dietary Macronutrient Composition on AMPK and SIRT1 Expression and Activity in Human Skeletal Muscle. Horm. Metab. Res. 2012, 44, 650–655. [Google Scholar] [CrossRef]
- McCarty, M.F.; DiNicolantonio, J.J.; O’Keefe, J.H. Ketosis may promote brain macroautophagy by activating Sirt1 and hypoxia-inducible factor-1. Med. Hypotheses 2015, 85, 631–639. [Google Scholar] [CrossRef]
- Xu, S.; Tao, H.; Cao, W.; Cao, L.; Lin, Y.; Zhao, S.-M.; Xu, W.; Cao, J.; Zhao, J.-Y. Ketogenic diets inhibit mitochondrial biogenesis and induce cardiac fibrosis. Signal Transduct. Target. Ther. 2021, 6, 1–13. [Google Scholar] [CrossRef]
- Burke, L.M.; Sharma, A.P.; Heikura, I.A.; Forbes, S.F.; Holloway, M.; McKay, A.K.A.; Bone, J.L.; Leckey, J.J.; Welvaert, M.; Ross, M.L. Crisis of confidence averted: Impairment of exercise economy and performance in elite race walkers by ketogenic low carbohydrate, high fat (LCHF) diet is reproducible. PLoS ONE 2020, 15, 31. [Google Scholar]
- Hawley, J.; Brouns, F.; Jeukendrup, A. Strategies to Enhance Fat Utilisation During Exercise. Sports Med. 1998, 25, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Burke, L.M. Re-Examining High-Fat Diets for Sports Performance: Did We Call the ‘Nail in the Coffin’ Too Soon? Sports Med. 2015, 45, 33–49. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.-K.; Borer, K.; Lin, P.-J. Low-Carbohydrate-High-Fat Diet: Can it Help Exercise Performance? J. Hum. Kinet. 2017, 56, 81–92. [Google Scholar] [CrossRef]
- Cermak, N.M.; van Loon, L.J. The use of carbohydrates during exercise as an ergogenic aid. Sports Med. 2013, 43, 1139–1155. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.D.; Hawley, J.; Morton, J.P. Carbohydrate availability and exercise training adaptation: Too much of a good thing? Eur. J. Sport Sci. 2015, 15, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.; Buckley, J.D.; Noakes, M.; Clifton, P.M.; Brinkworth, G.D. Long-Term Effects of a Very Low-Carbohydrate Weight Loss Diet on Exercise Capacity and Tolerance in Overweight and Obese Adults. J. Am. Coll. Nutr. 2014, 33, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Jeukendrup, A.E.; Craig, N.P.; Hawley, J. The bioenergetics of world class cycling. J. Sci. Med. Sport 2000, 3, 414–433. [Google Scholar] [CrossRef]
- Spriet, L.L. Regulation of Substrate Use During the Marathon. Sports Med. 2007, 37, 332–336. [Google Scholar] [CrossRef]
- Paoli, A.; Grimaldi, K.; D’Agostino, D.; Cenci, L.; Moro, T.; Bianco, A.; Palma, A. Ketogenic diet does not affect strength performance in elite artistic gymnasts. J. Int. Soc. Sports Nutr. 2012, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Zajac, A.; Poprzecki, S.; Maszczyk, A.; Czuba, M.; Michalczyk, M.; Zydek, G. The Effects of a Ketogenic Diet on Exercise Metabolism and Physical Performance in Off-Road Cyclists. Nutrients 2014, 6, 2493–2508. [Google Scholar] [CrossRef]
- Murphy, N.E.; Carrigan, C.T.; Margolis, L.M. High-Fat Ketogenic Diets and Physical Performance: A Systematic Review. Adv. Nutr. 2021, 12, 223–233. [Google Scholar] [CrossRef]
- Burke, L.M. Ketogenic low-CHO, high-fat diet: The future of elite endurance sport? J. Physiol. 2021, 599, 819–843. [Google Scholar] [CrossRef]
- Durkalec-Michalski, K.; Nowaczyk, P.M.; Główka, N.; Ziobrowska, A.; Podgórski, T. Is a Four-Week Ketogenic Diet an Effective Nutritional Strategy in CrossFit-Trained Female and Male Athletes? Nutrients 2021, 13, 864. [Google Scholar] [CrossRef]
- Masood, W.; Annamaraju, P.; Uppaluri, K.R. Ketogenic Diet. In StatPearls, StatPearls Publishing Copyright © 2021; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Greene, D.A.; Varley, B.J.; Hartwig, T.; Chapman, P.; Rigney, M. A Low-Carbohydrate Ketogenic Diet Reduces Body Mass Without Compromising Performance in Powerlifting and Olympic Weightlifting Athletes. J. Strength Cond. Res. 2018, 32, 3373–3382. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Carter, H. The Effect of Endurance Training on Parameters of Aerobic Fitness. Sports Med. 2000, 29, 373–386. [Google Scholar] [CrossRef]
- Bazyler, C.D.; Abbott, H.A.; Bellon, C.R.; Taber, C.B.; Stone, M.H. Strength Training for Endurance Athletes: Theory to Practice. Strength Cond. J. 2015, 37, 1–12. [Google Scholar] [CrossRef]
- Green, S.; Higgins, J.; Alderson, P. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.10 ed.; The Cochrane Collaboration: London, UK, 2008. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res. Methodol. 2014, 14, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, D. Cardiopulmonary Exercise Testing. Methods Mol. Biol. 2018, 1735, 285–295. [Google Scholar] [CrossRef]
- Gross, I.; Hirsch, H.J.; Constantini, N.; Nice, S.; Pollak, Y.; Genstil, L.; Eldar-Geva, T.; Tsur, V.G. Physical activity and maximal oxygen uptake in adults with Prader–Willi syndrome. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2017, 23, 615–620. [Google Scholar] [CrossRef]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Burke, L.M.; Whitfield, J.; Heikura, I.A.; Ross, M.L.R.; Tee, N.; Forbes, S.F.; Hall, R.; McKay, A.K.A.; Wallett, A.M.; Sharma, A.P. Adaptation to a low carbohydrate high fat diet is rapid but impairs endurance exercise metabolism and performance despite enhanced glycogen availability. J. Physiol. 2021, 599, 771–790. [Google Scholar] [CrossRef]
- Burke, L.M.; Ross, M.L.; Garvican-Lewis, L.A.; Welvaert, M.; Heikura, I.A.; Forbes, S.G.; Mirtschin, J.G.; Cato, L.E.; Strobel, N.; Sharma, A.P.; et al. Low carbohydrate, high fat diet impairs exercise economy and negates the performance benefit from intensified training in elite race walkers. J. Physiol. 2017, 595, 2785–2807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cipryan, L.; Plews, D.J.; Ferretti, A.; Maffetone, P.B.; Laursen, P.B. Effects of a 4-Week Very Low-Carbohydrate Diet on High-Intensity Interval Training Responses. J. Sports Sci. Med. 2018, 17, 259–268. [Google Scholar] [PubMed]
- Dostal, T.; Plews, D.J.; Hofmann, P.; Laursen, P.B.; Cipryan, L. Effects of a 12-Week Very-Low Carbohydrate High-Fat Diet on Maximal Aerobic Capacity, High-Intensity Intermittent Exercise, and Cardiac Autonomic Regulation: Non-randomized Parallel-Group Study. Front. Physiol. 2019, 10, 912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, J.; Sharman, M.J.; Avery, N.G.; Love, D.M.; Gómez, A.L.; Scheett, T.P.; Kraemer, W.J.; Volek, J.S. Endurance capacity and high-intensity exercise performance responses to a high fat diet. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 466–478. [Google Scholar] [CrossRef] [PubMed]
- Heatherly, A.J.; Killen, L.G.; Smith, A.F.; Waldman, H.S.; Seltmann, C.L.; Hollingsworth, A.; O’Neal, E.K. Effects of Ad libitum Low-Carbohydrate High-Fat Dieting in Middle-Age Male Runners. Med. Sci. Sports Exerc. 2018, 50, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Lambert, E.; Speechly, D.P.; Dennis, S.C.; Noakes, T.D. Enhanced endurance in trained cyclists during moderate intensity exercise following 2 weeks adaptation to a high fat diet. Graefes Arch. Clin. Exp. Ophthalmol. 1994, 69, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Prins, P.J.; Noakes, T.D.; Welton, G.L.; Haley, S.J.; Esbenshade, N.J.; Atwell, A.D.; Scott, K.E.; Abraham, J.; Raabe, A.S.; Buxton, J.D.; et al. High Rates of Fat Oxidation Induced by a Low-Carbohydrate, High-Fat Diet, Do Not Impair 5-km Running Performance in Competitive Recreational Athletes. J. Sports Sci. Med. 2019, 18, 738–750. [Google Scholar]
- Shaw, D.M.; Merien, F.; Braakhuis, A.; Maunder, E.; Dulson, D.K. Effect of a Ketogenic Diet on Submaximal Exercise Capacity and Efficiency in Runners. Med. Sci. Sports Exerc. 2019, 51, 2135–2146. [Google Scholar] [CrossRef] [PubMed]
- Lambert, E.; Goedecke, J.H.; Zyle, C.; Murphy, K.; Hawley, J.A.; Dennis, S.C.; Noakes, T.D.; Van Zyl, C. High-Fat Diet versus Habitual Diet Prior to Carbohydrate Loading: Effects on Exercise Metabolism and Cycling Performance. Int. J. Sport Nutr. Exerc. Metab. 2001, 11, 209–225. [Google Scholar] [CrossRef]
- Beelen, M.; Burke, L.M.; Gibala, M.J.; van Loon, L.J. Nutritional Strategies to Promote Postexercise Recovery. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 515–532. [Google Scholar] [CrossRef] [Green Version]
- Jentjens, R.; Jeukendrup, A.E. Determinants of Post-Exercise Glycogen Synthesis During Short-Term Recovery. Sports Med. 2003, 33, 117–144. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar]
- Romijn, J.A.; Coyle, E.F.; Sidossis, L.S.; Gastaldelli, A.; Horowitz, J.F.; Endert, E.; Wolfe, R.R. Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am. J. Physiol. Metab. 1993, 265, E380–E391. [Google Scholar] [CrossRef] [Green Version]
- Van Loon, L.J.C.; Greenhaff, P.; Constantin-Teodosiu, D.; Saris, W.H.M.; Wagenmakers, A. The effects of increasing exercise intensity on muscle fuel utilisation in humans. J. Physiol. 2001, 536, 295–304. [Google Scholar] [CrossRef]
- Helge, J.; Richter, E.A.; Kiens, B. Interaction of training and diet on metabolism and endurance during exercise in man. J. Physiol. 1996, 492, 293–306. [Google Scholar] [CrossRef]
- Soeters, M.; Soeters, P.B.; Schooneman, M.G.; Houten, S.; Romijn, J.A. Adaptive reciprocity of lipid and glucose metabolism in human short-term starvation. Am. J. Physiol. Metab. 2012, 303, E1397–E1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Havemann, L.; West, S.; Goedecke, J.; Macdonald, I.; Gibson, A.S.C.; Noakes, T.D.; Lambert, E. Fat adaptation followed by carbohydrate loading compromises high-intensity sprint performance. J. Appl. Physiol. 2006, 100, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Helge, J.W. Long-term fat diet adaptation effects on performance, training capacity, and fat utilization. Med. Sci. Sports Exerc. 2002, 34, 1499–1504. [Google Scholar] [CrossRef]
- Pellizzer, A.M.; Straznicky, N.E.; Lim, S.; Kamen, P.W.; Krum, H. Reduced dietary fat intake increases parasympathetic activity in healthy premenopausal women. Clin. Exp. Pharmacol. Physiol. 1999, 26, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Pendergast, D.R.; Leddy, J.J.; Venkatraman, J.T. A perspective on fat intake in athletes. J. Am. Coll. Nutr. 2000, 19, 345–350. [Google Scholar] [CrossRef]
- Havemann, L. The effect of Fat-Adaptation Followed by Carbohydrate-Loading on Simulated Ultra-Endurance Race Performance. Ph.D. Thesis, University of Cape Town, Cape Town, South Africa, 2008. [Google Scholar]
- Durkalec-Michalski, K.; Nowaczyk, P.M.; Siedzik, K. Effect of a four-week ketogenic diet on exercise metabolism in CrossFit-trained athletes. J. Int. Soc. Sports Nutr. 2019, 16, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahill, G.F. Alternate fuel utilization by brain. In Cerebral Metabolism and Neural Function; Passonneau, J.V., Hawkins, R.A., Lust, W.D., Welsh, F.A., Eds.; Williams & Wilkins: Baltimore, MD, USA, 1980. [Google Scholar]
- Owen, O.E.; Morgan, A.P.; Kemp, H.G.; Sullivan, J.M.; Herrera, M.G.; Cahill, G.F. Brain Metabolism during Fasting*. J. Clin. Investig. 1967, 46, 1589–1595. [Google Scholar] [CrossRef]
- Wentz, A.; D’Avignon, D.A.; Weber, M.L.; Cotter, D.G.; Doherty, J.M.; Kerns, R.; Nagarajan, R.; Reddy, N.; Sambandam, N.; Crawford, P.A. Adaptation of Myocardial Substrate Metabolism to a Ketogenic Nutrient Environment. J. Biol. Chem. 2010, 285, 24447–24456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, O.E. Ketone bodies as a fuel for the brain during starvation. Biochem. Mol. Biol. Educ. 2005, 33, 246–251. [Google Scholar] [CrossRef]
- Han, Y.-M.; Ramprasath, T.; Zou, M.-H. β-hydroxybutyrate and its metabolic effects on age-associated pathology. Exp. Mol. Med. 2020, 52, 548–555. [Google Scholar] [CrossRef] [Green Version]
- Achanta, L.B.; Rae, C.D. β-Hydroxybutyrate in the Brain: One Molecule, Multiple Mechanisms. Neurochem. Res. 2017, 42, 35–49. [Google Scholar] [CrossRef]
- Newman, J.C.; Verdin, E. β-Hydroxybutyrate: A Signaling Metabolite. Annu. Rev. Nutr. 2017, 37, 51–76. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citation, Year | Subjects | Age (Years) | Body Mass Change | Study Design | Dietary Components | Energy Intake | Intervention Duration | VO2max Test Type | Other Exercise Test | Exercise Session during the Intervention |
|---|---|---|---|---|---|---|---|---|---|---|
| Burke et al. 2017 [42] | 19 highly competitive male race walkers K-LCHF: n = 10 HC: n = 9 | K-LCHF: 28.3 ± 3.5 HC: 25.4 ± 4.0 | K-LCHF: significantly reduction HC: no significant change | Control study | K-LCHF: 3.5% CHO 17% protein 78% fat HC: 60% CHO 16% protein 20% fat | K-LCHF: 3560 kcal/d HC: 3519 kcal/d | 3 weeks | Graded economy test: Treadmill | 10-km race; 20-km race | Race walking, resistance training and cross-training (running, cycling or swimming) |
| Burke et al. 2020 (a) [41] | 13 male race walkers K-LCHF: n = 6 HC: n = 7 | K-LCHF: 28.3 ± 2.7 HC: 32.7 ± 4.8 | K-LCHF: significant reduction HC: no significant change | Parallel control study | K-LCHF: 4% CHO 16% protein 80% fat HC: 65% CHO 15% protein 20% fat | K-LCHF: 3766 ± 477 kcal/d HC: 3957 ± 726 kcal/d | 5 days | Incremental testing: Treadmill | 10-km race 25-km race | 25–40 km walk, interval training session (8–12 × 1 km on a 6-min cycle), tempo hill session (14 km with ~450 m elevation gain). Low-intensity walking sessions (6–12 km each), and a strength training session |
| Burke et al. 2020 (b) [18] | 18 highly competitive race walkers K-LCHF (M: 8; F: 2) HC (M: 5; F: 3) | K-LCHF: 29.9 ± 2.1 HC: 25.5 ± 3.6 | K-LCHF: significant reduction HC: no significant change | Parallel control study | K-LCHF: 4% CHO 16% protein 78% fat HC: 65% CHO 15% protein 18% fat | K-LCHF: 3679 ± 382 kcal/d HC: 3345 ± 529 kcal/d | 25 days | Graded exercise test (GXT): Treadmill | 10-km race; 20-km race | Race walking, resistance training and cross-training (e.g., running, cycling or swimming) |
| Cipryan et al. 2018 [43] | 17 moderately trained males K-LCHF: n = 9 HD: n = 8 | K-LCHF: 23.8 ± 2.4 HD: 23.8 ± 1.8 | K-LCHF: significant reduction HD: no significant change | Control study | K-LCHF: 8% CHO 29% protein 63% fat HD: 48% CHO 17% protein 35% fat | No report | 4 weeks | Graded exercise test (GXT): Treadmill | No report | HIIT: 10-min warmup at 60% VO2max, followed by 5 high-intensity exercises consisting of 3 min at 100% VO2max (work to rest ratio, 2:1) Endurance-based running sessions or exercise (3–5 times a week) |
| Dostal et al. 2019 [44] | 24 recreational trained runners K-LCHF: n = 12 HD: n = 12 | K-LCHF: 25.3 ± 2.0 HD: 23.9 ± 3.8 | K-LCHF: significant reduction HD: no significant change | Parallel control study | K-LCHF:8% CHO 23% protein 69% fat HD: 45% CHO 18% protein 37% fat | K-LCHF: 1960 ± 316 kcal/d HC: 1782 ± 412 kcal/d | 12 weeks | Graded exercise test (GXT): Treadmill | No report | HIIT (sessions lasted approximately 40 min in total and consisted of a 4-min warmup followed by 5 × 6-min sets, separated by 2-min recovery), endurance exercise (e.g., running, cycling, sport games) |
| Fleming et al. 2003 [45] | 20 non-highly trained men K-LCHF: n = 12 HC: n = 8 | K-LCHF: 35 ± 13 HC: 36 ± 12 | No report | Control study | K-LCHF: 8% CHO 30% protein 61% fat HC: 59% CHO 15% protein 25% fat | K-LCHF: 2235 ± 375 kcal/d HC: 1815 ± 195 kcal/d | 6 weeks | Graded exercise test: Cycle ergometer | Wingate Sprint, Time ride | Walking, running, cycling and cross-training |
| Heatherly et al. 2018 [46] | 8 trained runners | 39.5 ± 9.9 | K-LCHF: significant reduction HC: no significant change | Crossover study | K-LCHF: 7 ± 4% CHO 29 ± 9% protein 64 ± 9% fat HC: 43 ± 11% CHO 17 ± 8% protein 38 ± 7% fat | K-LCHF: 1886 ± 520 kcal/d HC: 2820 ± 955 kcal/d | 3 weeks | Graded exercise test: Treadmill | 50-min run in heat, 5-km time trial | No report |
| Lambert et al. 1994 [47] | 5 endurance trained male cyclists | 22.0 ± 1.80 | No report | Crossover study | K-LCHF: 7% CHO 23% protein 70% fat HC: 74% CHO 14% protein 12% fat | No report | 2 weeks | Progressive exercise test: Cycle ergometer | 30-s Wingate test | No report |
| Prins et al. 2019 [48] | 7 competitive recreational distance male runners | 35.6 ± 8.4 | No report | Randomized counterbalance crossover study | K-LCHF: 6.0 ± 1.3% CHO 25.1 ±1.5% protein 69 ± 2% fat HC: 56.4 ± 2.6% CHO 15.3 ±1.1% protein 28 ± 2% fat | K-LCHF: 2837 ± 251 kcal/d HC: 2947 ± 284 kcal/d | 6 weeks | Graded exercise test: Treadmill | 5-km time trial | Maintain usual training |
| Shaw et al. 2019 [49] | 8 trained male endurance athletes | 29.6 ± 5.1 | K-LCHF: significant reduction HD: no significant change | Randomized crossover study | K-LCHF: 4.1 ± 0.8% CHO 18.2 ± 3.5% protein 78 ± 4% fat HD: 42.9 ± 7.8% CHO 18.6 ± 1.4% protein 39 ± 7% fat | K-LCHF: 3122 kcal/d HD: 3280 kcal/d | 31 days | Graded metabolic test: Treadmill | Run to exhaustion trial | Running and cycling |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, J.; Lei, S.; Wang, X.; Cheng, S. The Effect of a Ketogenic Low-Carbohydrate, High-Fat Diet on Aerobic Capacity and Exercise Performance in Endurance Athletes: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2896. https://doi.org/10.3390/nu13082896
Cao J, Lei S, Wang X, Cheng S. The Effect of a Ketogenic Low-Carbohydrate, High-Fat Diet on Aerobic Capacity and Exercise Performance in Endurance Athletes: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(8):2896. https://doi.org/10.3390/nu13082896
Chicago/Turabian StyleCao, Jingguo, Siman Lei, Xiuqiang Wang, and Sulin Cheng. 2021. "The Effect of a Ketogenic Low-Carbohydrate, High-Fat Diet on Aerobic Capacity and Exercise Performance in Endurance Athletes: A Systematic Review and Meta-Analysis" Nutrients 13, no. 8: 2896. https://doi.org/10.3390/nu13082896
APA StyleCao, J., Lei, S., Wang, X., & Cheng, S. (2021). The Effect of a Ketogenic Low-Carbohydrate, High-Fat Diet on Aerobic Capacity and Exercise Performance in Endurance Athletes: A Systematic Review and Meta-Analysis. Nutrients, 13(8), 2896. https://doi.org/10.3390/nu13082896