
Combined Evaluation of Geriatric Nutritional Risk Index and Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis


Abstract
:1. Introduction
2. Materials and Methods
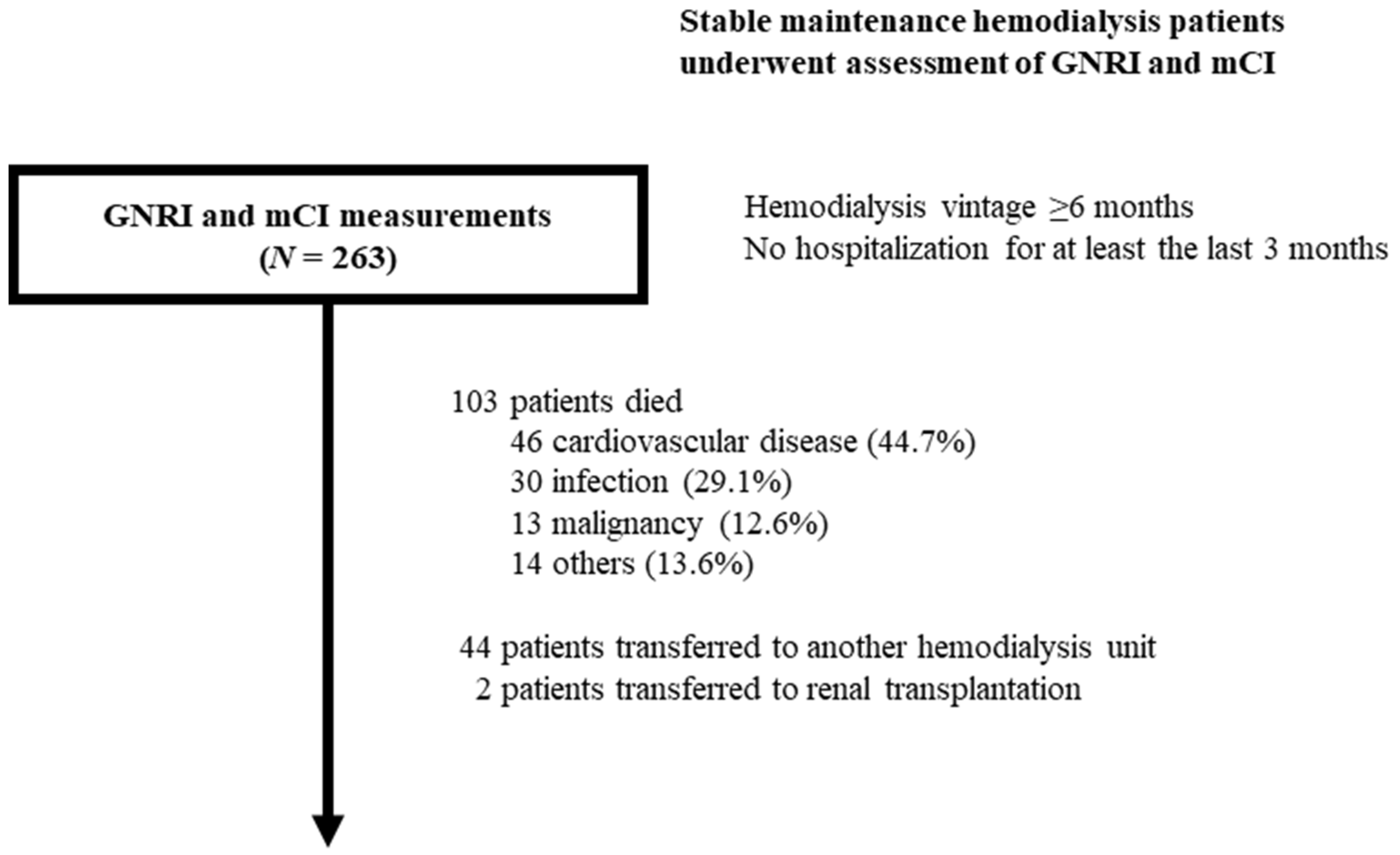
2.1. Study Population
2.2. Collection of Data
2.3. Calculation of Nutritional Indices and Patient Grouping
2.4. Study Endpoint and Patient Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Participants
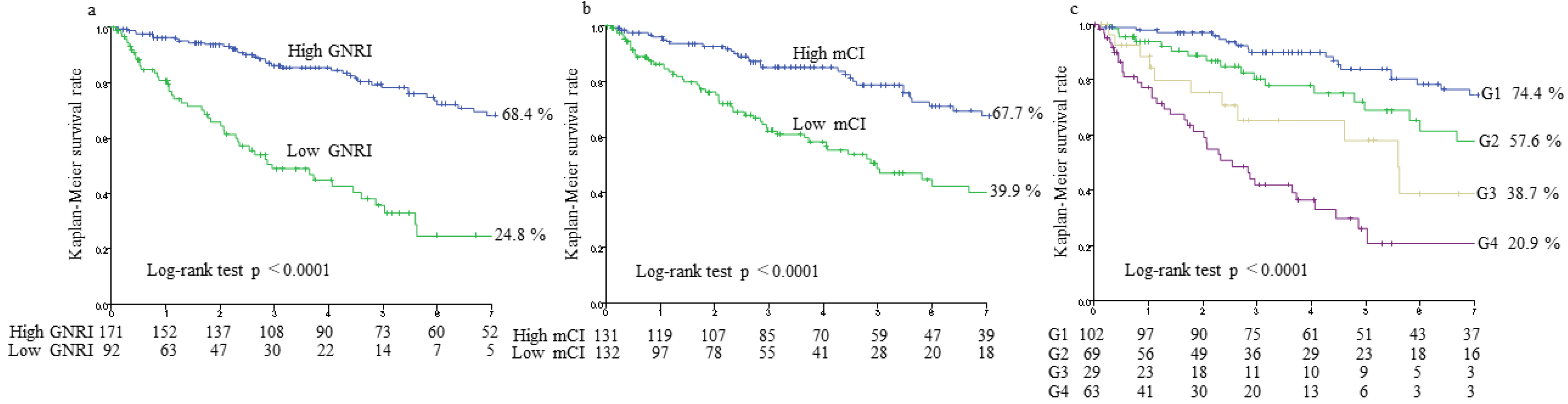
3.2. Associations of GNRI and mCI with All-Cause Mortality
3.3. Model Discrimination in Predicting All-Cause Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A Malnutrition-Inflammation Score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rambod, M.; Bross, R.; Zitterkoph, J.; Benner, D.; Pithia, J.; Colman, S.; Kovesdy, C.P.; Kopple, J.D.; Kalantar-Zadeh, K. Association of malnutrition-inflammation score with quality of life and mortality in hemodialysis patients: A 5-year prospective cohort study. Am. J. Kidney Dis. 2009, 53, 298–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Roij van Zuijdewijn, C.L.; ter Wee, P.M.; Chapdelaine, I.; Bots, M.L.; Blankestijn, P.J.; van den Dorpel, M.A.; Nubé, M.J.; Grooteman, M.P. A comparison of 8 nutrition-related tests to predict mortality in hemodialysis patients. J. Ren. Nutr. 2015, 25, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beberashvili, I.; Azar, A.; Sinuani, I.; Kadoshi, H.; Shapiro, G.; Feldman, L.; Averbukh, Z.; Weissgarten, J. Comparison analysis of nutritional scores for serial monitoring of nutritional status in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 443–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Canaud, B.; Granger Vallée, A.; Molinari, N.; Chenine, L.; Leray-Moragues, H.; Rodriguez, A.; Chalabi, L.; Morena, M.; Cristol, J.P. Creatinine index as a surrogate of lean body mass derived from urea Kt/V, pre-dialysis serum levels and anthropometric characteristics of haemodialysis patients. PLoS ONE 2014, 9, e93286. [Google Scholar]
- Yajima, T. Is modified creatinine index really superior to geriatric nutritional risk index for predicting malnutrition and clinical outcomes in hemodialysis patients? J. Ren. Nutr. 2022, S1051–S2276. [Google Scholar] [CrossRef]
- Kinugasa, Y.; Kato, M.; Sugihara, S.; Hirai, M.; Yamada, K.; Yanagihara, K.; Yamamoto, K. Geriatric nutritional risk index predicts functional dependency and mortality in patients with heart failure with preserved ejection fraction. Circ. J. 2013, 77, 705–711. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Wang, M.; Zhang, Y.; Nie, L.; He, T.; Wang, Y.; Huang, Y.; Feng, B.; Zhang, J.; Zhao, J. Association of geriatric nutritional risk index with mortality in hemodialysis patients: A meta-analysis of cohort studies. Kidney Blood Press. Res. 2018, 43, 1878–1889. [Google Scholar] [CrossRef]
- Huang, C.Y.; Lee, S.Y.; Yang, C.W.; Hung, S.C.; Chiang, C.K.; Huang, J.W.; Hung, K.Y. A simpler creatinine index can predict long-term survival in Chinese hemodialysis patients. PLoS ONE 2016, 11, e0165164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, W.; Cho, M.S.; Oh, J.E.; Lee, J.H.; Jeong, J.C.; Shin, G.T.; Kim, H.; Park, I. Comparison of creatinine index and geriatric nutritional risk index for nutritional evaluation of patients with hemodialysis. Hemodial. Int. 2018, 22, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Arase, H.; Yamada, S.; Yotsueda, R.; Taniguchi, M.; Yoshida, H.; Tokumoto, M.; Nakano, T.; Tsuruya, K.; Kitazono, T. Modified creatinine index and risk for cardiovascular events and all-cause mortality in patients undergoing hemodialysis: The Q-Cohort study. Atherosclerosis 2018, 275, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Yamamoto, S.; Fukuma, S.; Nakano, T.; Tsuruya, K.; Inaba, M. Geriatric nutritional risk index (GNRI) and creatinine index equally predict the risk of mortality in hemodialysis patients: J-DOPPS. Sci. Rep. 2020, 10, 5756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yajima, T.; Yajima, K.; Takahashi, H.; Yasuda, K. Combined predictive value of extracellular fluid/intracellular fluid ratio and the geriatric nutritional risk index for mortality in patients undergoing hemodialysis. Nutrients 2019, 11, 2659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yajima, T.; Yajima, K.; Takahashi, H. Association of the erythropoiesis-stimulating agent resistance index and the geriatric nutritional risk index with cardiovascular mortality in maintenance hemodialysis patients. PLoS ONE 2021, 16, e0245625. [Google Scholar] [CrossRef]
- Liu, J.; Huang, Z.; Gilbertson, D.T.; Foley, R.N.; Collins, A.J. An improved comorbidity index for outcome analyses among dialysis patients. Kidney Int. 2010, 77, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Beberashvili, I.; Cohen-Cesla, T.; Khatib, A.; Hamad, R.A.; Azar, A.; Stav, K.; Efrati, S. Comorbidity burden may explain adiponectin’s paradox as a marker of increased mortality risk in hemodialysis patients. Sci. Rep. 2021, 11, 9087. [Google Scholar] [CrossRef]
- Delong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Pencina, M.J.; Agostino, R.B.D.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2007, 27, 157–172, discussion 207. [Google Scholar] [CrossRef]
- Yajima, T.; Yajima, K.; Takahashi, H.; Yasuda, K. The impact of abdominal fat levels on all-cause mortality risk in patients undergoing hemodialysis. Nutrients 2018, 10, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yajima, T.; Arao, M.; Yajima, K.; Takahashi, H.; Yasuda, K. The associations of fat tissue and muscle mass indices with all-cause mortality in patients undergoing hemodialysis. PLoS ONE 2019, 14, e0211988. [Google Scholar] [CrossRef] [PubMed]
- Yajima, T.; Arao, M.; Yajima, K.; Takahashi, H. Usefulness of computed tomography-measured psoas muscle thickness per height for predicting mortality in patients undergoing hemodialysis. Sci. Rep. 2021, 11, 19070. [Google Scholar] [CrossRef] [PubMed]
- Yajima, T.; Yajima, K.; Takahashi, H. Annual change in the extracellular fluid/intracellular fluid ratio and mortality in patients undergoing maintenance hemodialysis. Sci. Rep. 2022, 12, 242. [Google Scholar] [CrossRef] [PubMed]
- Yajima, T.; Yajima, K.; Takahashi, H. Impact of annual change in geriatric nutritional risk index on mortality in patients undergoing hemodialysis. Nutrients 2020, 12, 3333. [Google Scholar] [CrossRef]
- Chen, J.; Qin, X.; Li, Y.; Yang, Y.; Yang, S.; Lu, Y.; Zhao, Y.; He, Y.; Li, Y.; Lei, Z.; et al. Comparison of three nutritional screening tools for predicting mortality in maintenance hemodialysis patients. Nutrition 2019, 67, 110532. [Google Scholar] [CrossRef]
- Canaud, B.; Ye, X.; Usvyat, L.; Kooman, J.; van der Sande, F.; Raimann, J.; Wang, Y.; Kotanko, P. Clinical and predictive value of simplified creatinine index used as muscle mass surrogate in end-stage kidney disease haemodialysis patients-results from the international MONitoring Dialysis Outcome initiative. Nephrol. Dial. Transplant. 2020, 35, 2161–2171. [Google Scholar] [CrossRef]
- Yamamoto, S.; Matsuzawa, R.; Hoshi, K.; Suzuki, Y.; Harada, M.; Watanabe, T.; Isobe, Y.; Imamura, K.; Osada, S.; Yoshida, A.; et al. Modified creatinine index and clinical outcomes of hemodialysis patients: An indicator of sarcopenia? J. Ren. Nutr. 2021, 31, 370–379. [Google Scholar] [CrossRef]
- Tsai, M.T.; Tseng, W.C.; Ou, S.M.; Lee, K.H.; Yang, C.Y.; Tarng, D.C. Comparison of simplified creatinine index and systemic inflammatory markers for nutritional evaluation of hemodialysis patients. Nutrients 2021, 30, 1870. [Google Scholar] [CrossRef]
- Arase, H.; Yamada, S.; Hiyamuta, H.; Taniguchi, M.; Tokumoto, M.; Tsuruya, K.; Nakano, T.; Kitazono, T. Modified creatinine index and risk for long-term infection-related mortality in hemodialysis patients: Ten-year outcomes of the Q-Cohort study. Sci. Rep. 2020, 10, 1241. [Google Scholar] [CrossRef] [Green Version]
- Robinson, B.M.; Bieber, B.; Pisoni, R.L.; Port, F.K. Dialysis Outcomes and Practice Patterns Study (DOPPS): Its strengths, limitations, and role in informing practices and policies. Clin. J. Am. Soc. Nephrol. 2012, 7, 1897–1905. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Patients (N = 263) | G1 (N = 102) | G2 (N = 69) | G3 (N= 29) | G4 (N = 63) | p-Value | |
|---|---|---|---|---|---|---|
| Age (years) | 63.8 ± 13.7 | 56.0 ± 14.2 | 66.8 ± 9.1 | 62.4 ± 12.9 | 73.8 ± 9.5 | <0.0001 |
| Men (%) | 66.5 | 76.5 | 59.4 | 82.8 | 50.8 | 0.0009 |
| Underlying renal disease | 0.012 | |||||
| Diabetic nephropathy (%) | 42.6 | 42.7 | 58.9 | 9.1 | 38.8 | |
| Chronic glomerulonephritis (%) | 29.6 | 31.3 | 14.3 | 54.5 | 32.7 | |
| Nephrosclerosis (%) | 20.2 | 19.8 | 16.1 | 27.2 | 22.4 | |
| Others (%) | 7.4 | 6.3 | 10.7 | 9.1 | 6.1 | |
| Type of vascular access | 0.0097 | |||||
| Arteriovenous fistula (%) | 76.4 | 80.4 | 71.0 | 89.7 | 69.8 | |
| Arteriovenous graft (%) | 22.1 | 19.6 | 29.0 | 10.3 | 23.8 | |
| Central venous catheter (%) | 1.5 | 0 | 0 | 0 | 6.3 | |
| Hemodialysis vintage (years) | 1.5 (0.7–4.3) | 3.7 (1.2–6.2) | 1.0 (0.7–2.0) | 2.5 (0.8–5.5) | 0.8 (0.6–1.7) | <0.0001 |
| Alcohol (%) | 25.8 | 25.5 | 29.0 | 34.4 | 19.0 | 0.39 |
| Smoking (%) | 27.8 | 28.4 | 37.7 | 37.9 | 11.1 | 0.0035 |
| Hypertension (%) | 94.3 | 95.1 | 97.1 | 96.6 | 88.9 | 0.18 |
| Comorbidity index | 4.4 ± 3.6 | 3.5 ± 3.5 | 5.6 ± 3.5 | 3.6 ± 3.6 | 4.9 ± 3.3 | 0.0007 |
| Diabetes mellitus (%) | 47.1 | 42.2 | 65.2 | 27.6 | 44.4 | 0.0021 |
| Atherosclerotic/ischemic heart disease (%) | 29.7 | 24.5 | 44.9 | 20.7 | 25.4 | 0.017 |
| Peripheral vascular disease (%) | 14.1 | 10.8 | 20.3 | 10.3 | 14.3 | 0.34 |
| Transient ischemic attack/cerebrovascular accident (%) | 16.7 | 16.7 | 15.9 | 17.2 | 17.5 | 0.99 |
| Congestive heart failure (%) | 57.4 | 44.1 | 72.5 | 48.3 | 66.7 | 0.0006 |
| Other cardiac disease (%) | 23.2 | 17.6 | 29.0 | 13.8 | 30.2 | 0.096 |
| Dysrhythmia (%) | 11.4 | 15.7 | 14.5 | 3.4 | 4.8 | 0.043 |
| Chronic obstructive pulmonary disease (%) | 3.4 | 2.0 | 5.8 | 3.4 | 3.2 | 0.62 |
| Liver disease (%) | 6.1 | 2.9 | 5.8 | 13.8 | 7.9 | 0.19 |
| Gastrointestinal bleeding (%) | 6.5 | 3.9 | 7.2 | 10.3 | 7.9 | 0.54 |
| Cancer (%) | 13.3 | 6.9 | 15.9 | 6.9 | 23.8 | 0.012 |
| RAS inhibitor usage (%) | 57.8 | 56.9 | 62.3 | 62.1 | 52.4 | 0.66 |
| Statin usage (%) | 44.1 | 46.0 | 53.6 | 31.0 | 36.5 | 0.10 |
| Height (cm) | 161 ± 9 | 163 ± 8 | 159 ± 8 | 164 ± 8 | 157 ± 9 | <0.0001 |
| Dry weight (kg) | 57.6 ± 13.4 | 62.1 ± 13.1 | 61.4 ± 12.2 | 54.2 ± 12.6 | 47.7 ± 9.2 | <0.0001 |
| Body mass index (kg/m2) | 22.1 ± 4.2 | 23.1 ± 3.8 | 24.1 ± 3.9 | 19.9 ± 3.3 | 19.4 ± 3.5 | <0.0001 |
| Blood urea nitrogen (mg/dL) | 56.7 ± 14.2 | 62.7 ± 12.8 | 52.2 ± 11.8 | 57.5 ± 12.7 | 51.5 ± 15.7 | <0.0001 |
| Creatinine (mg/dL) | 9.0 ± 3.1 | 11.6 ± 2.2 | 6.8 ± 1.8 | 10.7 ± 1.3 | 6.5 ± 1.7 | <0.0001 |
| Alb (g/dL) | 3.6 ± 0.4 | 3.9 ± 0.3 | 3.8 ± 0.3 | 3.3 ± 0.3 | 3.3 ± 0.4 | <0.0001 |
| Hb (g/dL) | 10.6 ± 1.4 | 10.8 ± 1.4 | 10.5 ± 1.2 | 10.4 ± 1.4 | 10.3 ± 1.5 | 0.23 |
| Total cholesterol (mg/dL) | 148 ± 33 | 149 ± 33 | 159 ± 35 | 135 ± 30 | 141 ± 30 | 0.0013 |
| Uric acid (mg/dL) | 6.9 ± 1.7 | 7.4 ± 1.8 | 6.7 ± 1.5 | 6.7 ± 1.7 | 6.4 ± 1.8 | 0.0051 |
| Ca (mg/dL) | 8.9 ± 0.8 | 9.2 ± 0.7 | 8.7 ± 0.6 | 8.6 ± 0.8 | 8.7 ± 1.0 | <0.0001 |
| P (mg/dL) | 4.9 ± 1.4 | 5.4 ± 1.5 | 4.5 ± 1.0 | 5.3 ± 1.0 | 4.4 ± 1.3 | <0.0001 |
| Intact parathyroid hormone (pg/mL) | 115 (51–183) | 116 (50–186) | 126 (67–185) | 115 (58–211) | 100 (29–169) | 0.59 |
| Glucose (mg/dL) | 144 ± 62 | 144 ± 66 | 160 ± 71 | 130 ± 44 | 132 ± 47 | 0.046 |
| CRP (mg/dL) | 0.15 (0.06–0.43) | 0.13 (0.06–0.28) | 0.12 (0.06–0.35) | 0.54 (0.11–1.12) | 0.21 (0.07–1.30) | 0.0050 |
| spKt/V for urea | 1.34 ± 0.29 | 1.32 ± 0.28 | 1.27 ± 0.28 | 1.43 ± 0.28 | 1.40 ± 0.31 | 0.018 |
| GNRI | 93.1 ± 7.6 | 98.1 ± 3.9 | 96.7 ± 3.5 | 86.0 ± 4.7 | 84.4 ± 6.1 | <0.0001 |
| mCI | 20.2 ± 3.0 | 22.8 ± 2.2 | 18.1 ± 1.4 | 21.6 ± 1.3 | 17.4 ± 1.7 | <0.0001 |
| Univariate Analysis | Multivariate Analysis * | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| GNRI (continuous) | 0.89 (0.87–0.91) | <0.0001 | 0.89 (0.86–0.92) | <0.0001 |
| mCI (continuous) | 0.81 (0.75–0.87) | <0.0001 | 0.83 (0.76–0.90) | <0.0001 |
| Lower GNRI | 4.26 (2.82–6.43) | <0.0001 | 4.96 (3.10–7.94) | <0.0001 |
| Lower mCI | 2.51 (1.68–3.74) | <0.0001 | 1.92 (1.22–3.02) | 0.0047 |
| Cross-classified (vs. G1) | <0.0001 | <0.0001 | ||
| G2 | 1.99 (1.16–3.42) | 0.013 | 1.11 (0.60–2.03) | 0.75 |
| G3 | 3.71 (1.89–7.27) | 0.0001 | 2.75 (1.31–5.76) | 0.0073 |
| G4 | 7.23 (4.25–12.32) | <0.0001 | 7.95 (4.38–14.43) | <0.0001 |
| Variables | C-Index | p-Value | NRI | p-Value | IDI | p-Value |
|---|---|---|---|---|---|---|
| Classical risk factors * | 0.801 (0.748–0.855) | Ref. | Ref. | |||
| + GNRI | 0.828 (0.777–0.878) | 0.061 | 0.399 | 0.0012 | 0.048 | 0.00051 |
| + mCI | 0.822 (0.771–0.872) | 0.083 | 0.391 | 0.0016 | 0.034 | 0.0028 |
| + GNRI and mCI | 0.835 (0.786–0.884) | 0.025 | 0.491 | 0.00006 | 0.058 | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yajima, T.; Yajima, K.; Arao, M. Combined Evaluation of Geriatric Nutritional Risk Index and Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis. Nutrients 2022, 14, 752. https://doi.org/10.3390/nu14040752
Yajima T, Yajima K, Arao M. Combined Evaluation of Geriatric Nutritional Risk Index and Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis. Nutrients. 2022; 14(4):752. https://doi.org/10.3390/nu14040752
Chicago/Turabian StyleYajima, Takahiro, Kumiko Yajima, and Maiko Arao. 2022. "Combined Evaluation of Geriatric Nutritional Risk Index and Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis" Nutrients 14, no. 4: 752. https://doi.org/10.3390/nu14040752
APA StyleYajima, T., Yajima, K., & Arao, M. (2022). Combined Evaluation of Geriatric Nutritional Risk Index and Modified Creatinine Index for Predicting Mortality in Patients on Hemodialysis. Nutrients, 14(4), 752. https://doi.org/10.3390/nu14040752