
Whey Protein, Leucine- and Vitamin-D-Enriched Oral Nutritional Supplementation for the Treatment of Sarcopenia



Abstract
:1. Introduction
2. Pathophysiology of the Aging Muscle and Rationale for Nutritional Therapy
3. Nutrikinetic and Nutridynamic Studies
4. Efficacy Trials
4.1. MT-ONS in the Community Setting
4.2. MT-ONS in Rehabilitation Units and Care Homes
4.3. MT-ONS in Sarcopenic Obesity
5. Discussion and Conclusion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Available online: https://www.icd10data.com/ICD10CM/Codes/M00-M99/M60-M63/M62-/M62.84 (accessed on 28 March 2022).
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zùniga, C.; Arai, H.; Boirie, Y.; Chen, L.-K.; Fielding, R.A.; Martin, F.C.; Michel, J.-P. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Fusco, D.; Sisto, A.; Ortolani, E.; Savera, G.; Salini, S.; Marzetti, E. Age-related variations of muscle mass, strength and physical performance in community-dwellers: Results from the Milan EXPO survey. J. Am. Med. Dir. Assoc. 2017, 18, 88.e17–88.e24. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Bianchi, L.; Cherubini, A.; Landi, F.; Maggio, M.; Savino, E.; Bandinelli, S.; Ceda, G.P.; Guralnik, J.M.; Zuliani, G.; et al. Prevalence and clinical correlates of sarcopenia in community-dwelling older people: Application of the EWGSOP definition and diagnostic algorithm. J. Gerontol. A. Biol. Sci. Med. Sci. 2014, 69, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Ligthart-Melis, G.C.; Luiking, Y.C.; Kakourou, A.; Cederholm, T.; Maier, A.B.; de van der Schueren, M.A.E. Frailty, Sarcopenia, and Malnutrition Frequently (Co-)occur in Hospitalized Older Adults: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1216–1228. [Google Scholar] [CrossRef]
- Woizischke, J.; van Wijngaarden, J.; van den Berg, C.; Cetinvurek-Yavuz, A.; Diekmann, R.; Luiking, Y.; Bauer, J. Nutritional status and functionality in geriatric rehabilitation patients: A systematic review and meta-analysis. Eur. Geriatr. Med. 2020, 11, 195–207. [Google Scholar] [CrossRef] [Green Version]
- Barazzoni, R.; Bischoff, S.C.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; Van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic obesity: Time to meet the challenge. Clin. Nutr. 2018, 37, 1787–1793. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Guelistan, B.; Bauer, J.; Boirie, Y.; Bruyère Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; Schneider, S.M.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Cereda, E.; Veronese, N.; Caccialanza, R. The final word on nutritional screening and assessment in older persons. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 24–29. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Bernabei, R.; Onder, G.; Marzetti, E. Sarcopenia as the biological substrate of physical frailty. Clin. Geriatr. Med. 2015, 31, 367–374. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Topinkova, E.; Michel, J.P. Understanding sarcopenia as a geriatric syndrome. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 1–7. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Wan, C.S.; Ktoris, K.; Reijnierse, E.M.; Maier, A.B. Sarcopenia Is Associated with Mortality in Adults: A Systematic Review and Meta-Analysis. Gerontology 2021, 27, 1–16. [Google Scholar] [CrossRef]
- Wang, D.X.M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Calvani, R.; Ortolani, E.; Salini, S.; Martone, A.M.; Santoro, L.; Santoliquido, A.; Sisto, A.; Picca, A.; Marzetti, E. The association between sarcopenia and functional outcomes among older patients with hip fracture undergoing in-hospital rehabilitation. Osteoporos Int. 2017, 28, 1569–1576. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Volpato, S.; Zuliani, G.; Maggi, S.; Cesari, M.; Lipnicki, D.M.; Smith, L.; Schofield, P.; Firth, J.; et al. Association between gait speed with mortality, cardiovascular disease and cancer: A systematic review and meta-analysis of prospective cohort studies. J. Am. Med. Dir. Assoc. 2018, 19, 981–988. [Google Scholar] [CrossRef]
- Welsh, C.E.; Celis-Morales, C.; Ho, F.K.; Brown, R.; MacKay, D.F.; Lyall, D.M.; Anderson, J.J.; Pell, J.P.; Gill, J.M.; Sattar, N.; et al. Grip strength and walking pace and cardiovascular disease risk prediction in 406,834 UK Biobank participants. Mayo Clin. Proc. 2020, 95, 879–888. [Google Scholar] [CrossRef]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The Healthcare costs of sarcopenia in the United States. J. Am. Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef]
- Norman, K.; Otten, L. Financial impact of sarcopenia or low muscle mass—A short review. Clin. Nutr. 2019, 38, 1489–1495. [Google Scholar] [CrossRef]
- Gielen, E.; Beckwée, D.; Delaere, A.; De Breucker, S.; Vandewoude, M.; Bautmans, I. Nutritional interventions to improve muscle mass, muscle strength, and physical performance in older people: An umbrella review of systematic reviews and meta-analyses. Nutr. Rev. 2021, 79, 121–147. [Google Scholar] [CrossRef]
- Martínez-Arnau, F.M.; Fonfría-Vivas, R.; Cauli, O. Beneficial Effects of Leucine Supplementation on Criteria for Sarcopenia: A Systematic Review. Nutrients 2019, 11, 2504. [Google Scholar] [CrossRef] [Green Version]
- Wright, J.; Baldwin, C. Oral nutritional support with or without exercise in the management of malnutrition in nutritionally vulnerable older people: A systematic review and meta-analysis. Clin. Nutr. 2018, 37, 1879–1891. [Google Scholar] [CrossRef] [Green Version]
- Martin-Cantero, A.; Reijnierse, E.M.; Gill, B.M.T.; Maier, A.B. Factors influencing the efficacy of nutritional interventions on muscle mass in older adults: A systematic review and meta-analysis. Nutr. Rev. 2021, 79, 315–330. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in elder people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Morley, J.E.; Argiles, J.M.; Evans, W.J.; Bhasin, S.; Cella, D.; Deutz, N.E.P.; Doehner, W.; Fearon, K.C.; Ferrucci, L.; Hellerstein, M.K.; et al. Nutritional recommendations for the management of sarcopenia. J. Am. Med. Dir. Assoc. 2010, 11, 391–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsanos, C.S.; Kobayashi, H.; Sheffield-Moore, M.; Aarsland, A.; Wolfe, R.R. Aging is associated with diminished accretion of muscle proteins after the ingestion of a small bolus of essential amino acids. Am. J. Clin. Nutr. 2005, 82, 1065–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reginster, J.-Y.; Beaudart, C.; Al-Daghri, N.; Avouac, B.; Bauer, J.; Bere, N.; Bruyère, O.; Cerreta, F.; Cesari, M.; Rosa, M.M.; et al. Update on the ESCEO recommendation for the conduct of clinical trials for drugs aiming at the treatment of sarcopenia in older adults. Aging Clin. Exp. Res. 2021, 33, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1772–1774. [Google Scholar] [CrossRef] [PubMed]
- Borack, M.S.; Volpi, E. Efficacy and safety of leucine supplementation in the elderly. J. Nutr. 2016, 146, 2625S–2629S. [Google Scholar] [CrossRef] [Green Version]
- Szwiega, S.; Pencharz, P.B.; Rafii, M.; Lebarron, M.; Chang, J.; Ball, R.O.; Kong, D.; Xu, L.; Elango, R.; Courtney-Martin, G. Dietary leucine requirement of older men and women is higher than current recommendations. Am. J. Clin. Nutr. 2021, 113, 410–419. [Google Scholar] [CrossRef]
- Boirie, Y.; Guillet, C. Fast digestive proteins and sarcopenia of aging. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 37–41. [Google Scholar] [CrossRef]
- Xu, Z.; Tan, Z.; Zhang, Q.; Gui, Q.; Yang, Y. The effectiveness of leucine on muscle protein synthesis, lean body mass and leg lean mass accretion in older people: A systematic review and meta-analysis. Br. J. Nutr. 2015, 113, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Seelaender, M.; Sotiropoulos, A.; Coletti, D.; Lancha, A.H., Jr. Vitamin D, muscle recovery, sarcopenia, cachexia, and muscle atrophy. Nutrition 2019, 60, 66–69. [Google Scholar] [CrossRef]
- Salles, J.; Chanet, A.; Giraudet, C.; Patrac, V.; Pierre, P.; Jourdan, M.; Luiking, Y.C.; Verlaan, S.; Migné, C.; Boirie, Y.; et al. 1,25(OH)2-vitamin D3 enhances the stimulating effect of leucine and insulin on protein synthesis rate through Akt/PBK and mTOR mediated pathways in murine C2C12 skeletal myotubes. Mol. Nutr. Food Res. 2013, 57, 2137–2146. [Google Scholar] [CrossRef]
- Beaudart, C.; Buckinx, F.; Rabenda, V.; Gillain, S.; Cavalier, E.; Slomian, J.; Petermans, J.; Reginster, J.-Y.; Bruyère, O. The effects of vitamin D on skeletal muscle strength, muscle mass and muscle power: A systematic review and meta-analysis of randomized controlled trials. J. Clin. Endocrinol. Metab. 2014, 99, 4336–4345. [Google Scholar] [CrossRef] [Green Version]
- Dhesi, J.K.; Jackson, S.H.D.; Bearne, L.M.; Moniz, C.; Hurley, M.V.; Swift, C.G.; Allain, T.J. Vitamin D supplementation improves neuromuscular function in older people who fall. Ageing 2004, 33, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Yang, A.; Lv, Q.; Chen, F.; Wang, Y.; Liu, Y.; Shi, W.; Liu, Y.; Wang, D. The effect of vitamin D on sarcopenia depends on the level of physical activity in older adults. J. Cachexia Sarcopenia Muscle 2020, 11, 678–689. [Google Scholar] [CrossRef]
- Pennings, B.; Boirie, Y.; Senden, J.M.G.; Gijsen, A.P.; Kuipers, H.; van Loon, L.J.C. Whey protein stimulates postprandial muscle protein accretion more effectively than do casein and casein hydrolysate in older men. Am. J. Clin. Nutr. 2011, 93, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Luiking, Y.C.; Deutz, N.E.P.; Memelink, R.G.; Verlaan, S.; Wolfe, R.R. Postprandial muscle protein synthesis is higher after a high whey protein, leucine-enriched supplement than after a dairy-like product in healthy older people: A randomized controlled trial. Nutr. J. 2014, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- Luiking, Y.C.; Abrahamse, E.; Ludwig, T.; Boirie, Y.; Verlaan, S. Protein type and caloric density of protein supplements modulate postprandial amino acid profile through changes in gastrointestinal behavior: A randomized trial. Clin. Nutr. 2016, 35, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Kramer, I.F.; Verdijk, L.B.; Hamer, H.M.; Verlaan, S.; Luiking, Y.; Kouw, I.W.K.; Senden, J.M.; Van Kranenburg, J.; Gijsen, A.P.; Poeze, M.; et al. Impact of the macronutrient composition of a nutritional supplement on muscle protein synthesis rates in older men: A randomized, double blind, controlled trial. J. Clin. Endocrinol. Metab. 2015, 100, 4124–4132. [Google Scholar] [CrossRef] [Green Version]
- Kramer, I.F.; Verdijk, L.B.; Hamer, H.M.; Verlaan, S.; Luiking, Y.C.; Kouw, I.W.K.; Senden, J.M.; van Kranenburg, J.; Gijsen, A.P.; Bierau, J.; et al. Both basal and post-prandial muscle protein synthesis rates, following the ingestion of a leucine-enriched whey protein supplement, are not impaired in sarcopenic older males. Clin. Nutr. 2017, 36, 1440–1449. [Google Scholar] [CrossRef]
- Chanet, A.; Verlaan, S.; Salles, J.; Giraudet, C.; Patrac, V.; Pidou, V.; Pouyet, C.; Hafnaoui, N.; Blot, A.; Cano, N.; et al. Supplementing breakfast with a vitamin D and leucine-enriched whey protein medical nutrition drink enhances postprandial muscle protein synthesis and muscle mass in healthy older men. J. Nutr. 2017, 147, 2262–2271. [Google Scholar] [CrossRef] [Green Version]
- van Vliet, S.; Fappi, A.; Reeds, D.N.; Mittendorfer, B. No independent or combined effects of vitamin D and conjugated linoleic acids on muscle protein synthesis in older adults: A randomized, double-blind, placebo-controlled clinical trial. Am. J. Clin. Nutr. 2020, 112, 1382–1389. [Google Scholar] [CrossRef]
- Bothwell, L.E.; Greene, J.A.; Podolski, S.H.; Jones, D.S. Assessing the gold standard—Lessons from the history of RCTs. N. Engl. J. Med. 2016, 374, 2175–2181. [Google Scholar] [CrossRef]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.; Mets, T.; Seal, C.; Wijers, S.L.; et al. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef]
- Barichella, M.; Cereda, E.; Pinelli, G.; Iorio, L.; Caroli, D.; Masiero, I.; Ferri, V.; Cassani, E.; Bolliri, C.; Caronni, S.; et al. Muscle-targeted nutritional support for rehabilitation in patients with parkinsonian syndrome. Neurology 2019, 93, e485–e496. [Google Scholar] [CrossRef]
- Liberman, K.; Njemini, R.; Luiking, Y.; Forti, L.N.; Verlaan, S.; Bauer, J.M.; Memelink, R.; Brandt, K.; Donini, L.M.; Maggio, M.; et al. Thirteen weeks of supplementation of vitamin D and leucine-enriched whey protein nutritional supplement attenuates chronic low-grade inflammation in sarcopenic older adults: The PROVIDE study. Aging Clin. Exp. Res. 2019, 31, 845–854. [Google Scholar] [CrossRef] [Green Version]
- Rondanelli, M.; Cereda, E.; Klersy, C.; Faliva, M.A.; Peroni, G.; Nichetti, M.; Gasparri, C.; Iannello, G.; Spadaccini, D.; Infantino, V. Improving Rehabilitation In Sarcopenia (IRIS) by muscle-targeted food for special medical purposes: A randomized, double-blind, controlled trial. J. Cachexia Sarcopenia Muscle 2020, 11, 1535–1547. [Google Scholar] [CrossRef]
- Hill, T.R.; Verlaan, S.; Biesheuvel, E.; Eastell, R.; Bauer, J.M.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; Mets, T.; et al. A Vitamin D, Calcium and Leucine-Enriched Whey Protein Nutritional Supplement Improves Measures of Bone Health in Sarcopenic Non- Malnourished Older Adults: The PROVIDE Study. Calcif. Tissue Int. 2019, 105, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Bouillanne, O.; Neveux, N.; Nicolis, I.; Curries, E.; Cynober, L.; Aussel, C. Long-lasting improved amino acid bioavailability associated with protein pulse feeding in hospitalized elderly patients: A randomized controlled trial. Nutrition 2014, 30, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Chanet, A.; Salles, J.; Guillet, C.; Giraudet, C.; Berry, A.; Patrac, V.; Domingues-Faria, C.; Tagliaferri, C.; Bouton, K.; Bertrand-Michel, J.; et al. Vitamin D supplementation restores the blunted muscle protein synthesis response in deficient old rats through an impact on ectopic fat deposition. J. Nutr. Biochem. 2017, 46, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Verreijen, A.M.; Verlaan, S.; Engberink, M.F.; Swinkels, S.; de Vogel-van den Bosch, J.; Weijs, P.J.M. A high whey protein-, leucine-, and vitamin D-enriched supplement preserves muscle mass during intentional weight loss in obese older adults: A double-blind randomized controlled trial. Am. J. Clin. Nutr. 2015, 101, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, S.; Maier, A.B.; Bauer, J.M.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.T.; Mets, T.; Seal, C.; et al. Sufficient levels of 25-hydroxyvitamin D and protein intake required to increase muscle mass in sarcopenic older adults—The PROVIDE study. Clin. Nutr. 2018, 37, 551–557. [Google Scholar] [CrossRef]
- Dimori, S.; Leoni, G.; Fior, L.; Gasparotto, F. Clinical nutrition and physical rehabilitation in a long-term care setting: Preliminary observations in sarcopenic older patients. Aging Clin. Exp. Res. 2018, 30, 951–958. [Google Scholar] [CrossRef]
- Chen, N.; Wan, Z.; Han, S.F.; Li, B.Y.; Zhang, Z.L.; Qin, L.Q. Effect of vitamin D supplementation on the level of circulating high-sensitivity C-Reactive Protein: A meta-analysis of randomized controlled trials. Nutrients 2014, 6, 2206–2216. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Xu, J.; Rao, C.; Han, S.; Wan, Z.; Qin, L. Effect of whey supplementation on circulating C-Reactive Protein: A meta-analysis of randomized controlled trials. Nutrients 2015, 7, 1131–1143. [Google Scholar] [CrossRef]
- Memelink, R.G.; Pasman, W.J.; Bongers, A.; Tump, A.; van Ginkel, A.; Tromp, W.; Wopereis, S.; Verlaan, S.; de Vogel-van den Bosch, J.; Weijs, P.J.M. Effect of an Enriched Protein Drink on Muscle Mass and Glycemic Control during Combined Lifestyle Intervention in Older Adults with Obesity and Type 2 Diabetes: A Double-Blind RCT. Nutrients 2020, 13, 64. [Google Scholar] [CrossRef]
- Pasman, W.J.; Memelink, R.G.; de Vogel-Van den Bosch, J.; Begieneman, M.P.V.; van den Brink, W.J.; Weijs, P.J.M.; Wopereis, S. Obese Older Type 2 Diabetes Mellitus Patients with Muscle Insulin Resistance Benefit from an Enriched Protein Drink during Combined Lifestyle Intervention: The PROBE Study. Nutrients 2020, 12, 2979. [Google Scholar] [CrossRef]
- Lewis, R.; Gomez Alvarez, C.B.; Rayman, M.; Lanham-New, S.; Woolf, A.; Mobashei, A. Strategies for optimizing musculoskeletal health in the 21st century. BMC Musculoskelet. Disord. 2019, 20, 164. [Google Scholar] [CrossRef] [Green Version]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Crutz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [Green Version]
- Nussbaumer-Streit, B.; Klerings, I.; Dobrescu, A.I.; Persad, E.; Stevens, A.; Garritty, C.; Kamel, C.; Affengruber, L.; King, V.; Gartlehner, G. Excluding non-English publications from evidence-syntheses did not change conclusions: A meta-epidemiological study. J. Clin. Epidemiol. 2020, 118, 42–54. [Google Scholar] [CrossRef]
- Bauer, J.M.; Mikušová, L.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; Mets, T.; Wijers, S.L.J.; Garthoff, J.A. Safety and tolerability of 6-month supplementation with a vitamin D, calcium and leucine-enriched whey protein medical nutrition drink in sarcopenic older adults. Aging Clin. Exp. Res. 2020, 32, 1501–1514. [Google Scholar] [CrossRef] [Green Version]
- Oesen, S.; Halper, B.; Hofmann, M.; Jandrasits, W.; Franzke, B.; Strasser, E.M.; Graf, A.; Tschan, H.; Bachl, N.; Quittan, M. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly--A randomized controlled trial. Exp. Gerontol. 2015, 72, 99–108. [Google Scholar] [CrossRef]
- Greenhaff, P.L.; Karagounis, L.G.; Peirce, N.; Simpson, E.J.; Hazell, M.; Layfield, R.; Wackerhage, H.; Smith, K.; Atherton, P.; Selby, A.; et al. Disassociation between the effects of amino acids and insulin on signaling, ubiquitin ligases, and protein turnover in human muscle. Am. J. Physiol. Endocrinol. Metab. 2008, 295, E595–E604. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author, Year [Ref] | Study Aim | Study Design | Participants | Experimental Intervention (Dosages) | Control Intervention (None or Description) | Combined Physical Activity Intervention (None or Description) | Findings | Other Findings |
|---|---|---|---|---|---|---|---|---|
| Pennings, 2011 [38] | To compare protein digestion and absorption kinetics and post-prandial muscle protein accretion after ingestion of different protein sources | Randomized, parallel-group trial | Healthy older men (n = 48; age, 74 ± 1 years) | Single bolus of whey protein (20 g) | Single bolus of casein (20 g) or casein hydrolisate (20 g) | None (avoidance any sort of exhaustive physical activity for 3 days before the experiment) |
| Strong positive correlation (r = 0.66; p < 0.01) between peak plasma leucine concentration and post-prandial FSR |
| Luiking, 2014 [39] | To evaluate muscle protein synthesis after ingestion of two different oral nutritional supplements (ONS) and to study the combined effect with resistance exercise, using a unilateral resistance exercise protocol. | Randomized, parallel-group, double-blind trial | Healthy older adults (n = 19; males, 47%; age, 69 ± 6 years) | Single bolus of whey protein (20 g) leucine-enriched (3 g) supplement | Conventional iso-caloric diary product (single bolus containing 6 g of proteins) | Unilateral resistance exercise protocol | FSR: higher after whey protein + leucine vs. control (p = 0.049) | None |
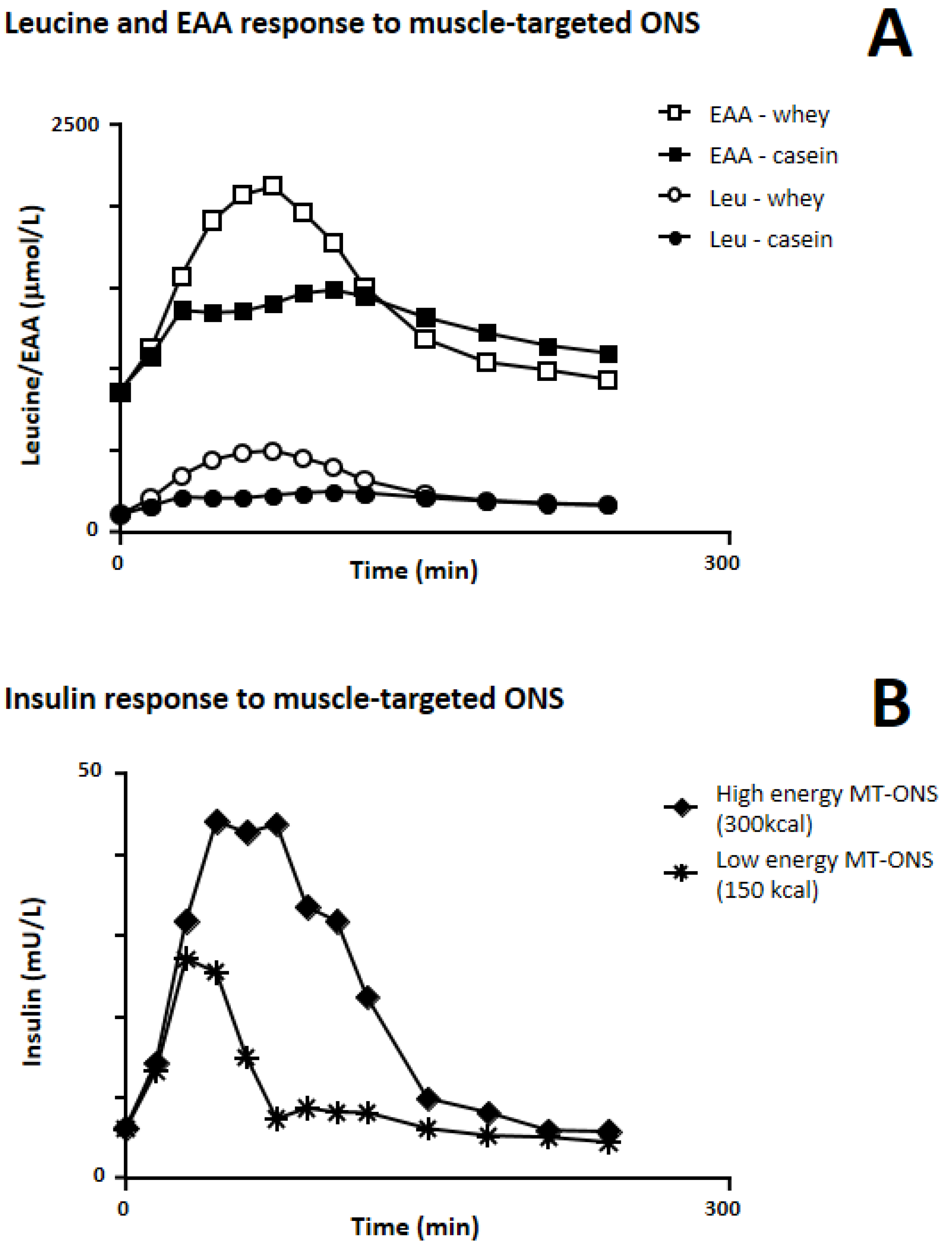
| Luiking, 2016 [40] | To evaluate the impact of ONS with distinct protein source and energy density on serum amino acids (AAs) profile | Randomized, cross-over, single-blind trial | Healthy adults (n = 12; males, 42%; age, 67 ± 2 years) | Single bolus of low-calorie (150 kcal) and high-calorie (300 kcal) whey-protein-based (20 g) ONS | Single bolus of low-calorie (150 kcal) and high-calorie (300 kcal) casein-based (20 g) ONS | None |
| In vitro digestion modelling for 90 min resulted in higher levels of free total AAs, essential AAs and leucine for low-calorie whey protein ONS vs. low-calorie casein ONS, for low-calorie whey protein ONS vs. high-calorie whey protein ONS, and for low-calorie casein ONS vs. high-calorie casein ONS. High-calorie ONS resulted in higher serum insulin concentration vs. low-calorie ONS (p < 0.001) |
| Kramer, 2015 [41] | To determine the impact of the macronutrient composition of ONS on the post-prandial muscle protein synthesis (MPS) rates | Randomized, parallel-group, double-blind trial | Non sarcopenic older men (n = 45; age, 69 ± 1 years) | Single bolus of two different isonitrogenous whey protein (20 g) leucine-enriched ONS containing (150 kcal) or not containing carbohydrate and fat | Protein-free isocaloric mixture (150 kcal) containing carbohydrate and fat | None |
| Insulin levels: greater post-prandial rise after protein-leucine ONS containing calories, but not significantly superior to ONS containing protein-leucine only |
| Kramer, 2017 [42] | To assess basal and post-prandial muscle protein FSR in healthy and sarcopenic subjects | Comparative study of two different patients populations | Healthy adults (n = 15; age, 69 ± 1 years) and sarcopenic older men (n = 15; age, 81 ± 1 years) | Single bolus of a low-calorie (150 kcal) whey protein (20 g) leucine-enriched ONS | None | None |
| None |
| Author, Year | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias |
|---|---|---|---|---|---|---|---|
| PROVIDE study Bauer, 2015 [44] Verlaan, 2018 [45] Liberman, 2019 [46] |  | | | | | |  |
| Verreijen, 2015 [47] | | | | | | | Single-center |
| Rondanelli, 2016 [48] | | | | | | | Single-center |
| Chanet, 2017 [43] | | | | | | | |
| Dimori, 2018 [49] |  | | | | | | Single-center |
| PRO-LEADER study Barichella, 2019 [48] | | | | | | | |
| IRIS study Rondanelli, 2020 [50] | | | | | | | Single-center |
| Author, Year [Ref] | Study Design | Setting | Study Duration | Muscle-Targeted Intervention (Dosages) | Control Intervention (None or Description) | Combined Physical Activity Intervention (None or Description) | Muscle Mass | Physical Performance Endpoints | Physical Function Endpoints | Other Endpoints |
|---|---|---|---|---|---|---|---|---|---|---|
| Bauer, 2015 [46] PROVIDE study (first analysis) | RCT, multi-centre | Community | 13 weeks | Twice daily (21 g whey protein, 3 g leucine and 800 IU vitamin D each serving) for 13 weeks | Isocaloric matched placebo | None | Appendicular muscle mass (Between-group difference of 0.17 kg; p = 0.045) | Handgrip strength (No between- group differences) | SPPB (No between- group differences) Chair stand test (Delta = −1.01 s, p = 0.018); gait speed; balance score | None |
| Verreijen, 2015 [53] | RCT, single-centre | Community | 13 weeks | 10 times/week (21 g whey protein, 3 g leucine and 800 IU of vitamin D each serving) for 13 weeks | Isocaloric matched placebo | Resistance training 3X/week for 13 weeks in both groups | Appendicular muscle mass (+0.4 kg vs. −0.5 kg; p = 0.03) | Handgrip strength (No between-group differences) | 400 m walking test; 4 m gait speed test; chair stand test | Body composition |
| Rondanelli 2016 [54] | RCT, single-centre | Rehabilitation center | 12 weeks | Once daily (22 g whey protein, 4 g leucine and 100 IU of vitamin D each serving) | Isocaloric matched placebo | Controlled physical activity program (20 min exercise session/day, 5 times/week) | Fat free mass (1.7 kg gain; p <0.001); relative skeletal muscle mass (p = 0.009) | Handgrip strength (improved with test product; p = 0.001) | Activities of daily living | Body composition; IGF-1 and PCR; HR-QoL; global nutritional status |
| Chanet, 2017 [43] | RCT, single-centre | Community | 6 weeks | Once daily before breakfast (21 g whey protein, 3 g leucine and 800 IU of vitamin D each serving) for 6 weeks | Non caloric flavored watery placebo | None | Mixed muscle protein synthesis rate(FSR) (higher in the test group; p = 0.001); appendicular lean mass (higher in the test group; p = 0.035) | Handgrip strength (No between- group differences) | SPPB (no between-group differences) | Body composition; blood glucose, insulin, EAA and leucine |
| Verlaan, 2018 [55] PROVIDE study (secondary analysis) | RCT, multi-centre; post hoc analysis | Community | 13 weeks | Twice daily (21 g whey protein, 3 g leucine and 800 IU vitamin D each serving) for 13 weeks | Isocaloric matched placebo | None | Appendicular muscle mass (higher baseline concentrations of 25(OH)D are associated with greater gain in AMM) | None | Chair stand test (no effect of baseline concentrations of 25(OH)D) | None |
| Dimori, 2018 [56] | Observational study: cross-sectional survey (Phase 1) + single-arm intervention trial (Phase 2) | Care home | 6 months on + 3 months off + 3 months on | Twice daily (21 g whey protein, 3 g leucine and 800 IU vitamin D each serving) when administered | None | Patients with Tinetti score >9: 40 min physical therapy session, 3 times/week for 12 months | Skeletal muscle mass | Handgrip strength | SPPB (patients with Tinetti score > 9); gait speed (4 m walking test) | Body composition; sarcopenia prevalence (Phase 1 of the study) |
| Liberman, 2019 [48] PROVIDE study (Tertiary analysis) | RCT, multi-centre | Community | 13 weeks | Twice daily (21 g whey protein, 3 g leucine and 800 IU vitamin D each serving) for 13 weeks | Isocaloric matched placebo | None | IL-8 (higher decrease with the test product; p = 0.03); IL-1RA and IL-6 (no significant between-group differences); sTNFR1; CRP; pre-albumin | |||
| Barichella, 2019 [47] PRO-LEADER study | RCT, pragmatic, bicentric, assessor-blind | Rehabilitation centre for patients with Parkinson’s disease | 30 days | Twice daily (21 g whey protein, 3 g leucine and 800 IU vitamin D each serving) for 30 days | Usual care | Multidisciplinary Intensive Rehabilitation Program (MIRT) | Skeletal muscle mass (increased vs. usual care; p = 0.029) and skeletal muscle index | Handgrip strength | 6 min walking test (+18.1 m vs. usual care; p = 0.039); 4 m walking speed, timed up and go, Berg balance scale (all improved vs. usual care) | |
| Rondanelli, 2020 [49] IRIS study | RCT, single-centre | Rehabilitation centre | Until discharge (at least 4 weeks and up to 8 weeks) | Twice daily (21 g whey protein, 3 g LEU and 800 IU vit. D each serving) for 4-8 weeks | Isocaloric control formula | Controlled physical activity program (20 min exercise session/day, 5 times/week) | Muscle mass (increased vs. control; p <0.03) | Handgrip strength (increased vs. control; p <0.03) | Change in4 m gait speed/month (+0.063 m/sec/month with active vs. control; p <0.001); chair stand test; timed up and go test; SPPB (all improved vs. control; p <0.001) | Cognitive function tests (both improved vs. control; p <0.001); rehabilitation intensity profile (improved vs. control; p = 0.003); probability of being discharged at home (higher vs. control; p = 0.002); overall economic benefit (duration of rehabilitation and length of hospital stay, both improved vs. control; p <0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cereda, E.; Pisati, R.; Rondanelli, M.; Caccialanza, R. Whey Protein, Leucine- and Vitamin-D-Enriched Oral Nutritional Supplementation for the Treatment of Sarcopenia. Nutrients 2022, 14, 1524. https://doi.org/10.3390/nu14071524
Cereda E, Pisati R, Rondanelli M, Caccialanza R. Whey Protein, Leucine- and Vitamin-D-Enriched Oral Nutritional Supplementation for the Treatment of Sarcopenia. Nutrients. 2022; 14(7):1524. https://doi.org/10.3390/nu14071524
Chicago/Turabian StyleCereda, Emanuele, Roberto Pisati, Mariangela Rondanelli, and Riccardo Caccialanza. 2022. "Whey Protein, Leucine- and Vitamin-D-Enriched Oral Nutritional Supplementation for the Treatment of Sarcopenia" Nutrients 14, no. 7: 1524. https://doi.org/10.3390/nu14071524
APA StyleCereda, E., Pisati, R., Rondanelli, M., & Caccialanza, R. (2022). Whey Protein, Leucine- and Vitamin-D-Enriched Oral Nutritional Supplementation for the Treatment of Sarcopenia. Nutrients, 14(7), 1524. https://doi.org/10.3390/nu14071524