


Characteristics of Dietary Supplements with Folic Acid Available on the Polish Market


 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Folic Acid Supplements Database
2.2. Materials and Reagents
2.3. Sample Preparation and Folic Acid Quantification
3. Results and Discussion
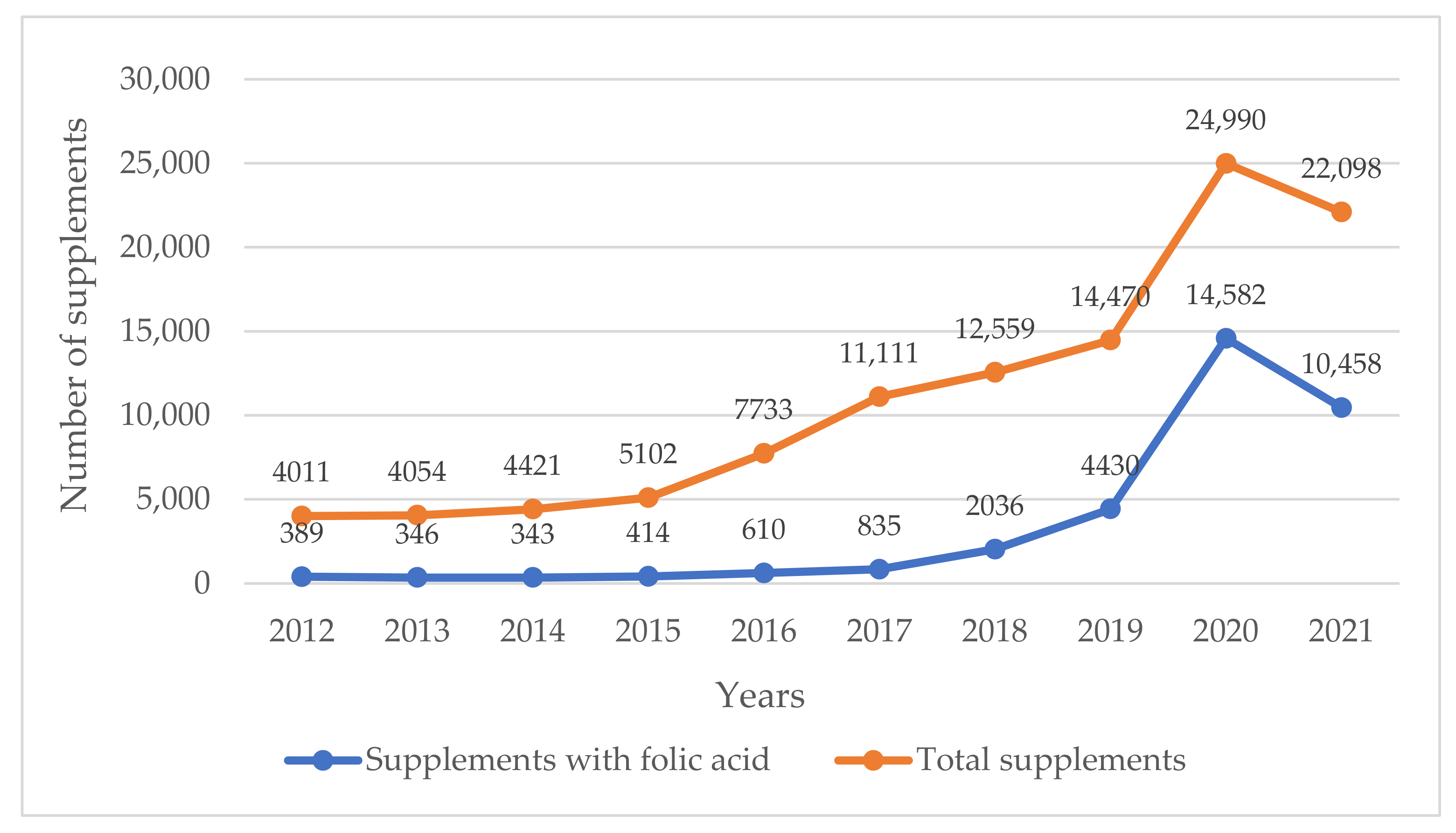
3.1. Market Analysis of Folic Acid Supplements
3.2. Folic Acid Content Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Polish Supreme Audit Office. Admission to Trading of the Dietary Supplements. Information about the Control Result. LLO.430.002.2016. Evidence Number 195/2016/P/16/078/LLO. 2017, pp. 1–61. Available online: https://www.nik.gov.pl/plik/id,13031,vp,15443.pdf (accessed on 16 April 2022). (In Polish)
- The Polish Supreme Audit Office. (Un)controlled Dietary Supplements. 2022. Available online: https://www.nik.gov.pl/aktualnosci/niekontrolowane-suplementy-diety.html (accessed on 16 April 2022). (In Polish)
- Directive 2002/46/EC of the European Parliament and of the Council of 10 June 2002 on the Approximation of the Laws of the Member States Relating to Food Supplements. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32002L0046 (accessed on 16 April 2022).
- Act of August 25, 2006 on Food and Nutrition Safety. Available online: https://lexlege.pl/ustawa-o-bezpieczenstwie-zywnosci-i-zywienia/ (accessed on 9 July 2022). (In Polish).
- MRC Vitamin Study Research Group. Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar] [CrossRef]
- WHO. Guideline: Optimal Serum and Red Blood Cell Folate Concentrations in Women of Reproductive Age for Prevention of Neural Tube Defects; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- An Official Website of the European Union. Folic Acid and Neural Tube Defects. Available online: https://eu-rd-platform.jrc.ec.europa.eu/eurocat/prevention-and-risk-factors/folic-acid-neural-tube-defects_en (accessed on 8 July 2022).
- Jarosz, M.; Stoś, K.; Przygoda, B.; Matczuk, E.; Stolińska-Fiedorowicz, H.; Kłys, W. Vitamins. In Standards for the Population of Poland; Jarosz, M., Ed.; IŻŻ: Warsaw, Poland, 2017; pp. 166–170. Available online: https://ncez.pl/upload/normy-net-1.pdf (accessed on 1 June 2022). (In Polish)
- DOZ.pl. Available online: https://www.doz.pl/ (accessed on 1 May 2022).
- Apteka Gemini. Available online: https://gemini.pl/ (accessed on 1 May 2022).
- Konings, E. Validated liquid chromatographic method for determining folates in vegetables, milk powder, liver, and flour. J. AOAC Int. 1999, 82, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Czarnowska-Kujawska, M.; Draszanowska, A.; Gujska, E.; Klepacka, J.; Kasińska, M. Folate Content and Yolk Color of Hen Eggs from Different Farming Systems. Molecules 2021, 26, 1034. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.F. Chemical and nutritional aspects of folate research, analytical procedures, methods of folate synthesis, stability, and bioavailabilty of dietary folates. Adv. Nutr. 1989, 33, 1–101. [Google Scholar] [CrossRef]
- Dang, J.; Arcot, J.; Shrestha, A. Folate retention in selected processed legumes. Food Chem. 2000, 68, 295–298. [Google Scholar] [CrossRef]
- Delchier, N.; Herbig, A.L.; Rychlik, M.; Renard, C.M.G.C. Folates in fruits and vegetables: Contents, processing and stability. Compr. Rev. Food Sci. Food Saf. 2016, 15, 506–528. [Google Scholar] [CrossRef]
- Saldanha, L.G.; Dwyer, J.T.; Haggans, C.J.; Mills, J.L.; Potischman, N. Perspective: Time to resolve confusion on folate amounts, units, and forms in prenatal supplements. Adv. Nutr. 2020, 11, 753–759. [Google Scholar] [CrossRef]
- Bomba-Opoń, D.; Hirnle, L.; Kalinka, J.; Seremak-Mrozikiewicz, A. Folate supplementation during the preconception period, pregnancy and puerperium. Polish Society of Gynecologists and Obstetri0cians Guidelines. Ginekol. Pol. 2017, 88, 633–636. [Google Scholar] [CrossRef]
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academy Press: Washington, DC, USA, 1998. [Google Scholar] [CrossRef]
- Dhonukshe-Rutten, R.A.M.; de Vries, J.H.M.; de Bree, A.; van der Put, N.; van Staveen, W.A.; de Groot, L.C.P.G.M. Dietary intake and status of folate and vitamin B12 and their association with homocysteine and cardiovascular disease in European populations. Eur. J. Clin. Nutr. 2009, 63, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Arnesen, E.; Refsum, H.; Bonaa, K.H.; Ueland, P.M.; Forde, O.H.; Nordrehaug, J.E. Serum total homocysteine and coronary heartdisease. Int. J. Epidemiol. 1995, 24, 704–709. [Google Scholar] [CrossRef]
- Morris, M.S.; Jacques, P.F.; Rosenberg, I.H.; Selhub, J. Folate and vitamin B-12 status in relation to anemia, macrocytosis, and cognitive impairment in older, Americans in the age of folic acid fortification. Am. J. Clin. Nutr. 2007, 85, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Qin, X.; Demirtas, H.; Li, J.; Mao, G.; Huo, Y. Efficacy of folic acid supplementation in stroke prevention: A meta-analysis. Lancet 2007, 369, 1876–1882. [Google Scholar] [CrossRef]
- Choi, S.W.; Mason, J.B. Folate and carcinogenesis: An integrated scheme. J. Nutr. 2000, 130, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Selhub, J.; Jacques, P.F.; Wilson, P.W.F.; Rush, D.; Rosenberg, I.H. Vitamin status and intake as primary determinants of homocysteinemia in an elderly population. JAMA 1993, 270, 2693–2698. [Google Scholar] [CrossRef] [PubMed]
- Rampersaud, G.C.; Bailey, L.B.; Kauwell, G.P.A. Folate: Relationship to colorectal and cervical cancer. Review and recommendations for practitioners. J. Am. Diet Assoc. 2002, 102, 1273–1282. [Google Scholar] [CrossRef]
- Bean, L.J.; Allen, E.G.; Tinker, S.W.; Hollis, N.D.; Locke, A.E.; Druschel, C.; Hobbs, C.A.; O’Leary, L.; Romitti, P.A.; Royle, M.H.; et al. Lack of maternal folic acid supplementation is associated with heart defects in Down syndrome: A report from the National Down Syndrome Project. Birth Defects Res. A Clin. Mol. Teratol. 2011, 91, 885–893. [Google Scholar] [CrossRef]
- Li, Z.; Ye, R.; Zhang, L.; Li, H.; Liu, J.; Ren, A. Folic acid supplementation during early pregnancy and the risk of gestational hypertension and preeclampsia. Hypertension 2013, 61, 873–879. [Google Scholar] [CrossRef]
- Wen, S.W.; Guo, Y.; Rodger, M.; White, R.R.; Yang, Q.; Smith, G.N.; Perkins, S.L.; Walker, M.C. Folic Acid Supplementation in Pregnancy and the Risk of Pre-Eclampsia-A Cohort Study. PLoS ONE 2016, 11, e0149818. [Google Scholar] [CrossRef]
- Sicińska, E.; Wyka, J. Spożycie folianów w Polsce na podstawie piśmiennictwa z ostatnich 10 lat (2000-2010). Folate intake in Poland on the basis of literature from the last ten years (2000–2010). Roczn. PZH 2011, 62, 247–256. (In Polish) [Google Scholar]
- National Diet and Nutrition Survey Results from 2008 to 2017 Assessing Time and Income Trends for Diet, Nutrient Intake and Nutritional Status for the UK. Available online: https://www.gov.uk/government/statistics/ndns-time-trend-and-income-analyses-for-years-1-to-9 (accessed on 1 June 2022).
- Chief Sanitary Inspectorate. Food Safety and Nutrition Department. Register of Products Subjected to the Notification of the First Placing to the Market. Available online: https://powiadomienia.gis.gov.pl/ (accessed on 9 July 2022). (In Polish)
- Raport. Polacy a Suplementy Diety. Report. Poles and Dietary Supplements. Supplementation Habits. 2022. Available online: https://pulsmedycyny.pl/67-proc-polakow-zazywa-suplementy-diety-blisko-polowa-nie-konsultuje-tego-z-zadnym-specjalista-raport-1148877 (accessed on 10 July 2022). (In Polish).
- Dziedziński, M.; Goryńska-Goldmann, E.; Kobus-Cisowska, J.; Szczepaniak, O.; Marciniak, G. Problem nadkonsumpcji suplementów diety przez Polaków. The problem of overconsumption of supplements by Poles. Intercathedra 2019, 3, 235–242. [Google Scholar]
- Journal of Laws 2018 Item 1951. Announcement of the Minister of Health of 17 September 2018 on the Publication of the Uniform Text of the Regulation of the Minister of Health on the Composition and Labeling of Dietary Supplements. Available online: https://www.infor.pl/akt-prawny/DZU.2018.199.0001951,rozporzadzenie-ministra-zdrowia-w-sprawie-skladu-oraz-oznakowania-suplementow-diety.html (accessed on 15 August 2022).
- McNulty, H.; Pentieva, K. Folate bioavailability. Proc. Nutr. Soc. 2004, 63, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.R.; McPartlin, J.; Scott, J. Folic acid fortification and public health: Report on threshold doses above which unmetabolised folic acid appear in serum. BMC Public Health 2007, 7, 41. [Google Scholar] [CrossRef] [PubMed]
- Altic, L.; McNulty, H.; Hoey, L.; McAnena, L.; Pentieva, K. Validation of Folate-Enriched eggs as a functional food for improving folate intake in consumers. Nutrients 2016, 8, 777. [Google Scholar] [CrossRef]
- The UK Government. Proposal to Add Folic Acid to Flour: Consultation Document. 2021. Available online: https://www.gov.uk/government/consultations/adding-folic-acid-to-flour/proposal-to-add-folic-acid-to-flour-consultation-document (accessed on 9 July 2022).
- No. 7/2019 of the Team for Dietary Supplements of June 11, 2019 on Expressing an Opinion on the Maximum Dose of Folic Acid in the Recommended Daily Dose in Dietary Supplements. Available online: https://www.gov.pl/web/gis/zespol-do-spraw-suplementow-diety (accessed on 11 August 2022). (In Polish)
- Sicinska, E.; Wasik, M. Suplementy diety jako dodatkowe źródło kwasu foliowego. Dietary supplements as additional sources of folic acid. Bromat. Chem. Toxicol. XLV 2012, 2, 152–158. (In Polish) [Google Scholar]
- Kancherla, V.; Botto, L.D.; Rowe, L.A.; Shlobin, N.A.; Caceres, A.; Arynchyna-Smith, A.; Zimmerman, K.; Blount, J.; Kibruyisfaw, Z.; Ghotme, K.A.; et al. Preventing birth defects, saving lives, and promoting health equity: An urgent call to action for universal mandatory food fortification with folic acid. Lancet Glob. Health 2022, 10, e1053–e1057. [Google Scholar] [CrossRef]
- Kim, Y. Folate: A magic bullet or a double edged sword for colorectal cancer prevention? Gut 2006, 55, 1387–1389. [Google Scholar] [CrossRef]
- Moazzen, S.; Dolatkhah, R.; Tabrizi, J.S.; Shaarbafi, J.; Alizadeh, B.Z.; de Bock, G.H.; Dastgiri, S. Folic acid intake and folate status and colorectal cancer risk: A systematic review and meta-analysis. Clin. Nutr. 2018, 37, 1926–1934. [Google Scholar] [CrossRef]
- Blakley, R. The Biochemistry of Folic Acid and Related Pteridines; North-Holland Publishing Company: Amsterdam, The Netherlands, 1969; Volume 13. [Google Scholar]
- Garrett, G.S.; Bailey, L.B. A public health approach for preventing neural tube defects: Folic acid fortification and beyond. Ann. N. Y. Acad. Sci. 2018, 1414, 47–58. [Google Scholar] [CrossRef]
- Samaniego-Vaesken, M.L.; Alonso-Aperte, E.; Varela-Moreiras, G. Voluntary fortification with folic acid in Spain: An updated food composition database. Food Chem. 2016, 193, 148–153. [Google Scholar] [CrossRef]
- Gujska, E.; Michalak, J.; Czarnowska, M. Effect of storage time and temperature on the stability of folic acid and folate in selected fruit and fruit and vegetable juices. Zywn. Nauka, Technol. Jakosc. 2013, 6, 130–138. (In Polish) [Google Scholar] [CrossRef]
- Rampersaud, G.C.; Kauwell, G.P.; Bailey, L.B. Folate: A key to optimizing health and reducing disease risk in the elderly. J. Am. Coll. Nutr. 2003, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Finglas, P.M.; de Meer, K.; Molloy, A.; Verhoef, P.; Pietrzik, K.; Powers, H.J.; van der Straeten, D.; Jägerstad, M.; Varela-Moreiras, G.; van Vliet, T.; et al. Research goals for folate and related B vitamin in Europe. Eur. J. Clin. Nutr. 2006, 60, 287–294. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Gender and Age | Folate Equivalent (µg/day) | |
|---|---|---|
| RDA | AI | |
| Infants | ||
| 0–6 months | 65 | |
| 7–11 months | 80 | |
| Children | ||
| 1–3 | 150 | |
| 4–6 | 200 | |
| 7–9 | 300 | |
| Teenagers | ||
| 10–12 | 300 | |
| 13–18 | 400 | |
| Adults | ||
| 19–75 | 400 | |
| Pregnant women | 600 | |
| Lactating | 500 | |
| Intended Use | No. of Products | Declared Folic Acid Content (µg per Dose) | |
|---|---|---|---|
| Min-Max | Mode * | ||
| For adults | |||
| Supplementation of the daily diet | 164 | 16–1000 | 200 |
| Proper heart function, maintenance of normal cholesterol levels and homocysteine metabolism | 29 | 30–600 | 200 |
| Promotes proper vision | 6 | 100–400 | 200 |
| Increased physical and mental effort | 19 | 40–400 | 200 |
| Supporting the functioning of the nervous system, supporting the work of the brain | 11 | 200–400 | 200 |
| For women | |||
| For women (general) | 21 | 100–400 | 200 |
| For women planning and/or pregnant and breastfeeding | 76 | 100–800 | 400 |
| Better condition of skin, hair and nails | 28 | 25–600 | 200 |
| For women over 50 and going through menopause | 12 | 20–400 | 400 |
| For men | 18 | 133–400 | 200 |
| For children | 36 | 12.5–300 | 100 |
| For the elderly | 14 | 100–400 | 100 |
| Product No. | Determined FA Content | Declared FA Content (DV 1) | Difference with the Declared FA Content |
|---|---|---|---|
| One-ingredient supplements (µg per tablet, capsule) | [%] | ||
| 1 | 296.52 ± 8.4 | 400 | 25.9 |
| 2 | 374.6 ± 9.3 | 400 | 6.4 |
| 3 | 374.5 ± 10.8 | 400 | 6.4 |
| 4 | 290.4 ± 22.7 | 400 | 27.4 |
| 5 | 292.5 ± 20.5 | 400 | 26.9 |
| 6 | 361.1 ± 2.9 | 400 | 9.7 |
| 7 | 320.2 ± 26.6 | 400 | 20.0 |
| 8 | 304.0 ± 14.7 | 400 | 24.0 |
| Multi-ingredients supplements (µg per tablet, capsule) | [%] | ||
| 9 | 3.8 ± 0.3 | 400 | 99.1 |
| 10 | 339.2 ± 13.5 | 400 | 15.2 |
| 11 | 327.2 ± 20.4 | 400 | 18.2 |
| 12 | 3.6 ± 0.2 | 400 | 99.1 |
| 13 | 193.9 ± 9.1 | 600 | 67.7 |
| 14 | 314.7 ± 28.1 | 400 | 21.3 |
| 15 | 371.6 ± 48.4 | 600 | 38.1 |
| 16 | 209.9 ± 8.57 | 400 | 47.5 |
| 17 | 258.2 ± 1.79 | 400 | 35.5 |
| 18 | 250.4 ± 6.8 | 300 | 16.5 |
| 19 | 195.2 ± 8.94 | 200 | 2.4 |
| 20 | 167.3 ± 2.56 | 200 | 16.4 |
| Multi-ingredients liquid supplements (µg per portion mL) | [%] | ||
| 21 | 204.1 ± 7.7 | 200 | +2.0 |
| 22 | 10.7 ± 0.7 | 30 | 64.4 |
| 23 | 87.8 ± 3.4 | 180 | 51.2 |
| 24 | 173.4 ± 4.1 | 200 | 13.3 |
| 25 | 80.6 ± 3.1 | 100 | 19.4 |
| 26 | 65.1 ± 0.9 | 147 | 55.7 |
| 27 | 1.2 ± 0.1 | 50 | 97.5 |
| 28 | 184.1 ± 17.9 | 200 | 8.0 |
| 29 | 1.2 ± 0.1 | 169 | 99.3 |
| 30 | 57.9 ± 1.0 | 290 | 80.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czarnowska-Kujawska, M.; Klepacka, J.; Zielińska, O.; Samaniego-Vaesken, M.d.L. Characteristics of Dietary Supplements with Folic Acid Available on the Polish Market. Nutrients 2022, 14, 3500. https://doi.org/10.3390/nu14173500
Czarnowska-Kujawska M, Klepacka J, Zielińska O, Samaniego-Vaesken MdL. Characteristics of Dietary Supplements with Folic Acid Available on the Polish Market. Nutrients. 2022; 14(17):3500. https://doi.org/10.3390/nu14173500
Chicago/Turabian StyleCzarnowska-Kujawska, Marta, Joanna Klepacka, Olga Zielińska, and María de Lourdes Samaniego-Vaesken. 2022. "Characteristics of Dietary Supplements with Folic Acid Available on the Polish Market" Nutrients 14, no. 17: 3500. https://doi.org/10.3390/nu14173500
APA StyleCzarnowska-Kujawska, M., Klepacka, J., Zielińska, O., & Samaniego-Vaesken, M. d. L. (2022). Characteristics of Dietary Supplements with Folic Acid Available on the Polish Market. Nutrients, 14(17), 3500. https://doi.org/10.3390/nu14173500