

Effect of Fortified Formula on Growth and Nutritional Status in Young Children: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
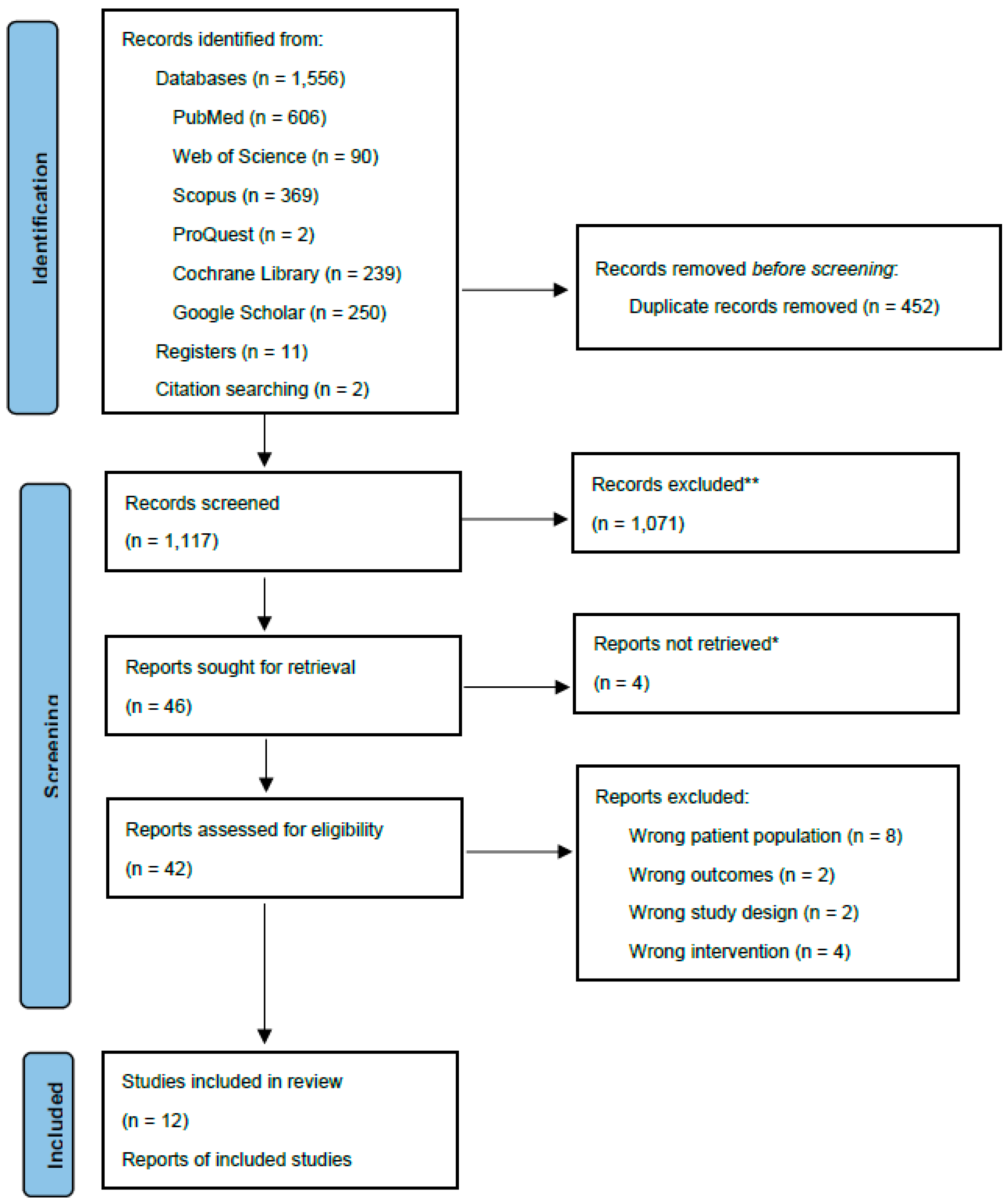
2.1. Information Sources and Search Strategy
2.2. Study Eligibility Criteria
- Population was apparently-healthy children aged between 9 and 48 months at recruitment;
- intervention group received fortified milk or formula;
- comparison group received non-fortified milk or formula;
- outcomes included growth parameters and/or biochemical markers; and
- studies were randomised controlled trials (RCT).
2.3. Study Selection and Data Extraction
2.4. Data Synthesis
2.5. Study Quality Appraisal
2.6. Statistical Analysis
2.6.1. Sensitivity Analyses
2.6.2. Subgroup Analyses
3. Results
3.1. Study Characteristics
3.2. Effect of Formula on Infant Growth and Body Composition
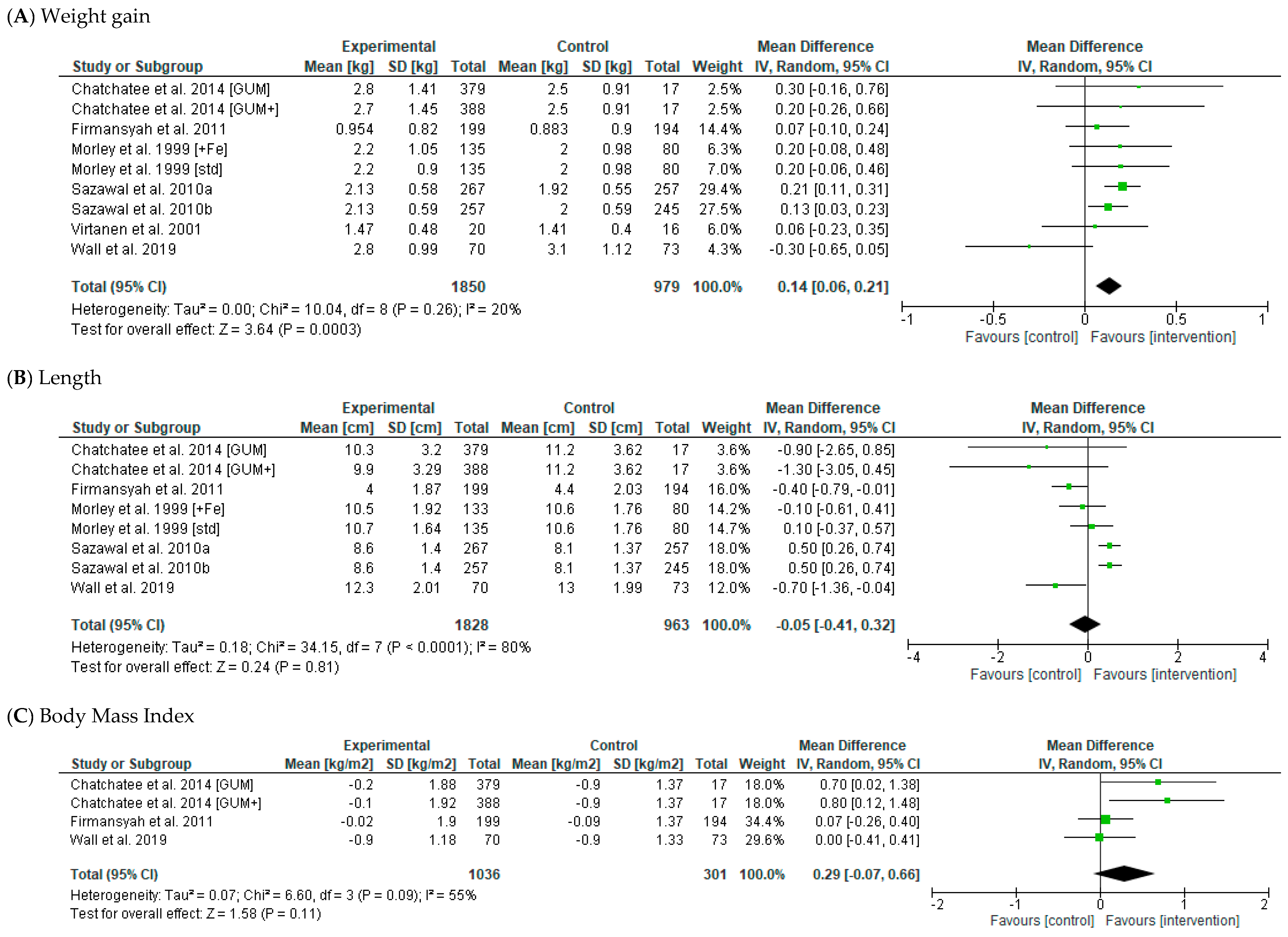
3.2.1. Anthropometric Outcomes
3.2.2. Body Composition Outcomes
3.3. Effect of Formula on Biochemical Outcomes
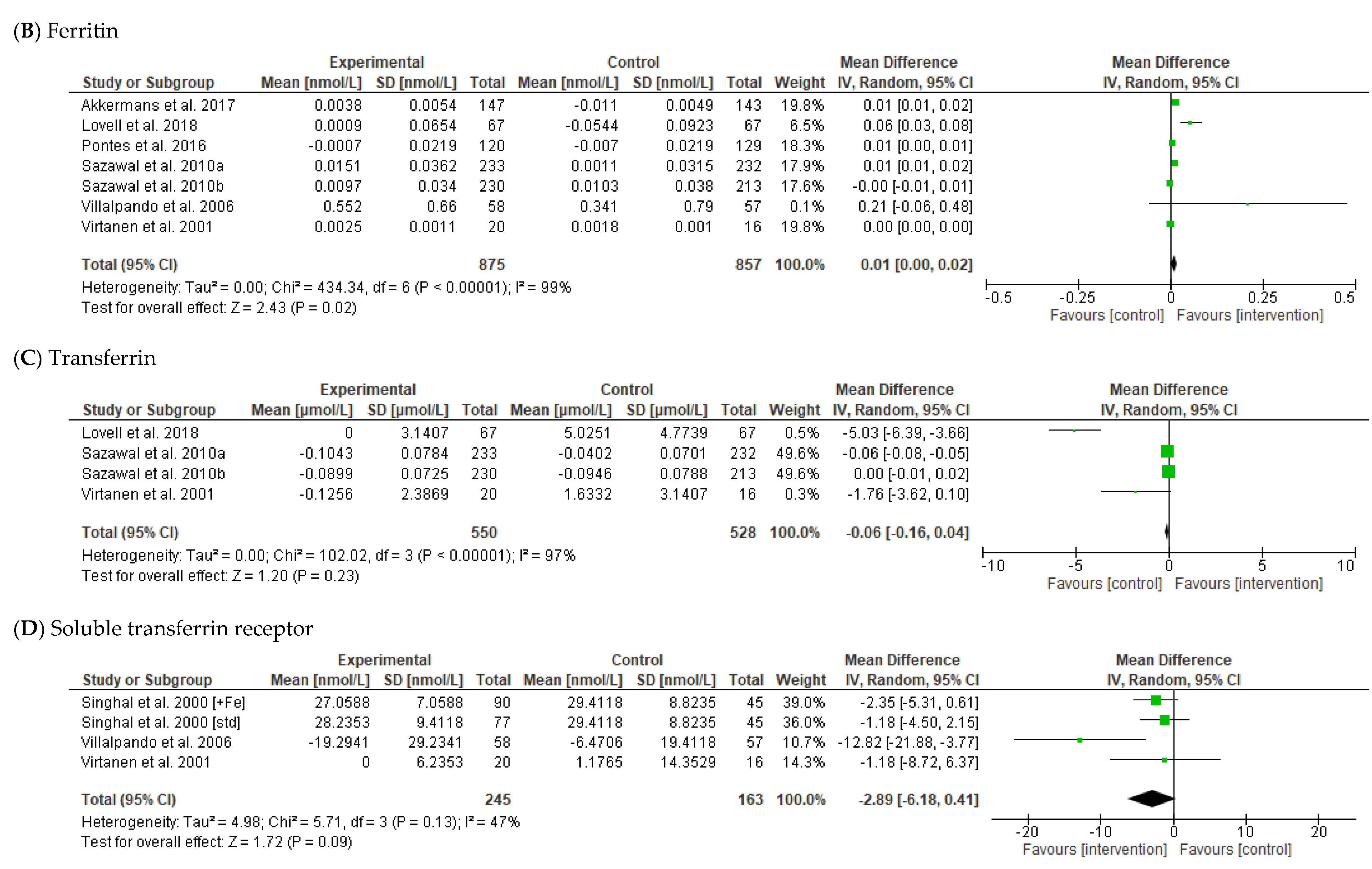
3.3.1. Iron
3.3.2. Other Biochemical Markers
3.4. Dietary Intake
3.5. Sensitivity Analyses
3.6. Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Organisation for Economic Co-operation and Development (OECD) and World Health Organization. Health at a Glance: Asia/Pacific2020; OECD: Paris, France, 2020. [Google Scholar]
- World Health Organization. Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- National Health and Medical Research Council. Eat for Health Infant Feeding Guidelines Summary; Department of Health and Ageing, Ed.; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- World Health Organization. Healthy Diet 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 8 September 2022).
- Csölle, I.; Felső, R.; Szabó, É.; Metzendorf, M.-I.; Schwingshackl, L.; Ferenci, T.; Lohner, S. Health outcomes associated with micronutrient-fortified complementary foods in infants and young children aged 6–23 months: A systematic review and meta-analysis. Lancet Child Adolesc. Health 2022, 6, 533–544. [Google Scholar] [CrossRef]
- Atkins, L.A.; McNaughton, S.A.; Campbell, K.J.; Szymlek-Gay, E.A. Iron intakes of Australian infants and toddlers: Findings from the Melbourne Infant Feeding, Activity and Nutrition Trial (InFANT) Program. Br. J. Nutr. 2016, 115, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Roess, A.A.; Jacquier, E.F.; Catellier, D.J.; Carvalho, R.; Lutes, A.C.; Anater, A.S.; Dietz, W.H. Food Consumption Patterns of Infants and Toddlers: Findings from the Feeding Infants and Toddlers Study (FITS) 2016. J. Nutr. 2018, 148, 1525S–1535S. [Google Scholar] [CrossRef] [Green Version]
- Jun, S.; Catellier, D.J.; Eldridge, A.L.; Dwyer, J.T.; Eicher-Miller, H.A.; Bailey, R.L. Usual Nutrient Intakes from the Diets of US Children by WIC Participation and Income: Findings from the Feeding Infants and Toddlers Study (FITS) 2016. J. Nutr. 2018, 148, 1567S–1574S. [Google Scholar] [CrossRef] [Green Version]
- Byrne, R.; Zhou, Y.; Perry, R.; Mauch, C.; Magarey, A. Beverage intake of Australian children and relationship with intake of fruit, vegetables, milk and body weight at 2, 3.7 and 5 years of age. Nutr. Diet. 2018, 75, 159–166. [Google Scholar] [CrossRef]
- Marr, C.; Breeze, P.; Caton, S.J. Examination of dietary intake of UK preschool children by varying carers: Evidence from the 2008–2016 UK National Diet and Nutrition Survey. Br. J. Nutr. 2021, 128, 1–12. [Google Scholar] [CrossRef]
- Scott, J.A.; Gee, G.; Devenish, G.; Ha, D.; Do, L. Determinants and Sources of Iron Intakes of Australian Toddlers: Findings from the SMILE Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 181. [Google Scholar] [CrossRef] [Green Version]
- Moumin, N.A.; Netting, M.J.; Golley, R.K.; Mauch, C.E.; Makrides, M.; Green, T.J. Does Food Intake of Australian Toddlers 12–24 Months Align with Recommendations: Findings from the Australian Feeding Infants and Toddlers Study (OzFITS) 2021. Nutrients 2022, 14, 2890. [Google Scholar] [CrossRef]
- Gedfie, S.; Getawa, S.; Melku, M. Prevalence and Associated Factors of Iron Deficiency and Iron Deficiency Anemia Among Under-5 Children: A Systematic Review and Meta-Analysis. Glob. Pediatr. Health 2022, 9, 2333794X221110860. [Google Scholar] [CrossRef]
- United Nations Children’s Fund, World Health Organization, World Bank Group. Levels and Trends in Child Malnutrition: UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates: Key Findings of the 2021 Edition; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Obesity and Overweight. Available online: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 16 July 2021).
- World Health Organisation. Children: Improving Survival and Well-Being. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 8 September 2022).
- Matsuyama, M.; Harb, T.; David, M.; Davies, P.S.; Hill, R.J. Effect of fortified milk on growth and nutritional status in young children: A systematic review and meta-analysis. Public Health Nutr. 2016, 20, 1214–1225. [Google Scholar] [CrossRef]
- Lippman, H.E.; Desjeux, J.-F.; Ding, Z.-Y.; Tontisirin, K.; Uauy, R.; Pedro, R.A.; Van Dael, P. Nutrient Recommendations for Growing-up Milk: A Report of an Expert Panel. Crit. Rev. Food Sci. Nutr. 2013, 56, 141–145. [Google Scholar] [CrossRef]
- Hojsak, I.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hulst, J.; Indrio, F.; Lapillonne, A.; Mølgaard, C.; et al. Young Child Formula: A Position Paper by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 177–185. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Ronne, N.D.; Sompel, A.V.D. A Belgian consensus-statement on growing-up milks for children 12–36 months old. Eur. J. Pediatr. 2014, 173, 1365–1371. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; University of York: York, UK, 2006. [Google Scholar]
- EndNote x9 [Computer Software]. Clarivate. 2018. Available online: https://support.clarivate.com/Endnote/s/article/Citing-the-EndNote-program-as-a-reference?language=en_US (accessed on 14 July 2022).
- Covidence-Better Systematic Review Management. 2022. Available online: www.covidence.org (accessed on 14 July 2022).
- Review Manager (RevMan), version 5.4; The Cochrane Collaboration: London, UK, 2020.
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane. 2022. Available online: www.training.cochrane.org/handbook (accessed on 7 September 2022).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Firmansyah, A.; Dwipoerwantoro, P.G.; Kadim, M.; Alatas, S.; Conus, N.; Lestarina, L.; Bouisset, F.; Steenhout, P. Improved growth of toddlers fed a milk containing synbiotics. Asia Pac. J. Clin. Nutr. 2011, 20, 69–76. [Google Scholar]
- Morley, R.; Abbott, R.; Fairweather-Tait, S.; MacFadyen, U.; Stephenson, T.; Lucas, A. Iron fortified follow on formula from 9 to 18 months improves iron status but not development or growth: A randomised trial. Arch. Dis. Child. 1999, 81, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Wall, C.R.; Hill, R.J.; Lovell, A.L.; Matsuyama, M.; Milne, T.; Grant, C.C.; Jiang, Y.; Chen, R.X.; Wouldes, T.A.; Davies, P.S. A multicenter, double-blind, randomized, placebo-controlled trial to evaluate the effect of consuming Growing Up Milk “Lite” on body composition in children aged 12-23 mo. Am. J. Clin. Nutr. 2019, 109, 576–585. [Google Scholar] [CrossRef]
- Lovell, A.L.; Davies, P.S.W.; Hill, R.J.; Milne, T.; Matsuyama, M.; Jiang, Y.; Chen, R.X.; Wouldes, T.A.; Heath, A.-L.M.; Grant, C.C.; et al. Compared with Cow Milk, a Growing-Up Milk Increases Vitamin D and Iron Status in Healthy Children at 2 Years of Age: The Growing-Up Milk-Lite (GUMLi) Randomized Controlled Trial. J. Nutr. 2018, 148, 1570–1579. [Google Scholar] [CrossRef] [Green Version]
- Chatchatee, P.; Lee, W.S.; Carrilho, E.; Kosuwon, P.; Simakachorn, N.; Yavuz, Y.; Schouten, B.; Graaff, P.L.-D.; Szajewska, H. Effects of Growing-Up Milk Supplemented with Prebiotics and LCPUFAs on Infections in Young Children. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 428–437. [Google Scholar] [CrossRef] [Green Version]
- Akkermans, M.D.; Eussen, S.R.; van der Horst-Graat, J.M.; van Elburg, R.M.; van Goudoever, J.B.; Brus, F. A micronutrient-fortified young-child formula improves the iron and vitamin D status of healthy young European children: A randomized, double-blind controlled trial. Am. J. Clin. Nutr. 2017, 105, 391–399. [Google Scholar] [CrossRef]
- Virtanen, M.A.; Svahn, C.J.E.; Viinikka, L.U.; Räihä, N.C.R.; Siimes, M.A.; Axelsson, I.E.M. Iron-fortified and unfortified cow’s milk: Effects on iron intakes and iron status in young children. Acta Paediatr. 2001, 90, 724–731. [Google Scholar] [CrossRef]
- Sazawal, S.; Dhingra, U.; Dhingra, P.; Hiremath, G.; Sarkar, A.; Dutta, A.; Menon, V.P.; Black, R.E. Micronutrient fortified milk improves iron status, anemia and growth among children 1-4 years: A double masked, randomized, controlled trial. PLoS ONE 2010, 5, e12167. [Google Scholar] [CrossRef] [Green Version]
- Sazawal, S.; Dhingra, U.; Hiremath, G.; Sarkar, A.; Dhingra, P.; Dutta, A.; Menon, V.P.; Black, R. Effects of Bifidobacterium lactis HN019 and Prebiotic Oligosaccharide Added to Milk on Iron Status, Anemia, and Growth Among Children 1 to 4 Years Old. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 341–346. [Google Scholar] [CrossRef]
- Villalpando, S.; Shamah, T.; Rivera, J.A.; Lara, Y.; Monterrubio, E. Fortifying milk with ferrous gluconate and zinc oxide in a public nutrition program reduced the prevalence of anemia in toddlers. J. Nutr. 2006, 136, 2633–2637. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Schroll, J.B.; Moustgaard, R.; Gøtzsche, P.C. Dealing with substantial heterogeneity in Cochrane reviews. Cross-sectional study. BMC Med. Res. Methodol. 2011, 11, 22. [Google Scholar] [CrossRef] [Green Version]
- von Hippel, P.T. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [Green Version]
- Pontes, M.V.; Ribeiro, T.C.M.; Ribeiro, H.; de Mattos, A.P.; Almeida, I.R.; Leal, V.M.; Cabral, G.N.; Stolz, S.; Zhuang, W.; Scalabrin, D.M.F. Cow’s milk-based beverage consumption in 1- to 4-year-olds and allergic manifestations: An RCT. Nutr. J. 2015, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Rivera, J.A.; Shamah, T.; Villalpando, S.; Monterrubio, E. Effectiveness of a large-scale iron-fortified milk distribution program on anemia and iron deficiency in low-income young children in Mexico. Am. J. Clin. Nutr. 2009, 91, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Szymlek-Gay, E.A.; Ferguson, E.L.; Heath, A.-L.M.; Gray, A.R.; Gibson, R.S. Food-based strategies improve iron status in toddlers: A randomized controlled trial. Am. J. Clin. Nutr. 2009, 90, 1541–1551. [Google Scholar] [CrossRef]
- Lovell, A.L.; Davies, P.S.W.; Hill, R.J.; Milne, T.; Matsuyama, M.; Jiang, Y.; Chen, R.X.; Grant, C.C.; Wall, C.R. A comparison of the effect of a Growing Up Milk-Lite (GUMLi) v. cows’ milk on longitudinal dietary patterns and nutrient intakes in children aged 12-23 months: The GUMLi randomised controlled trial. Br. J. Nutr. 2019, 121, 678–687. [Google Scholar] [CrossRef]
- Lovell, A.L.; Milne, T.; Matsuyama, M.; Hill, R.J.; Davies, P.S.W.; Grant, C.C.; Wall, C.R. Protein Intake, IGF-1 Concentrations, and Growth in the Second Year of Life in Children Receiving Growing Up Milk-Lite (GUMLi) or Cow’s Milk (CM) Intervention. Front Nutr. 2021, 8, 666228. [Google Scholar] [CrossRef]
- Singhal, A.; Morley, R.; Abbott, R.; Fairweather-Tait, S.; Stephenson, T.; Lucas, A. Clinical Safety of Iron-Fortified Formulas. Pediatrics 2000, 105, e38. [Google Scholar] [CrossRef] [Green Version]
- Morgan, E.J.; Heath, A.-L.M.; Szymlek-Gay, E.A.; Gibson, R.S.; Gray, A.R.; Bailey, K.B.; Ferguson, E.L. Red Meat and a Fortified Manufactured Toddler Milk Drink Increase Dietary Zinc Intakes without Affecting Zinc Status of New Zealand Toddlers. J. Nutr. 2010, 140, 2221–2226. [Google Scholar] [CrossRef] [Green Version]
- Houghton, L.A.; Gray, A.R.; Szymlek-Gay, E.A.; Heath, A.-L.M.; Ferguson, E.L. Vitamin D-Fortified Milk Achieves the Targeted Serum 25-Hydroxyvitamin D Concentration without Affecting That of Parathyroid Hormone in New Zealand Toddlers. J. Nutr. 2011, 141, 1840–1846. [Google Scholar] [CrossRef] [Green Version]
- Szymlek-Gay, E.A.; Gray, A.R.; Heath, A.-L.M.; Ferguson, E.L.; Edwards, T.; Skeaff, S.A. Iodine-fortified toddler milk improves dietary iodine intakes and iodine status in toddlers: A randomised controlled trial. Eur. J. Nutr. 2019, 59, 909–919. [Google Scholar] [CrossRef]
- Terrin, N.; Schmid, C.H.; Lau, J. In an empirical evaluation of the funnel plot, researchers could not visually identify publication bias. J. Clin. Epidemiol. 2005, 58, 894–901. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. WHO Child Growth Standards: Weight-for-Age BOYS. Birth to 2 years (z-Scores). Available online: https://cdn.who.int/media/docs/default-source/child-growth/child-growth-standards/indicators/weight-for-age/cht-wfa-boys-z-0-2.pdf?sfvrsn=e5bfbbee_12 (accessed on 8 September 2022).
- World Health Organisation. WHO Child Growth Standards: Weight-for-Age GIRLS. Birth to 2 Years (z-Scores). Available online: https://cdn.who.int/media/docs/default-source/child-growth/child-growth-standards/indicators/weight-for-age/cht-wfa-girls-z-0-2.pdf?sfvrsn=d6ab1ab8_14 (accessed on 8 September 2022).
- Mennella, J.; Smethers, A.; Decker, J.; Delahanty, M.; Stallings, V.; Trabulsi, J.C. Effects of Early Weight Gain Velocity Diet Quality Snack Food Access on Toddler Weight Status at 1.5 Years: Follow-Up of a Randomized Controlled Infant Formula, Trial. Nutrients 2021, 13, 3946. [Google Scholar] [CrossRef]
- Joint Statement by the World Health Organization tWFP, and the United Nations Children’s Fund. Preventing and Controlling Micronutrient Deficiencies in Populations Affected by an Emergency: Multiple Vitamin and Mineral Supplements for Pregnant and Lactating Women, and for Children Aged 6 to 59 Months: World Health Organization. 2006. Available online: https://www.who.int/publications/m/item/WHO-WFP-UNICEF-statement-micronutrients-deficiencies-emergency#:~:text=More%20than%202%20billion%20people,in%20more%20than%20one%20micronutrient (accessed on 8 September 2022).
- Soh, P.; Ferguson, E.L.; McKenzie, J.; Homs, M.Y.V.; Gibson, R.S. Iron deficiency and risk factors for lower iron stores in 6–24-month-old New Zealanders. Eur. J. Clin. Nutr. 2003, 58, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Soh, P.; Ferguson, E.L.; McKenzie, J.E.; Skeaff, S.; Parnell, W.; Gibson, R.S. Dietary intakes of 6–24-month-old urban South Island New Zealand children in relation to biochemical iron status. Public Health Nutr. 2002, 5, 339–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butte, N.F.; Fox, M.K.; Briefel, R.R.; Siega-Riz, A.M.; Dwyer, J.T.; Deming, D.M.; Reidy, K.C. Nutrient Intakes of US Infants, Toddlers, and Preschoolers Meet or Exceed Dietary Reference Intakes. J. Am. Diet. Assoc. 2010, 110, S27–S37. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.J.; Gibson, R.A.; Gibson, R.S.; Makrides, M. Nutrient intakes and status of preschool children in Adelaide, South Australia. Med. J. Aust. 2012, 196, 696–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donker, A.E.; van der Staaij, H.; Swinkels, D.W. The critical roles of iron during the journey from fetus to adolescent: Developmental aspects of iron homeostasis. Blood Rev. 2021, 50, 100866. [Google Scholar] [CrossRef]
- Karakochuk, C.D.; Hess, S.Y.; Moorthy, D.; Namaste, S.; Parker, M.E.; Rappaport, A.I.; Wegmüller, R.; Dary, O.; The HEmoglobin MEasurement (HEME) Working Group. Measurement and interpretation of hemoglobin concentration in clinical and field settings: A narrative review. Ann. N. Y. Acad. Sci. 2019, 1450, 126–146. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, C.M.; Looker, A.C. Laboratory methodologies for indicators of iron status: Strengths, limitations, and analytical challenges. Am. J. Clin. Nutr. 2017, 106, 1606S–1614S. [Google Scholar] [CrossRef] [Green Version]
- European Commission, Directorate-General for Health and Food Safety. Report from the Commission to the European Parliament and the Council on Young Child Formulae; European Commission: Brussels, Belgium, 2016. [Google Scholar]
- Morrison, A.; Polisena, J.; Husereau, D.; Moulton, K.; Clark, M.; Fiander, M.; Mierzwinski-Urban, M.; Clifford, T.; Hutton, B.; Rabb, D. The effect of english-language restriction on systematic review-based meta-analyses: A systematic review of empirical studies. Int. J. Technol. Assess. Health Care 2012, 28, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Rao, G.; Lopez-Jimenez, F.; Boyd, J.; D’Amico, F.; Durant, N.H.; Hlatky, M.; Howard, G.; Kirley, K.; Masi, C.; Powell-Wiley, T.M.; et al. Methodological Standards for Meta-Analyses and Qualitative Systematic Reviews of Cardiac Prevention and Treatment Studies: A Scientific Statement from the American Heart Association. Circulation 2017, 136, e172–e194. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Apparently Healthy Children Aged 9 to 48 * Months at Trial Commencement |
| Intervention/Exposure | Fortified milk or formula with added macronutrients, micronutrients and/or prebiotics, probiotics, or synbiotics |
| Comparison | Non-fortified milk or formula |
| Outcomes | Growth parameters including body size (e.g., weight, length (/height), body mass index, head circumference) Body composition (including skinfold thickness, waist circumference, body fat) Biochemical markers (including vitamin D, zinc, iron-related measures (serum ferritin, serum transferrin, haemoglobin) Dietary intake (energy, macro-, and micro-nutrients) |
| Study design | Randomised controlled trials |
| Exclusion criteria | Studies published prior to 1990 Studies published in non-English language Animal studies In vitro studies Studies in adolescents and adults Acute studies (<3-month intervention period) Observational studies, review articles, conference abstracts, protocol papers |
| Author, Year [Reference] | Country | Study Design | Intervention Length | Sample Size (Enrolled) | Sex (n, % Male) | Age Range Recruited | Co-Conditions | Quality Assessment |
|---|---|---|---|---|---|---|---|---|
| Akkermans et al., 2017 [33] | The Netherlands, United Kingdom, Germany | Randomised, double-blinded controlled trial | 20 weeks | n = 318 | n = 180, 57% | 12–36 months | 18% of sample had anaemia | Some concerns |
| Chatchatee et al., 2014 [32] | Malaysia, the Netherlands, Poland, Portugal, Thailand | Randomised, double-blinded controlled trial | 12 months | n = 804 | Mixed sex, distribution NR | 11–29 months | NR | Some concerns |
| Firmansyah et al., 2011 [28] | Indonesia | Randomised, double-blinded controlled trial | 12 months § | n = 393 | n = 203, 52% | 12 months | NR | Some concerns |
| Pontes et al., 2016 [41] | Brazil | Randomised, double-blinded controlled trial | 28 weeks | n = 256 | Mixed sex, distribution NR | 12–48 months | NR | Some concerns |
| Rivera et al., 2010 [42] | Brazil | Double-blinded, group randomised effectiveness trial | 12 months | n = 795 | Mixed sex, distribution NR | 12–30 months | ~43% of sample had anaemia | Some concerns |
| Sazawal et al., 2010a [35] | India | Randomised, double-blinded controlled trial | 12 months | n = 633 | Mixed sex, distribution NR | 12–36 months | ~54% of sample had iron deficiency anaemia ~47% were stunted ~5% were wasted ~16% were wasted and stunted | Some concerns |
| Sazawal et al., 2010b [36] | India | Randomised, double-blinded controlled trial | 12 months | n = 624 | Mixed sex, distribution NR | 12–36 months | ~56% of sample had iron deficiency anaemia ~47% were stunted ~5% were wasted ~16% were wasted and stunted | Low risk of bias |
| Villalpando et al., 2006 [37] | Mexico | Randomised, double blinded clinical trial | 6 months | n = 130 | n = 65, 50% | 10–30 months | ~36% of sample had anaemia | High risk of bias |
| Virtanen et al., 2001 [34] | Sweden | Randomised, double blinded controlled trial | 6 months | n = 54 | n = 21, 39% | 12 months | NR | High risk of bias |
| Studies with more than one article | ||||||||
| GUMLi trial | ||||||||
| Wall et al., 2019 [30] Lovell et al., 2018 [31] ⱡ Lovell et al., 2019 [44] ⱡ Lovell et al., 2021 [45] ⱡ | Australia, New Zealand | Randomised, double-blinded controlled trial | 12 months | n = 160 | n = 85, 53% | 12 months ± 2 weeks | NR | Some concerns Some concerns Some concerns Some concerns |
| Large UK trial | ||||||||
| Morley et al., 1999 [29] Singhal et al., 2000 [46] ⱡ | United Kingdom | Randomised, blinded controlled trial | 9 months | n = 493 | n = 257, 52% | 9 months | NR | Low risk of bias Low risk of bias |
| Toddler Food Study | ||||||||
| Szymlek-Gay et al., 2009 [43] * Morgan et al., 2010 [47] ⱡ,* Houghton et al., 2011 [48] ⱡ,* Szymlek-Gay et al., 2020 [49] ⱡ,* | New Zealand | Randomised, blinded placebo-controlled trial | 5 months | n = 135 | n = 62, 46% | 12–20 months | NR | Low risk of bias Some concerns Some concerns Some concerns |
| First Author, Year [Reference] | Study Outcomes Included in the Review | Intervention Condition/s | Control Condition | Adherence Check (Method) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Milk Type | Amount of Milk Prescribed | Amount of Milk Consumed | Completers (n, %) | Milk Type | Amount of Milk Prescribed | Amount of Milk Consumed | COMPLETERS (n, %) | |||
| Akkermans et al., 2017 [33] | Biochemical: Fe (Hb, SF), Fe deficiency, Fe deficiency anaemia, Vit D | Young child formula | >150 mL/d | NR | 114 (72%) | Cow’s milk | >150 mL/d | NR | 113 (71%) | Parent phone calls |
| Chatchatee et al., 2014 [32] | Growth: weight, length, BMI | Int 1 = Growing Up Milk (GUM) with added prebiotics and LCPUFAs Int 2 = GUM | 400 to 750 mL/d | Int 1 = 529 mL/d Int 2 = 527 mL/d | Int 1 = 348 (90%) Int 2 = 349 (92%) | Cow’s milk | 400 to 750 mL/d | 527 mL/day | 33 (100%) | Study diary |
| Firmansyah et al., 2011 [28] § | Growth: weight, length, BMI, WFA | Synbiotic Milk (BL999, LPR and prebiotics) with LCPUFA | 400 mL/d (200 mL twice, daily) | 426 ± 25.9 mL/d | 161 (81%) | Cow’s milk | 400 mL/d (200 mL twice, daily) | 426 ± 31.2 mL/d | 153 (79%) | NR |
| Pontes et al., 2016 [41] | Growth: WFA, length, LFA Biochemical: Fe (Hb, SF), Zn | Cow’s milk-based beverage fortified with DHA, prebiotics (PDX, GOS, β-glucan) and other nutrients | 720 mL/d (240 mL thrice daily) | 12–24 months of age: 504 mL/d 25–48 months of age: 498 mL/d | 120 (96%) | Cow’s milk-based beverage | 720 mL/d (240 mL thrice daily) | 12–24 months of age: 531 mL/d 25–48 months of age: 547 mL/d | 129 (98%) | NR |
| Rivera et al., 2010 [42] | Growth: WFA, LFA, WFL (data not shown) Biochemical: Fe (Hb, SF, sTfR), anaemia | Fortified milk formula | 400 mL/d (200 mL twice daily) | 611 mL/d ⱡ | 371 | Non-fortified milk formula | 400 mL/d (200 mL twice daily) | 609 mL/d ⱡ | 213 | Field workers conducted weekly surveys |
| Sazawal et al., 2010a [35] | Growth: weight, WFA, length, LFA, WFL Biochemical: Fe (Hb, SF, Tf) Fe deficiency, Fe deficiency anaemia, Zn Nutrient intake: energy, protein, fat, CHO, Fe, Zn | Milk powder fortified with Zn, Fe, Se, Cu, Vits A, C and E | 96 g (32 g single-serving sachet thrice daily) | NR | 289 (91%) | Cow’s milk powder | 96 g (32 g single-serving sachet thrice daily) | NR | 281 (89%) | Household milk assistants collected weekly data on compliance |
| Sazawal et al., 2010b [36] | Growth: weight, WFA, length, length, LFA, WFL Biochemical: Fe (Hb, SF, Tf), Fe deficiency, Fe deficiency anaemia, Zn | Milk powder fortified with probiotic B lactis HN019 and prebiotic oligosaccharides | 96 g (32 g single-serving sachet thrice daily) | NR | 296 (95%) | Cow’s milk powder | 96 g (32 g single-serving sachet thrice daily) | NR | 285 (91%) | NR |
| Villalpando et al., 2006 [37] | Biochemical: Fe (Hb, SF, sTfR) | Milk powder fortified with Fe and other micronutrients | 400 mL/d (200 mL twice daily) | 482 mL/d | 58 (88%) | Cow’s milk powder | 400 mL/d (200 mL twice daily) | 529 mL/d | 57 (88%) | A field worker observed and registered milk intake |
| Virtanen et al., 2001 [34] | Growth: weight Biochemical: Fe (Hb, SF, Tf, sTfR), iron deficiency, Fe deficiency anaemia Nutrient intake: Fe | Iron-fortified (lower protein) cow’s milk | Ad lib | 445 mL/d | 20 | Cow’s milk | Ad lib | 562 mL/d | 16 | NR |
| Studies with more than one article | ||||||||||
| GUMLi trial | ||||||||||
| Wall et al., 2019 [30] | Growth: weight, WFA, length, LFA, WFL, BMI, BMIFA, WC, waist-height ratio | GUM Lite (GUMLi) with reduced protein, synbiotics, and micronutrients added | 300 mL/d | NR | 67 (84%) | Cow’s milk | 300 mL/d | NR | 67 (84%) | Monthly telephone or face-to-face questionnaire with parents or guardians |
| Lovell et al., 2018 [31] | Biochemical: Fe (Hb, SF, Tf, sTfR), iron deficiency, Fe deficiency anaemia, Vit D Nutrient intake: Fe | |||||||||
| Lovell et al., 2019 [44] | Nutrient intake: energy, protein, fat, CHO, Fe | |||||||||
| Lovell et al., 2021 [45] | Growth: weight, WFA, length, LFA, WFL, BMI, BMIFA, body fat %, FFM, FM, FMI Nutrient intake: energy, protein | |||||||||
| Large UK trial | ||||||||||
| Morley et al., 1999 [29] | Growth: weight, length, skinfold, HC, MUAC Biochemical: Fe (Hb, SF, sTfR) | Int 1 = Fe-fortified formula (12 mg/L as ferrous sulfate) Int 2 = Standard formula (0.9 mg/L of Fe) | Ad lib | NR | n(int 1) = 135 (82%) n(int 2) = 133 (82%) | Cow’s milk | Ad lib | NR | n(con) = 160 (96%) | Nurse visit at mid- and end-intervention (12 and 15 months, respectively) |
| Singhal et al., 2000 [46] | Growth: weight. Biochemical: Fe (Hb, SF, sTfR) Nutrient intake: energy | |||||||||
| Toddler Food Study | ||||||||||
| Szymlek-Gay et al., 2009 [43] * | Biochemical: Fe (Hb, SF, sTfR) Nutrient intake: Fe | Iron, zinc, vitamin C and vitamin D, iodine fortified milk (lower protein) | ~370 mL/d | 407 | 41 (91%) | Non-fortified milk (with required vit D and A) | ~370 mL/d | 445 | 81 (90%) | Parents kept adherence records |
| Morgan et al., 2010 [47] * | Biochemical: Zn Nutrient intake: energy, fibre, Zn, Ca | |||||||||
| Houghton et al., 2011 [48] * | Biochemical: Vit D | |||||||||
| Szymlek-Gay et al., 2020 [49] * | Biochemical: Iodine Nutrient intake: energy, iodine | |||||||||
| Weight (kg) | Length/Height (cm) | Hb (g/L) | Ferritin (nmol/L) | Transferrin (μmol/L) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n Participants (n Studies) [Reference] | MD [95% CI] (Overall Effect p-Value; I2 %) | n Participants (n Studies) [Reference] | MD [95% CI] (Overall Effect p-Value; I2 %) | n Participants (n Studies) [Reference] | MD [95% CI] (Overall Effect p-Value; I2 %) | n Participants (n Studies) [Reference] | MD [95% CI] (Overall Effect p-Value; I2 %) | n Participants (n Studies) [Reference] | MD [95% CI] (Overall Effect p-Value; I2 %) | |
| Pooled result | n = 2829 (7 studies) [28,29,30,32,34,35,36] | 0.14 [0.06, 0.21] (p = 0.0003; I2 = 20%) | n = 2791 (6 studies) [28,29,30,32,35,36] | −0.05 [−0.41, 0.32] (p = 0.81; I2 = 80%) | n = 1991 (9 studies) [29,31,33,34,35,36,37,41,43] | 3.76 [0.17, 7.34] (p = 0.04; I2 = 93%) | n = 1732 (7 studies) [31,33,34,35,36,37,41] | 0.01 [0.00, 0.02] (p = 0.02; I2 = 99%) | n = 1078 (4 studies) [31,34,35,36] | −0.06 [−0.16, 0.04] (p = 0.23; I2 = 97%) |
| Subgroup analyses | ||||||||||
| Country economic status * | ||||||||||
| Lower-income countries | n = 1419 (3 studies) [28,35,36] | 0.16 [0.08, 0.23] (p < 0.0001; I2 = 16%) | n = 1419 (3 studies) [28,35,36] | 0.23 [−0.25, 0.70] (p = 0.36; I2 = 89%) | n = 1272 (4 studies) [35,36,37,41] | 6.44 [−1.24, 14.12] (p = 0.10; I2 = 97%) | n = 1272 (4 studies) [35,36,37,41] | 0.01 [−0.00, 0.02] (p = 0.11; I2 = 75%) | N/A § | |
| Higher-income countries | n = 609 (3 studies) [29,30,34] | 0.06 [−0.15, 0.27] (p = 0.57; I2 = 51%) | N/A § | n = 719 (5 studies) [29,31,33,34,43] | 1.18 [−0.83, 3.19] (p = 0.25; I2 = 51%) | n = 460 (3 studies) [31,33,34] | 0.01 [0.00, 0.03] (p = 0.02; I2 = 100%) | N/A § | ||
| Intervention length | ||||||||||
| ≤6 months | N/A § | N/A § | n = 599 (4 studies) [33,34,37,43] | 1.50 [−1.95. 4.95] (p = 0.39; I2 = 80%) | n = 441 (3 studies) [33,34,37] | 0.01 [−0.01, 0.02] (p = 0.24; I2 = 100%) | N/A § | |||
| >6 months | n = 2400 (5 studies) [29,30,32,35,36] | 0.15 [0.06, 0.25] (p = 0.001; I2 = 31%) | n = 2398 (5 studies) [29,30,32,35,36] | 0.05 [−0.30, 0.41] (p = 0.77; I2 = 73%) | n = 1391 (5 studies) [29,31,35,36,41] | 5.19 [−0.32, 10.69] (p = 0.07; I2 = 95%) | n = 1291 (4 studies) [31,35,36,41] | 0.01 [0.00, 0.02] (p = 0.03; I2 = 86%) | n = 1042 (3 studies) [31,35,36] | −0.05 [−0.15, 0.04] (p = 0.27; I2 = 98%) |
| Sensitivity analyses | ||||||||||
| Data treatment | ||||||||||
| Excluding studies with imputed data | n = 1863 (4 studies) [32,34,35,36] | 0.17 [0.10, 0.24] (p < 0.00001; I2 = 0%) | n = 1827 (3 studies) [32,35,36] | 0.39 [0.05, 0.72] (p = 0.02; I2 = 53%) | n = 733 (4 studies) [33,34,41,43] | −0.11 [−1.29, 1.07] (p = 0.86; I2 = 0%) | n = 690 (4 studies) [32,33,37,41] | 0.01 [−0.00, 0.02], p = 0.18; I2 = 99%) | N/A § | |
| Risk of bias | ||||||||||
| Excluding studies with high risk of bias [34,37] | n = 2793 (6 studies) [28,29,30,32,35,36] | 0.14 [0.06, 0.22] (p = 0.0007; I2 = 28%) | N/A ⱡ | n = 1840 (7 studies) [29,31,33,35,36,41,43] | 3.74 [−0.35, 7.84] (p = 0.07; I2 = 94%) | n = 1581 (5 studies) [31,33,35,36,41] | 0.01 [0.00, 0.02] (p = 0.002; I2 = 89%] | n = 1042 (3 studies) [31,35,36] | −0.05 [−0.15, 0.04] (p = 0.27; I2 = 98%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brooker, P.G.; Rebuli, M.A.; Williams, G.; Muhlhausler, B.S. Effect of Fortified Formula on Growth and Nutritional Status in Young Children: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 5060. https://doi.org/10.3390/nu14235060
Brooker PG, Rebuli MA, Williams G, Muhlhausler BS. Effect of Fortified Formula on Growth and Nutritional Status in Young Children: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(23):5060. https://doi.org/10.3390/nu14235060
Chicago/Turabian StyleBrooker, Paige G., Megan A. Rebuli, Gemma Williams, and Beverly S. Muhlhausler. 2022. "Effect of Fortified Formula on Growth and Nutritional Status in Young Children: A Systematic Review and Meta-Analysis" Nutrients 14, no. 23: 5060. https://doi.org/10.3390/nu14235060
APA StyleBrooker, P. G., Rebuli, M. A., Williams, G., & Muhlhausler, B. S. (2022). Effect of Fortified Formula on Growth and Nutritional Status in Young Children: A Systematic Review and Meta-Analysis. Nutrients, 14(23), 5060. https://doi.org/10.3390/nu14235060