
Effect of Magnesium Supplementation on Inflammatory Parameters: A Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction
2.4. Outcomes
2.5. Quality Assessment
2.6. Data Synthesis and Analysis
3. Results
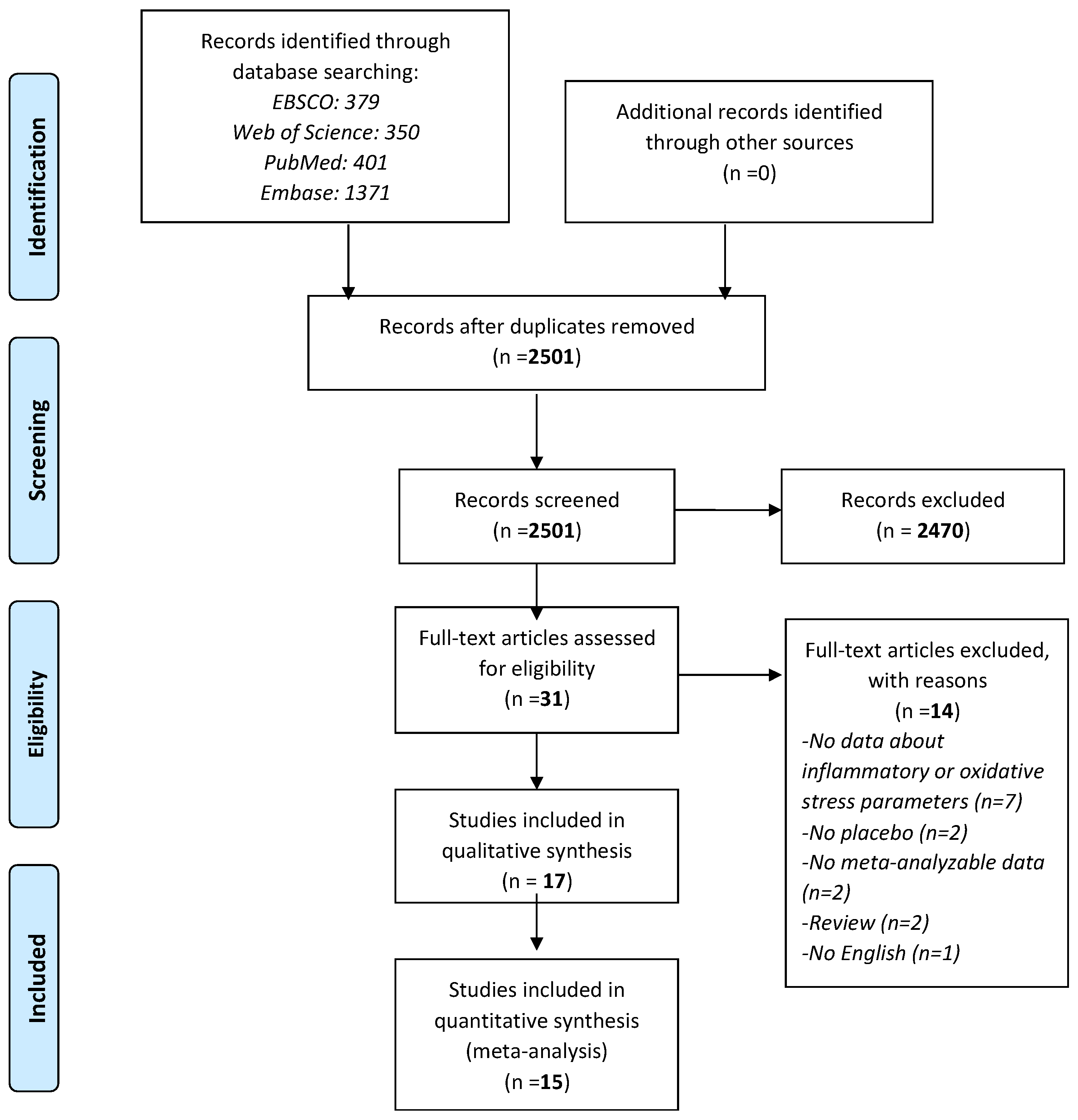
3.1. Search Results
3.2. Study and Patient Characteristics
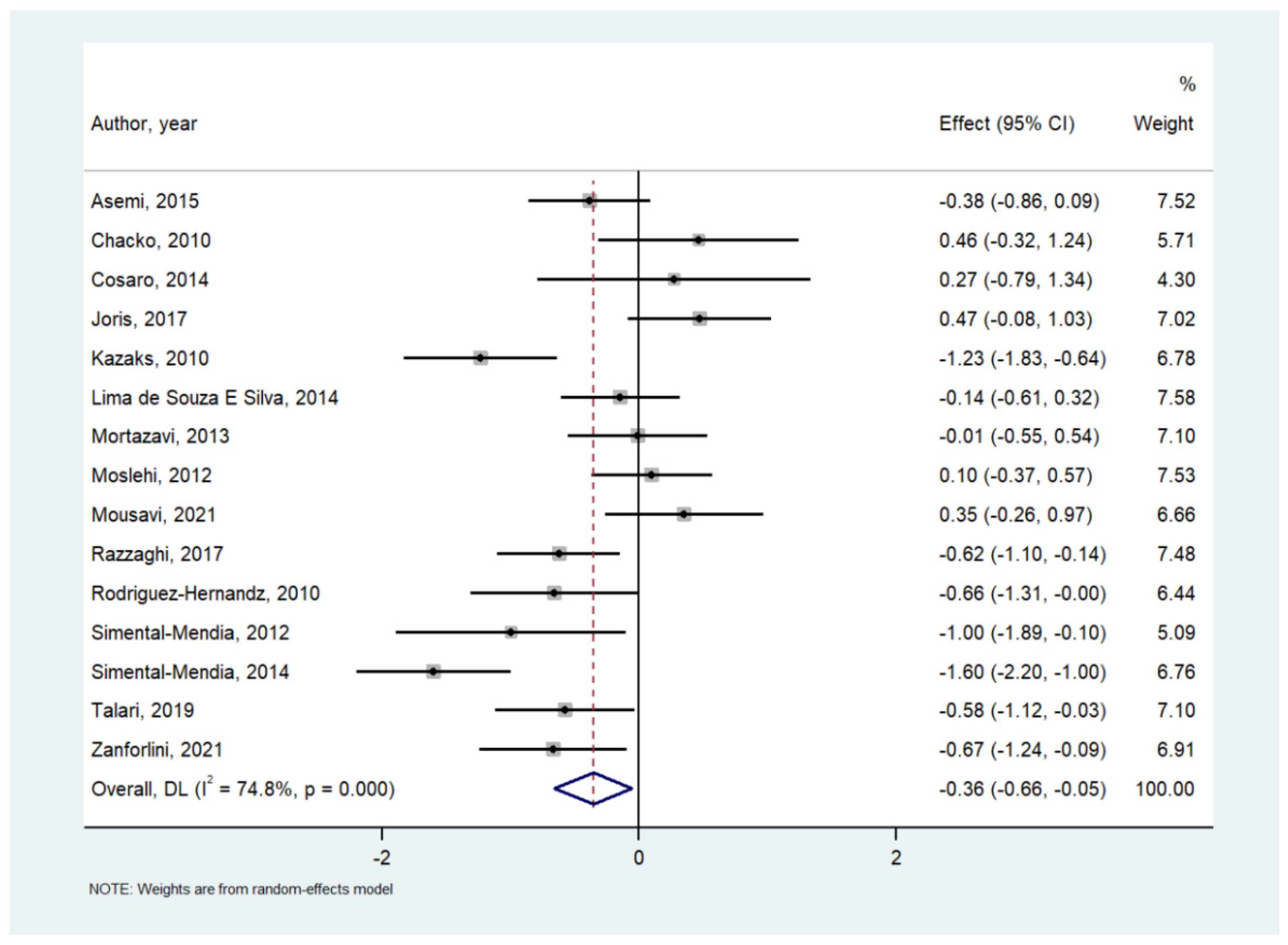
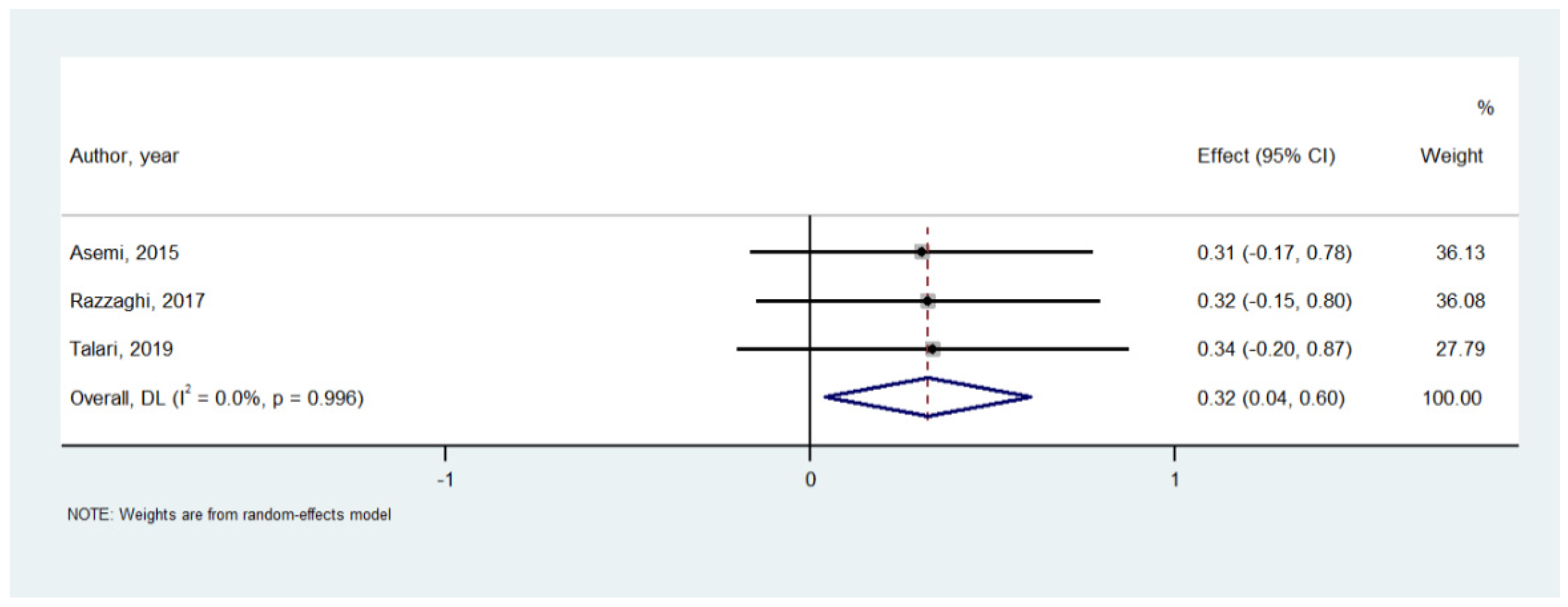
3.3. Meta-Analysis of Mg Supplementation versus Placebo on Serum Inflammatory Parameters
3.4. Risk of Bias
3.5. Meta-Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Veronese, N.; Demurtas, J.; Pesolillo, G.; Celotto, S.; Barnini, T.; Calusi, G.; Caruso, M.G.; Notarnicola, M.; Reddavide, R.; Stubbs, B. Magnesium and health outcomes: An umbrella review of systematic reviews and meta-analyses of observational and intervention studies. Eur. J. Nutr. 2020, 59, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Caspi, R.; Altman, T.; Billington, R.; Dreher, K.; Foerster, H.; Fulcher, C.A.; Holland, T.A.; Keseler, I.M.; Kothari, A.; Kubo, A. The MetaCyc database of metabolic pathways and enzymes and the BioCyc collection of Pathway/Genome Databases. Nucleic Acids Res. 2014, 42, D459–D471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacs, L.; Molnar, B.; Huhn, E.; Bodis, L. Magnesium substitution in pregnancy. A prospective, randomized double-blind study. Geburtshilfe Frauenheilkd. 1988, 48, 595–600. [Google Scholar]
- Bartal, M.F.; Sibai, B.M. Eclampsia in the 21st century. Am. J. Obstet. Gynecol. 2020. ahead of print. [Google Scholar] [CrossRef]
- Fanni, D.; Gerosa, C.; Nurchi, V.; Manchia, M.; Saba, L.; Coghe, F.; Crisponi, G.; Gibo, Y.; Van Eyken, P.; Fanos, V. The role of magnesium in pregnancy and in fetal programming of adult diseases. Biol. Trace Elem. Res. 2021, 199, 3647–3657. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose–response meta-analysis of prospective cohort studies. BMC Med. 2016, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, L.; Veronese, N.; Barbagallo, M. Magnesium and Hypertension in Old Age. Nutrients 2021, 13, 139. [Google Scholar] [CrossRef]
- Gröber, U.; Schmidt, J.; Kisters, K. Magnesium in prevention and therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, L.J.; Veronese, N.; Guerrero-Romero, F.; Barbagallo, M. Magnesium in Infectious Diseases in Older People. Nutrients 2021, 13, 180. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in aging, health and diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Watutantrige-Fernando, S.; Luchini, C.; Solmi, M.; Sartore, G.; Sergi, G.; Manzato, E.; Barbagallo, M.; Maggi, S.; Stubbs, B. Effect of magnesium supplementation on glucose metabolism in people with or at risk of diabetes: A systematic review and meta-analysis of double-blind randomized controlled trials. Eur. J. Clin. Nutr. 2016, 70, 1354–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veronese, N.; Dominguez, L.J.; Pizzol, D.; Demurtas, J.; Smith, L.; Barbagallo, M. Oral Magnesium Supplementation for Treating Glucose Metabolism Parameters in People with or at Risk of Diabetes: A Systematic Review and Meta-Analysis of Double-Blind Randomized Controlled Trials. Nutrients 2021, 13, 4074. [Google Scholar] [CrossRef] [PubMed]
- King, D.E.; Mainous, A.G., III; Geesey, M.E.; Woolson, R.F. Dietary magnesium and C-reactive protein levels. J. Am. Coll. Nutr. 2005, 24, 166–171. [Google Scholar] [CrossRef]
- Mazidi, M.; Rezaie, P.; Banach, M. Effect of magnesium supplements on serum C-reactive protein: A systematic review and meta-analysis. Arch. Med. Sci. AMS 2018, 14, 707–716. [Google Scholar] [CrossRef]
- Simental-Mendia, L.E.; Sahebkar, A.; Rodriguez-Moran, M.; Zambrano-Galvan, G.; Guerrero-Romero, F. Effect of Magnesium Supplementation on Plasma C-reactive Protein Concentrations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Pharm. Des. 2017, 23, 4678–4686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, J.A.; Castiglioni, S.; Locatelli, L.; Zocchi, M.; Mazur, A. Magnesium and inflammation: Advances and perspectives. Semin. Cell Dev. Biol. 2021, 115, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Karamali, M.; Jamilian, M.; Foroozanfard, F.; Bahmani, F.; Heidarzadeh, Z.; Benisi-Kohansal, S.; Surkan, P.J.; Esmaillzadeh, A. Magnesium supplementation affects metabolic status and pregnancy outcomes in gestational diabetes: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2015, 102, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Kazaks, A.G.; Uriu-Adams, J.Y.; Albertson, T.E.; Shenoy, S.F.; Stern, J.S. Effect of oral magnesium supplementation on measures of airway resistance and subjective assessment of asthma control and quality of life in men and women with mild to moderate asthma: A randomized placebo controlled trial. J. Asthma 2010, 47, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Chacko, S.A.; Sul, J.; Song, Y.; Li, X.; LeBlanc, J.; You, Y.; Butch, A.; Liu, S. Magnesium supplementation, metabolic and inflammatory markers, and global genomic and proteomic profiling: A randomized, double-blind, controlled, crossover trial in overweight individuals. Am. J. Clin. Nutr. 2011, 93, 463–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simental-Mendia, L.E.; Rodriguez-Moran, M.; Reyes-Romero, M.A.; Guerrero-Romero, F. No positive effect of oral magnesium supplementation in the decreases of inflammation in subjects with prediabetes: A pilot study. Magnes. Res. 2012, 25, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Mortazavi, M.; Moeinzadeh, F.; Saadatnia, M.; Shahidi, S.; McGee, J.C.; Minagar, A. Effect of magnesium supplementation on carotid intima-media thickness and flow-mediated dilatation among hemodialysis patients: A double-blind, randomized, placebo-controlled trial. Eur. Neurol. 2013, 69, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Cosaro, E.; Bonafini, S.; Montagnana, M.; Danese, E.; Trettene, M.S.; Minuz, P.; Delva, P.; Fava, C. Effects of magnesium supplements on blood pressure, endothelial function and metabolic parameters in healthy young men with a family history of metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Lima de Souza, E.S.M.L.; Cruz, T.; Rodrigues, L.E.; Ladeia, A.M.; Bomfim, O.; Olivieri, L.; Melo, J.; Correia, R.; Porto, M.; Cedro, A. Magnesium replacement does not improve insulin resistance in patients with metabolic syndrome: A 12-week randomized double-blind study. J. Clin. Med. Res. 2014, 6, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Simental-Mendia, L.E.; Rodriguez-Moran, M.; Guerrero-Romero, F. Oral magnesium supplementation decreases C-reactive protein levels in subjects with prediabetes and hypomagnesemia: A clinical randomized double-blind placebo-controlled trial. Arch. Med. Res. 2014, 45, 325–330. [Google Scholar] [CrossRef]
- Joris, P.J.; Plat, J.; Bakker, S.J.; Mensink, R.P. Effects of long-term magnesium supplementation on endothelial function and cardiometabolic risk markers: A randomized controlled trial in overweight/obese adults. Sci. Rep. 2017, 7, 106. [Google Scholar] [CrossRef]
- Razzaghi, R.; Pidar, F.; Momen-Heravi, M.; Bahmani, F.; Akbari, H.; Asemi, Z. Magnesium Supplementation and the Effects on Wound Healing and Metabolic Status in Patients with Diabetic Foot Ulcer: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2018, 181, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Talari, H.R.; Zakizade, M.; Soleimani, A.; Bahmani, F.; Ghaderi, A.; Mirhosseini, N.; Eslahi, M.; Babadi, M.; Mansournia, M.A.; Asemi, Z. Effects of magnesium supplementation on carotid intima-media thickness and metabolic profiles in diabetic haemodialysis patients: A randomised, double-blind, placebo-controlled trial. Br. J. Nutr. 2019, 121, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Chen, L.Y.; Rudser, K.D.; Norby, F.L.; Rooney, M.R.; Lutsey, P.L. Effect of Magnesium Supplementation on Circulating Biomarkers of Cardiovascular Disease. Nutrients 2020, 12, 1697. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Hernandez, H.; Cervantes-Huerta, M.; Rodriguez-Moran, M.; Guerrero-Romero, F. Oral magnesium supplementation decreases alanine aminotransferase levels in obese women. Magnes. Res. 2010, 23, 90–96. [Google Scholar] [CrossRef]
- Moslehi, N.; Vafa, M.; Rahimi-Foroushani, A.; Golestan, B. Effects of oral magnesium supplementation on inflammatory markers in middle-aged overweight women. J. Res. Med. Sci. 2012, 17, 607. [Google Scholar]
- Hosseini, S.A.; Fathi, N.; Tavakkol, H.; Yadollahpour, A. Investigating the effects of oral magnesium citrate supplement on lung function, magnesium level and interlukine-17 in patients with asthma. Int. J. Pharm. Res. Allied Sci. 2016, 5, 86–92. [Google Scholar]
- Zanforlini, B.M.; Ceolin, C.; Trevisan, C.; Alessi, A.; Seccia, D.M.; Noale, M.; Maggi, S.; Guarnieri, G.; Vianello, A.; Sergi, G. Clinical trial on the effects of oral magnesium supplementation in stable-phase COPD patients. Aging Clin. Exp. Res. 2021, 34, 167–174. [Google Scholar] [CrossRef]
- Mousavi, R.; Alizadeh, M.; Jafarabadi, M.A.; Heidari, L.; Nikbakht, R.; Rezaei, H.B.; Karandish, M. Effects of Melatonin and/or Magnesium Supplementation on Biomarkers of Inflammation and Oxidative Stress in Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2021, 200, 1010–1019. [Google Scholar] [CrossRef]
- Rose-John, S. Interleukin-6 Family Cytokines. Cold Spring Harb. Perspect. Biol. 2018, 10, a028415. [Google Scholar] [CrossRef] [Green Version]
- Padron-Monedero, A.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Dietary micronutrients intake and plasma fibrinogen levels in the general adult population. Sci. Rep. 2021, 11, 1–9. [Google Scholar]
- Nielsen, F.H. Magnesium deficiency and increased inflammation: Current perspectives. J. Inflamm. Res. 2018, 11, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libako, P.; Nowacki, W.; Rock, E.; Rayssiguier, Y.; Mazur, A. Phagocyte priming by low magnesium status: Input to the enhanced inflammatory and oxidative stress responses. Magnes. Res. 2010, 23, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.; Tsai, P.; Hung, Y.; Huang, C. L-type calcium channels are involved in mediating the anti-inflammatory effects of magnesium sulphate. Br. J. Anaesth. 2010, 104, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, J.; Romani, A.M.; Valentin-Torres, A.M.; Luciano, A.A.; Kitchen, C.M.R.; Funderburg, N.; Mesiano, S.; Bernstein, H.B. Magnesium decreases inflammatory cytokine production: A novel innate immunomodulatory mechanism. J. Immunol. 2012, 188, 6338–6346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.; de Oliveira Otto, M.C.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arsenault, K.A.; Yusuf, A.M.; Crystal, E.; Healey, J.S.; Morillo, C.A.; Nair, G.M.; Whitlock, R.P. Interventions for preventing post-operative atrial fibrillation in patients undergoing heart surgery. Cochrane Database Syst. Rev. 2013, 2013, CD003611. [Google Scholar] [CrossRef]
- Wang, L. Role of nitric oxide in regulating cardiac electrophysiology. Exp. Clin. Cardiol. 2001, 6, 167. [Google Scholar]
- Fordyce, A.; Gouliouk, V.; Henkin, R. Age and gender changes in calcium and magnesium metabolism. FASEB J. 2011, 25, 766–768. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Magnesium | Placebo | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author, Year | Country | Condition | Inflammatory Parameters | Daily Mg Doses (mg) | Type of Mg | Follow-Up (Weeks) | Sample Size | Age (SD) (Years) | Women (%) | BMI (SD) | Sample Size | Age (SD) (Years) | Women (%) | BMI (SD) |
| Alonso, 2020 [34] | USA | Cardiovascular Diseases | CRP, NO, TAC, GSH, MDA, Tartrate-resistant acid phosphatase type 5, ST2 protein, Interleukin-1 receptor type 1 | 400 | Oxide | 10 | 24 | 62 ± 5 | 88 | 28.3 ± 5.01 | 28 | 62 ± 6 | 61 | 27.8 ± 4.2 |
| Asemi, 2015 [17] | Iran | Pregnancy | CRP, NO, TAC, MDA | 250 | Oxide | 6 | 35 | 29.1 ± 4.6 | 100 | 29.6 ± 5.4 | 35 | 29.4 ± 3.1 | 100 | 29.1 ± 3.5 |
| Chacko, 2010 [25] | USA | Overweight | CRP, IL-6, TNF-alfa | 500 | Citrate | 4 | 13 | 47 ± 13.8 | 43 | 28.3 ± 1.6 | 13 | 41.9 ± 12.7 | 24 | 28.1 ± 2.2 |
| Cosaro, 2014 [28] | Italy | Family history of metabolic syndrome | CRP | 368 | Pidolate | 8 | 8 | 6 | ||||||
| Hosseini, 2016 [37] | Iran | Asthma | IL-17 | 340 | Citrate | 8 | 50 | 36.38 ± 9.72 | 50 | 25.6 ± 3.8 | 50 | 34.56 ± 8.28 | 44 | 26.19 ± 3.69 |
| Joris, 2017 [31] | The Netherlands | Overweight/ obese | CRP, IL-6, IL-8, TNF-alfa, amyloid | 350 | Citrate | 24 | 26 | 25 | ||||||
| Kazaks, 2010 [24] | USA | Asthma | CRP | 340 | Citrate | 26 | 27 | 37 ± 2 | 50 | 29 ± 1 | 25 | 37 ± 2 | 61.1 | 28 ± 1 |
| Lima de Souza E Silva, 2014 [29] | Brasil | Metabolic Syndrome | CRP | 400 | Chelate | 12 | 35 | 44.6 ± 9.7 | 35.5 ± 8.2 | 37 | 46.6 ± 12.3 | 35.1 ± 6.3 | ||
| Mortazavi, 2013 [27] | USA | Hemodialysis patients | CRP | 440 | Oxide | 24 | 27 | 56.93 ± 12.19 | 48.3 | 25 | 56.36 ± 11.15 | 48 | ||
| Moslehi, 2012 [36] | Iran | Overweight | CRP, IL-6, fibrinogen | 250 | Oxide | 8 | 35 | 100 | 27.9 ± 3.2 | 34 | 100 | 27.9 ± 3 | ||
| Mousavi, 2021 [39] | Iran | Polycystic ovary syndrome | CRP, TAC, MDA, TNF-alfa | 250 | Oxide | 8 | 21 | 25.6 ± 4.9 | 100 | 28.0 ± 3.2 | 20 | 26.2 ± 5.7 | 100 | 26.9 ± 3.8 |
| Razzaghi, 2018 [32] | Iran | Diabetic foot ulcer | CRP, NO, TAC, GSH, MDA, ERS | 250 | Oxide | 12 | 35 | 60.1 ± 11.1 | 37.1 | 28.2 ± 5.2 | 35 | 59 ± 10.1 | 31.4 | 26.3 ± 4.2 |
| Rodriguez-Hernandez, 2010 [35] | Mexico | Obese | CRP | 450 | Chloride | 16 | 19 | 44.2 ± 10.8 | 63.6 | 30.5 ± 4.4 | 19 | 43.2 ± 7.8 | 63.6 | 35.1 ± 7.9 |
| Simental-Mendia, 2012 [26] | Mexico | Prediabetes | CRP, IL-6, IL-10, TNF-alfa | 382 | Chloride | 12 | 11 | 44.2 ± 10.8 | 63.6 | 30.5 ± 4.4 | 11 | 43.2 ± 7.8 | 63.6 | 35.1 ± 7.9 |
| Simental-Mendia, 2014 [30] | Mexico | Prediabetes | CRP | 382 | Chloride | 12 | 29 | 39.8 ± 16 | 55.2 | 30.5 ± 5.7 | 28 | 41.1 ± 13.1 | 60.7 | 30 ± 5.7 |
| Talari, 2019 [33] | Iran | Diabetic hemodialysis | CRP, NO, TAC, GSH, MDA | 250 | Oxide | 24 | 27 | 58.8 ± 10.1 | 51.9 | 27.2 ± 5.6 | 27 | 61.8 ± 10.2 | 55.6 | 26.2 ± 4.4 |
| Zanforlini, 2021 [38] | Italy | Chronic obstructive pulmonary disease | CRP, TNF-alfa | 300 | Citrate | 24 | 21 | 73 ± 8.9 | 24 | 26.9 ± 4.3 | 20 | 72.2 ± 11 | 20.8 | 26.9 ± 3.8 |
| Total | Median = 12 | 447 | 47.1 ± 9.3 | 62.5 | 29.0 ± 4.4 | 442 | 46.8 ± 8.7 | 59.6 | 29.2 ± 4.4 | |||||
| Inflammatory Parameter | Number of Comparisons | Number of Participants | SMD | 95% CI | p Value | I2 | Egger’s Test (p-Value) | |
|---|---|---|---|---|---|---|---|---|
| CRP | 15 | 737 | −0.356 | −0.659 | −0.054 | 0.02 | 74.8 | −0.28 (0.92) |
| IL-6 | 3 | 142 | −0.258 | −1.083 | 0.567 | 0.54 | 81.3 | 0.94 (0.38) |
| NO | 3 | 194 | 0.321 | 0.037 | 0.604 | 0.03 | 0 | 0.67 (0.40) |
| TAC | 4 | 235 | 0.189 | −0.491 | 0.869 | 0.59 | 84.8 | 8.86 (0.53) |
| GSH | 3 | 194 | −0.181 | −0.463 | 0.102 | 0.21 | 0 | 3.00 (0.61) |
| MDA | 3 | 194 | −0.604 | −1.224 | 0.02 | 0.06 | 77.8 | −13.9 (0.68) |
| TNF-a | 3 | 112 | 0.168 | −0.433 | 0.768 | 0.58 | 58.8 | 3.84 (0.68) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veronese, N.; Pizzol, D.; Smith, L.; Dominguez, L.J.; Barbagallo, M. Effect of Magnesium Supplementation on Inflammatory Parameters: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 679. https://doi.org/10.3390/nu14030679
Veronese N, Pizzol D, Smith L, Dominguez LJ, Barbagallo M. Effect of Magnesium Supplementation on Inflammatory Parameters: A Meta-Analysis of Randomized Controlled Trials. Nutrients. 2022; 14(3):679. https://doi.org/10.3390/nu14030679
Chicago/Turabian StyleVeronese, Nicola, Damiano Pizzol, Lee Smith, Ligia J. Dominguez, and Mario Barbagallo. 2022. "Effect of Magnesium Supplementation on Inflammatory Parameters: A Meta-Analysis of Randomized Controlled Trials" Nutrients 14, no. 3: 679. https://doi.org/10.3390/nu14030679
APA StyleVeronese, N., Pizzol, D., Smith, L., Dominguez, L. J., & Barbagallo, M. (2022). Effect of Magnesium Supplementation on Inflammatory Parameters: A Meta-Analysis of Randomized Controlled Trials. Nutrients, 14(3), 679. https://doi.org/10.3390/nu14030679