
Nutrient Intake with Early Progressive Enteral Feeding and Growth of Very Low-Birth-Weight Newborns

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
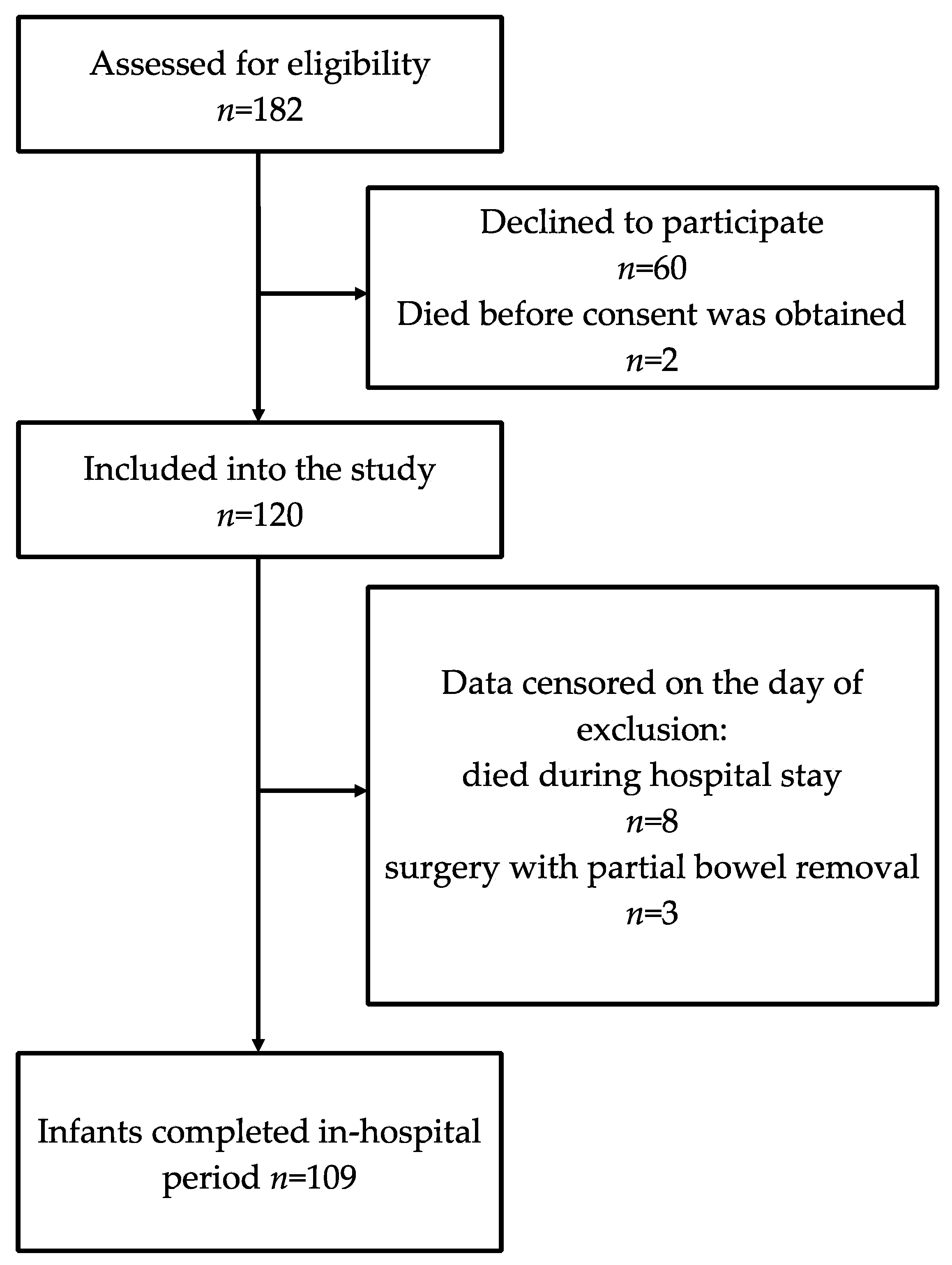
2.1. Study Population
2.2. Nutritional Practices
2.3. Nutritional Calculations
2.4. Anthropometric Measurements
2.5. Data Analysis
3. Results
3.1. Sample Description
3.2. Nutritional Characteristics
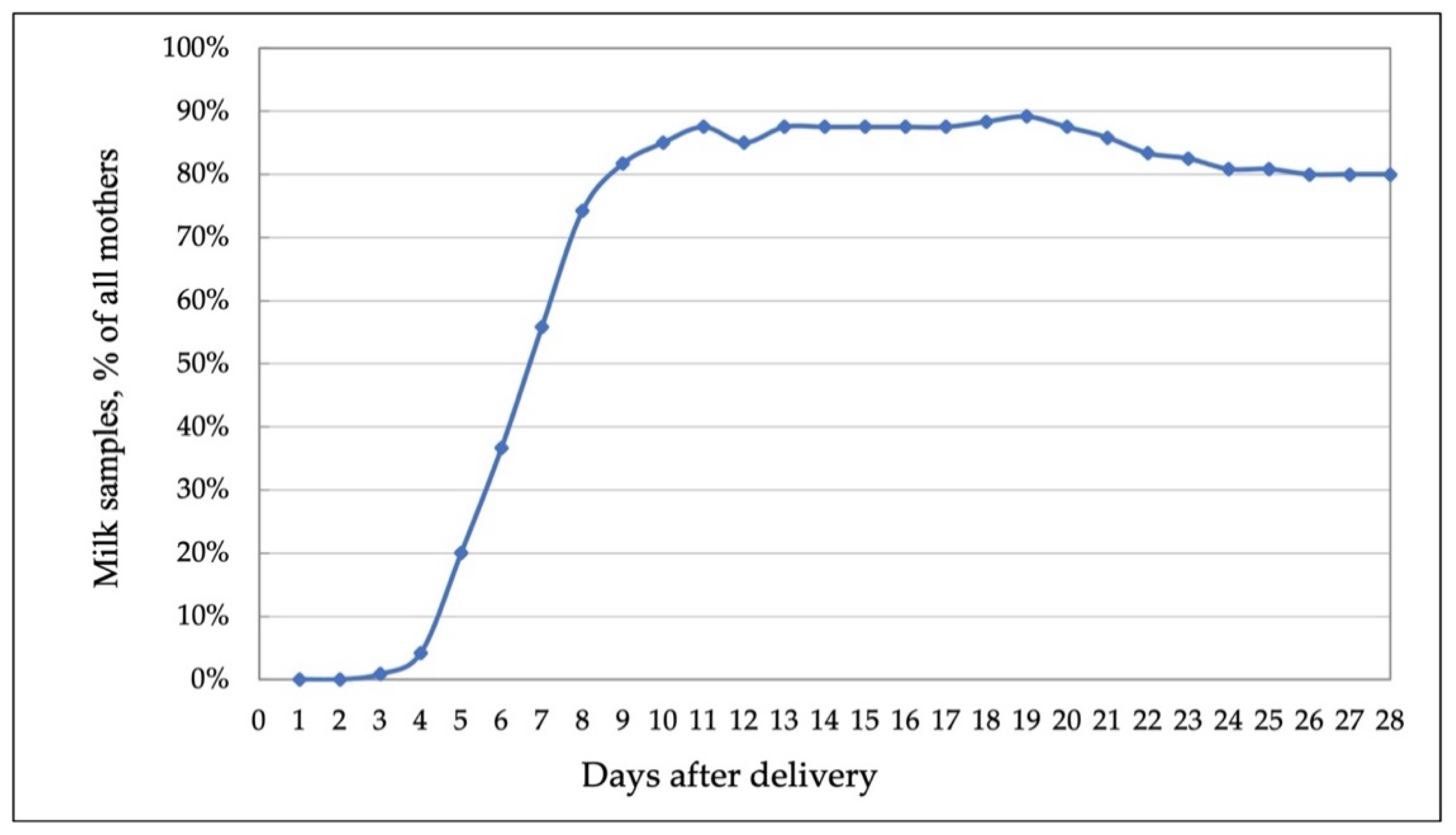
3.3. Availability of Mother’s Milk Data
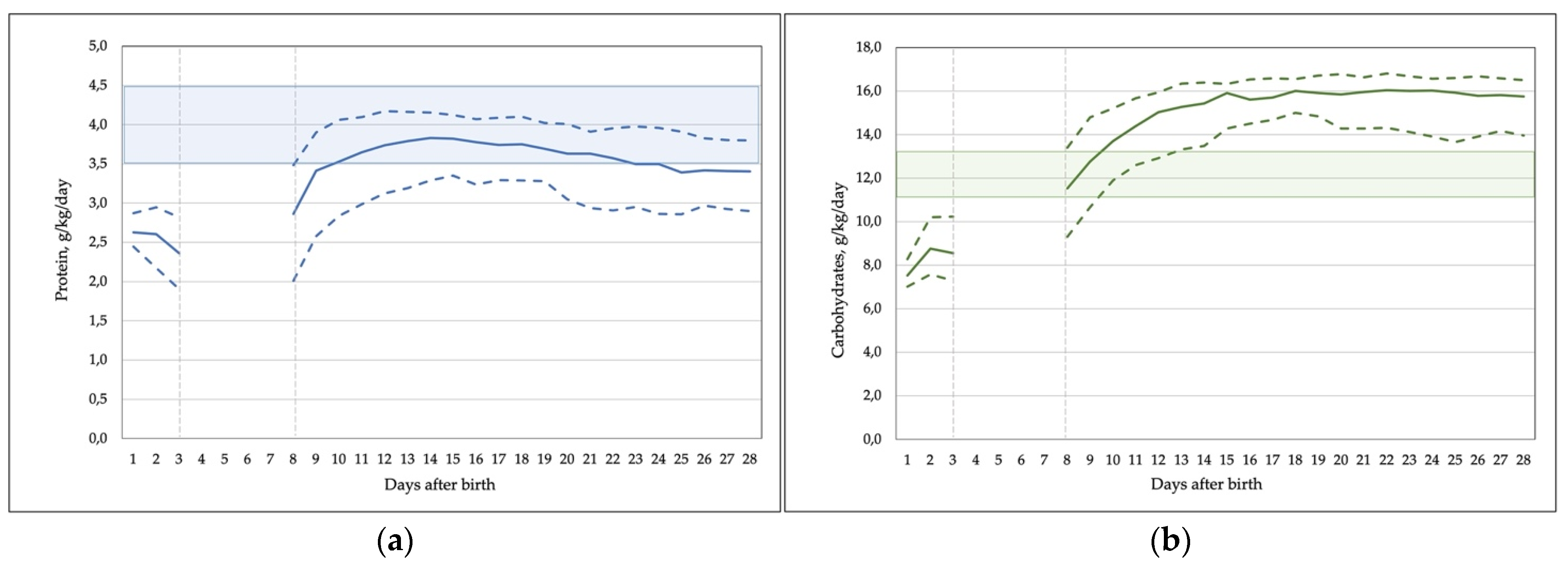
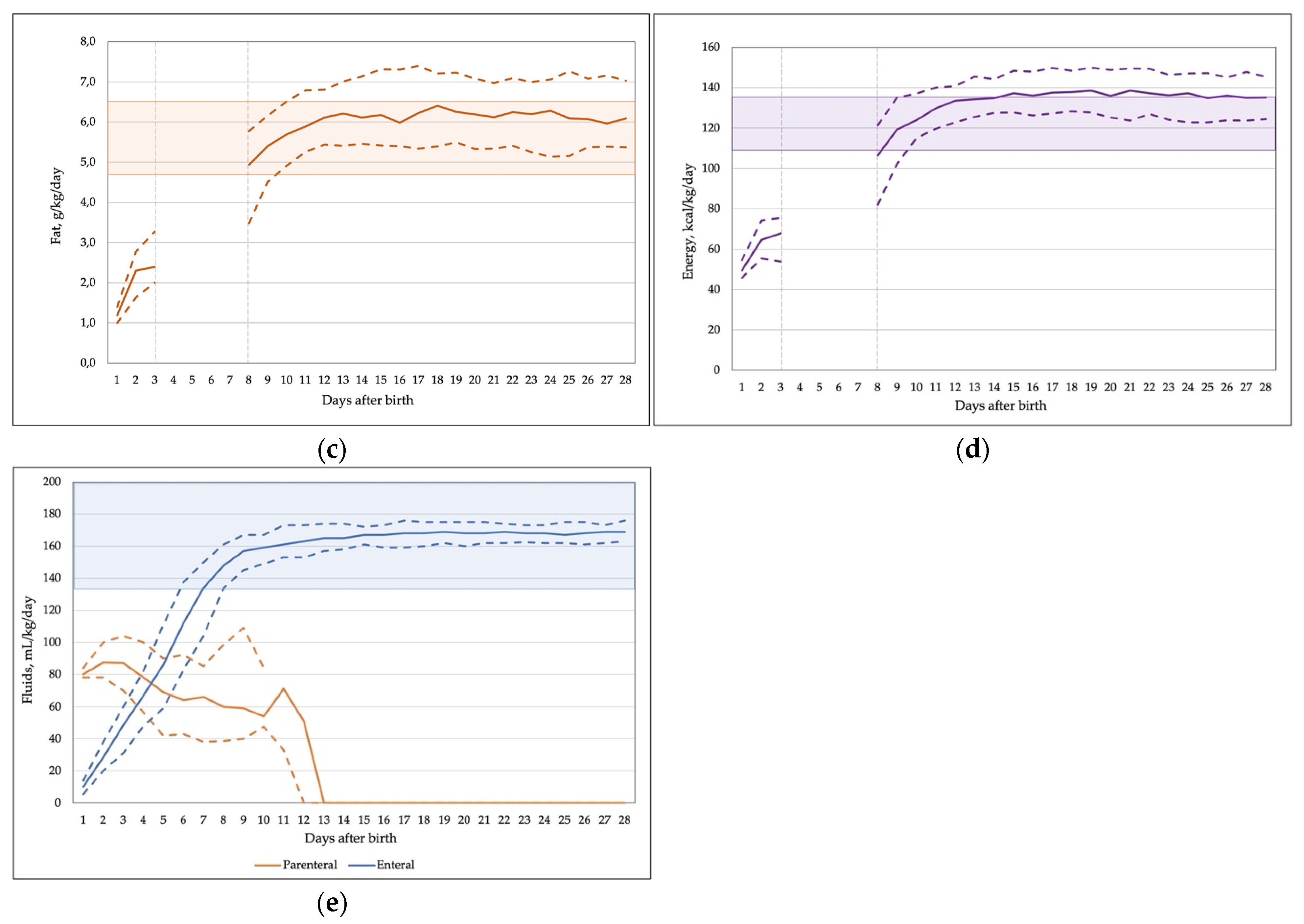
3.4. Daily Intake of Macronutrients and Energy
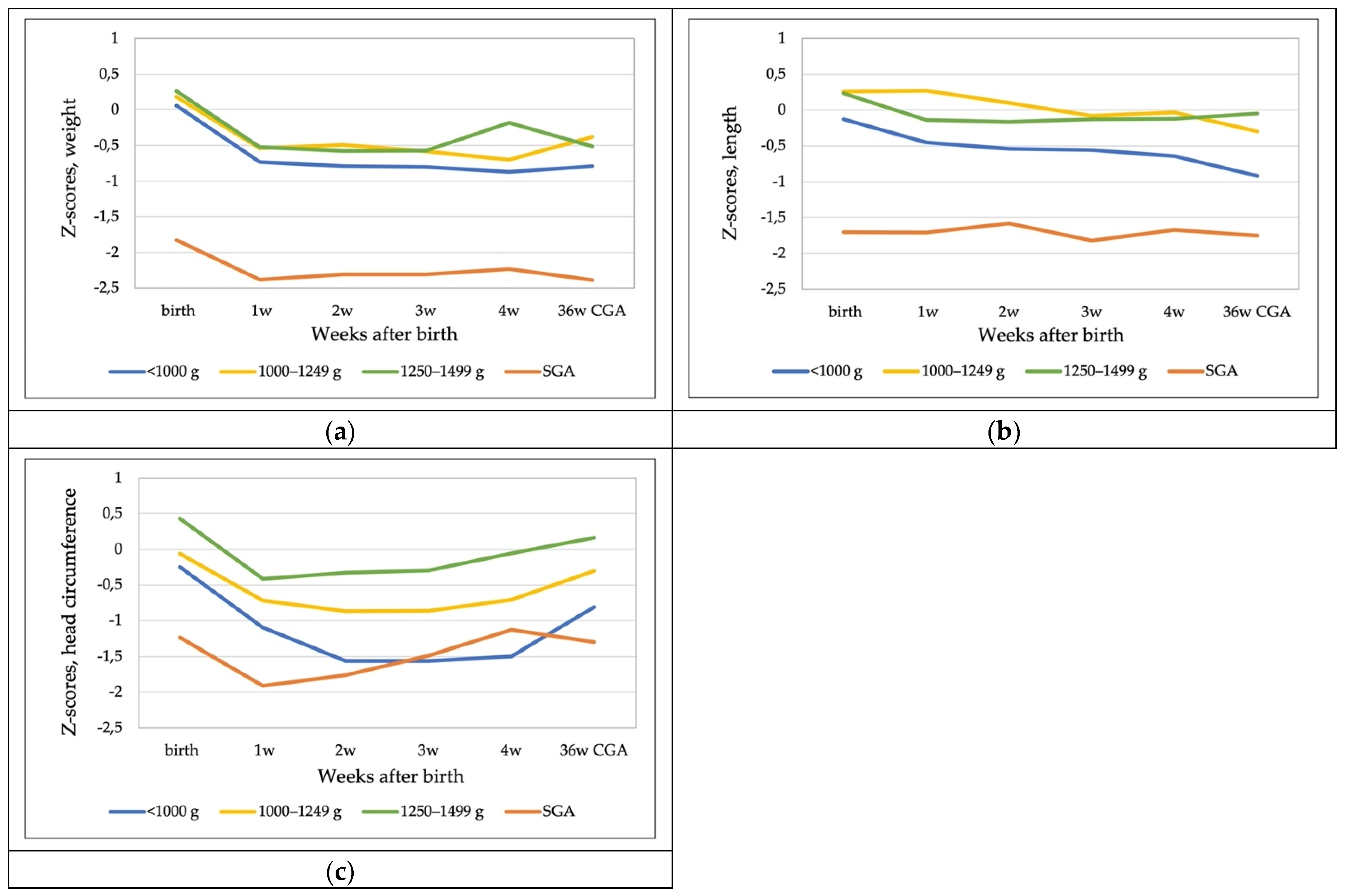
3.5. Growth
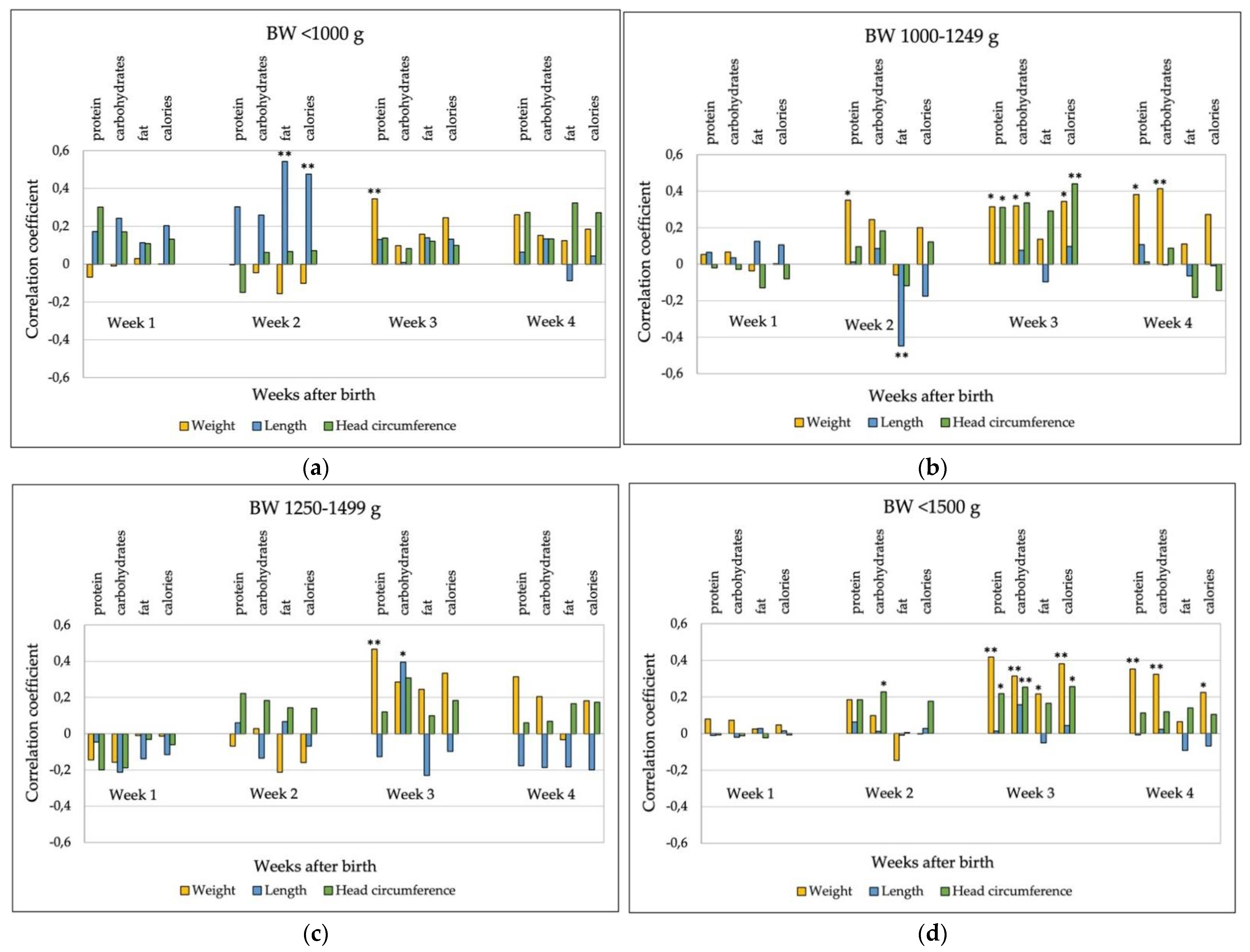
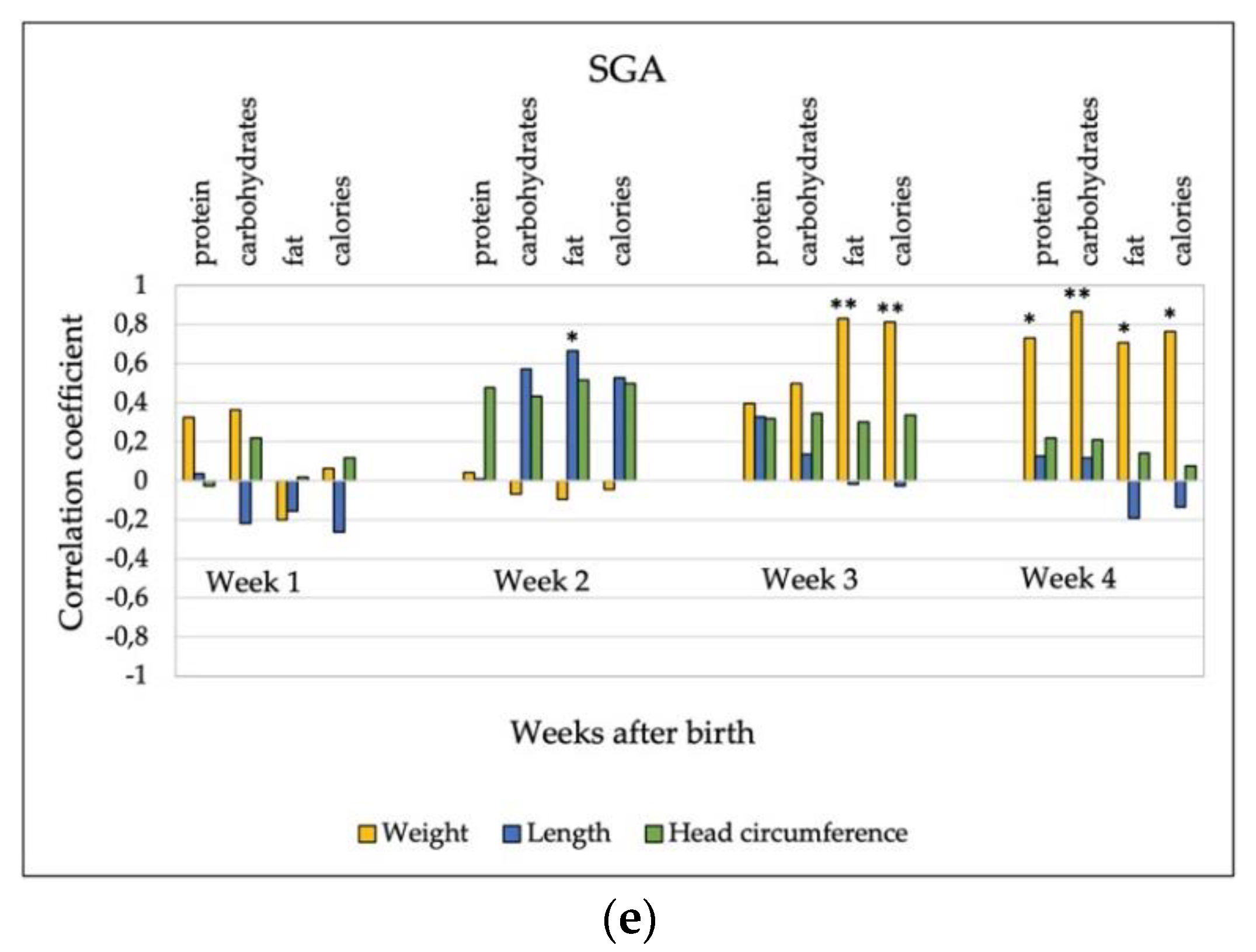
3.6. Relationship between Nutrient Intake and Growth
4. Discussion
4.1. Early Enteral Feeding
4.2. Nutritional Intake
4.3. Growth
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Niklasson, A. Growth from 24 Weeks to 24 Months in Preterm Infants: Experience from a Swedish Population. In Handbook of Growth and Growth Monitoring in Health and Disease; Springer: New York, NY, USA, 2012; pp. 2923–3295. [Google Scholar]
- Vinall, J.; Miller, S.P.; Chau, V.; Brummelte, S.; Synnes, A.R.; Grunau, R.E. Neonatal pain in relation to postnatal growth in infants born very preterm. Pain 2012, 153, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Lima, P.A.T.; de Carvalho, M.; da Costa, A.C.C.; Moreira, M.E.L. Variables associated with extra uterine growth restriction in very low birth weight infants. J. Pediatr. 2014, 90, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.M.; Kim, N.; Namgung, R.; Park, M.S.; Park, K.; Jeon, J. Prediction of Postnatal Growth Failure among Very Low Birth Weight Infants. Sci. Rep. 2018, 8, 3729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cormack, B.E.; Embleton, N.D.; van Goudoever, J.B.; Hay, W.W., Jr.; Bloomfield, F.H. Comparing apples with apples: It is time for standardized reporting of neonatal nutrition and growth studies. Pediatr. Res. 2016, 79, 810–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Waard, M.; Li, Y.; Zhu, Y.; Ayede, A.I.; Berrington, J.; Bloomfield, F.H.; Busari, O.O.; Cormack, B.E.; Embleton, N.; van Goudoever, J.; et al. Time to Full Enteral Feeding for Very Low-Birth-Weight Infants Varies Markedly Among Hospitals Worldwide But May Not Be Associated With Incidence of Necrotizing Enterocolitis: The NEOMUNE-NeoNutriNet Cohort Study. J. Parenter. Enter. Nutr. 2019, 43, 658–667. [Google Scholar] [CrossRef]
- Dutta, S.; Singh, B.; Chessell, L.; Wilson, J.; Janes, M.; McDonald, K.; Shahid, S.; Gardner, V.A.; Hjartarson, A.; Purcha, M.; et al. Guidelines for feeding very low birthweight infants. Nutrients 2015, 7, 423–442. [Google Scholar] [CrossRef] [Green Version]
- Hay, W.W. Optimizing nutrition of the preterm infant. Chin. J. Contemp. Pediatr. 2017, 19, 1–21. [Google Scholar]
- Underwood, M.A. Human Milk for the Premature Infant. Pediatr. Clin. N. Am. 2013, 60, 189–207. [Google Scholar] [CrossRef] [Green Version]
- Oddie, S.J.; Young, L.; McGuire, W. Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst. Rev. 2017, 2017, 1241. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Boquien, C.-Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef]
- Picaud, J.-C.; Houeto, N.; Buffin, R.; Loys, C.-M.; Godbert, I.; Haÿs, S. Additional Protein Fortification Is Necessary in Extremely Low-Birth-Weight Infants Fed Human Milk. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Upadhyay, J.; Singh, P.; Kumar, M. Early versus late fortification of breast milk in preterm infants: A systematic review and meta-analysis. Eur. J. Pediatr. 2020, 179, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Thanigainathan, S.; Abiramalatha, T. Early fortification of human milk versus late fortification to promote growth in preterm infants. Cochrane Database Syst. Rev. 2019, 14, 13392. [Google Scholar] [CrossRef]
- Jochum, F.; Moltu, S.; Senterre, T.; Nomayo, A.; Goulet, O.; Iacobelli, S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Fluid and electrolytes. Clin. Nutr. 2018, 37, 2344–2353. [Google Scholar] [CrossRef] [Green Version]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral Nutrient Supply for Preterm Infants: Commentary From the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef]
- Seigel, J.K.; Smith, P.B.; Ashley, P.L.; Cotten, C.M.; Herbert, C.C.; King, B.A.; Maynor, A.R.; Neill, S.; Wynn, J.; Bidegain, M. Early Administration of Oropharyngeal Colostrum to Extremely Low Birth Weight Infants. Breastfeed. Med. 2013, 8, 491–495. [Google Scholar] [CrossRef] [Green Version]
- The International Fetal and Newborn Growth Consortium International Fetal and Newborn Growth Standards for the 21st Century Anthropometry Handbook. 2012. Available online: https://www.medscinet.net/Intergrowth/patientinfodocs/Anthropometry%20Handbook%20April%202012.pdf (accessed on 29 November 2021).
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- Mečėjus, G. Lithuanian National Birthweight Standards by Gestational Age. Med. Teor. Prakt. 2004, 39, 178–181. [Google Scholar]
- Maas, C.; Mitt, S.; Full, A.; Arand, J.; Bernhard, W.; Poets, C.; Franz, A. A Historic Cohort Study on Accelerated Advancement of Enteral Feeding Volumes in Very Premature Infants. Neonatology 2013, 103, 67–73. [Google Scholar] [CrossRef]
- Salas, A.A.; Li, P.; Parks, K.; Lal, C.V.; Martin, C.R.; Carlo, W.A. Early progressive feeding in extremely preterm infants: A randomized trial. Am. J. Clin. Nutr. 2018, 107, 365–370. [Google Scholar] [CrossRef]
- Shulhan, J.; Dicken, B.; Hartling, L.; Larsen, B.M. Current Knowledge of Necrotizing Enterocolitis in Preterm Infants and the Impact of Different Types of Enteral Nutrition Products. Adv. Nutr. Int. Rev. J. 2017, 8, 80–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsaied, A.; Islam, N.; Thalib, L. Global incidence of Necrotizing Enterocolitis: A systematic review and Meta-analysis. BMC Pediatr. 2020, 20, 344. [Google Scholar] [CrossRef] [PubMed]
- Aldakauskienė, I.; Tamelienė, R.; Marmienė, V.; Rimdeikienė, I.; Šmigelskas, K.; Kėvalas, R. Influence of parenteral nutrition delivery techniques on growth and neurodevelopment of very low birth weight newborns: A randomized trial. Medicina 2019, 55, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, A.-M.; Fenton, S.; Murphy, B.P.; Kiely, M.E. Transition Phase Nutrition Recommendations. J. Parenter. Enter. Nutr. 2017, 53, 343–351. [Google Scholar] [CrossRef]
- Liotto, N.; Amato, O.; Piemontese, P.; Menis, C.; Orsi, A.; Corti, M.G.; Colnaghi, M.; Cecchetti, V.; Pugni, L.; Mosca, F.; et al. Protein Intakes during Weaning from Parenteral Nutrition Drive Growth Gain and Body Composition in Very Low Birth Weight Preterm Infants. Nutrients 2020, 12, 1298. [Google Scholar] [CrossRef]
- Bell, E.; Acarregui, M. Restricted versus liberal water intake for preventing morbidity and mortality in preterm infants. In The Cochrane Database of Systematic Reviews; Bell, E., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2014. [Google Scholar]
- Brennan, A.-M.; Kiely, M.E.; Fenton, S.; Murphy, B.P. Standardized Parenteral Nutrition for the Transition Phase in Preterm Infants: A Bag That Fits. Nutrients 2018, 10, 170. [Google Scholar] [CrossRef] [Green Version]
- Alyahya, W.; Simpson, J.; Garcia, A.L.; Mactier, H.; Edwards, C.A. Early versus Delayed Fortification of Human Milk in Preterm Infants: A Systematic Review. Neonatology 2019, 117, 24–32. [Google Scholar] [CrossRef]
- Hilditch, C.; Keir, A.; Collins, C.T.; Middleton, P.; Gomersall, J. Early versus delayed introduction of human milk fortification in enterally fed preterm infants: A systematic review and meta-analysis. J. Paediatr. Child Health 2021, 58, 30–38. [Google Scholar] [CrossRef]
- Maas, C.; Mathes, M.; Bleeker, C.; Vek, J.; Bernhard, W.; Wiechers, C.; Peter, A.; Poets, C.F.; Franz, A.R. Effect of Increased Enteral Protein Intake on Growth in Human Milk–Fed Preterm Infants: A Randomized Clinical Trial. JAMA Pediatr. 2017, 171, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Reid, J.; Makrides, M.; McPhee, A.J.; Stark, M.J.; Miller, J.; Collins, C.T. The Effect of Increasing the Protein Content of Human Milk Fortifier to 1.8 g/100 mL on Growth in Preterm Infants: A Randomised Controlled Trial. Nutrients 2018, 10, 634. [Google Scholar] [CrossRef] [Green Version]
- Luque, V.; Closa-Monasterolo, R.; Escribano, J.; Ferré, N. Early Programming by Protein Intake: The Effect of Protein on Adiposity Development and the Growth and Functionality of Vital Organs. Nutr. Metab. Insights 2015, 8 (Suppl. S1), 49–56. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Giuliani, F.; Figueras-Aloy, J.; Barros, F.; Bertino, E.; Bhutta, Z.A.; Kennedy, S.H. Growth of preterm infants at the time of global obesity. Arch. Dis. Child. 2019, 104, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Dogra, S.; Thakur, A.; Garg, P.; Kler, N. Effect of differential enteral protein on growth and neurodevelopment in infants <1500 g: A randomized controlled trial. J. Pediatric Gastroenterol. Nutr. 2017, 64, e126–e132. [Google Scholar] [CrossRef]
- Cormack, B.E.; Jiang, Y.; Harding, J.E.; Crowther, C.A.; Bloomfield, F.H. Relationships between Neonatal Nutrition and Growth to 36 Weeks’ Corrected Age in ELBW Babies–Secondary Cohort Analysis from the Provide Trial. Nutrients 2020, 12, 760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falciglia, G.H.; Murthy, K.; Holl, J.; Palac, H.L.; Oumarbaeva, Y.; Yadavalli, P.; Woods, D.; Robinson, D.T. Association Between the 7-Day Moving Average for Nutrition and Growth in Very Low Birth Weight Infants. J. Parenter. Enter. Nutr. 2017, 42, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Coviello, C.; Keunen, K.; Kersbergen, K.J.; Groenendaal, F.; Leemans, A.; Peels, B.; Isgum, I.; Viergever, M.A.; De Vries, L.S.; Buonocore, G.; et al. Effects of early nutrition and growth on brain volumes, white matter microstructure, and neurodevelopmental outcome in preterm newborns. Pediatr. Res. 2017, 83, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Horbar, J.D.; Ehrenkranz, R.A.; Badger, G.J.; Edwards, E.M.; Morrow, K.A.; Soll, R.F.; Buzas, J.S.; Bertino, E.; Gagliardi, L.; Bellù, R. Weight Growth Velocity and Postnatal Growth Failure in Infants 501 to 1500 Grams: 2000–2013. Pediatrics 2015, 136, e84–e92. [Google Scholar] [CrossRef] [Green Version]
- Griffin, I.J.; Tancredi, D.J.; Bertino, E.; Lee, H.C.; Profit, J. Postnatal growth failure in very low birthweight infants born between 2005 and 2012. Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Izquierdo Renau, M.; Aldecoa-Bilbao, V.; Balcells Esponera, C.; del Rey Hurtado de Mendoza, B.; Iriondo Sanz, M.; Iglesias-Platas, I. Applying Methods for Postnatal Growth Assessment in the Clinical Setting: Evaluation in a Longitudinal Cohort of Very Preterm Infants. Nutrients 2019, 11, 2772. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.; Tang, Q.; Wang, Y.; Wu, J.; Ruan, H.; Lu, L.; Tao, Y.; Cai, W. Analysis of Nutrition Support in Very Low-Birth-Weight Infants With Extrauterine Growth Restriction. Nutr. Clin. Pract. 2019, 34, 436–443. [Google Scholar] [CrossRef] [Green Version]
- Senterre, T.; Rigo, J. Optimizing Early Nutritional Support Based on Recent Recommendations in VLBW Infants and Postnatal Growth Restriction. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Flidel-Rimon, O.; Raz, M.; Balla, U.; Hofi, L.; Juster-Reicher, A.; Shinwell, E.S. Early, rapidly progressive enteral nutrition promotes growth of very low birth weight (VLBW) infants. J. Matern. Neonatal Med. 2016, 30, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Cormack, B.; Goldberg, D.; Nasser, R.; Alshaikh, B.; Eliasziw, M.; Hay, W.W.; Hoyos, A.; Anderson, D.; Bloomfield, F.; et al. “Extrauterine growth restriction” and “postnatal growth failure” are misnomers for preterm infants. J. Perinatol. 2020, 40, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Greenbury, S.F.; Angelini, E.D.; Ougham, K.; Battersby, C.; Gale, C.; Uthaya, S.; Modi, N. Birthweight and patterns of postnatal weight gain in very and extremely preterm babies in England and Wales, 2008–2019: A cohort study. Lancet Child Adolesc. Health 2021, 5, 719–728. [Google Scholar] [CrossRef]
- Villar, J.; Giuliani, F.; Barros, F.; Roggero, P.; Coronado Zarco, I.A.; Rego, M.A.S.; Ochieng, R.; Gianni, M.L.; Rao, S.; Lambert, A.; et al. Monitoring the Postnatal Growth of Preterm Infants: A Paradigm Change. Pediatrics 2018, 141, e20172467. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, D.L.; Becker, P.J.; Brigham, K.; Carlson, S.; Fleck, L.; Gollins, L.; Sandrock, M.; Fullmer, M.; Van Poots, H.A. Identifying Malnutrition in Preterm and Neonatal Populations: Recommended Indicators. J. Acad. Nutr. Diet. 2018, 118, 1571–1582. [Google Scholar] [CrossRef]
- Rochow, N.; Raja, P.; Liu, K.; Fenton, T.; Landau-Crangle, E.; Göttler, S.; Jahn, A.; Lee, S.; Seigel, S.; Campbell, D.; et al. Physiological adjustment to postnatal growth trajectories in healthy preterm infants. Pediatr. Res. 2016, 79, 870–879. [Google Scholar] [CrossRef]
- Fu, T.T.; Schroder, P.E.; Poindexter, B.B. Macronutrient Analysis of Target-Pooled Donor Breast Milk and Corresponding Growth in Very Low Birth Weight Infants. Nutrients 2019, 11, 1884. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Group 1 (<1000 g) n = 43 | Group 2 (1000–1249 g) n = 43 | Group 3 (1250–1499 g) n = 34 |
|---|---|---|---|
| At birth | |||
| Birth weight, g | 830 (684–910) | 1148 (1084–1204) | 1370 (1311.5–1435) |
| Gestation, weeks | 26 (25–27) | 28 (27–29) | 29 (28–31) |
| Apgar score: 1 min. | 6 (3–8) | 7 (5–8) | 8 (7–8) |
| 5 min. | 8 (6–8) | 8 (7–9) | (8–9) |
| Male | 18 (41.9) | 25 (58.1) | 14 (41.2) |
| SGA: National reference [20] | 14 (32.6) | 10 (23.3) | 2 (5.9) |
| Fenton reference [19] | 6 (14.0) | 4 (9.3) | 2 (5.9) |
| Cesarean section | 20 (46.5) | 21 (48.8) | 21 (61.8) |
| Multiple pregnancy | 9 (20.9) | 10 (23.3) | 10 (29.4) |
| Antenatal steroids, full course | 39 (90.7) | 33 (76.7) | 29 (85.3) |
| Weight Z-score [19] | −0.29 (−1.02–0.46) | 0.05 (−0.7–0.7) | 0.21 (−0.52–0.81) |
| From birth to discharge | |||
| Mechanical ventilation, any | 23 (53.5) | 11 (25.6) | 2 (5.6) |
| Necrotizing enterocolitis, stage II-III/SIP | 6 (14.0) | 1 (2.3) | 1 (2.9) |
| Late onset sepsis | 11 (25.6) | 7 (16.3) | 1 (2.9) |
| Bronchopulmonary dysplasia (O2 at 36 weeks CGA) | 5 (11.6) | 3 (7.0) | 0 (0) |
| ROP, total | 17 (39.5) | 1 (2.3) | 0 (0) |
| laser treatment | 5 (20.9) | 0 (0) | 0 (0) |
| Intraventricular hemorrhage, grade ≥ III | 9 (9.2) | 1 (2.3) | 1 (2.9) |
| CGA at discharge, weeks | 36 (34–36) | 35 (35–36) | 36 (34–36) |
| Characteristics | Group 1 | Group 2 | Group 3 | p-Value * |
|---|---|---|---|---|
| First feeding, hours | 6 (4–8) | 3 (3–5) | 4 (3–5) | <0.001 a,b |
| First colostrum, hours | 9 (5–21) | 5 (3–15) | 8 (5–21) | 0.091 |
| Duration of PN, days | 7 (6–9) | 6 (5–7) | 5 (4–6) | <0.05 a,b,c |
| Donor human milk, days | 2 (1–3) | 3 (2–4) | 4 (3–12) | <0.05 b,c |
| Fortification started, days | 9 (7–10) | 8 (7–9) | 7 (6–8) | <0.01 b,c |
| Days to regain birth weight | 10 (8–14) | 11 (9–12) | 12 (9–14) | 0.359 |
| Time Interval | Parameter | Birth Weight Group | p-Value * | ||
|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 3 | |||
| Week 1 | Weight | −0.65 (−0.84–−0.36) | −0.66 (−0.84–−0.52) | −0.74 (−1.01–−0.59) | 0.06 |
| Length | −0.28 (−0.58–0.02) | 0.07 (−0.49–0.35) | −0.26 (−0.49–0.03) | 0.074 | |
| HC | −0.75 (−1.32–−0.56) | −0.67 (−1.09–−0.39) | −0.83 (−1.20–−0.40) | 0.194 | |
| Week 2 | Weight | −0.01 (−0.09–0.04) | −0.02 (−0.09–0.09) | −0.02 (−0.10–0.11) | 0.749 |
| Length | −0.02 (−0.19–0.18) | −0.15 (−0.44–0.12) | −0.05 (−0.38–0.14) | 0.239 | |
| HC | −0.25 (−0.46–−0.06) | 0.02 (−0.28–0.12) | 0.09 (−0.14–0.23) | <0.05 a,b | |
| Week 3 | Weight | −0.07 (−0.16–0.03) | −0.05 (−0.17–0.07) | 0.05 (−0.10–0.10) | 0.077 |
| Length | −0.19 (−0.35–0.16) | −0.01(−0.26–0.19) | −0.11 (−0.32–0.26) | 0.476 | |
| HC | 0.00 (−0.20–0.16) | 0.01 (−0.14–0.18) | 0.08 (−0.00–0.28) | 0.371 | |
| Week 4 | Weight | −0.06 (−0.10–0.05) | −0.04 (−0.16–0.13) | 0.12 (0.00–0.20) | <0.01 b,c |
| Length | −0.16 (−0.40–0.03) | 0.04 (−0.24–0.28) | 0.03 (−0.20–0.17) | 0.056 | |
| HC | 0.08 (−0.22–0.15) | 0.17 (−0.02–0.32) | 0.25 (0.00–0.38) | 0.013 b | |
| birth to 36 weeks CGA | Weight | −0.64 (−1.41–−0.25) | −0.62 (−1.04–−0.26) | −0.82 (−1.01–−0.33) | 0.812 |
| Length | −0.61 (−1.17–−0.25) | −0.47 (−0.83–0.04) | −0.36 (−0.74–−0.02) | 0.092 | |
| HC | −0.41 (−1.02–−0.02) | −0.04 (−0.78–0.34) | −0.27 (−0.79–0.20) | 0.171 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brinkis, R.; Albertsson-Wikland, K.; Tamelienė, R.; Vinskaitė, A.; Šmigelskas, K.; Verkauskienė, R. Nutrient Intake with Early Progressive Enteral Feeding and Growth of Very Low-Birth-Weight Newborns. Nutrients 2022, 14, 1181. https://doi.org/10.3390/nu14061181
Brinkis R, Albertsson-Wikland K, Tamelienė R, Vinskaitė A, Šmigelskas K, Verkauskienė R. Nutrient Intake with Early Progressive Enteral Feeding and Growth of Very Low-Birth-Weight Newborns. Nutrients. 2022; 14(6):1181. https://doi.org/10.3390/nu14061181
Chicago/Turabian StyleBrinkis, Rasa, Kerstin Albertsson-Wikland, Rasa Tamelienė, Asta Vinskaitė, Kastytis Šmigelskas, and Rasa Verkauskienė. 2022. "Nutrient Intake with Early Progressive Enteral Feeding and Growth of Very Low-Birth-Weight Newborns" Nutrients 14, no. 6: 1181. https://doi.org/10.3390/nu14061181
APA StyleBrinkis, R., Albertsson-Wikland, K., Tamelienė, R., Vinskaitė, A., Šmigelskas, K., & Verkauskienė, R. (2022). Nutrient Intake with Early Progressive Enteral Feeding and Growth of Very Low-Birth-Weight Newborns. Nutrients, 14(6), 1181. https://doi.org/10.3390/nu14061181