
Dietary Habits of a Group of Children with Crohn’s Disease Compared to Healthy Subjects: Assessment of Risk of Nutritional Deficiencies through a Bromatological Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
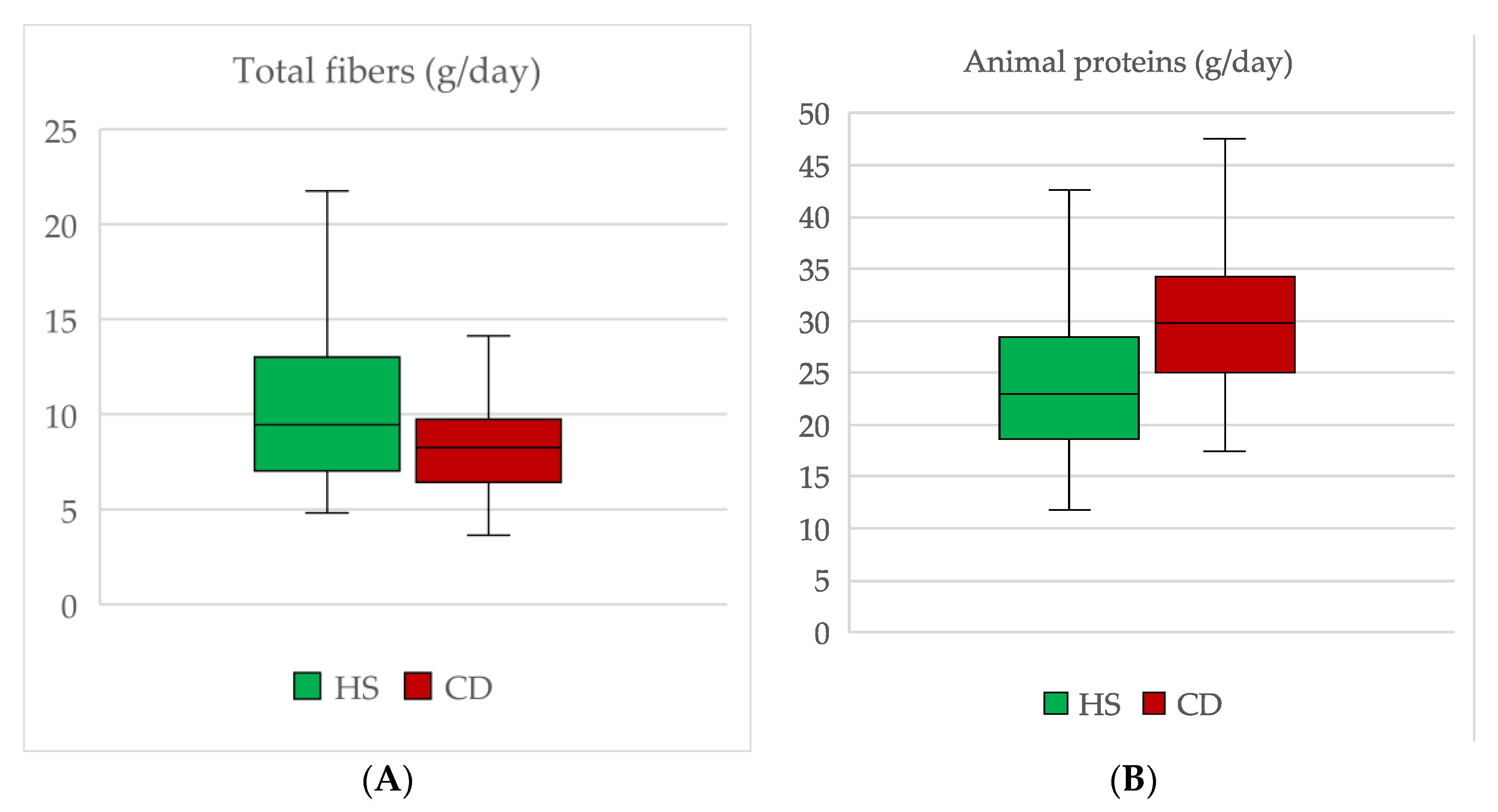
3.1. Fibers
3.2. Proteins and Amino Acids
3.3. Carbohydrates
3.4. Lipids
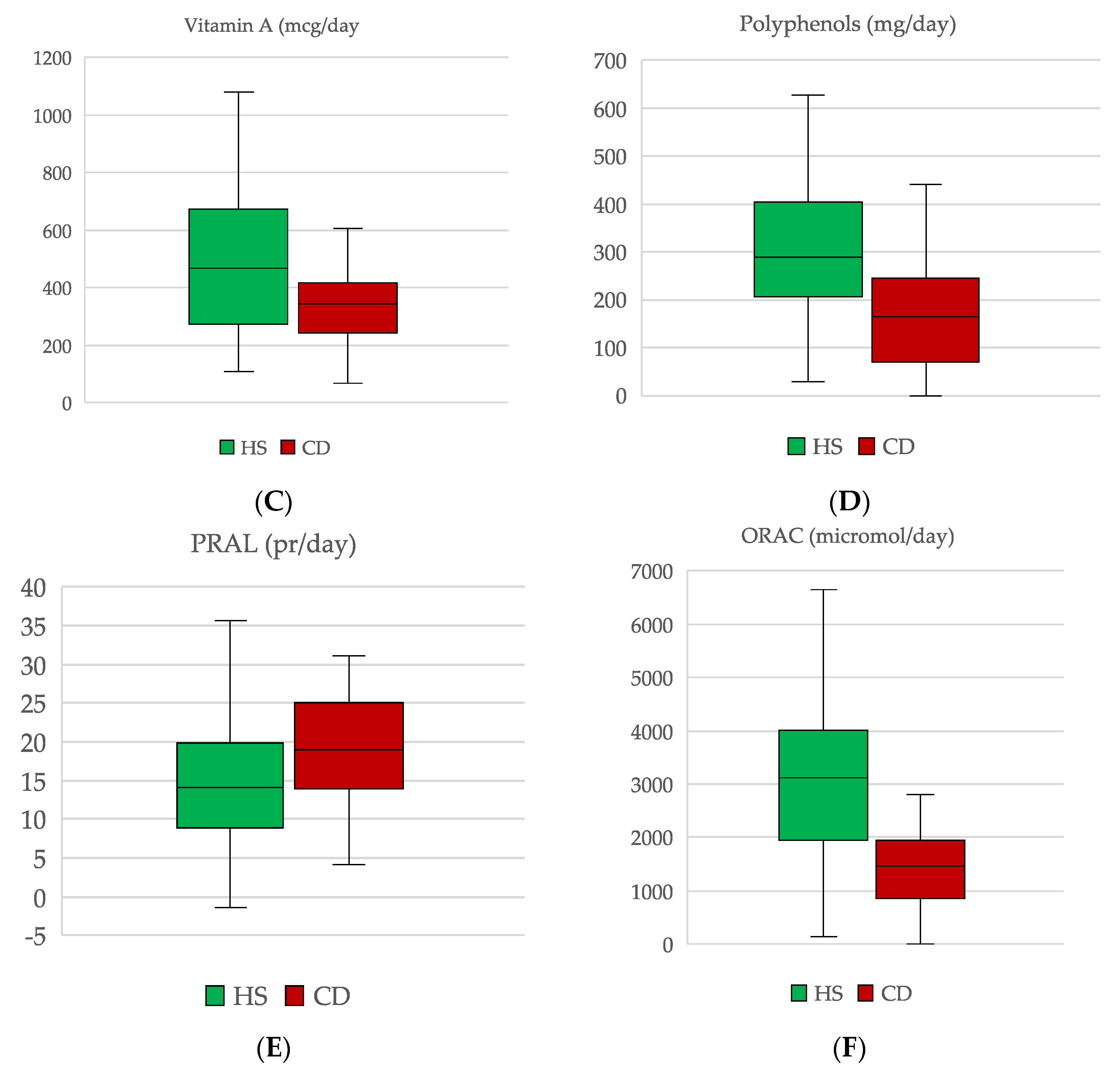
3.5. Micronutrients
3.6. ORAC and PRAL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mills, S.C.; von Roon, A.C.; Tekkis, P.P.; Orchard, T.R. Crohn’s Disease. BMJ Clin. Evid. 2011, 2011, 0416. [Google Scholar] [PubMed]
- Griffiths, A.M. Specificities of Inflammatory Bowel Disease in Childhood. Best Pract. Res. Clin. Gastroenterol. 2004, 18, 509–523. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.G. The Global Burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing Incidence and Prevalence of the Inflammatory Bowel Diseases with Time, Based on Systematic Review. Gastroenterology 2012, 142, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Sýkora, J.; Pomahačová, R.; Kreslová, M.; Cvalínová, D.; Štych, P.; Schwarz, J. Current Global Trends in the Incidence of Pediatric-Onset Inflammatory Bowel Disease. World J. Gastroenterol. 2018, 24, 2741–2763. [Google Scholar] [CrossRef]
- Heselmans, M.; Reid, G.; Akkermans, L.M.; Savelkoul, H.; Timmerman, H.; Rombouts, F.M. Gut flora in health and disease: Potential role of probiotics. Curr. Issues Intest. Microbiol. 2005, 6, 1–7. [Google Scholar]
- Rizzello, F.; Spisni, E.; Giovanardi, E.; Imbesi, V.; Salice, M.; Alvisi, P.; Valerii, M.C.; Gionchetti, P. Implications of the Westernized Diet in the Onset and Progression of IBD. Nutrients 2019, 11, 1033. [Google Scholar] [CrossRef] [Green Version]
- Crooks, B.; Misra, R.; Arebi, N.; Kok, K.; Brookes, M.; McLaughlin, J.; Limdi, J.K. The Dietary Practices and Beliefs of People Living with Older-Onset Inflammatory Bowel Disease. Eur. J. Gastroenterol. Hepatol. 2021, 33, e442–e448. [Google Scholar] [CrossRef]
- Thomas, A.G.; Taylor, F.; Miller, V. Dietary Intake and Nutritional Treatment in Childhood Crohn’s Disease. J. Pediatric Gastroenterol. Nutr. 1993, 17, 75–81. [Google Scholar] [CrossRef]
- Gavin, J.; Anderson, C.E.; Bremner, A.R.; Beattie, R.M. Energy Intakes of Children with Crohn’s Disease Treated with Enteral Nutrition as Primary Therapy. J. Hum. Nutr. Diet 2005, 18, 337–342. [Google Scholar] [CrossRef]
- Pons, R.; Whitten, K.E.; Woodhead, H.; Leach, S.T.; Lemberg, D.A.; Day, A.S. Dietary Intakes of Children with Crohn’s Disease. Br. J. Nutr. 2009, 102, 1052–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman, C.; Marderfeld, L.; Davidson, K.; Mozer-Glassberg, Y.; Poraz, I.; Silbermintz, A.; Zevit, N.; Shamir, R. Food Intake Adequacy in Children and Adolescents with Inflammatory Bowel Disease. J. Pediatric Gastroenterol. Nutr. 2016, 63, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; de Ridder, L.; Kolho, K.-L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. The ESPGHAN Revised Porto Criteria for the Diagnosis of Inflammatory Bowel Disease in Children and Adolescents. J. Pediatric Gastroenterol. Nutr. 2013, 58, 795–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, A.; Griffiths, A.; Markowitz, J.; Wilson, D.C.; Turner, D.; Russell, R.K.; Fell, J.; Ruemmele, F.M.; Walters, T.; Sherlock, M.; et al. Pediatric Modification of the Montreal Classification for Inflammatory Bowel Disease: The Paris Classification. Inflamm. Bowel Dis. 2011, 17, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Otley, A.R.; Mack, D.; Hyams, J.; de Bruijne, J.; Uusoue, K.; Walters, T.D.; Zachos, M.; Mamula, P.; Beaton, D.E.; et al. Development, Validation, and Evaluation of a Pediatric Ulcerative Colitis Activity Index: A Prospective Multicenter Study. Gastroenterology 2007, 133, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Sette, S.; Le Donne, C.; Piccinelli, R.; Arcella, D.; Turrini, A.; Leclercq, C. INRAN-SCAI 2005-6 Study Group The Third Italian National Food Consumption Survey, INRAN-SCAI 2005-06--Part 1: Nutrient Intakes in Italy. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 922–932. [Google Scholar] [CrossRef]
- Ishige, T. Growth Failure in Pediatric Onset Inflammatory Bowel Disease: Mechanisms, Epidemiology, and Management. Transl. Pediatric 2019, 8, 16–22. [Google Scholar] [CrossRef]
- Oliva, M.M.; Lake, A.M. Nutritional Considerations and Management of the Child with Inflammatory Bowel Disease. Nutrition 1996, 12, 151–158. [Google Scholar] [CrossRef]
- Nguyen, G.C.; Munsell, M.; Harris, M.L. Nationwide Prevalence and Prognostic Significance of Clinically Diagnosable Protein-Calorie Malnutrition in Hospitalized Inflammatory Bowel Disease Patients. Inflamm. Bowel Dis. 2008, 14, 1105–1111. [Google Scholar] [CrossRef]
- Van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohn’s Colitis 2021, 15, 171–194. [Google Scholar] [CrossRef]
- Scarallo, L.; Lionetti, P. Dietary Management in Pediatric Patients with Crohn’s Disease. Nutrients 2021, 13, 1611. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Dolev, N.; Sladek, M.; Hussey, S.; Turner, D.; Veres, G.; Koletzko, S.; de Carpi, J.M.; Staiano, A.; Shaoul, R.; Lionetti, P.; et al. Differences in Outcomes Over Time with Exclusive Enteral Nutrition Compared with Steroids in Children With Mild to Moderate Crohn’s Disease: Results From the GROWTH CD Study. J. Crohns Colitis 2018, 12, 306–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, A.; Wine, E.; Assa, A.; Boneh, R.S.; Shaoul, R.; Kori, M.; Cohen, S.; Peleg, S.; Shamaly, H.; On, A.; et al. Crohn’s Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. Gastroenterology 2019, 157, 440–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boneh, R.S.; Shabat, C.S.; Yanai, H.; Chermesh, I.; Ben Avraham, S.; Boaz, M.; Levine, A. Dietary Therapy with the Crohn’s Disease Exclusion Diet Is a Successful Strategy for Induction of Remission in Children and Adults Failing Biological Therapy. J. Crohn’s Colitis 2017, 11, 1205–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigall-Boneh, R.; Pfeffer-Gik, T.; Segal, I.; Zangen, T.; Boaz, M.; Levine, A. Partial Enteral Nutrition with a Crohn’s Disease Exclusion Diet Is Effective for Induction of Remission in Children and Young Adults with Crohns Disease. Inflamm. Bowel Dis. 2014, 20, 1353–1360. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Wine, E. Effects of Enteral Nutrition on Crohn’s Disease: Clues to the Impact of Diet on Disease Pathogenesis. Inflamm. Bowel Dis. 2013, 19, 1322–1329. [Google Scholar] [CrossRef]
- Miele, E.; Shamir, R.; Aloi, M.; Assa, A.; Braegger, C.; Bronsky, J.; de Ridder, L.; Escher, J.C.; Hojsak, I.; Kolaček, S.; et al. Nutrition in Pediatric Inflammatory Bowel Disease: A Position Paper on Behalf of the Porto Inflammatory Bowel Disease Group of the European Society of Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatric Gastroenterol. Nutr. 2018, 66, 687–708. [Google Scholar] [CrossRef] [Green Version]
- Den Besten, G.; van Eunen, K.; Groen, A.K.; Venema, K.; Reijngoud, D.-J.; Bakker, B.M. The Role of Short-Chain Fatty Acids in the Interplay between Diet, Gut Microbiota, and Host Energy Metabolism. J. Lipid Res. 2013, 54, 2325–2340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidal-Lletjós, S.; Beaumont, M.; Tomé, D.; Benamouzig, R.; Blachier, F.; Lan, A. Dietary Protein and Amino Acid Supplementation in Inflammatory Bowel Disease Course: What Impact on the Colonic Mucosa? Nutrients 2017, 9, 310. [Google Scholar] [CrossRef] [Green Version]
- Shoda, R.; Matsueda, K.; Yamato, S.; Umeda, N. Epidemiologic Analysis of Crohn Disease in Japan: Increased Dietary Intake of n-6 Polyunsaturated Fatty Acids and Animal Protein Relates to the Increased Incidence of Crohn Disease in Japan. Am. J. Clin. Nutr. 1996, 63, 741–745. [Google Scholar] [CrossRef]
- Jantchou, P.; Morois, S.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Carbonnel, F. Animal Protein Intake and Risk of Inflammatory Bowel Disease: The E3N Prospective Study. Am. J. Gastroenterol. 2010, 105, 2195–2201. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.K.; Abraham, B.; El-Serag, H. Dietary Intake and Risk of Developing Inflammatory Bowel Disease: A Systematic Review of the Literature. Am. J. Gastroenterol. 2011, 106, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Opstelten, J.L.; de Vries, J.H.M.; Wools, A.; Siersema, P.D.; Oldenburg, B.; Witteman, B.J.M. Dietary Intake of Patients with Inflammatory Bowel Disease: A Comparison with Individuals from a General Population and Associations with Relapse. Clin. Nutr. 2019, 38, 1892–1898. [Google Scholar] [CrossRef] [PubMed]
- Andriamihaja, M.; Davila, A.-M.; Eklou-Lawson, M.; Petit, N.; Delpal, S.; Allek, F.; Blais, A.; Delteil, C.; Tomé, D.; Blachier, F. Colon Luminal Content and Epithelial Cell Morphology Are Markedly Modified in Rats Fed with a High-Protein Diet. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 299, G1030–G1037. [Google Scholar] [CrossRef] [Green Version]
- Beaumont, M.; Andriamihaja, M.; Lan, A.; Khodorova, N.; Audebert, M.; Blouin, J.-M.; Grauso, M.; Lancha, L.; Benetti, P.-H.; Benamouzig, R.; et al. Detrimental Effects for Colonocytes of an Increased Exposure to Luminal Hydrogen Sulfide: The Adaptive Response. Free Radic. Biol. Med. 2016, 93, 155–164. [Google Scholar] [CrossRef]
- De Filippo, C.; Di Paola, M.; Ramazzotti, M.; Albanese, D.; Pieraccini, G.; Banci, E.; Miglietta, F.; Cavalieri, D.; Lionetti, P. Diet, Environments, and Gut Microbiota. A Preliminary Investigation in Children Living in Rural and Urban Burkina Faso and Italy. Front. Microbiol. 2017, 8, 1979. [Google Scholar] [CrossRef] [Green Version]
- Spooren, C.E.G.M.; Pierik, M.J.; Zeegers, M.P.; Feskens, E.J.M.; Masclee, A.A.M.; Jonkers, D.M.A.E. Review Article: The Association of Diet with Onset and Relapse in Patients with Inflammatory Bowel Disease. Aliment Pharmacol. Ther. 2013, 38, 1172–1187. [Google Scholar] [CrossRef] [Green Version]
- Amre, D.K.; D’Souza, S.; Morgan, K.; Seidman, G.; Lambrette, P.; Grimard, G.; Israel, D.; Mack, D.; Ghadirian, P.; Deslandres, C.; et al. Imbalances in Dietary Consumption of Fatty Acids, Vegetables, and Fruits Are Associated with Risk for Crohn’s Disease in Children. Am. J. Gastroenterol. 2007, 102, 2016–2025. [Google Scholar] [CrossRef]
- Ferreira, P.; Cravo, M.; Guerreiro, C.S.; Tavares, L.; Santos, P.M.; Brito, M. Fat Intake Interacts with Polymorphisms of Caspase9, FasLigand and PPARgamma Apoptotic Genes in Modulating Crohn’s Disease Activity. Clin. Nutr. 2010, 29, 819–823. [Google Scholar] [CrossRef]
- Tanaka, M.; Iwao, Y.; Sasaki, S.; Okamoto, S.; Ogata, H.; Hibi, T.; Kazuma, K. Moderate Dietary Temperance Effectively Prevents Relapse of Crohn Disease: A Prospective Study of Patients in Remission. Gastroenterol. Nurs. 2007, 30, 202–210. [Google Scholar] [CrossRef]
- Sirisinha, S. The Pleiotropic Role of Vitamin A in Regulating Mucosal Immunity. Asian Pac. J. Allergy Immunol. 2015, 33, 71–89. [Google Scholar] [PubMed]
- Tejón, G.; Manríquez, V.; De Calisto, J.; Flores-Santibáñez, F.; Hidalgo, Y.; Crisóstomo, N.; Fernández, D.; Sauma, D.; Mora, J.R.; Bono, M.R.; et al. Vitamin A Impairs the Reprogramming of Tregs into IL-17-Producing Cells during Intestinal Inflammation. Biomed. Res. Int. 2015, 2015, 137893. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Banares, F.; Abad-Lacruz, A.; Xiol, X.; Gine, J.J.; Dolz, C.; Cabre, E.; Esteve, M.; Gonzalez-Huix, F.; Gassull, M.A. Vitamin Status in Patients with Inflammatory Bowel Disease. Am. J. Gastroenterol. 1989, 84, 744–748. [Google Scholar] [PubMed]
- Filippi, J.; Al-Jaouni, R.; Wiroth, J.-B.; Hébuterne, X.; Schneider, S.M. Nutritional Deficiencies in Patients with Crohn’s Disease in Remission. Inflamm. Bowel Dis. 2006, 12, 185–191. [Google Scholar] [CrossRef]
- Sampietro, G.M.; Cristaldi, M.; Cervato, G.; Maconi, G.; Danelli, P.; Cervellione, R.; Rovati, M.; Porro, G.B.; Cestaro, B.; Taschieri, A.M. Oxidative Stress, Vitamin A and Vitamin E Behaviour in Patients Submitted to Conservative Surgery for Complicated Crohn’s Disease. Dig. Liver Dis. 2002, 34, 696–701. [Google Scholar] [CrossRef]
- Soares-Mota, M.; Silva, T.A.; Gomes, L.M.; Pinto, M.A.S.; Mendonça, L.M.C.; Farias, M.L.F.; Nunes, T.; Ramalho, A.; Zaltman, C. High Prevalence of Vitamin A Deficiency in Crohn’s Disease Patients According to Serum Retinol Levels and the Relative Dose-Response Test. World J. Gastroenterol. 2015, 21, 1614–1620. [Google Scholar] [CrossRef]
- Battat, R.; Kopylov, U.; Szilagyi, A.; Saxena, A.; Rosenblatt, D.S.; Warner, M.; Bessissow, T.; Seidman, E.; Bitton, A. Vitamin B12 Deficiency in Inflammatory Bowel Disease: Prevalence, Risk Factors, Evaluation, and Management. Inflamm. Bowel Dis. 2014, 20, 1120–1128. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology Consensus Guidelines on the Management of Inflammatory Bowel Disease in Adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [Green Version]
- Yakut, M.; Ustün, Y.; Kabaçam, G.; Soykan, I. Serum Vitamin B12 and Folate Status in Patients with Inflammatory Bowel Diseases. Eur. J. Intern. Med. 2010, 21, 320–323. [Google Scholar] [CrossRef]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food Sources and Bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [Green Version]
- Kruidenier, L.; Verspaget, H.W. Review Article: Oxidative Stress as a Pathogenic Factor in Inflammatory Bowel Disease--Radicals or Ridiculous? Aliment Pharmacol. Ther. 2002, 16, 1997–2015. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CD (g/day) | HS (g/day) | ||||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p | |
| Lys | 2.45 | 1.87, 2.74 | 1.74 | 1.25, 2.25 | 0.004 |
| His | 1.10 | 0.95, 1.27 | 0.82 | 0.55, 1.00 | 0.002 |
| Arg | 1.75 | 1.56, 1.97 | 1.30 | 1.06, 1.56 | 0.001 |
| Asp | 2.56 | 2.12, 2.99 | 2.11 | 1.60, 2.53 | 0.019 |
| Val | 1.74 | 1.51,1.98 | 0.68 | 1.07, 1.72 | 0.015 |
| Gly | 1.18 | 1.12, 1.39 | 0.99 | 0.75, 1.14 | 0.001 |
| Ile | 1.54 | 1.36, 1.72 | 1.21 | 0.90, 1.45 | 0.001 |
| Thr | 1.40 | 1.11, 1.58 | 1.05 | 0.81, 1.26 | 0.002 |
| Ala | 1.54 | 1.26, 1.78 | 1.12 | 0.87,1.49 | 0.002 |
| Met | 0.85 | 0.68, 0.94 | 0.68 | 0.46, 0.82 | 0.015 |
| Tyr | 1.26 | 0.92, 1.37 | 1.03 | 0.66, 1.20 | 0.034 |
| CD (g/day) | HS (g/day) | ||||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p | |
| Palmitic | 1.94 | 1.53, 3.23 | 2.68 | 2.20, 3.90 | 0.037 |
| Arachidic | 0.02 | 0.01, 0.02 | 0.04 | 0.02, 0.08 | 0.005 |
| Oleic | 5.47 | 3.21, 7.30 | 7.45 | 5.66, 10.93 | 0.003 |
| Linolenic | 0.15 | 0.09, 0.23 | 0.21 | 0.16, 0.26 | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labriola, F.; Marcato, C.; Zarbo, C.; Betti, L.; Catelli, A.; Valerii, M.C.; Spisni, E.; Alvisi, P. Dietary Habits of a Group of Children with Crohn’s Disease Compared to Healthy Subjects: Assessment of Risk of Nutritional Deficiencies through a Bromatological Analysis. Nutrients 2022, 14, 499. https://doi.org/10.3390/nu14030499
Labriola F, Marcato C, Zarbo C, Betti L, Catelli A, Valerii MC, Spisni E, Alvisi P. Dietary Habits of a Group of Children with Crohn’s Disease Compared to Healthy Subjects: Assessment of Risk of Nutritional Deficiencies through a Bromatological Analysis. Nutrients. 2022; 14(3):499. https://doi.org/10.3390/nu14030499
Chicago/Turabian StyleLabriola, Flavio, Caterina Marcato, Chiara Zarbo, Ludovica Betti, Arianna Catelli, Maria Chiara Valerii, Enzo Spisni, and Patrizia Alvisi. 2022. "Dietary Habits of a Group of Children with Crohn’s Disease Compared to Healthy Subjects: Assessment of Risk of Nutritional Deficiencies through a Bromatological Analysis" Nutrients 14, no. 3: 499. https://doi.org/10.3390/nu14030499
APA StyleLabriola, F., Marcato, C., Zarbo, C., Betti, L., Catelli, A., Valerii, M. C., Spisni, E., & Alvisi, P. (2022). Dietary Habits of a Group of Children with Crohn’s Disease Compared to Healthy Subjects: Assessment of Risk of Nutritional Deficiencies through a Bromatological Analysis. Nutrients, 14(3), 499. https://doi.org/10.3390/nu14030499