
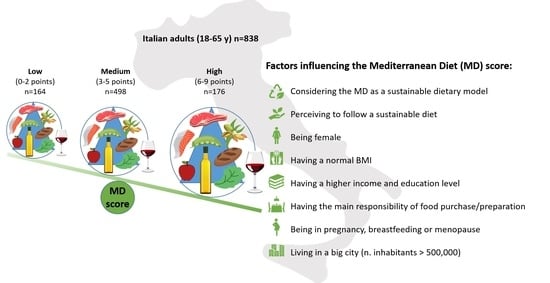
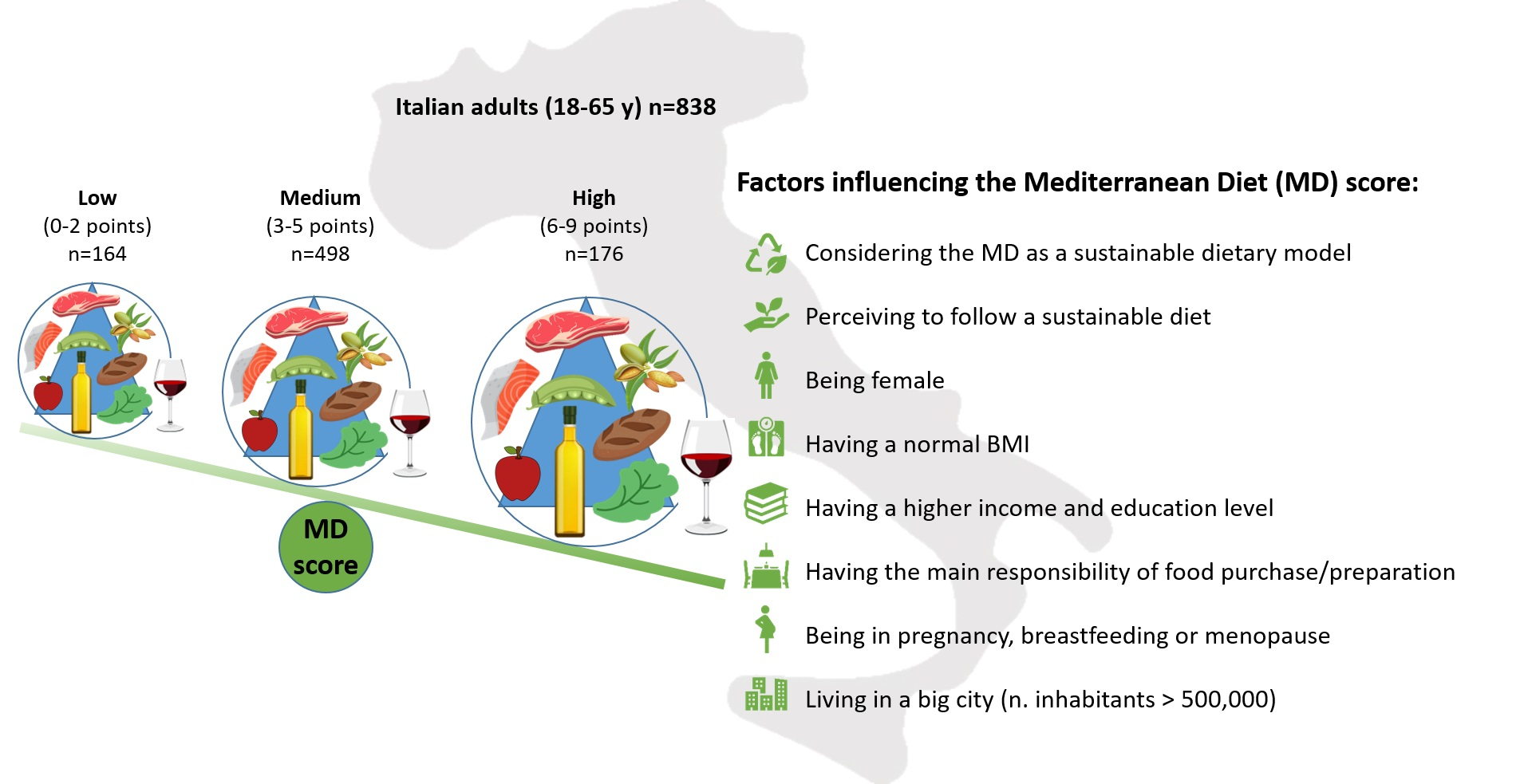
Adherence to the Mediterranean Diet in Association with Self-Perception of Diet Sustainability, Anthropometric and Sociodemographic Factors: A Cross-Sectional Study in Italian Adults


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Participants’ Characteristics and Adherence to the MD
3.2. Compliance with Food Recommendations
3.3. Associations between Adherence to the MD and Anthropometric, Sociodemographic, and Sustainability Perception of Diet Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galbete, C.; Schwingshackl, L.; Schwedhelm, C.; Boeing, H.; Schulze, M.B. Evaluating Mediterranean diet and risk of chronic disease in cohort studies: An umbrella review of meta-analyses. Eur. J. Epidemiol. 2018, 33, 909–931. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Pagliai, G.; Angelino, D.; Rosi, A.; Dall’Asta, M.; Bresciani, L.; Ferraris, C.; Guglielmetti, M.; Godos, J.; Del Bo’, C.; et al. Effects of Popular Diets on Anthropometric and Cardiometabolic Parameters: An Umbrella Review of Meta-Analyses of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 815–833. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2017, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Georgoulis, M.; Kontogianni, M.D.; Yiannakouris, N. Mediterranean Diet and Diabetes: Prevention and Treatment. Nutrients 2014, 6, 1406–1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becerra-Tomás, N.; Mejía, S.B.; Viguiliouk, E.; Khan, T.; Kendall, C.W.; Kahleova, H.; Rahelić, D.; Sievenpiper, J.L.; Salas-Salvadó, J. Mediterranean diet, cardiovascular disease and mortality in diabetes: A systematic review and meta-analysis of prospective cohort studies and randomized clinical trials. Crit. Rev. Food Sci. Nutr. 2019, 60, 1207–1227. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Zappalà, G.; Bernardini, S.; Giambini, I.; Bes-Rastrollo, M.; Martinez-Gonzalez, M.A. Adherence to the Mediterranean diet is inversely associated with metabolic syndrome occurrence: A meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2016, 68, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef]
- Godos, J.; Ferri, R.; Caraci, F.; Cosentino, F.I.I.; Castellano, S.; Galvano, F.; Grosso, G. Adherence to the Mediterranean Diet is Associated with Better Sleep Quality in Italian Adults. Nutrients 2019, 11, 976. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- HLPE. Nutrition and Food Systems. A Report by the High Level Panel Experts on Food Security Nutrition; Committee on World Food Security: Rome, Italy, 2017; p. 152. [Google Scholar]
- FAO; OIE; WHO; UN System Influenza Coordination; UNICEF; World Bank. Contributing to One World, One Health: A Strategic Framework for Reducing Risks of Infectious Diseases at the Animal-Human-Ecosystems Interface, Consultation Document; Food and Agriculture Organization; World Health Organization; UN System Influenza Coordinator United Nations Children Fund; World Bank: Sharm-el-Sheikh, Egypt, 2008.
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Dernini, S.; Berry, E.M. Mediterranean Diet: From a Healthy Diet to a Sustainable Dietary Pattern. Front. Nutr. 2015, 2, 15. [Google Scholar] [CrossRef] [Green Version]
- Burlingame, B.; Dernini, S. Sustainable diets: The Mediterranean diet as an example. Public Health Nutr. 2011, 14, 2285–2287. [Google Scholar] [CrossRef] [Green Version]
- Dernini, S.; Berry, E.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.X.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0: The Mediterranean diet with four sustainable benefits. Public Health Nutr. 2016, 20, 1322–1330. [Google Scholar] [CrossRef]
- Tilman, D.; Clark, M. Global diets link environmental sustainability and human health. Nature 2014, 515, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Blas, A.; Garrido, A.; Unver, O.; Willaarts, B.A. A comparison of the Mediterranean diet and current food consumption patterns in Spain from a nutritional and water perspective. Sci. Total. Environ. 2019, 664, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- UNESCO. Representative List of the Intangible Cultural Heritage of Humanity. Paris. 2010. Available online: http://www.unesco.org/culture/ich/RL/00884 (accessed on 30 June 2021).
- Ruiz, A.H.; García-Villanova, B.; Hernández, E.J.G.; Amiano, P.; Azpiri, M.; Montes, E.M. Description of indexes based on the adherence to the Mediterranean dietary pattern: A review. Nutr. Hosp. 2015, 32, 1872–1884. [Google Scholar]
- Bach, A.; Serra-Majem, L.; Carrasco, J.L.; Roman, B.; Ngo, J.; Bertomeu, I.; Obrador, B. The use of indexes evaluating the adherence to the Mediterranean diet in epidemiological studies: A review. Public Health Nutr. 2006, 9, 132–146. [Google Scholar] [CrossRef]
- Rosi, A.; Paolella, G.; Biasini, B.; Scazzina, F.; Alicante, P.; De Blasio, F.; Russo, M.D.; Rendina, D.; Tabacchi, G.; Cairella, G.; et al. Dietary habits of adolescents living in North America, Europe or Oceania: A review on fruit, vegetable and legume consumption, sodium intake, and adherence to the Mediterranean Diet. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 544–560. [Google Scholar] [CrossRef] [PubMed]
- Germani, A.; Vitiello, V.; Giusti, A.M.; Pinto, A.; Donini, L.M.; Del Balzo, V. Environmental and economic sustainability of the Mediterranean Diet. Int. J. Food Sci. Nutr. 2014, 65, 1008–1012. [Google Scholar] [CrossRef]
- Belahsen, R. Nutrition transition and food sustainability. Proc. Nutr. Soc. 2014, 73, 385–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benton, T.; Bieg, C.; Harwatt, H.; Pudasaini, R.; Wellesley, L. Food System Impacts on Biodiversity Loss: Three Levers for Food System Transformation in Support of Nature; Royal Institute of International Affairs: London, UK, 2021. [Google Scholar]
- Biasini, B. Understanding, Assessing and Modelling Sustainable Eating Behaviours. Ph.D. Thesis, University of Parma, Parma, Italy, 2020. [Google Scholar]
- WHO. Cut-Off for BMI According to WHO Standards 2010. Available online: https://gateway.euro.who.int/en/indicators/mn_survey_19-cut-off-for-bmi-according-to-who-standards/ (accessed on 30 June 2021).
- Graziano, P.R.; Forno, F. Political Consumerism and New Forms of Political Participation. Ann. Am. Acad. Politi.-Soc. Sci. 2012, 644, 121–133. [Google Scholar] [CrossRef]
- Vittersø, G.; Torjusen, H.; Laitala, K.; Tocco, B.; Biasini, B.; Csillag, P.; De Labarre, M.D.; Lecoeur, J.-L.; Maj, A.; Majewski, E.; et al. Short Food Supply Chains and Their Contributions to Sustainability: Participants’ Views and Perceptions from 12 European Cases. Sustainability 2019, 11, 4800. [Google Scholar] [CrossRef] [Green Version]
- Gnagnarella, P.; Dragà, D.; Misotti, A.; Sieri, S.; Spaggiari, L.; Cassano, E.; Baldini, F.; Soldati, L.; Maisonneuve, P. Validation of a short questionnaire to record adherence to the Mediterranean diet: An Italian experience. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- CREA. Guidelines for Healthy Italian Nutrition. 2019. Available online: https://www.crea.gov.it/web/alimenti-e-nutrizione/-/linee-guida-per-una-sana-alimentazione-2018 (accessed on 30 June 2021).
- Burlingame, B.; Dernini, S. Sustainable Diets and Biodiversity: Directions and Solutions for Policy, Research and Action. In Proceedings of the International Scientific Symposium, Biodiversity and Sustainable Diets United Against Hunger, Rome, Italy, 3–5 November 2010; Food and Agriculture Organization of the United Nations (FAO): Rome, Italy, 2012. [Google Scholar]
- Riddell, L.J.; Ang, B.; Keast, R.S.; Hunter, W. Impact of living arrangements and nationality on food habits and nutrient intakes in young adults. Appetite 2011, 56, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Psychology Press: New York, NY, USA, 2010. [Google Scholar]
- García-González, Á.; Achón, M.; Krug, A.C.; Varela-Moreiras, G.; Alonso-Aperte, E. Food Sustainability Knowledge and Attitudes in the Spanish Adult Population: A Cross-Sectional Study. Nutrients 2020, 12, 3154. [Google Scholar] [CrossRef]
- Vermeir, I.; Weijters, B.; De Houwer, J.; Geuens, M.; Slabbinck, H.; Spruyt, A.; Verbeke, W. Environmentally sustainable food consumption: A review and research agenda from a goal-directed perspective. Front. Psychol. 2020, 11, 1603. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Giangrandi, I.; Colombini, B.; Toniolo, L.; Gensini, G.; Sofi, F. Adherence to the Mediterranean diet among Italian adults: Results from the web-based Medi-Lite questionnaire. Int. J. Food Sci. Nutr. 2020, 72, 271–279. [Google Scholar] [CrossRef]
- Caparello, G.; Galluccio, A.; Giordano, C.; Lofaro, D.; Barone, I.; Morelli, C.; Sisci, D.; Catalano, S.; Andò, S.; Bonofiglio, D. Adherence to the Mediterranean diet pattern among university staff: A cross-sectional web-based epidemiological study in Southern Italy. Int. J. Food Sci. Nutr. 2019, 71, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.; Bach-Faig, A.; Quintana, B.R.; Buckland, G.; De Almeida, M.D.V.; Serra-Majem, L. Worldwide variation of adherence to the Mediterranean diet, in 1961–1965 and 2000–2003. Public Health Nutr. 2009, 12, 1676–1684. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Notarnicola, M.; Cisternino, A.M.; Inguaggiato, R.; Guerra, V.; Reddavide, R.; Donghia, R.; Rotolo, O.; Zinzi, I.; Leandro, G.; et al. Trends in adherence to the Mediterranean diet in South Italy: A cross sectional study. Nutr. Metab. Cardiovasc. Dis. 2019, 30, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Galeone, C.; Negri, E.; La Vecchia, C. Trends in adherence to the Mediterranean diet in an Italian population between 1991 and 2006. Eur. J. Clin. Nutr. 2010, 64, 1052–1056. [Google Scholar] [CrossRef] [Green Version]
- Cavaliere, A.; Banterle, A.; De Marchi, E. Exploring the Adherence to the Mediterranean Diet and Its Relationship with Individual Lifestyle: The Role of Healthy Behaviors, Pro-Environmental Behaviors, Income, and Education. Nutrients 2018, 10, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; De Lucia, F.; Persichillo, M.; Zito, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Decline of the Mediterranean diet at a time of economic crisis. Results from the Moli-sani study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, S. What are the determinants of adherence to the mediterranean diet? Int. J. Food Sci. Nutr. 2021, 72, 143–144. [Google Scholar] [CrossRef]
- Van Bussel, L.M.; Van Rossum, C.T.; Temme, E.H.; Boon, P.E.; Ocké, M.C. Educational differences in healthy, environmentally sustainable and safe food consumption among adults in the Netherlands. Public Health Nutr. 2020, 23, 2057–2067. [Google Scholar] [CrossRef] [PubMed]
- WHO. Promoting Fruit and Vegetable Consumption around the World; Global Strategy on Diet, Physical Activity and Health; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Luchetti, F. Importance and future of olive oil in the world market—An introduction to olive oil. Eur. J. Lipid Sci. Technol. 2002, 104, 559–563. [Google Scholar] [CrossRef]
- Abrahamse, W. How to Effectively Encourage Sustainable Food Choices: A Mini-Review of Available Evidence. Front. Psychol. 2020, 11, 589674. [Google Scholar] [CrossRef] [PubMed]
- Sogari, G.; Li, J.; Lefebvre, M.; Menozzi, D.; Pellegrini, N.; Cirelli, M.; Gómez, M.I.; Mora, C. The Influence of Health Messages in Nudging Consumption of Whole Grain Pasta. Nutrients 2019, 11, 2993. [Google Scholar] [CrossRef] [Green Version]
- Castellari, E.; Marette, S.; Moro, D.; Sckokai, P. Can menu labeling affect away-from-home-dietary choices? Bio-Based Appl. Econ. 2018, 7, 249–263. [Google Scholar]
- Afshin, A.; Penalvo, J.L.; Del Gobbo, L.; Silva, J.; Michaelson, M.; O’Flaherty, M.; Capewell, S.; Spiegelman, D.; Danaei, G.; Mozaffarian, D. The prospective impact of food pricing on improving dietary consumption: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0172277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fresco, L.O.; Geerling-Eiff, F.; Hoes, A.-C.; van Wassenaer, L.; Poppe, K.J.; Vorst, J.G.A.J.V.D. Sustainable food systems: Do agricultural economists have a role? Eur. Rev. Agric. Econ. 2021, 48, 694–718. [Google Scholar] [CrossRef]
- Santini, F.; Ronzon, T.; Perez Dominguez, I.; Araujo Enciso, S.R.; Proietti, I. What if meat consumption would decrease more than expected in the high-income countries? Bio-Based Appl. Econ. J. 2017, 6, 37–56. [Google Scholar]

{kind=link}
| All (n = 838) | Female (n = 434) | Male (n = 404) | p Value | |
|---|---|---|---|---|
| Age range (years) | 0.131 a | |||
| 18–24 | 89 (10.6) | 53 (12.2) | 36 (8.9) | |
| 25–34 | 157 (18.7) | 79 (18.2) | 78 (19.3) | |
| 35–44 | 198 (23.6) | 111 (25.6) | 87 (21.5) | |
| 45–54 | 209 (24.9) | 95 (21.9) | 114 (28.2) | |
| 55–65 | 185 (22.1) | 96 (22.1) | 89 (22.0) | |
| BMI (kg/m2) | <0.001 a | |||
| <18.5 (underweight) | 36 (4.3) | 33 (7.6) | 3 (0.7) | |
| 18.5–24.9 (normal weight) | 497 (59.3) | 284 (65.4) | 213 (52.7) | |
| 25.0–29.9 (overweight) | 230 (27.4) | 82 (18.9) | 148 (36.6) | |
| ≥30.0–34.9 (obesity) | 75 (8.9) | 26 (6.0) | 31 (7.7) | |
| Health conditions | <0.001 a | |||
| Anemia, hypertension, or dyslipidemia | 83 (9.9) | 36 (8.3) | 47 (11.6) | |
| Food intolerance or allergies | 138 (16.5) | 70 (16.1) | 68 (16.8) | |
| Menopause, pregnancy, or breastfeeding | 70 (8.4) | 70 (16.1) | - | |
| None of the above | 547 (65.3) | 258 (59.4) | 289 (71.5) | |
| Geographical area of residence | 0.683 a | |||
| Northwest | 220 (26.3) | 116 (26.7) | 104 (25.7) | |
| Northeast | 168 (20.0) | 86 (19.8) | 82 (20.3) | |
| Central | 167 (19.9) | 85 (19.6) | 82 (20.3) | |
| South | 192 (22.9) | 94 (21.7) | 98 (24.3) | |
| Islands | 91 (10.9) | 53 (12.2) | 38 (9.4) | |
| Size of residence (number of inhabitants) | 0.300 a | |||
| <5000 | 148 (17.7) | 80 (18.4) | 68 (16.8) | |
| 5000–49,999 | 348 (41.5) | 188 (43.3) | 160 (39.6) | |
| 50,000–500,000 | 206 (24.6) | 95 (21.9) | 111 (27.5) | |
| >500,000 | 136 (16.2) | 71 (16.4) | 65 (16.1) | |
| Education level | 0.151 a | |||
| Primary or lower secondary | 62 (7.4) | 26 (6.0) | 36 (8.9) | |
| Secondary | 448 (53.5) | 243 (56.0) | 205 (50.7) | |
| Tertiary * | 328 (39.1) | 165 (38.0) | 163 (40.3) | |
| Occupation | <0.001 a | |||
| Full-time employee | 441 (52.6) | 167 (38.5) | 274 (67.8) | |
| Part-time employee | 133 (15.9) | 93 (21.4) | 40 (9.9) | |
| Unemployed | 158 (18.9) | 113 (26.0) | 45 (11.1) | |
| Retired | 35 (4.2) | 16 (3.7) | 19 (4.7) | |
| Student | 71 (8.5) | 45 (10.4) | 26 (6.4) | |
| Monthly household net income | 0.005 a | |||
| ≤EUR 1499 | 193 (23.0) | 115 (26.5) | 78 (19.3) | |
| EUR 1500–2499 | 267 (31.9) | 132 (30.4) | 135 (33.4) | |
| ≥EUR 2500 | 294 (35.1) | 131 (30.2) | 163 (40.3) | |
| Do not wish to tell or do not know | 84 (10.0) | 56 (12.9) | 28 (6.9) | |
| N. household members | 0.084 a | |||
| 1 | 76 (9.1) | 33 (7.6) | 43 (10.6) | |
| 2 | 182 (21.7) | 106 (24.4) | 76 (18.8) | |
| 3 | 267 (31.9) | 129 (29.7) | 138 (34.2) | |
| >3 | 313 (37.4) | 166 (38.2) | 147 (36.4) | |
| N. household members < 18 years | 0.263 a | |||
| None | 526 (62.8) | 284 (65.4) | 242 (59.9) | |
| 1 | 172 (20.5) | 80 (18.4) | 92 (22.8) | |
| 2 | 118 (14.1) | 57 (13.1) | 61 (15.1) | |
| ≥3 | 22 (2.6) | 13 (3.0) | 9 (2.2) | |
| Responsibility of food purchases | <0.001 a | |||
| Mainly responsible | 601 (71.7) | 347 (80.0) | 254 (62.9) | |
| Co-responsible | 222 (26.5) | 84 (19.4) | 138 (34.2) | |
| Little or not at all responsible | 15 (1.8) | 3 (0.7) | 12 (3.0) | |
| Responsibility in meal preparation | <0.001 a | |||
| Mainly responsible | 529 (63.1) | 346 (79.7) | 183 (45.3) | |
| Co-responsible | 262 (31.3) | 78 (18.0) | 184 (45.5) | |
| Little or not at all responsible | 47 (5.6) | 10 (2.3) | 37 (9.2) | |
| Frequency of eating out | <0.001 a | |||
| Never or seldom | 129 (15.4) | 83 (19.1) | 46 (11.4) | |
| <1 time/week | 167 (19.9) | 101 (23.3) | 66 (16.3) | |
| 1 time/week | 195 (23.3) | 101 (23.3) | 94 (23.3) | |
| 2–4 times/week | 249 (29.7) | 117 (27.0) | 132 (23.7) | |
| ≥5 times/week | 98 (11.7) | 32 (7.4) | 66 (16.3) | |
| Taking part in SPGs or EAs | 0.634 a | |||
| Yes | 93 (11.1) | 46 (10.6) | 47 (11.6) | |
| No | 745 (88.9) | 388 (89.4) | 357 (88.4) | |
| MD score (on a 0–9 scale) | 4.0 (3.0–5.0) | 4.0 (3.0–6.0) | 3.0 (2.0–5.0) | <0.001 b |
| Adherence to the Mediterranean Diet | <0.001 a | |||
| Low | 164 (19.6) | 52 (12.0) | 112 (27.7) | |
| Medium | 498 (59.4) | 261 (60.1) | 237 (58.7) | |
| High | 176 (21.0) | 121 (27.9) | 55 (13.6) | |
| MD considered a sustainable dietary model | 0.375 a | |||
| No | 10 (1.2) | 3 (0.7) | 7 (1.7) | |
| Maybe | 410 (48.9) | 212 (48.8) | 198 (49.0) | |
| Yes | 418 (49.9) | 219 (50.5) | 199 (49.3) | |
| Self-perceived adoption of a sustainable diet within the last 3 months | 0.317 a | |||
| No | 175 (20.9) | 85 (19.6) | 90 (22.3) | |
| Not much | 526 (62.8) | 283 (65.2) | 243 (60.1) | |
| Yes | 137 (16.3) | 66 (15.2) | 71 (17.6) |
| Ref. Intake | Adherence to the MD | ||||
|---|---|---|---|---|---|
| Low (n = 164) | Medium (n = 498) | High (n = 176) | p Value | ||
| Wholegrains | MD (≥1/d) | 87 (53.0) | 417 (83.7) | 158 (89.8) | <0.001 |
| IT (n.a.) | n.a. | n.a. | n.a. | ||
| Vegetables | MD (≥2/d) | 3 (1.8) | 121 (24.3) | 137 (77.8) | <0.001 |
| IT (≥2/d) | 3 (1.8) | 121 (24.3) | 137 (77.8) | <0.001 | |
| Fruit | MD (≥2/d) | 8 (4.9) | 188 (37.8) | 150 (85.2) | <0.001 |
| IT (≥3/d) | – | 33 (6.6) | 41 (23.3) | <0.001 | |
| Milk and yogurt | MD (n.a.) | n.a. | n.a. | n.a. | |
| IT (≥3/d) | 1 (0.6) | 8 (1.6) | 8 (4.5) | 0.021 | |
| Olive oil | MD (≥3/d) | 1 (0.6) | 46 (9.2) | 64 (36.4) | <0.001 |
| IT (3–4/d) | 1 (0.6) | 41 (8.2) | 54 (30.7) | <0.001 | |
| Butter, margarine, or cooking cream | MD (n.a.) | n.a. | n.a. | n.a. | |
| IT (<3/d) | 163 (99.4) | 488 (98.0) | 170 (96.6) | 0.187 | |
| Wine | MD (1–2/d, M; >0 < 1/d, F) | 44 (26.8) | 291 (58.4) | 134 (76.1) | <0.001 |
| IT (never or hardly never) | 81 (49.4) | 236 (47.4) | 88 (50.0) | 0.800 | |
| Red meat or meat products | MD (≤3/w) | 125 (76.2) | 461 (92.6) | 173 (98.3) | <0.001 |
| IT (≤1/w) | 53 (32.3) | 183 (36.7) | 94 (53.4) | <0.001 | |
| White meat | MD (n.a.) | n.a. | n.a. | n.a. | |
| IT (1–3/w) | 84 (51.2) | 296 (59.4) | 97 (55.1) | 0.158 | |
| Carbonated or SSB | MD | n.a. | n.a. | n.a. | |
| IT (<1/w) | 108 (65.9) | 346 (69.5) | 142 (80.7) | 0.005 | |
| Sweets | MD | n.a. | n.a. | n.a. | |
| IT (<1/w) | 103 (62.8) | 295 (59.2) | 112 (63.6) | 0.501 | |
| Fish or seafood | MD (≥2/w) | 4 (2.4) | 155 (31.1) | 115 (65.3) | <0.001 |
| IT (2–3/w) | 3 (1.8) | 146 (29.3) | 104 (59.1) | <0.001 | |
| Nuts | MD (≥2/w) | 3 (1.8) | 123 (24.7) | 117 (66.5) | <0.001 |
| IT (2–3/w) | 2 (1.2) | 89 (17.9) | 70 (39.8) | <0.001 | |
| Pulses | MD (≥2/w) | 7 (4.3) | 120 (24.1) | 111 (63.1) | <0.001 |
| IT (2–3/w) | 7 (4.3) | 112 (22.5) | 96 (54.5) | <0.001 | |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Gender | ||||
| Females | -1- | -1- | ||
| Males | 0.408 (0.286–0.580) | <0.001 | 0.366 (0.220–0.609) | <0.001 |
| Age (years) | ||||
| 18–24 | -1- | -1- | ||
| 25–34 | 0.948 (0.479–1.873) | 0.877 | 0.459 (0.164–1.287) | 0.139 |
| 35–44 | 1.342 (0.711–2.532) | 0.364 | 0.704 (0.251–1.979) | 0.506 |
| 45–54 | 1.182 (0.625–2.234) | 0.607 | 0.764 (0.275–2.123) | 0.606 |
| 55–65 | 1.467 (0.776–2.772) | 0.239 | 0.667 (0.222–2.002) | 0.470 |
| BMI (kg/m2) | ||||
| <18.5 | -1- | -1- | ||
| 18.5–24.9 | 0.623 (0.302–1.283) | 0.199 | 0.693 (0.265–1.811) | 0.454 |
| 25.0–29.9 | 0.383 (0.176–0.834) | 0.016 | 0.632 (0.225–1.774) | 0.383 |
| ≥30.0 | 0.273 (0.102–0.728) | 0.010 | 0.647 (0.187–2.235) | 0.491 |
| Health conditions | ||||
| Anemia, hypertension, or dyslipidemia | 1.180 (0.663–2.100) | 0.573 | 1.062 (0.503–2.242) | 0.875 |
| Food intolerance or allergies | 1.498 (0.960–2.336) | 0.075 | 1.558 (0.909–2.669) | 0.106 |
| Menopause, pregnancy, or breastfeeding | 2.877 (1.696–4.880) | <0.001 | 1.924 (0.916–4.042) | 0.084 |
| None of the above | -1- | -1- | ||
| Geographical area of residence | ||||
| Northwest | -1- | -1- | ||
| Northeast | 0.986 (0.608–1.599) | 0.953 | 1.008 (0.537–1.893) | 0.980 |
| Central | 0.925 (0.567–1.510) | 0.756 | 0.840 (0.457–1.544) | 0.574 |
| South | 0.918 (0.573–1.471) | 0.723 | 1.109 (0.605–2.033) | 0.738 |
| Islands | 0.689 (0.364–1.304) | 0.252 | 0.635 (0.280–1.438) | 0.276 |
| Size of residence (number of inhabitants) | ||||
| <5000 | -1- | -1- | ||
| 5000–49,999 | 1.160 (0.705–1.911) | 0.559 | 0.880 (0.471–1.643) | 0.687 |
| 50,000–500,000 | 1.166 (0.677–2.009) | 0.580 | 0.876 (0.439–1.749) | 0.707 |
| >500,000 | 1.955 (1.115–3.428) | 0.019 | 1.622 (0.791–3.324) | 0.187 |
| Educational level | ||||
| Primary or lower secondary | -1- | -1- | ||
| Secondary | 2.946 (1.148–7.560) | 0.025 | 3.098 (1.020–9.410) | 0.046 |
| Tertiary * or higher | 3.617 (1.401–9.339) | 0.008 | 3.072 (0.973–9.700) | 0.056 |
| Occupation | ||||
| Full-time employee | -1- | -1- | ||
| Part-time employee | 1.186 (0.753–1.867) | 0.461 | 1.372 (0.737–2.551) | 0.318 |
| Unemployed | 0.741 (0.462–1.187) | 0.213 | 1.041 (0.514–2.107) | 0.912 |
| Retired | 1.437 (0.667–3.097) | 0.354 | 1.961 (0.706–5.451) | 0.196 |
| Student | 0.589 (0.291–1.193) | 0.142 | 0.599 (0.181–1.982) | 0.401 |
| Monthly household net income | ||||
| ≤EUR 1499 | -1- | -1- | ||
| EUR 1500–2499 | 1.705 (1.026–2.832) | 0.039 | 1.950 (1.051–3.620) | 0.034 |
| ≥EUR 2500 | 2.160 (1.324–3.527) | 0.002 | 2.419 (1.225–4.777) | 0.011 |
| Number of household members | ||||
| 1 | -1- | -1- | ||
| 2 | 1.195 (0.594–2.405) | 0.618 | 0.890 (0.364–2.178) | 0.798 |
| 3 | 1.623 (0.841–3.135) | 0.149 | 1.880 (0.748–4.725) | 0.180 |
| >3 | 1.149 (0.594–2.224) | 0.679 | 0.722 (0.261–1.995) | 0.529 |
| Number of household members <18 years | ||||
| None | -1- | -1- | ||
| 1 | 1.179 (0.774–1.794) | 0.443 | 0.576 (0.312–1.065) | 0.079 |
| 2 | 1.417 (0.888–2.261) | 0.144 | 1.789 (0.793–4.033) | 0.161 |
| ≥3 | 1.559 (0.595–4.083) | 0.366 | 1.970 (0.549–7.060) | 0.298 |
| Responsibility of food purchases # | ||||
| Main responsible | -1- | -1- | ||
| Co-, little, or not at all responsible | 0.495 (0.326–0.752) | 0.001 | 0.905 (0.446–1.836) | 0.781 |
| Responsibility in food preparation | ||||
| Main responsible | -1- | -1- | ||
| Co-responsible | 0.516 (0.348–0.763) | 0.001 | 0.875 (0.453–1.690) | 0.690 |
| Little or not at all responsible | 0.201 (0.061–0.658) | 0.008 | 0.748 (0.170–3.287) | 0.700 |
| Frequency of eating out | ||||
| Never or seldom | -1- | -1- | ||
| <1 time/week | 1.648 (0.897–3.029) | 0.108 | 1.730 (0.815–3.674) | 0.154 |
| 1 time/week | 1.737 (0.963–3.133) | 0.067 | 1.906 (0.903–4.022) | 0.091 |
| 2–4 times/week | 1.641 (0.927–2.907) | 0.089 | 1.405 (0.649–3.039) | 0.388 |
| ≥5 times/week | 1.484 (0.743–2.965) | 0.263 | 1.317 (0.534–3.252) | 0.550 |
| Taking part in SPGs or EAs | ||||
| Yes | -1- | -1- | ||
| No | 0.650 (0.399–1.057) | 0.083 | 1.038 (0.557–1.936) | 0.906 |
| MD considered a sustainable dietary model # | ||||
| No/maybe | -1- | -1- | ||
| Yes | 2.617 (1.840–3.723) | <0.001 | 2.293 (1.487–3.534) | <0.001 |
| Self-perceived adoption of a sustainable diet | ||||
| No | -1- | -1- | ||
| Not much | 3.388 (1.815–6.323) | <0.001 | 2.162 (1.089–4.293) | 0.028 |
| Yes | 10.275 (5.222–20.216) | <0.001 | 7.667 (3.517–16.711) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biasini, B.; Rosi, A.; Menozzi, D.; Scazzina, F. Adherence to the Mediterranean Diet in Association with Self-Perception of Diet Sustainability, Anthropometric and Sociodemographic Factors: A Cross-Sectional Study in Italian Adults. Nutrients 2021, 13, 3282. https://doi.org/10.3390/nu13093282
Biasini B, Rosi A, Menozzi D, Scazzina F. Adherence to the Mediterranean Diet in Association with Self-Perception of Diet Sustainability, Anthropometric and Sociodemographic Factors: A Cross-Sectional Study in Italian Adults. Nutrients. 2021; 13(9):3282. https://doi.org/10.3390/nu13093282
Chicago/Turabian StyleBiasini, Beatrice, Alice Rosi, Davide Menozzi, and Francesca Scazzina. 2021. "Adherence to the Mediterranean Diet in Association with Self-Perception of Diet Sustainability, Anthropometric and Sociodemographic Factors: A Cross-Sectional Study in Italian Adults" Nutrients 13, no. 9: 3282. https://doi.org/10.3390/nu13093282
APA StyleBiasini, B., Rosi, A., Menozzi, D., & Scazzina, F. (2021). Adherence to the Mediterranean Diet in Association with Self-Perception of Diet Sustainability, Anthropometric and Sociodemographic Factors: A Cross-Sectional Study in Italian Adults. Nutrients, 13(9), 3282. https://doi.org/10.3390/nu13093282