
Serum Folate Related to Five Measurements of Obesity and High-Sensitivity C-Reactive Protein in Korean Adults


Abstract
:1. Introduction
2. Materials and Methods
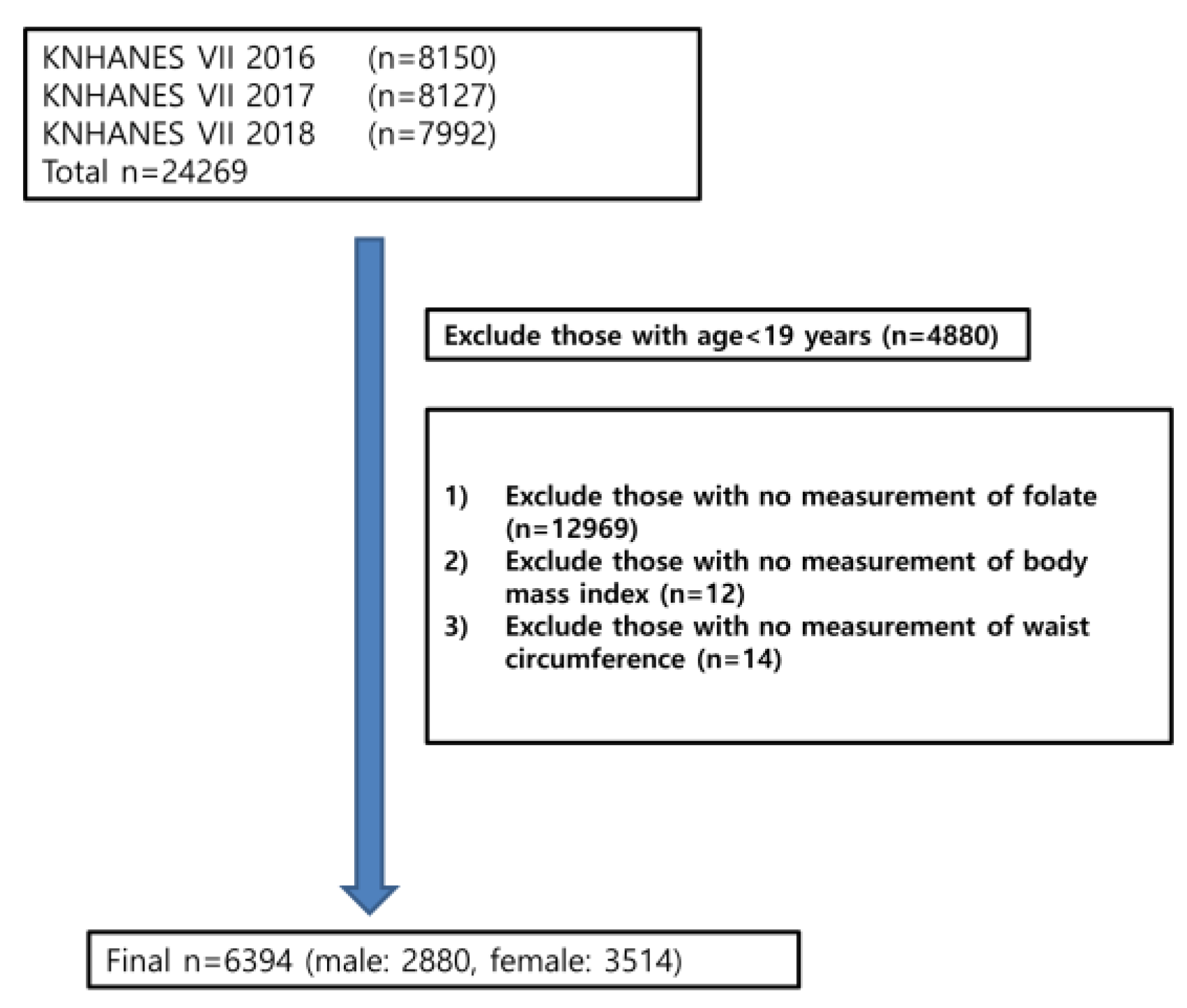
2.1. Study Design and Study Population
2.2. Measurement of Folic Acid and High-Sensitivity C-Reactive Protein
2.3. Obesity Assessment
2.4. Covariates
2.5. Statistical Analysis
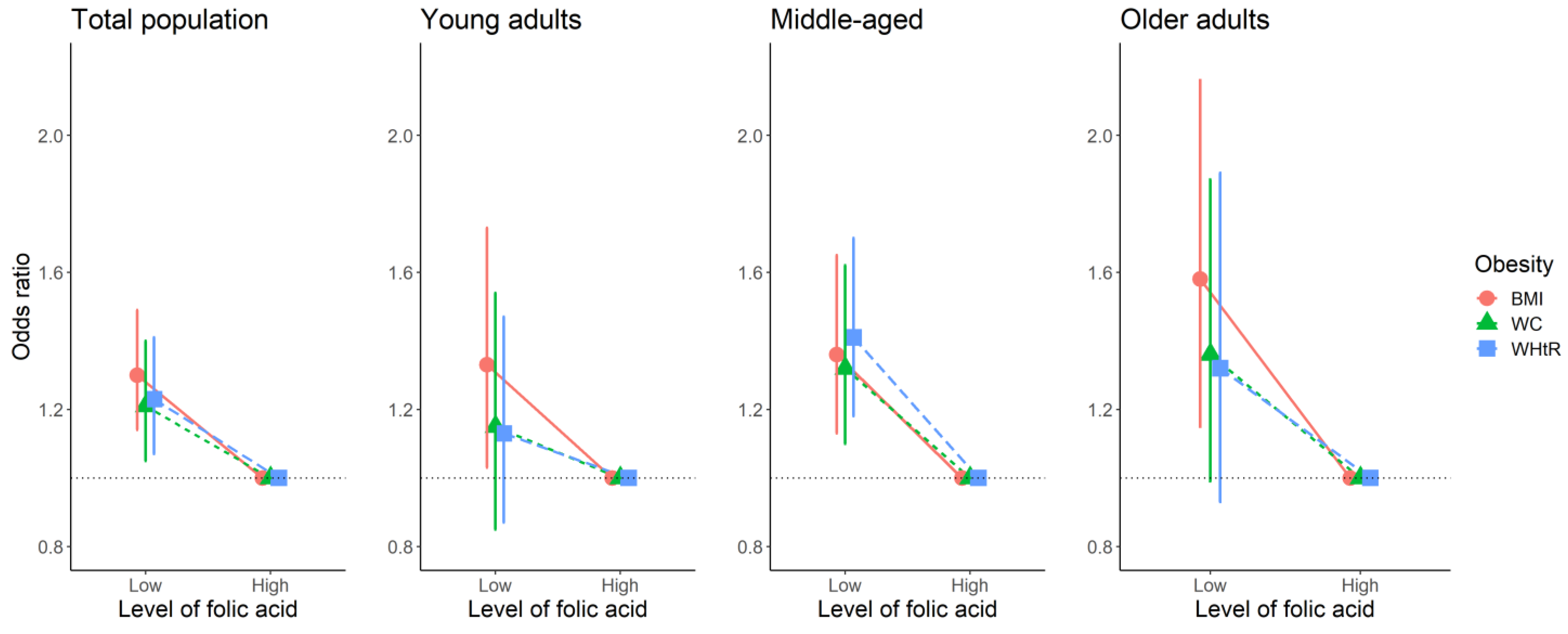
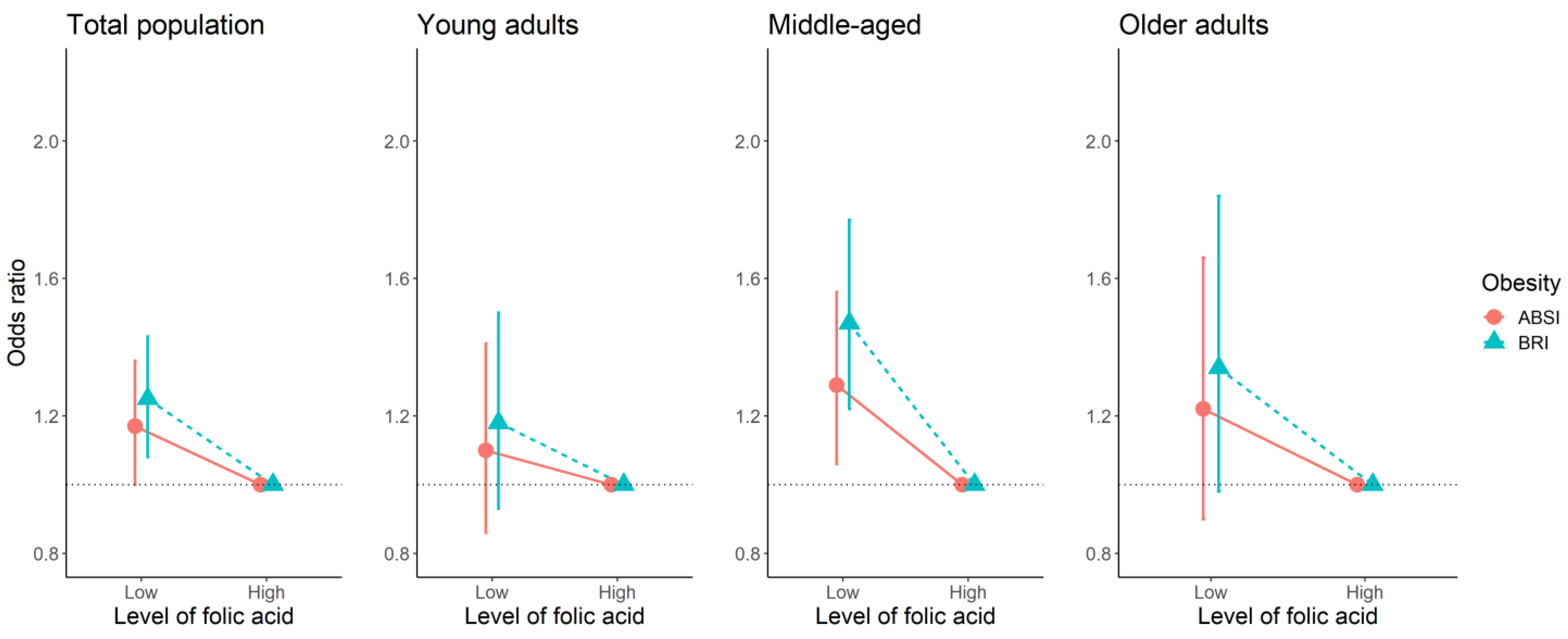
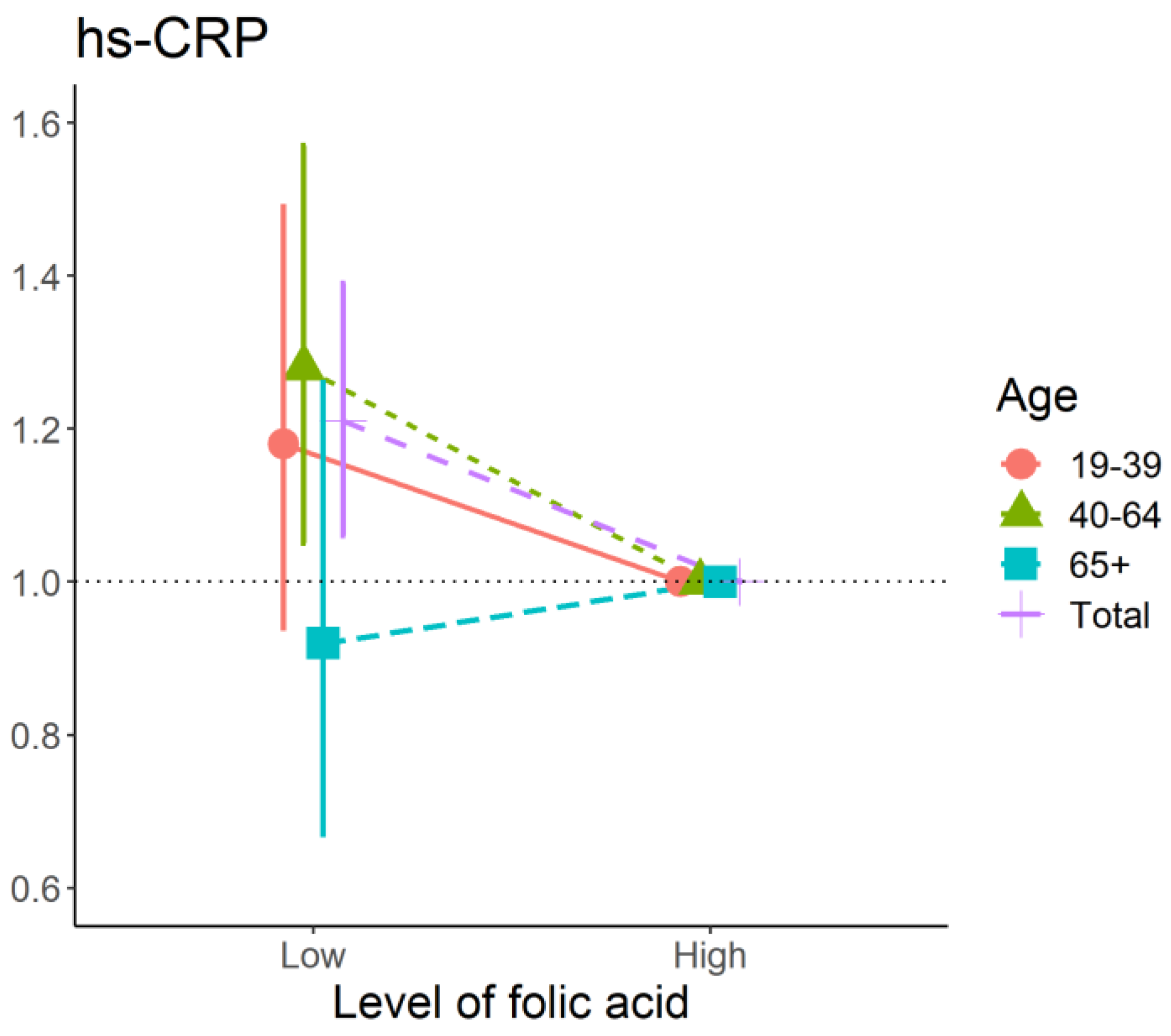
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight#:~:text=Worldwide%20obesity%20has%20nearly%20tripled,%2C%20and%2013%25%20were%20obese (accessed on 12 August 2022).
- Ye, J. Mechanisms of insulin resistance in obesity. Front. Med. 2013, 7, 14–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yatsuya, H.; Li, Y.; Hilawe, E.H.; Ota, A.; Wang, C.; Chiang, C.; Zhang, Y.; Uemura, M.; Osako, A.; Ozaki, Y.; et al. Global trend in overweight and obesity and its association with cardiovascular disease incidence. Circ. J. 2014, 78, 2807–2818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horn, J.W.; Feng, T.; Mørkedal, B.; Strand, L.B.; Horn, J.; Mukamal, K.; Janszky, I. Obesity and Risk for First Ischemic Stroke Depends on Metabolic Syndrome: The HUNT Study. Stroke 2021, 52, 3555–3561. [Google Scholar] [CrossRef]
- Wolin, K.Y.; Carson, K.; Colditz, G.A. Obesity and cancer. Oncologist 2010, 15, 556–565. [Google Scholar] [CrossRef]
- Johnston, B.C.; Kanters, S.; Bandayrel, K.; Wu, P.; Naji, F.; Siemieniuk, R.A.; Ball, G.D.; Busse, J.W.; Thorlund, K.; Guyatt, G.; et al. Comparison of weight loss among named diet programs in overweight and obese adults: A meta-analysis. JAMA 2014, 312, 923–933. [Google Scholar] [CrossRef]
- Sun, Y.; Sun, M.; Liu, B.; Du, Y.; Rong, S.; Xu, G.; Snetselaar, L.G.; Bao, W. Inverse Association between Serum Vitamin B12 Concentration and Obesity among Adults in the United States. Front. Endocrinol. 2019, 10, 414. [Google Scholar] [CrossRef] [Green Version]
- Lotfi-Dizaji, L.; Mahboob, S.; Aliashrafi, S.; Vaghef-Mehrabany, E.; Ebrahimi-Mameghani, M.; Morovati, A. Effect of vitamin D supplementation along with weight loss diet on meta-inflammation and fat mass in obese subjects with vitamin D deficiency: A double-blind placebo-controlled randomized clinical trial. Clin. Endocrinol. 2019, 90, 94–101. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.M.; Jialal, I. Folic Acid Deficiency. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Haggarty, P. UK introduces folic acid fortification of flour to prevent neural tube defects. Lancet 2021, 398, 1199–1201. [Google Scholar] [CrossRef]
- Mlodzik-Czyzewska, M.A.; Malinowska, A.M.; Chmurzynska, A. Low folate intake and serum levels are associated with higher body mass index and abdominal fat accumulation: A case control study. Nutr. J. 2020, 19, 53. [Google Scholar] [CrossRef]
- Koo, Y.S.; Lee, Y.J.; Park, J.M. Inverse Association of Serum Folate Level with Metabolic Syndrome and Its Components in Korean Premenopausal Women: Findings of the 2016–2018 Korean National Health Nutrition Examination Survey. Nutrients 2022, 14, 880. [Google Scholar] [CrossRef]
- Wiebe, N.; Field, C.J.; Tonelli, M. A systematic review of the vitamin B12, folate and homocysteine triad across body mass index. Obes. Rev. 2018, 19, 1608–1618. [Google Scholar] [CrossRef] [PubMed]
- Navarrete-Muñoz, E.-M.; Vioque, J.; Toledo, E.; Oncina-Canovas, A.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Romaguera, D.; Alonso-Gómez, Á.M.; et al. Dietary folate intake and metabolic syndrome in participants of PREDIMED-Plus study: A cross-sectional study. Eur. J. Nutr. 2021, 60, 1125–1136. [Google Scholar] [CrossRef] [PubMed]
- Donfrancesco, C.; Profumo, E.; Lo Noce, C.; Minutoli, D.; Di Lonardo, A.; Buttari, B.; Vespasiano, F.; Vannucchi, S.; Galletti, F.; Onder, G.; et al. Trends of overweight, obesity and anthropometric measurements among the adult population in Italy: The CUORE Project health examination surveys 1998, 2008, and 2018. PLoS ONE 2022, 17, e0264778. [Google Scholar] [CrossRef] [PubMed]
- Mohammadian Khonsari, N.; Khashayar, P.; Shahrestanaki, E.; Kelishadi, R.; Mohammadpoor Nami, S.; Heidari-Beni, M.; Esmaeili Abdar, Z.; Tabatabaei-Malazy, O.; Qorbani, M. Normal Weight Obesity and Cardiometabolic Risk Factors: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2022, 13, 857930. [Google Scholar] [CrossRef]
- Nevill, A.M.; Duncan, M.J.; Myers, T. BMI is dead; long live waist-circumference indices: But which index should we choose to predict cardio-metabolic risk? Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1642–1650. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar]
- Thomas, D.M.; Bredlau, C.; Bosy-Westphal, A.; Mueller, M.; Shen, W.; Gallagher, D.; Maeda, Y.; McDougall, A.; Peterson, C.M.; Ravussin, E.; et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity 2013, 21, 2264–2271. [Google Scholar] [CrossRef] [Green Version]
- Schlecht, I.; Fischer, B.; Behrens, G.; Leitzmann, M.F. Relations of Visceral and Abdominal Subcutaneous Adipose Tissue, Body Mass Index, and Waist Circumference to Serum Concentrations of Parameters of Chronic Inflammation. Obes. Facts 2016, 9, 144–157. [Google Scholar] [CrossRef]
- Mahwati, Y.; Nurrika, D. Obesity Indicators and C-Reactive Protein in Indonesian Adults (More than Equal to 40 Years Old): The Indonesian Family Life Survey 5. J. Kesehat. Masy. Nas. 2020, 15, 169–174. [Google Scholar] [CrossRef]
- Biswas, D.C.; Rahman, M.; Sharmin, F.; Jahan, I.; Roy, A.; Begum, S. Association of high-sensitivity C-reactive protein level with central obesity of the children in a tertiary care hospital of Bangladesh. Issues Dev. Health Res. 2021, 8, 17–25. [Google Scholar]
- Rasheed, A.; Acharya, S.; Shukla, S.; Kumar, S.; Yarappa, R.; Gupte, Y.; Hulkoti, V. High-Sensitivity C-Reactive Protein in Metabolic Healthy Obesity (MHO). J. Evol. Med. Dent. Sci. 2020, 9, 443–447. [Google Scholar] [CrossRef]
- Santa-Paavola, R.; Lehtinen-Jacks, S.; Jääskeläinen, T.; Männistö, S.; Lundqvist, A. The association of high-sensitivity C-reactive protein with future weight gain in adults. Int. J. Obes. 2022, 46, 1234–1240. [Google Scholar] [CrossRef]
- Pfeiffer, C.M.; Sternberg, M.R.; Zhang, M.; Fazili, Z.; Storandt, R.J.; Crider, K.S.; Yamini, S.; Gahche, J.J.; Juan, W.; Wang, C.-Y.; et al. Folate status in the US population 20 y after the introduction of folic acid fortification. Am. J. Clin. Nutr. 2019, 110, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.A.; Bressan, J.; Oliveira, F.L.P.; Sant’Ana, H.M.P.; Pimenta, A.M.; Lopes, L.L.; Hermsdorff, H.H.M. Dietary Folate Intake Is Negatively Associated with Excess Body Weight in Brazilian Graduates and Postgraduates (CUME Project). Nutrients 2019, 11, 518. [Google Scholar] [CrossRef] [Green Version]
- Zargarzadeh, N.; Severo, J.S.; Pizarro, A.B.; Persad, E.; Mousavi, S.M. The Effects of Folic Acid Supplementation on Pro-inflammatory Mediators: A Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Clin. Ther. 2021, 43, e346–e363. [Google Scholar] [CrossRef]
- Asbaghi, O.; Ashtary-Larky, D.; Bagheri, R.; Moosavian, S.P.; Nazarian, B.; Afrisham, R.; Kelishadi, M.R.; Wong, A.; Dutheil, F.; Suzuki, K.; et al. Effects of Folic Acid Supplementation on Inflammatory Markers: A Grade-Assessed Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 2327. [Google Scholar] [CrossRef]
- Moltrer, M.; Pala, L.; Cosentino, C.; Mannucci, E.; Rotella, C.M.; Cresci, B. Body mass index (BMI), waist circumference (WC), waist-to-height ratio (WHtR) e waist body mass index (wBMI): Which is better? Endocrine 2022, 76, 578–583. [Google Scholar] [CrossRef]
- Christakoudi, S.; Tsilidis, K.K.; Evangelou, E.; Riboli, E. A Body Shape Index (ABSI), hip index, and risk of cancer in the UK Biobank cohort. Cancer Med. 2021, 10, 5614–5628. [Google Scholar] [CrossRef]
- Christakoudi, S.; Tsilidis, K.K.; Muller, D.C.; Freisling, H.; Weiderpass, E.; Overvad, K.; Söderberg, S.; Häggström, C.; Pischon, T.; Dahm, C.C.; et al. A Body Shape Index (ABSI) achieves better mortality risk stratification than alternative indices of abdominal obesity: Results from a large European cohort. Sci. Rep. 2020, 10, 14541. [Google Scholar] [CrossRef]
- Zhang, S.; Fu, X.; Du, Z.; Guo, X.; Li, Z.; Sun, G.; Zhou, Y.; Yang, H.; Yu, S.; Zheng, L.; et al. Is waist-to-height ratio the best predictive indicator of cardiovascular disease incidence in hypertensive adults? A cohort study. BMC Cardiovasc. Disord. 2022, 22, 214. [Google Scholar] [CrossRef] [PubMed]
- Mehran, L.; Amouzegar, A.; Fanaei, S.M.; Masoumi, S.; Azizi, F. Anthropometric measures and risk of all-cause and cardiovascular mortality: An 18 years follow-up. Obes. Res. Clin. Pract. 2022, 16, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.N. Elderly Obesity: Is It Harmful or Beneficial? J. Obes. Metab. Syndr. 2018, 27, 84–92. [Google Scholar] [CrossRef]
- Li, J.; Goh, C.E.; Demmer, R.T.; Whitcomb, B.W.; Du, P.; Liu, Z. Association between Serum Folate and Insulin Resistance among U.S. Nondiabetic Adults. Sci. Rep. 2017, 7, 9187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klee, G.G. Cobalamin and folate evaluation: Measurement of methylmalonic acid and homocysteine vs. vitamin B(12) and folate. Clin. Chem. 2000, 46, 1277–1283. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Cheng, Y.; Zhong, X.; Zhang, B.; Bao, Z.; Zhang, Y.; Wang, Z. Nuclear factor erythroid 2-related factor 2 activation mediates hyperhomocysteinemia-associated lipolysis suppression in adipocytes. Exp. Biol. Med. 2018, 243, 926–933. [Google Scholar] [CrossRef]
- Chan, C.-W.; Chan, P.-H.; Lin, B.-F. Folate Deficiency Increased Lipid Accumulation and Leptin Production of Adipocytes. Front. Nutr. 2022, 9, 852451. [Google Scholar] [CrossRef]
- Marseglia, L.; Manti, S.; D’Angelo, G.; Nicotera, A.; Parisi, E.; Di Rosa, G.; Gitto, E.; Arrigo, T. Oxidative stress in obesity: A critical component in human diseases. Int. J. Mol. Sci. 2014, 16, 378–400. [Google Scholar] [CrossRef] [Green Version]
- Cagnacci, A.; Cannoletta, M.; Xholli, A.; Piacenti, I.; Palma, F.; Palmieri, B. Folate administration decreases oxidative status and blood pressure in postmenopausal women. Eur. J. Nutr. 2015, 54, 429–435. [Google Scholar] [CrossRef]
- Folic Acid Recommendations. Available online: https://www.cdc.gov/ncbddd/folicacid/recommendations.html#:~:text=All%20women%20of%20reproductive%20age,and%20spine%20(spina%20bifida) (accessed on 12 August 2022).
- Folate Fact Sheet for Health Professionals. Available online: https://ods.od.nih.gov/factsheets/Folate-HealthProfessional/#en18] (accessed on 12 August 2022).
- Adams, J.B.; Kirby, J.K.; Sorensen, J.C.; Pollard, E.L.; Audhya, T. Evidence based recommendations for an optimal prenatal supplement for women in the US: Vitamins and related nutrients. Matern. Health Neonatol. Perinatol. 2022, 8, 4. [Google Scholar] [CrossRef]
- Xu, R.; Shen, P.; Wu, C.; Wan, Y.; Fan, Z.; Gao, X. BMI, high-sensitivity C-reactive protein and the conversion from metabolically healthy to unhealthy phenotype in Chinese adults: A cohort study. Public Health Nutr. 2021, 24, 4124–4131. [Google Scholar] [CrossRef] [PubMed]
- Köse, S.; Sözlü, S.; Bölükbaşi, H.; Ünsal, N.; Gezmen-Karadağ, M. Obesity is associated with folate metabolism. Int. J. Vitam. Nutr. Res. 2020, 90, 353–364. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total | 19–39 | 40–64 | 65+ | p Value |
|---|---|---|---|---|---|
| n | 6394 | 2013 | 3086 | 1295 | |
| Age, y | 49.3 ± 16.3 | 30.4 ± 6.1 | 51.9 ± 7.0 | 72.5 ± 5.1 | <0.001 |
| Women | 3514(50.3) | 1092(47.4) | 1733(51.0) | 689(54.1) | 0.004 |
| Education | |||||
| Low | 1496(20.0) | 23(0.8) | 639(18.8) | 834(65.3) | <0.001 |
| Medium | 1680(26.9) | 320(15.6) | 1113(37.7) | 247(20.3) | |
| High | 2923(53.1) | 1589(83.6) | 1189(43.5) | 145(14.4) | |
| No response | 295 | 81 | 145 | 69 | |
| Smoking status | |||||
| Non-smoker | 3752(57.7) | 1203(58.9) | 1798(55.8) | 751(60.6) | <0.001 |
| Former smoker | 1339(21.9) | 314(17.0) | 632(22.6) | 393(30.0) | |
| Current smoker | 1230(20.4) | 476(24.1) | 630(21.6) | 124(9.4) | |
| No response | 73 | 20 | 26 | 27 | |
| Alcohol consumption | |||||
| Non-drinker | 2788(40.1) | 654(31.2) | 1317(40.4) | 817(64.3) | <0.001 |
| Alcohol drinker | 3545(58.9) | 1346(68.8) | 1744(59.6) | 455(35.7) | |
| No response | 61 | 13 | 25 | 23 | |
| Physical activity | |||||
| No | 3336(52.3) | 877(43.1) | 1644(54.4) | 815(66.1) | <0.001 |
| Yes | 2762(47.7) | 1054(56.9) | 1301(45.6) | 407(33.9) | |
| No response | 296 | 82 | 141 | 73 | |
| BMI | |||||
| <25 | 4195(65.5) | 1412(69.5) | 1974(65.5) | 809(62.6) | 0.0002 |
| ≥25 | 2199(34.5) | 601(30.5) | 1112(36.5) | 486(37.4) | |
| WC | |||||
| Male < 90, Female < 85 | 4556(72.5) | 1577(79.0) | 2224(72.0) | 755(60.1) | <0.001 |
| Male ≥ 90, Female ≥ 85 | 1838(27.5) | 436(21.1) | 862(28.0) | 540(39.9) | |
| WHtR | |||||
| WHtR < 0.5 | 3147(52.1) | 1409(71.0) | 1433(47.5) | 305(24.7) | <0.001 |
| WHtR ≥ 0.5 | 3247(47.9) | 604(29.0) | 1653(52.5) | 990(75.3) | |
| ABSI | 77.56(4.64) | 74.94(3.96) | 77.56(3.92) | 81.62(4.25) | <0.001 |
| BRI | 3.49(1.14) | 2.94(1.13) | 3.53(1.06) | 4.24(1.27) | <0.001 |
| hs-CRP, mg/L | 1.17 ± 2.00 | 1.10 ± 1.96 | 1.09 ± 1.70 | 1.49 ± 2.60 | <0.001 |
| Folic acid, ng/mL | 7.39 ± 3.58 | 6.49 ± 3.40 | 7.76 ± 3.45 | 7.91 ± 3.88 | <0.001 |
| Total | 19–39 | 40–64 | 65+ | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | High | p | Low | High | p | Low | High | p | Low | High | p | |
| Age, y | 46.76 ± 16.98 | 51.78 ± 15.19 | <0.001 | 29.75 ± 6.26 | 31.51 ± 5.63 | <0.001 | 51.27 ± 6.98 | 52.83 ± 6.84 | <0.001 | 72.82 ± 5.11 | 72.16 ± 4.99 | 0.021 |
| women | 1296 (41.75) | 2218 (67.42) | <0.001 | 527 (43.3) | 565 (70.9) | <0.001 | 778 (44.4) | 955 (71.7) | <0.001 | 345 (45.6) | 344 (63.8) | <0.001 |
| Education | ||||||||||||
| Low | 645 (22.0) | 851 (26.9) | <0.001 | 18 (1.5) | 5 (0.6) | 0.027 | 333 (20.0) | 306 (24.1) | 0.020 | 495 (70.5) | 339 (64.7) | 0.092 |
| Medium | 787 (26.8) | 893 (28.2) | 208 (17.9) | 112 (14.6) | 656 (39.3) | 457 (35.9) | 132 (18.8) | 115 (21.9) | ||||
| High | 1505 (51.2) | 1418 (44.9) | 937 (80.6) | 652 (84.8) | 680 (40.7) | 509 (40.0) | 75 (10.7) | 70 (13.4) | ||||
| No response | 167 | 128 | 53 | 28 | 85 | 60 | 54 | 15 | ||||
| Smoking status | ||||||||||||
| Non-smoker | 1502 (49.0) | 2250 (69.2) | <0.001 | 662 (54.9) | 541 (68.8) | <0.001 | 838 (48.2) | 960 (72.7) | <0.001 | 376 (51.2) | 375 (70.2) | <0.001 |
| Former smoker | 685 (22.3) | 654 (20.1) | 173 (14.3) | 141 (18.0) | 408 (23.5) | 224 (16.9) | 258 (35.2) | 135 (25.3) | ||||
| Current smoker | 880 (28.7) | 350 (10.8) | 372 (30.8) | 104 (13.2) | 493 (28.4) | 137 (10.4) | 100 (13.6) | 24 (4.5) | ||||
| No response | 37 | 36 | 9 | 11 | 15 | 11 | 22 | 5 | ||||
| Alcohol consumption | ||||||||||||
| Non-drinker | 1176 (38.2) | 1612 (49.5) | <0.001 | 364 (30.0) | 290 (36.8) | 0.002 | 661 (38.0) | 656 (49.6) | <0.001 | 440 (59.8) | 377 (70.3) | <0.001 |
| Drinker | 1899 (61.8) | 1646 (50.5) | 848 (70.0) | 498 (63.2) | 1078 (62.0) | 666 (50.4) | 296 (40.2) | 159 (29.7) | ||||
| No response | 29 | 32 | 4 | 9 | 15 | 10 | 20 | 3 | ||||
| Physical activity | ||||||||||||
| No | 1666 (56.7) | 1670 (52.9) | <0.001 | 536 (46.1) | 341 (44.3) | 0.441 | 1006 (60.1) | 638 (50.2) | <0.001 | 491 (70.1) | 324 (62.1) | 0.003 |
| Yes | 1273 (43.3) | 1489 (47.1) | 626 (53.9) | 428 (55.7) | 667 (39.9) | 634 (49.8) | 209 (29.9) | 198 (37.9) | ||||
| No response | 165 | 131 | 54 | 28 | 81 | 60 | 56 | 17 | ||||
| BMI, kg/m2 | 24.15 ± 3.75 | 23.69 ± 3.32 | <0.001 | 23.83 ± 4.19 | 22.92 ± 3.69 | <0.001 | 24.44 ± 3.42 | 23.65 ± 3.13 | <0.001 | 24.19 ± 3.26 | 24.09 ± 3.09 | 0.593 |
| WC, cm | 83.29 ± 10.59 | 81.13 ± 9.75 | <0.001 | 80.76 ± 11.70 | 77.49 ± 10.61 | <0.001 | 83.95 ± 9.47 | 80.60 ± 8.95 | <0.001 | 86.09 ± 8.90 | 85.03 ± 9.02 | 0.036 |
| WHtR | 0.50 ± 0.07 | 0.50 ± 0.06 | 0.426 | 0.48 ± 0.06 | 0.47 ± 0.06 | <0.001 | 0.51 ± 0.06 | 0.50 ± 0.05 | <0.001 | 0.54 ± 0.06 | 0.54 ± 0.06 | 0.597 |
| ABSI | 77.65 ± 4.7 | 77.47 ± 4.58 | 0.139 | 75.09 ± 3.87 | 74.71 ± 4.08 | 0.037 | 77.87 ± 3.88 | 77.14 ± 3.95 | <0.001 | 81.83 ± 4.30 | 81.34 ± 4.16 | 0.041 |
| BRI | 3.51 ± 1.26 | 3.47 ± 1.18 | 0.283 | 3.01 ± 1.18 | 2.84 ± 1.06 | <0.001 | 3.62 ± 1.09 | 3.41 ± 1.00 | <0.001 | 4.26 ± 1.27 | 4.22 ± 1.27 | 0.597 |
| hs-CRP, mg/L | 1.24 ± 2.05 | 1.11 ± 1.95 | 0.013 | 1.13 ± 1.92 | 1.04 ± 2.03 | 0.287 | 1.17 ± 1.76 | 0.98 ± 1.61 | 0.003 | 1.54 ± 2.70 | 1.41 ± 2.44 | 0.398 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.-R.; Jung, S.M. Serum Folate Related to Five Measurements of Obesity and High-Sensitivity C-Reactive Protein in Korean Adults. Nutrients 2022, 14, 3461. https://doi.org/10.3390/nu14173461
Lee M-R, Jung SM. Serum Folate Related to Five Measurements of Obesity and High-Sensitivity C-Reactive Protein in Korean Adults. Nutrients. 2022; 14(17):3461. https://doi.org/10.3390/nu14173461
Chicago/Turabian StyleLee, Mee-Ri, and Sung Min Jung. 2022. "Serum Folate Related to Five Measurements of Obesity and High-Sensitivity C-Reactive Protein in Korean Adults" Nutrients 14, no. 17: 3461. https://doi.org/10.3390/nu14173461
APA StyleLee, M. -R., & Jung, S. M. (2022). Serum Folate Related to Five Measurements of Obesity and High-Sensitivity C-Reactive Protein in Korean Adults. Nutrients, 14(17), 3461. https://doi.org/10.3390/nu14173461