
High Plasma Vitamin B12 and Cancer in Human Studies: A Scoping Review to Judge Causality and Alternative Explanations


Abstract
:1. Introduction
2. Materials and Methods
Search Methodology
3. Results
3.1. Vitamin B12 and Liver Cancer
3.2. Critical Evaluation
3.3. Vitamin B12 and Other Type of Cancers
3.4. Genetic and Mendelian Randomization Studies
3.5. Randomized Controlled Trials, Their Secondary Analyses and Meta-Analyses
4. Discussion
4.1. Does High Plasma B12 Concentrations or High B12 Intake Cause Cancer
4.2. Alternative Mechanisms That Could Be in Play
4.3. Additional Arguments against a Causal Role of B12 in the Etiology of Cancer and Possible Non-Causal Explanations
4.4. Studies Needed to Clarify the Nature of the Association between High Plasma B12 and Cancer
4.5. Vitamin B12 Deficiency in Patients with Cancers
4.6. Limitations of the Present Study
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hall, C.A. Transcobalamins I and II as natural transport proteins of vitamin B12. J. Clin. Investig. 1975, 56, 1125–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, A.P.; Ilter, D.; Low, V.; Endress, J.E.; Fernandez-Garcia, J.; Rosenzweig, A.; Schild, T.; Broekaert, D.; Ahmed, A.; Planque, M.; et al. Age-induced accumulation of methylmalonic acid promotes tumour progression. Nature 2020, 585, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.P.; Ilter, D.; Low, V.; Drapela, S.; Schild, T.; Mullarky, E.; Han, J.; Elia, I.; Broekaert, D.; Rosenzweig, A.; et al. Altered propionate metabolism contributes to tumour progression and aggressiveness. Nat. Metab. 2022, 4, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Bowen, R.A.; Drake, S.K.; Vanjani, R.; Huey, E.D.; Grafman, J.; Horne, M.K., III. Markedly increased vitamin B12 concentrations attributable to IgG-IgM-vitamin B12 immune complexes. Clin. Chem. 2006, 52, 2107–2114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remacha, A.F.; Zapico, E.; Sarda, M.P.; Rojas, E.; Simo, M.; Remacha, J.; Homs, R.; Queralto, J.M. Immune complexes and persistent high levels of serum vitamin B12. Int. J. Lab. Hematol. 2014, 36, 92–97. [Google Scholar] [CrossRef]
- Duim, S.N.; Vlasveld, L.T.; Mezger, S.T.P.; Mingels, A.M.A.; Ramakers, C.R.B.; de Boer, D.; Heil, S.G.; Nexo, E.; van Rossum, A.P. “Macro transcobalamin causing raised vitamin B12: Case-based laboratory investigation”. Ann. Clin. Biochem. 2022, 59, 302–307. [Google Scholar] [CrossRef]
- Lin, C.Y.; Kuo, C.S.; Lu, C.L.; Wu, M.Y.; Huang, R.F. Elevated serum vitamin B(12) levels in association with tumor markers as the prognostic factors predictive for poor survival in patients with hepatocellular carcinoma. Nutr. Cancer 2010, 62, 190–197. [Google Scholar] [CrossRef]
- Cui, L.H.; Quan, Z.Y.; Piao, J.M.; Zhang, T.T.; Jiang, M.H.; Shin, M.H.; Choi, J.S. Plasma Folate and Vitamin B12 Levels in Patients with Hepatocellular Carcinoma. Int. J. Mol. Sci. 2016, 17, 1032. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, K.; Rode, A.; Nicoll, A.; Villadsen, G.; Espelund, U.; Lim, L.; Angus, P.; Arachchi, N.; Vilstrup, H.; Nexo, E.; et al. Vitamin B(1)(2) and its binding proteins in hepatocellular carcinoma and chronic liver diseases. Scand. J. Gastroenterol. 2014, 49, 1096–1102. [Google Scholar] [CrossRef]
- Chang, S.C.; Goldstein, B.Y.; Mu, L.; Cai, L.; You, N.C.; He, N.; Ding, B.G.; Zhao, J.K.; Yu, S.Z.; Heber, D.; et al. Plasma folate, vitamin B12, and homocysteine and cancers of the esophagus, stomach, and liver in a Chinese population. Nutr. Cancer 2015, 67, 212–223. [Google Scholar] [CrossRef]
- Arendt, J.F.; Farkas, D.K.; Pedersen, L.; Nexo, E.; Sorensen, H.T. Elevated plasma vitamin B12 levels and cancer prognosis: A population-based cohort study. Cancer Epidemiol. 2016, 40, 158–165. [Google Scholar] [CrossRef] [Green Version]
- He, T.T.; Xiao, H.W.; Wusiman, M.; Yishake, D.; Fang, A.P.; Luo, Y.; Liu, X.Z.; Liu, Z.Y.; Zhu, H.L. Dietary intake of one-carbon metabolism-related nutrients and hepatocellular carcinoma survival in the Guangdong Liver Cancer Cohort. Food Funct. 2022, 13, 8081–8090. [Google Scholar] [CrossRef]
- Liu, G.J.; Wang, Y.J.; Yue, M.; Zhao, L.M.; Guo, Y.D.; Liu, Y.P.; Yang, H.C.; Liu, F.; Zhang, X.; Zhi, L.H.; et al. High expression of TCN1 is a negative prognostic biomarker and can predict neoadjuvant chemosensitivity of colon cancer. Sci. Rep. 2020, 10, 11951. [Google Scholar] [CrossRef]
- Gohari, M.; Moghimi, M.; Aarafi, H.; Shajari, A.; Jafari-Nedooshan, J.; Lookzadeh, M.H.; Mirjalili, S.R.; Neamatzadeh, H. Association of MTHFR 677C > T, 1298A > C and MTR 2756A > G Polymorphisms with Susceptibility to Childhood Retinoblastoma: A Systematic Review and Met-Analysis. Fetal Pediatr. Pathol. 2021, 40, 612–625. [Google Scholar] [CrossRef]
- Ma, L.M.; Yang, H.P.; Yang, X.W.; Ruan, L.H. Methionine synthase A2756G polymorphism influences pediatric acute lymphoblastic leukemia risk: A meta-analysis. Biosci. Rep. 2019, 39, BSR20181770. [Google Scholar] [CrossRef] [Green Version]
- Lu, M.; Wang, F.; Qiu, J. Methionine synthase A2756G polymorphism and breast cancer risk: A meta-analysis involving 18,953 subjects. Breast Cancer Res. Treat. 2010, 123, 213–217. [Google Scholar] [CrossRef]
- Yu, K.; Zhang, J.; Zhang, J.; Dou, C.; Gu, S.; Xie, Y.; Mao, Y.; Ji, C. Methionine synthase A2756G polymorphism and cancer risk: A meta-analysis. Eur. J. Hum. Genet. 2010, 18, 370–378. [Google Scholar] [CrossRef] [Green Version]
- Zhong, S.; Xu, J.; Li, W.; Chen, Z.; Ma, T.; Zhao, J. Methionine synthase A2756G polymorphism and breast cancer risk: An up-to-date meta-analysis. Gene 2013, 527, 510–515. [Google Scholar] [CrossRef]
- Guo, Y.; Lu, Y.; Jin, H. Appraising the role of circulating concentrations of micro-nutrients in epithelial ovarian cancer risk: A Mendelian randomization analysis. Sci. Rep. 2020, 10, 7356. [Google Scholar] [CrossRef]
- Tsilidis, K.K.; Papadimitriou, N.; Dimou, N.; Gill, D.; Lewis, S.J.; Martin, R.M.; Murphy, N.; Markozannes, G.; Zuber, V.; Cross, A.J.; et al. Genetically predicted circulating concentrations of micronutrients and risk of colorectal cancer among individuals of European descent: A Mendelian randomization study. Am. J. Clin. Nutr. 2021, 113, 1490–1502. [Google Scholar]
- Chen, J.; Stampfer, M.J.; Ma, J.; Selhub, J.; Malinow, M.R.; Hennekens, C.H.; Hunter, D.J. Influence of a methionine synthase (D919G) polymorphism on plasma homocysteine and folate levels and relation to risk of myocardial infarction. Atherosclerosis 2001, 154, 667–672. [Google Scholar] [CrossRef]
- Tsai, M.Y.; Bignell, M.; Yang, F.; Welge, B.G.; Graham, K.J.; Hanson, N.Q. Polygenic influence on plasma homocysteine: Association of two prevalent mutations, the 844ins68 of cystathionine beta-synthase and A(2756)G of methionine synthase, with lowered plasma homocysteine levels. Atherosclerosis 2000, 149, 131–137. [Google Scholar] [CrossRef]
- Zhao, L.; Wei, Y.; Song, A.; Li, Y. Association study between genome-wide significant variants of vitamin B12 metabolism and gastric cancer in a han Chinese population. IUBMB Life 2016, 68, 303–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surendran, S.; Adaikalakoteswari, A.; Saravanan, P.; Shatwaan, I.A.; Lovegrove, J.A.; Vimaleswaran, K.S. An update on vitamin B12-related gene polymorphisms and B12 status. Genes Nutr. 2018, 13, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbing, M.; Bonaa, K.H.; Nygard, O.; Arnesen, E.; Ueland, P.M.; Nordrehaug, J.E.; Rasmussen, K.; Njolstad, I.; Refsum, H.; Nilsen, D.W.; et al. Cancer incidence and mortality after treatment with folic acid and vitamin B12. JAMA 2009, 302, 2119–2126. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Manson, J.E.; Lee, I.M.; Cook, N.R.; Paul, L.; Selhub, J.; Giovannucci, E.; Zhang, S.M. Effect of combined folic acid, vitamin B(6), and vitamin B(12) on colorectal adenoma. J. Natl. Cancer Inst. 2012, 104, 1562–1575. [Google Scholar] [CrossRef] [Green Version]
- Hankey, G.J.; Eikelboom, J.W.; Yi, Q.; Lees, K.R.; Chen, C.; Xavier, D.; Navarro, J.C.; Ranawaka, U.K.; Uddin, W.; Ricci, S.; et al. Treatment with B Vitamins and Incidence of Cancer in Patients with Previous Stroke or Transient Ischemic Attack: Results of a Randomized Placebo-Controlled Trial. Stroke 2012, 43, 1572–1577. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.M.; Cook, N.R.; Albert, C.M.; Gaziano, J.M.; Buring, J.E.; Manson, J.E. Effect of combined folic acid, vitamin B6, and vitamin B12 on cancer risk in women: A randomized trial. JAMA 2008, 300, 2012–2021. [Google Scholar] [CrossRef] [Green Version]
- Oliai, A.S.; Kiefte-de Jong, J.C.; van Dijk, S.C.; Swart, K.M.A.; van Laarhoven, H.W.; van Schoor, N.M.; de Groot, L.C.P.G.; Lemmens, V.; Stricker, B.H.; Uitterlinden, A.G.; et al. Folic Acid and Vitamin B12 Supplementation and the Risk of Cancer: Long-term Follow-up of the B Vitamins for the Prevention of Osteoporotic Fractures (B-PROOF) Trial. Cancer Epidemiol. Biomarkers Prev. 2019, 28, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Clarke, R.; Halsey, J.; Lewington, S.; Lonn, E.; Armitage, J.; Manson, J.E.; Bonaa, K.H.; Spence, J.D.; Nygard, O.; Jamison, R.; et al. Effects of lowering homocysteine levels with B vitamins on cardiovascular disease, cancer, and cause-specific mortality: Meta-analysis of 8 randomized trials involving 37,485 individuals. Arch. Intern. Med 2010, 170, 1622–1631. [Google Scholar]
- Ragasudha, P.N.; Thulaseedharan, J.V.; Wesley, R.; Jayaprakash, P.G.; Lalitha, P.; Pillai, M.R. A case-control nutrigenomic study on the synergistic activity of folate and vitamin B12 in cervical cancer progression. Nutr. Cancer 2012, 64, 550–558. [Google Scholar] [CrossRef]
- Maritsi, D.N.; Vartzelis, G.; Dana, H.; Kosmidis, H.; Douna, V.; Kossiva, L. Plasma Folate, Vitamin B12 and Homocysteine Levels in Children with Solid Tumors at Diagnosis; Results from a Pediatric Referral Centre. Indian J. Pediatr. 2016, 83, 483–484. [Google Scholar] [CrossRef]
- Kharb, S.; Kumar, S.; Kundu, Z.S. Homocysteine, a biomarker of osteosarcoma. J. Cancer Res. Ther. 2015, 11, 51–53. [Google Scholar] [CrossRef]
- Wu, Y.H.; Wu, Y.C.; Chu, F.Y.; Cheng, S.J.; Sun, A.; Chen, H.M. Significantly higher frequencies of hematinic deficiencies and hyperhomocysteinemia in oral precancer patients. J. Formos. Med. Assoc. 2019, 118, 1299–1307. [Google Scholar] [CrossRef]
- Kwanbunjan, K.; Saengkar, P.; Cheeramakara, C.; Tangjitgamol, S.; Chitcharoenrung, K. Vitamin B12 status of Thai women with neoplasia of the cervix uteri. Southeast Asian J. Trop. Med. Public Health 2006, 37, 178–183. [Google Scholar]
- Ilhan, I.E.; Sari, N.; Yesil, S.; Eren, T.; Tacyildiz, N. Anthropometric and Biochemical Assessment of Nutritional Status in Pediatric Cancer Patients. Pediatr. Hematol. Oncol. 2015, 32, 415–422. [Google Scholar]
- Gorgulu, O.; Selcuk, T.; Ozdemir, S.; Sayar, C.; Beyazit, Y.; Akbas, Y. Evaluation of the roles of serum vitamin B(12), folate and homocysteine levels in laryngeal squamous cell carcinoma. J. Int. Med. Res. 2010, 38, 2047–2052. [Google Scholar] [CrossRef] [Green Version]
- Pan, D.; Wang, S.; Su, M.; Sun, G.; Zhu, X.; Ghahvechi, C.M.; Guo, Z.; Wang, N.; Zhang, Z.; Cui, M. Vitamin B12 may play a preventive role in esophageal precancerous lesions: A case-control study based on markers in blood and 3-day duplicate diet samples. Eur. J. Nutr. 2021, 60, 3375–3386. [Google Scholar] [CrossRef]
- Vollset, S.E.; Igland, J.; Jenab, M.; Fredriksen, A.; Meyer, K.; Eussen, S.; Gjessing, H.K.; Ueland, P.M.; Pera, G.; Sala, N.; et al. The association of gastric cancer risk with plasma folate, cobalamin, and methylenetetrahydrofolate reductase polymorphisms in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol. Biomark. Prev. 2007, 16, 2416–2424. [Google Scholar] [CrossRef] [Green Version]
- de Vogel, S.; Meyer, K.; Fredriksen, A.; Ulvik, A.; Ueland, P.M.; Nygard, O.; Vollset, S.E.; Tell, G.S.; Tretli, S.; Bjorge, T. Serum folate and vitamin B12 concentrations in relation to prostate cancer risk—A Norwegian population-based nested case-control study of 3000 cases and 3000 controls within the JANUS cohort. Int. J. Epidemiol. 2013, 42, 201–210. [Google Scholar] [CrossRef] [Green Version]
- Al-Ghnaniem, R.; Peters, J.; Foresti, R.; Heaton, N.; Pufulete, M. Methylation of estrogen receptor alpha and mutL homolog 1 in normal colonic mucosa: Association with folate and vitamin B-12 status in subjects with and without colorectal neoplasia. Am. J. Clin. Nutr. 2007, 86, 1064–1072. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.P.; Lin, C.C.; Chen, T.H.; Tsai, M.C.; Huang, Y.C. Higher plasma homocysteine is associated with increased risk of developing colorectal polyps. Nutr. Cancer 2013, 65, 195–201. [Google Scholar] [CrossRef]
- Johnston, J.; Bollekens, J.; Allen, R.H.; Berliner, N. Structure of the cDNA encoding transcobalamin I, a neutrophil granule protein. J. Biol. Chem. 1989, 264, 15754–15757. [Google Scholar] [CrossRef]
- Kane, S.P.; Peters, T.J. Analytical subcellular fractionation of human granulocytes with reference to the localization of vitamin B12-binding proteins. Clin. Sci. Mol. Med. 1975, 49, 171–182. [Google Scholar] [CrossRef]
- Zou, D.D.; Xu, D.; Deng, Y.Y.; Wu, W.J.; Zhang, J.; Huang, L.; He, L. Identification of key genes in cutaneous squamous cell carcinoma: A transcriptome sequencing and bioinformatics profiling study. Ann. Transl. Med. 2021, 9, 1497. [Google Scholar] [CrossRef]
- Sheppard, K.; Bradbury, D.A.; Davies, J.M.; Ryrie, D.R. Cobalamin and folate binding proteins in human tumour tissue. J. Clin. Pathol. 1984, 37, 1336–1338. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Guo, L.; Cai, Z. TCN1 is a potential prognostic biomarker and correlates with immune infiltrates in lung adenocarcinoma. World J. Surg. Oncol. 2022, 20, 83. [Google Scholar] [CrossRef]
- Wang, Y.; Yue, C.; Fang, J.; Gong, L.; Lian, M.; Wang, R.; Feng, L.; Ma, H.; Ma, Z.; Liu, H. Transcobalamin I: A novel prognostic biomarker of neoadjuvant chemotherapy in locally advanced hypopharyngeal squamous cell cancers. OncoTargets Ther. 2018, 11, 4253–4261. [Google Scholar] [CrossRef] [Green Version]
- Burger, R.L.; Waxman, S.; Gilbert, H.S.; Mehlman, C.S.; Allen, R.H. Isolation and characterization of a novel vitamin B12-binding protein associated with hepatocellular carcinoma. J. Clin. Investig. 1975, 56, 1262–1270. [Google Scholar] [CrossRef]
- Wang, J.; Hossain, M.; Thanabalasuriar, A.; Gunzer, M.; Meininger, C.; Kubes, P. Visualizing the function and fate of neutrophils in sterile injury and repair. Science 2017, 358, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liew, P.X.; Kubes, P. The Neutrophil’s Role During Health and Disease. Physiol. Rev. 2019, 99, 1223–1248. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, J. Intravital Imaging of Inflammatory Response in Liver Disease. Front. Cell Dev. Biol. 2022, 10, 922041. [Google Scholar] [CrossRef]
- Zhu, X.; Yi, K.; Hou, D.; Huang, H.; Jiang, X.; Shi, X.; Xing, C. Clinicopathological Analysis and Prognostic Assessment of Transcobalamin I (TCN1) in Patients with Colorectal Tumors. Med. Sci. Monit. 2020, 26, e923828. [Google Scholar] [CrossRef] [PubMed]
- Carmel, R.; Hollander, D. Extreme elevation of transcobalamin II levels in multiple myeloma and other disorders. Blood 1978, 51, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Collin, S.M. Folate and B12 in prostate cancer. Adv. Clin. Chem. 2013, 60, 1–63. [Google Scholar]
- Lo-Bisgaard, T.; Espelund, U.; Frystyk, J.; Rasmussen, T.R.; Nexo, E.; Arendt, J.F.H. Vitamin B12 and its binding proteins in patients with non-small cell lung cancer referred to fast-track diagnostic work-up for lung cancer. Scand. J. Clin. Lab. Investig. 2020, 80, 14–19. [Google Scholar] [CrossRef]
- Lacombe, V.; Patsouris, A.; Delattre, E.; Lacout, C.; Urbanski, G. Evolution of plasma vitamin B12 in patients with solid cancers during curative versus supportive care. Arch Med. Sci. 2021, 17, 1811–1815. [Google Scholar] [CrossRef]
- Waibel, R.; Treichler, H.; Schaefer, N.G.; van Staveren, D.R.; Mundwiler, S.; Kunze, S.; Kuenzi, M.; Alberto, R.; Nuesch, J.; Knuth, A.; et al. New derivatives of vitamin B12 show preferential targeting of tumors. Cancer Res. 2008, 68, 2904–2911. [Google Scholar] [CrossRef] [Green Version]
- Collins, D.A.; Hogenkamp, H.P.; O’Connor, M.K.; Naylor, S.; Benson, L.M.; Hardyman, T.J.; Thorson, L.M. Biodistribution of radiolabeled adenosylcobalamin in patients diagnosed with various malignancies. Mayo Clin. Proc. 2000, 75, 568–580. [Google Scholar] [CrossRef]
- Piyathilake, C.J.; Macaluso, M.; Alvarez, R.D.; Bell, W.C.; Heimburger, D.C.; Partridge, E.E. Lower risk of cervical intraepithelial neoplasia in women with high plasma folate and sufficient vitamin B12 in the post-folic acid fortification era. Cancer Prev. Res. 2009, 2, 658–664. [Google Scholar] [CrossRef] [Green Version]
- Hatami, M.; Vahid, F.; Esmaeil, A.M.; Sadeghi, M.; Ameri, F.; Eini-Zeinab, H.; Jamshidi-Naeini, Y.; Hossein, D.S. The Vitamins Involved in One-Carbon Metabolisms are Associated with Reduced Risk of Breast Cancer in Overall and Subtypes. Int. J. Vitam. Nutr. Res. 2020, 90, 131–140. [Google Scholar] [CrossRef]
- Boot, I.W.A.; Wesselius, A.; Yu, E.Y.W.; Brinkman, M.; van den Brandt, P.; Grant, E.J.; White, E.; Weiderpass, E.; Ferrari, P.; Schulze, M.B.; et al. Dietary B group vitamin intake and the bladder cancer risk: A pooled analysis of prospective cohort studies. Eur. J. Nutr. 2022, 61, 2397–2416. [Google Scholar] [CrossRef]
- Marley, A.R.; Fan, H.; Hoyt, M.L.; Anderson, K.E.; Zhang, J. Intake of methyl-related nutrients and risk of pancreatic cancer in a population-based case-control study in Minnesota. Eur. J. Clin. Nutr. 2018, 72, 1128–1135. [Google Scholar] [CrossRef]
- Jessri, M.; Rashidkhani, B.; Hajizadeh, B.; Jessri, M.; Gotay, C. Macronutrients, vitamins and minerals intake and risk of esophageal squamous cell carcinoma: A case-control study in Iran. Nutr. J. 2011, 10, 137. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Q.; Freedman, N.D.; Ren, J.; Hollenbeck, A.R.; Abnet, C.C.; Park, Y. Intakes of folate, methionine, vitamin B6, and vitamin B12 with risk of esophageal and gastric cancer in a large cohort study. Br. J. Cancer 2014, 110, 1328–1333. [Google Scholar] [CrossRef]
- Ibiebele, T.I.; Hughes, M.C.; Pandeya, N.; Zhao, Z.; Montgomery, G.; Hayward, N.; Green, A.C.; Whiteman, D.C.; Webb, P.M. High intake of folate from food sources is associated with reduced risk of esophageal cancer in an Australian population. J. Nutr. 2011, 141, 274–283. [Google Scholar]



{kind=link}
{kind=link}
| Study, Design | Exposure/Outcome | High B12 vs. Reference Category | Results Summary | Adjustments/Limitations |
|---|---|---|---|---|
| Lin et al., 2010 [7], Case-control | P-B12 (and B12 intake) in relation to survival in patients with hepatocellular carcinoma 90 cases and 90 controls, “Taiwan” | Tertile T1 < 699 ng/L * = reference T2; 699–1500 ng/L T3; >1500 ng/L B12 > 699 (cut-off) vs. < 699 ng/L B12 intake did not differ by tertiles of plasma B12: in T1 2.8 ± 2.0 µg/d; in T2 2.6 ± 2.0 µg/d; in T3 2.4 ± 1.5 µg/d | HR (95%CI) of survival 2.95 (1.22–7.11) 3.24 (0.99–10.60) 2.88 (1.26–6.60) B12 intake: 3.0 ± 5.7 μg/d in patients vs. 4.3 ± 8.3 μg/d in the age and sex matched controls. | Adjustments not clear for what. High B12 associated with low albumin, hemoglobin, erythrocytes count, and alanina amino transferase, but with high alpha-fetal protein and tumor size. High B12 concentrations associated with malnourishment, liver injuries, and tumor progression. |
| Cui et al., 2016 [8], Case-control | P-B12 among 312 patients with hepatic cancer and 325 controls “China” | lowest Q1 (227–265) = reference Q2 (266–406) Q3 (407–589) Q4 (590–1478) pmol/L | OR (95%CI) for liver cancer 1.43 (0.72–2.81) 0.63 (0.31–1.25) 2.01 (1.02–3.98) | Adjusted for age, sex, smoking, and Hepatitis B surface antigen. Small sample size and uncontrolled confounders. Higher proportion of patients with hepatic cancer had low B12 concentrations than in the controls. |
| Simonsen et al., 2014 [9], Case-control | P-B12 in 120 hepatic cancers and 46 controls and 102 patients with chronic liver diseases “Denmarkand Australia” | Median (range) of p-B12 = 500 (120–1480) pmol/L in patients with liver cancer vs. 330 (140–800) pmol/L in the controls | P < 0.001 | Also TCN1 was elevated in plasma of patients with chronic liver diseases and those with liver cancer. |
| Chang et al., 2015 [10], Case-control | P-B12 in 204 cases with liver cancer and 415 controls “China” | p-B12, pmol/L Q1 (<154) = reference Q2 (154–229) Q3 (229–324) Q4 (>324) | OR (95%CI) = 1.00 1.37 (0.59–3.16) 4.27 (2.00–9.10) 9.90 (4.80–20.44) | Adjusted for age, sex, BMI, education, smoking, H.Pylori (in stomach cancer), Hepatitis B infection and aflatoxin (in liver cancer), and other micronutrients. Found positive association between p-B12 and esophagus, stomach cancer for the Q4 vs. Q1. But the association with liver cancer was stronger. |
| Arendt et al., 2016 [11], Cohort | P-B12 measured in the previous year/30-day mortality post diagnosis. 327 liver cancers were identified in health registers data of B12 measurements “Denmark” | < 200 pmol/L excluded 200–600 pmol/L = reference 601–800 pmol/L > 800 pmol/L | mortality risk ratio 1.0 1.2 (0.6–2.5) 3.0 (1.7–5.3) | Adjusted for age, sex, calendar year, Charlson comorbidity score index, and cancer stage. Analyzing the data by cancer type do not consistently support that the mortality is higher in patients with high B12. Excluded all B12 levels < 200 pmol/L, possible confounding by indication, and underreported supplements. |
| He et al., 2022 [12], Cohort | B12 intake in relation to mortality among 905 newly diagnosed hepatic cancer patients were recruited in the Guangdong Liver Cancer Cohort “China” | Median (P25, P75) of B12 intake, µg/d Q1 0.4 (0.1, 0.7) = reference Q2 1.1 (1.0, 1.2) Q3 1.6 (1.5, 1.8) Q4 2.8 (2.3, 4.3) | Median B12 (IQR) intake in 12 months pre diagnosis of cancer 1.3 (0.9, 2.0) μg/d. HR (95% CI) for all-cause and hepatic cancer-specific mortality during the follow up of 791 days according to intake quartiles 1.04 (0.76–1.42) 0.86 (0.61–1.20) 0.83 (0.61–1.13) For hepatic cancer specific mortality 1.04 (0.76–1.42) 0.86 (0.61–1.20) 0.83 (0.61–1.13) | Adjusted for sex, age, BMI, energy intake, physical activity, and education level, smoking, alcohol drinking, presence of chronic diseases (hypertension, diabetes, dyslipidemia, fatty liver disease, and cirrhosis), Barcelona Clinic Liver Cancer stage (0, A, B, C), and treatment (surgery, other treatments). |
| Criteria | Results | Criteria Fulfillment |
|---|---|---|
| Strength of association | The strength of the associations varied between studies on the same type of cancer (except for liver cancer) and between types of cancer. In general, the association appears to be confounded by the tumor size, stage of cancer at diagnosis, and general health condition of the patients [7]. Adjustments for confounders were performed in some, but not all studies. The adjustments were sometimes insufficient (i.e., [31]). Residual confounding is very likely. | Not fulfilled |
| Consistency | The direction of the association was not consistent across all studies and all types of cancer. Additionally, low B12 was associated with cancer [32,33,34,35,36,37] and high B12 was associated with lower risk of cancer [38,39]. In studies reporting plasma B12 and MMA, or B12 and holoTC [38,39,40], the results of non-significant association or protective association with B12 were confirmed by MMA and holoTC. Studies on vitamin B12 intake as an exposure variable were also not consistent and did not support that high plasma B12 in some cancers could be due to high B12 intake. The majority of the studies on B12 concentrations or intake found non-significant associations. Nevertheless, high plasma B12 showed consistent association only with liver cancer (Table 1). This inconsistency strongly suggests that vitamin B12 itself (i.e., its role as a cofactor in one carbon metabolism and mitochondrial metabolism) is not the explanation or the cause of cancer progression. A U-shape association (high risk of cancer at low and high plasma B12) is also not supported by the results of this search. | Not fulfilled, except for liver cancer |
| Specificity | High plasma B12 concentration is not specific for cancers. All disorders (other than cancer) that affect the liver cause high concentrations of vitamin B12 in plasma [9]. Thus, high plasma B12 is the result of tissue and cell damage secondary to cancer or other disorders that damage the cells. | Not fulfilled |
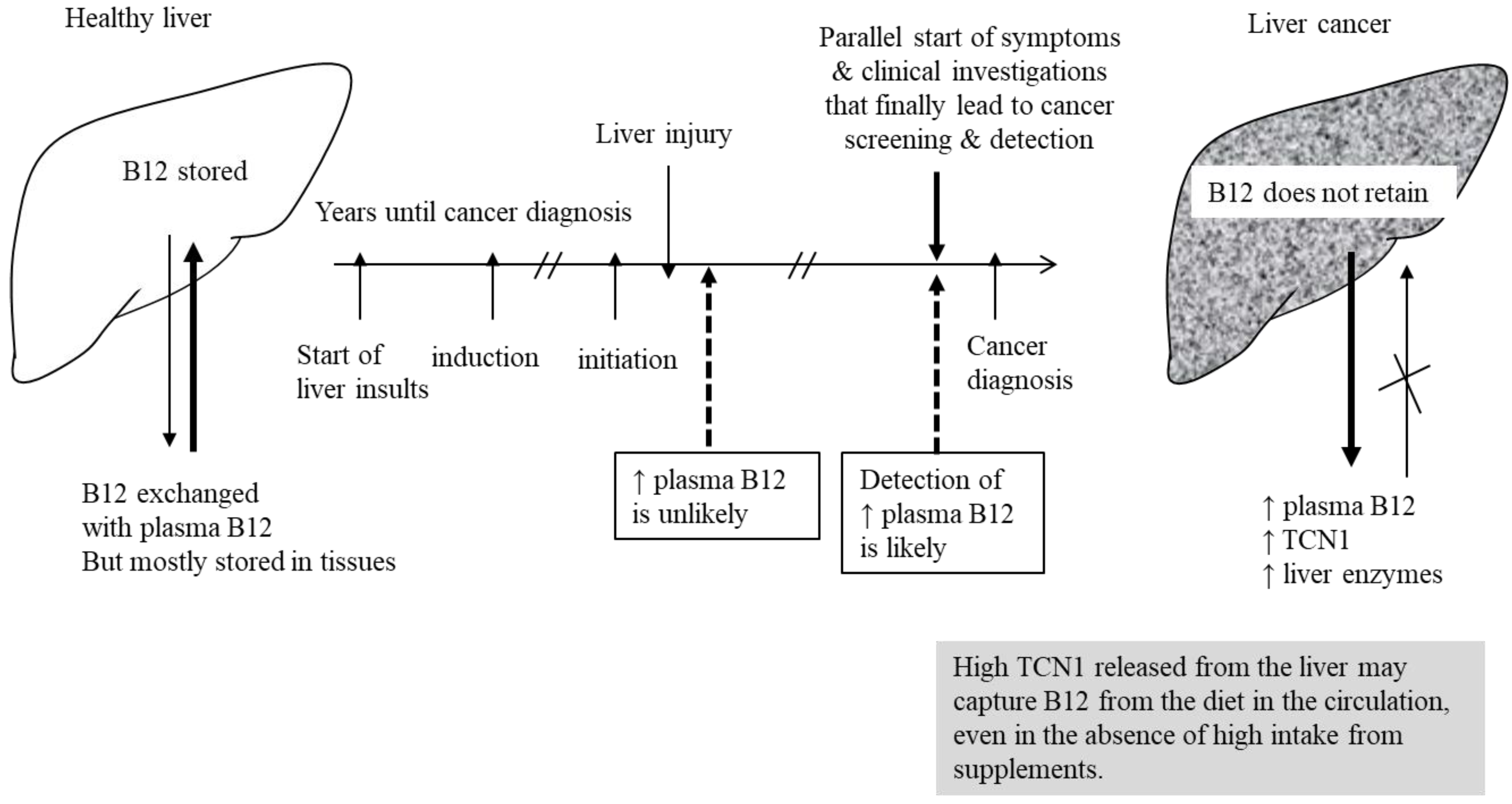
| Temporality | Early stages of cancer (i.e., hyperplastic polyps [41,42] were not associated with high plasma B12 concentrations. If high plasma B12 is not present early enough in the course of cancer, it is not plausible that B12 can have a role in tumor progression (the cause must precede the effect in a due time). The health register studies consistently showing that plasma B12 concentrations in the year before cancer diagnosis is associated with higher mortality are subject to bias (Figure S3). | Not fulfilled |
| Biological gradient | We found no evidence of a threshold for the association between high plasma B12 or B12 intake and cancer. The threshold associated with high risk was rarely in the supraphysiological blood range, but often in the range needed for physiological body functions, which is not biologically meaningful if plasma B12 would be a risk or a safety marker. Several studies have used data-driven cut-off (i.e., quartiles or quintiles). Many of these studies reported positive associations between plasma B12 and the OR or RR of cancer within the population reference range of plasma B12. On the other hand, there could be underestimation of supplement use in observational studies making the associations subject to confounding by underreported intake. Most studies that showed positive associations between high plasma B12 or B12 intake and cancer did not show a dose-response association. | Not fulfilled |
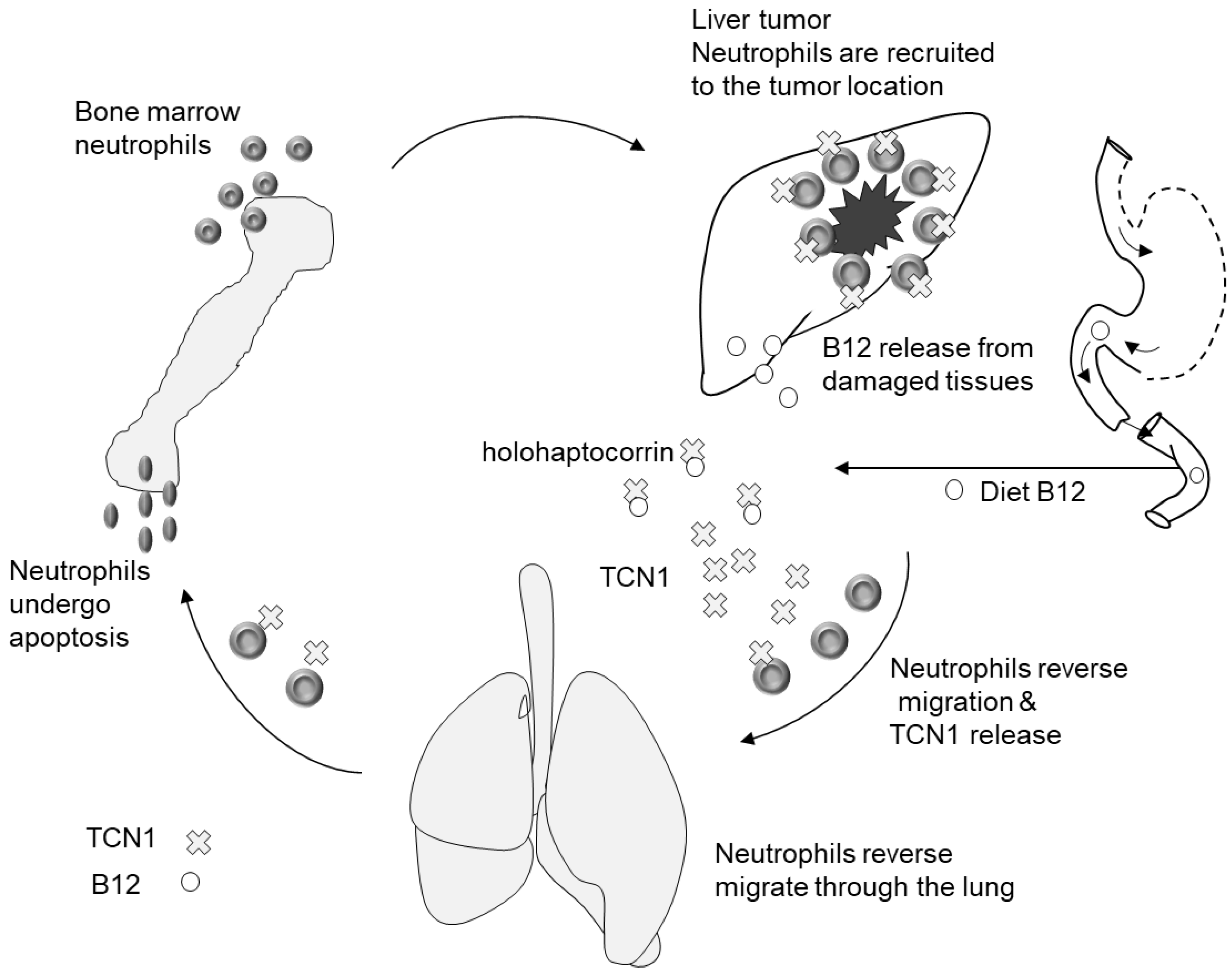
| Plausibility | High plasma B12 was argued to play a role in cancer progression due to its role as a cofactor in one carbon metabolism or in the mitochondria. However, from the studies presented here, we found no support for a causal role of B12 in promoting cancer growth or death due to cancer. In addition, elevated MMA (i.e., a marker of B12 deficiency) has been linked to cancer progression [2]. When B12 is high (thus MMA is low), we would expect low MMA to be associated with cancer. But this was not the case in the studies reviewed here. TCN1 has been shown in several studies to be overexpressed in cancer tissues [13]. TCN1 carries B12 in plasma but is not responsible for delivering B12 into the cells, thus it is in theory possible that high expression of TCN1 is causing high plasma B12, while intracellular B12 is not elevated. The more likely explanation is that raised plasma B12 is caused by cancer (among other systemic disorders) and not vice versa. | Not fulfilled |
| Coherence | We focused on the literature since 2005. Since the early reports on the association between elevated plasma B12 and cancer, there have been many negative studies. The theory of elevated plasma B12 being causally related to cancer progression is not comprehensive regarding various aspects of the exposure-to-disease paradigm. | Not fulfilled |
| Experimental evidence | RCTs with B12 alone are not available. RCTs with multivitamins were not designed to answer the question and were un-blinded in one trial [29] after the intervention and before studying the outcome of cancer. | No evidence (RCTs) |
| Analogy | If high plasma B12 would cause cancer, then factors that increase plasma B12 would also cause cancer. This is a rather weak criterion and cannot be definitely judged in case of B12. For example, all liver damaging diseases would increase B12 and are risk factors of cancer in the same time. But they are better judged as confounders. Additionally, high B12 intake that is usually associated with higher plasma level showed even less convincing association with cancer, suggesting no analogy. | Not clear/Not fulfilled |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obeid, R. High Plasma Vitamin B12 and Cancer in Human Studies: A Scoping Review to Judge Causality and Alternative Explanations. Nutrients 2022, 14, 4476. https://doi.org/10.3390/nu14214476
Obeid R. High Plasma Vitamin B12 and Cancer in Human Studies: A Scoping Review to Judge Causality and Alternative Explanations. Nutrients. 2022; 14(21):4476. https://doi.org/10.3390/nu14214476
Chicago/Turabian StyleObeid, Rima. 2022. "High Plasma Vitamin B12 and Cancer in Human Studies: A Scoping Review to Judge Causality and Alternative Explanations" Nutrients 14, no. 21: 4476. https://doi.org/10.3390/nu14214476
APA StyleObeid, R. (2022). High Plasma Vitamin B12 and Cancer in Human Studies: A Scoping Review to Judge Causality and Alternative Explanations. Nutrients, 14(21), 4476. https://doi.org/10.3390/nu14214476