

Glucosamine Use Is Associated with a Higher Risk of Cardiovascular Diseases in Patients with Osteoarthritis: Results from a Large Study in 685,778 Subjects
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
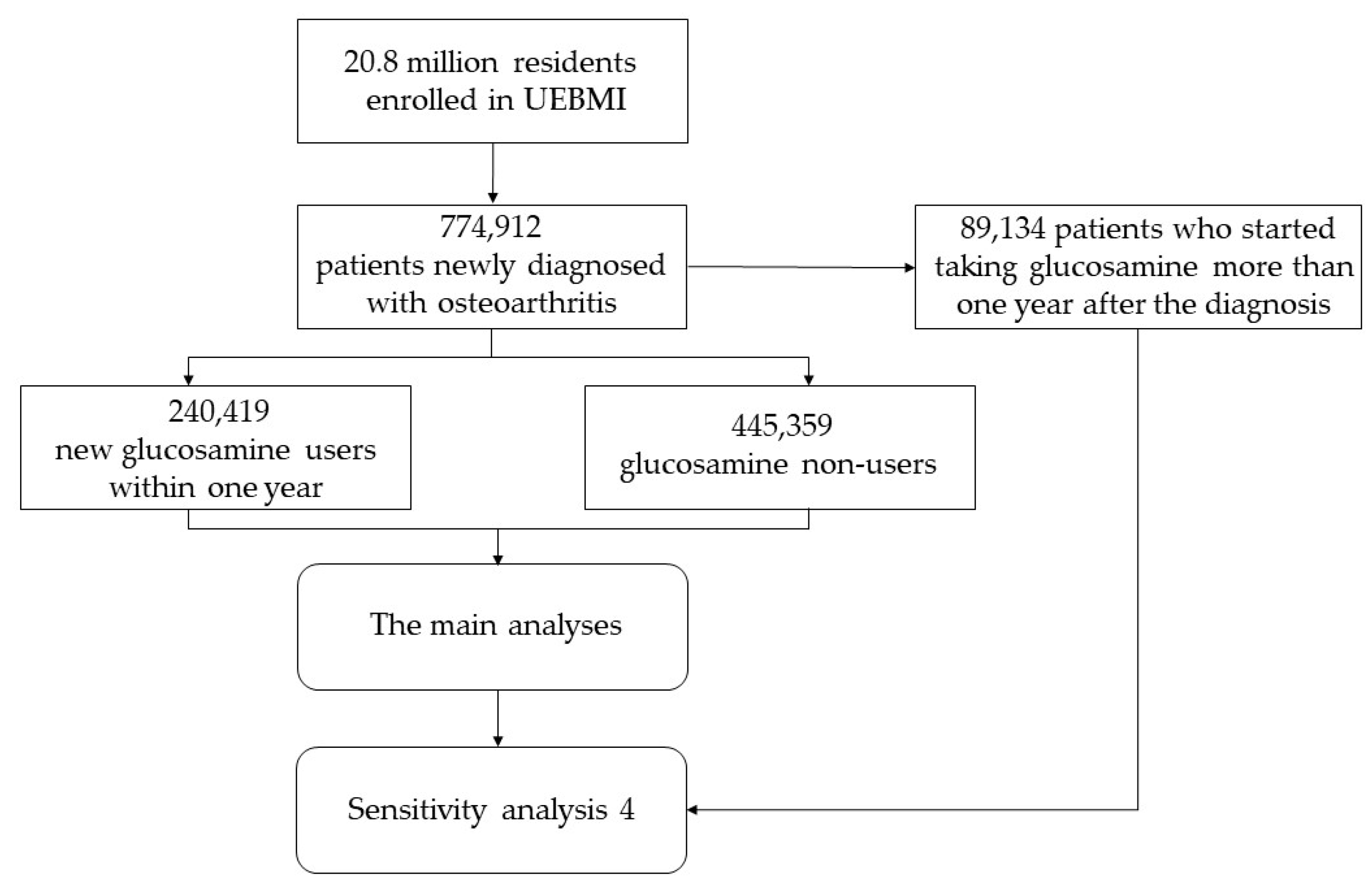
2.2. Population
2.3. Exposure, Outcome, and Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Study Population
3.2. Incidence of CVD Events
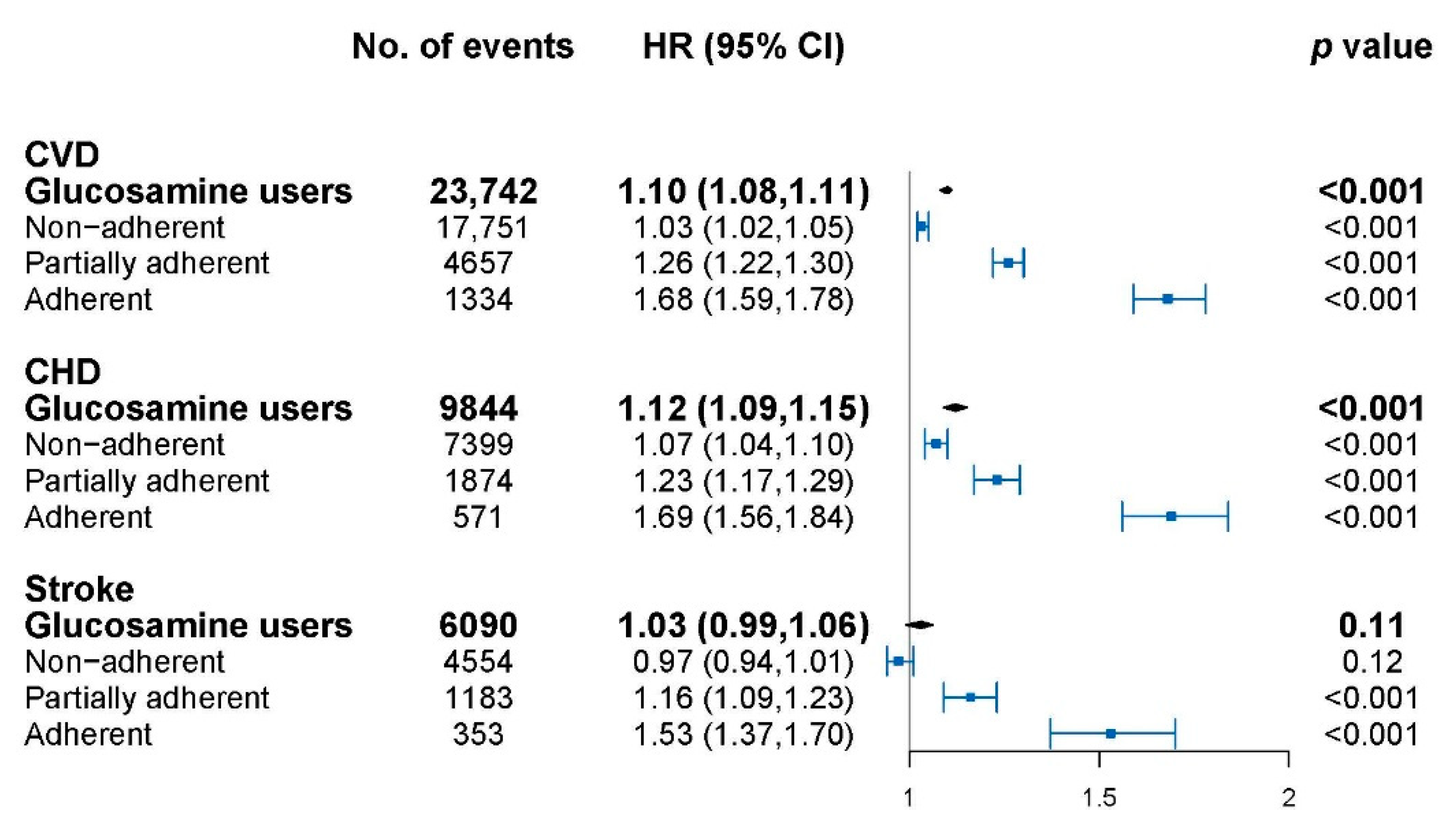
3.3. Association of Glucosamine with Cardiovascular Events
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Adjusted Covariates | HR (95% CI) for Glucosamine Use |
|---|---|
| None | 1.11 (1.09, 1.13) |
| +Age | 1.06 (1.04, 1.07) |
| +Sex | 1.09 (1.08, 1.11) |
| +Hypertension | 1.10 (1.08, 1.11) |
| +Lipid treatment | 1.07 (1.05, 1.09) |
| +Antiplatelet treatment | 1.06 (1.05, 1.08) |
| +NSAIDs therapy | 1.06 (1.05, 1.08) |
| +CCI | 1.09 (1.07, 1.10) |
| +HCUI (full model) | 1.10 (1.08, 1.11) |

References
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Bruyère, O.; Honvo, G.; Veronese, N.; Arden, N.K.; Branco, J.; Curtis, E.M.; Al-Daghri, N.M.; Herrero-Beaumont, G.; Martel-Pelletier, J.; Pelletier, J.P.; et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Semin. Arthritis Rheum. 2019, 49, 337–350. [Google Scholar] [CrossRef]
- Barnes, P.M.; Bloom, B.; Nahin, R.L. Complementary and alternative medicine use among adults and children: United States, 2007. Natl. Health Stat. Rep. 2008, 10, 1–23. [Google Scholar]
- Sibbritt, D.; Adams, J.; Lui, C.W.; Broom, A.; Wardle, J. Who uses glucosamine and why? A study of 266,848 Australians aged 45 years and older. PLoS ONE 2012, 7, e41540. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Li, X.; Sun, D.; Zhou, T.; Ley, S.H.; Gustat, J.; Heianza, Y.; Qi, L. Association of habitual glucosamine use with risk of cardiovascular disease: Prospective study in UK Biobank. BMJ 2019, 365, l1628. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.; Cornea, A.; Blick, K.E.; Jenkins, A.; Scofield, R.H. Oral glucosamine in doses used to treat osteoarthritis worsens insulin resistance. Am. J. Med. Sci. 2007, 333, 333–339. [Google Scholar] [CrossRef]
- Almada, A.; Harvey, P.; Platt, K. Effect of chronic oral glucosamine sulfate upon fasting insulin resistance index (FIRI) in non-diabetic individuals. Faseb J. 2000, 14, A750. [Google Scholar]
- Monauni, T.; Zenti, M.G.; Cretti, A.; Daniels, M.C.; Targher, G.; Caruso, B.; Caputo, M.; McClain, D.; Del Prato, S.; Giaccari, A.; et al. Effects of glucosamine infusion on insulin secretion and insulin action in humans. Diabetes 2000, 49, 926–935. [Google Scholar] [CrossRef]
- Biggee, B.A.; Blinn, C.M.; Nuite, M.; Silbert, J.E.; McAlindon, T.E. Effects of oral glucosamine sulphate on serum glucose and insulin during an oral glucose tolerance test of subjects with osteoarthritis. Ann. Rheum. Dis. 2007, 66, 260–262. [Google Scholar] [CrossRef]
- Meininger, C.J.; Kelly, K.A.; Li, H.; Haynes, T.E.; Wu, G. Glucosamine inhibits inducible nitric oxide synthesis. Biochem. Biophys. Res. Commun. 2000, 279, 234–239. [Google Scholar] [CrossRef]
- Numaguchi, K.; Egashira, K.; Takemoto, M.; Kadokami, T.; Shimokawa, H.; Sueishi, K.; Takeshita, A. Chronic inhibition of nitric oxide synthesis causes coronary microvascular remodeling in rats. Hypertension 1995, 26, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Toda, N. Age-related changes in endothelial function and blood flow regulation. Pharmacol. Ther. 2012, 133, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Kendzerska, T.; Jüni, P.; King, L.K.; Croxford, R.; Stanaitis, I.; Hawker, G.A. The longitudinal relationship between hand, hip and knee osteoarthritis and cardiovascular events: A population-based cohort study. Osteoarthr. Cartil. 2017, 25, 1771–1780. [Google Scholar] [CrossRef] [PubMed]
- Schieir, O.; Tosevski, C.; Glazier, R.H.; Hogg-Johnson, S.; Badley, E.M. Incident myocardial infarction associated with major types of arthritis in the general population: A systematic review and meta-analysis. Ann. Rheum. Dis. 2017, 76, 1396–1404. [Google Scholar] [CrossRef]
- Atiquzzaman, M.; Karim, M.E.; Kopec, J.; Wong, H.; Anis, A.H. Role of Nonsteroidal Antiinflammatory Drugs in the Association between Osteoarthritis and Cardiovascular Diseases: A Longitudinal Study. Arthritis Rheumatol. 2019, 71, 1835–1843. [Google Scholar] [CrossRef] [PubMed]
- Clegg, D.O.; Reda, D.J.; Harris, C.L.; Klein, M.A.; O’Dell, J.R.; Hooper, M.M.; Bradley, J.D.; Bingham, C.O.; Weisman, M.H.; Jackson, C.G.; et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N. Engl. J. Med. 2006, 354, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C.; Martel-Pelletier, J.; Monfort, J.; Möller, I.; Castillo, J.R.; Arden, N.; Berenbaum, F.; Blanco, F.J.; Conaghan, P.G.; Doménech, G.; et al. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis: A multicentre, randomised, double-blind, non-inferiority trial versus celecoxib. Ann. Rheum. Dis. 2016, 75, 37–44. [Google Scholar] [CrossRef]
- Roman-Blas, J.A.; Castañeda, S.; Sánchez-Pernaute, O.; Largo, R.; Herrero-Beaumont, G. Combined Treatment with Chondroitin Sulfate and Glucosamine Sulfate Shows no Superiority over Placebo for Reduction of Joint Pain and Functional Impairment in Patients with Knee Osteoarthritis: A Six-Month Multicenter, Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Arthritis Rheumatol. 2017, 69, 77–85. [Google Scholar] [CrossRef]
- McAlindon, T.E.; LaValley, M.P.; Gulin, J.P.; Felson, D.T. Glucosamine and chondroitin for treatment of osteoarthritis: A systematic quality assessment and meta-analysis. JAMA 2000, 283, 1469–1475. [Google Scholar] [CrossRef]
- Sawitzke, A.D.; Shi, H.; Finco, M.F.; Dunlop, D.D.; Harris, C.L.; Singer, N.G.; Bradley, J.D.; Silver, D.; Jackson, C.G.; Lane, N.E.; et al. Clinical efficacy and safety of glucosamine, chondroitin sulphate, their combination, celecoxib or placebo taken to treat osteoarthritis of the knee: 2-year results from GAIT. Ann. Rheum. Dis. 2010, 69, 1459–1464. [Google Scholar] [CrossRef]
- Li, Z.H.; Gao, X.; Chung, V.C.; Zhong, W.F.; Fu, Q.; Lv, Y.B.; Wang, Z.H.; Shen, D.; Zhang, X.R.; Zhang, P.D.; et al. Associations of regular glucosamine use with all-cause and cause-specific mortality: A large prospective cohort study. Ann. Rheum. Dis. 2020, 79, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yang, C.; Xi, H.; Zhang, Y.; Zhou, Z.; Hu, Y. Prescription of antibacterial agents for acute upper respiratory tract infections in Beijing, 2010–2012. Eur. J. Clin. Pharmacol. 2016, 72, 359–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Liu, H.; Wu, Y.; Si, Y.; Song, J.; Cao, Y.; Li, M.; Wu, Y.; Wang, X.; Chen, L.; et al. Association between ambient fine particulate pollution and hospital admissions for cause specific cardiovascular disease: Time series study in 184 major Chinese cities. BMJ 2019, 367, l6572. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Liu, H.; Si, Y.; Cao, Y.; Song, J.; Li, M.; Wu, Y.; Wang, X.; Xiang, X.; Juan, J.; et al. Association between temperature variability and daily hospital admissions for cause-specific cardiovascular disease in urban China: A national time-series study. PLoS Med. 2019, 16, e1002738. [Google Scholar] [CrossRef]
- Yip, W.C.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Benner, J.S.; Glynn, R.J.; Mogun, H.; Neumann, P.J.; Weinstein, M.C.; Avorn, J. Long-term persistence in use of statin therapy in elderly patients. JAMA 2002, 288, 455–461. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2022. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 14 June 2022).
- Xie, J.; Strauss, V.Y.; Martinez-Laguna, D.; Carbonell-Abella, C.; Diez-Perez, A.; Nogues, X.; Collins, G.S.; Khalid, S.; Delmestri, A.; Turkiewicz, A.; et al. Association of Tramadol vs Codeine Prescription Dispensation with Mortality and Other Adverse Clinical Outcomes. JAMA 2021, 326, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef]
- Palma Dos Reis, R.; Giacovelli, G.; Girolami, F.; André, R.; Bonazzi, A.; Rovati, L.C. Crystalline glucosamine sulfate in the treatment of osteoarthritis: Evidence of long-term cardiovascular safety from clinical trials. Open Rheumatol. J. 2011, 5, 69–77. [Google Scholar] [CrossRef]
- Ma, H.; Li, X.; Zhou, T.; Sun, D.; Liang, Z.; Li, Y.; Heianza, Y.; Qi, L. Glucosamine Use, Inflammation, and Genetic Susceptibility, and Incidence of Type 2 Diabetes: A Prospective Study in UK Biobank. Diabetes Care 2020, 43, 719–725. [Google Scholar] [CrossRef]
- Traxinger, R.R.; Marshall, S. Coordinated regulation of glutamine:fructose-6-phosphate amidotransferase activity by insulin, glucose, and glutamine. Role of hexosamine biosynthesis in enzyme regulation. J. Biol. Chem. 1991, 266, 10148–10154. [Google Scholar] [CrossRef]
- Marshall, S.; Bacote, V.; Traxinger, R.R. Discovery of a metabolic pathway mediating glucose-induced desensitization of the glucose transport system. Role of hexosamine biosynthesis in the induction of insulin resistance. J. Biol. Chem. 1991, 266, 4706–4712. [Google Scholar] [CrossRef]
- Baron, A.D.; Zhu, J.S.; Zhu, J.H.; Weldon, H.; Maianu, L.; Garvey, W.T. Glucosamine induces insulin resistance in vivo by affecting GLUT 4 translocation in skeletal muscle. Implications for glucose toxicity. J. Clin. Investig. 1995, 96, 2792–2801. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.B.; Zhu, J.S.; Zierath, J.R.; Shen, H.Q.; Baron, A.D.; Kahn, B.B. Glucosamine infusion in rats rapidly impairs insulin stimulation of phosphoinositide 3-kinase but does not alter activation of Akt/protein kinase B in skeletal muscle. Diabetes 1999, 48, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Patti, M.E.; Virkamäki, A.; Landaker, E.J.; Kahn, C.R.; Yki-Järvinen, H. Activation of the hexosamine pathway by glucosamine in vivo induces insulin resistance of early postreceptor insulin signaling events in skeletal muscle. Diabetes 1999, 48, 1562–1571. [Google Scholar] [CrossRef]
- Werstuck, G.H.; Khan, M.I.; Femia, G.; Kim, A.J.; Tedesco, V.; Trigatti, B.; Shi, Y. Glucosamine-induced endoplasmic reticulum dysfunction is associated with accelerated atherosclerosis in a hyperglycemic mouse model. Diabetes 2006, 55, 93–101. [Google Scholar] [CrossRef]
- Haffner, S.M. Pre-diabetes, insulin resistance, inflammation and CVD risk. Diabetes Res. Clin. Pract. 2003, 61 (Suppl. 1), S9–S18. [Google Scholar] [CrossRef]
- Caccamo, G.; Bonura, F.; Bonura, F.; Vitale, G.; Novo, G.; Evola, S.; Evola, G.; Grisanti, M.R.; Novo, S. Insulin resistance and acute coronary syndrome. Atherosclerosis 2010, 211, 672–675. [Google Scholar] [CrossRef]
- Effoe, V.S.; Wagenknecht, L.E.; Echouffo Tcheugui, J.B.; Chen, H.; Joseph, J.J.; Kalyani, R.R.; Bell, R.A.; Wu, W.H.; Casanova, R.; Bertoni, A.G. Sex Differences in the Association between Insulin Resistance and Incident Coronary Heart Disease and Stroke Among Blacks without Diabetes Mellitus: The Jackson Heart Study. J. Am. Heart Assoc. 2017, 6, e004229. [Google Scholar] [CrossRef]
- Kernan, W.N.; Inzucchi, S.E.; Viscoli, C.M.; Brass, L.M.; Bravata, D.M.; Horwitz, R.I. Insulin resistance and risk for stroke. Neurology 2002, 59, 809–815. [Google Scholar] [CrossRef]
- Balarini, C.M.; Leal, M.A.; Gomes, I.B.; Pereira, T.M.; Gava, A.L.; Meyrelles, S.S.; Vasquez, E.C. Sildenafil restores endothelial function in the apolipoprotein E knockout mouse. J. Transl. Med. 2013, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Nielsen, R.J.P.A. Why Propensity Scores Should Not Be Used for Matching. Political Anal. 2019, 27, 1–20. [Google Scholar] [CrossRef] [Green Version]

| Characteristics | Glucosamine Non-Users (n = 445,359) | Glucosamine Users (n= 240,419) | p Value |
|---|---|---|---|
| Age, years, mean (SD) | 55.44 (15.40) | 58.43 (12.24) | <0.001 |
| Female, n(%) | 247,181 (55.50) | 159,826 (66.48) | <0.001 |
| Hypertension, n(%) | 89,394 (20.07) | 55,974 (23.28) | <0.001 |
| Lipid treatment, n(%) | 153,169 (34.39) | 102,571 (42.66) | <0.001 |
| Antiplatelet treatment 1, n(%) | 113,118 (25.40) | 77,084 (32.06) | <0.001 |
| NSAIDs therapy 2, n(%) | 140,099 (31.46) | 63,387 (26.37) | <0.001 |
| CCI, mean (SD) | 0.65 (0.93) | 0.71 (0.86) | <0.001 |
| HCUI, median (IQR) | 22 (7, 45) | 20 (6, 45) | <0.001 |
| Glucosamine Non-Users | Glucosamine Users | p Value 2 | |||
|---|---|---|---|---|---|
| Number of Events | Incidence 1 (95% CI) | Number of Events | Incidence 1 (95% CI) | ||
| Overall CVD | 40,858 | 15.08 (14.93, 15.23) | 23,742 | 16.63 (16.42, 16.84) | <0.001 |
| CHD | 16,686 | 6.01 (5.91, 6.10) | 9844 | 6.72 (6.59, 6.85) | <0.001 |
| Stroke | 11,742 | 4.21 (4.13, 4.28) | 6090 | 4.13 (4.03, 4.23) | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.; Wu, J.; Chen, H.; Wang, M.; Wang, S.; Yang, R.; Zhan, S.; Qin, X.; Wu, T.; Wu, Y.; et al. Glucosamine Use Is Associated with a Higher Risk of Cardiovascular Diseases in Patients with Osteoarthritis: Results from a Large Study in 685,778 Subjects. Nutrients 2022, 14, 3694. https://doi.org/10.3390/nu14183694
Yu H, Wu J, Chen H, Wang M, Wang S, Yang R, Zhan S, Qin X, Wu T, Wu Y, et al. Glucosamine Use Is Associated with a Higher Risk of Cardiovascular Diseases in Patients with Osteoarthritis: Results from a Large Study in 685,778 Subjects. Nutrients. 2022; 14(18):3694. https://doi.org/10.3390/nu14183694
Chicago/Turabian StyleYu, Huan, Junhui Wu, Hongbo Chen, Mengying Wang, Siyue Wang, Ruotong Yang, Siyan Zhan, Xueying Qin, Tao Wu, Yiqun Wu, and et al. 2022. "Glucosamine Use Is Associated with a Higher Risk of Cardiovascular Diseases in Patients with Osteoarthritis: Results from a Large Study in 685,778 Subjects" Nutrients 14, no. 18: 3694. https://doi.org/10.3390/nu14183694
APA StyleYu, H., Wu, J., Chen, H., Wang, M., Wang, S., Yang, R., Zhan, S., Qin, X., Wu, T., Wu, Y., & Hu, Y. (2022). Glucosamine Use Is Associated with a Higher Risk of Cardiovascular Diseases in Patients with Osteoarthritis: Results from a Large Study in 685,778 Subjects. Nutrients, 14(18), 3694. https://doi.org/10.3390/nu14183694