
Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Sleep Phases and Duration
1.2. Insomnia and Its Risk Factors
1.3. Functions of Sleep
2. Search Strategy
3. Review
3.1. Diet and Sleep Quality
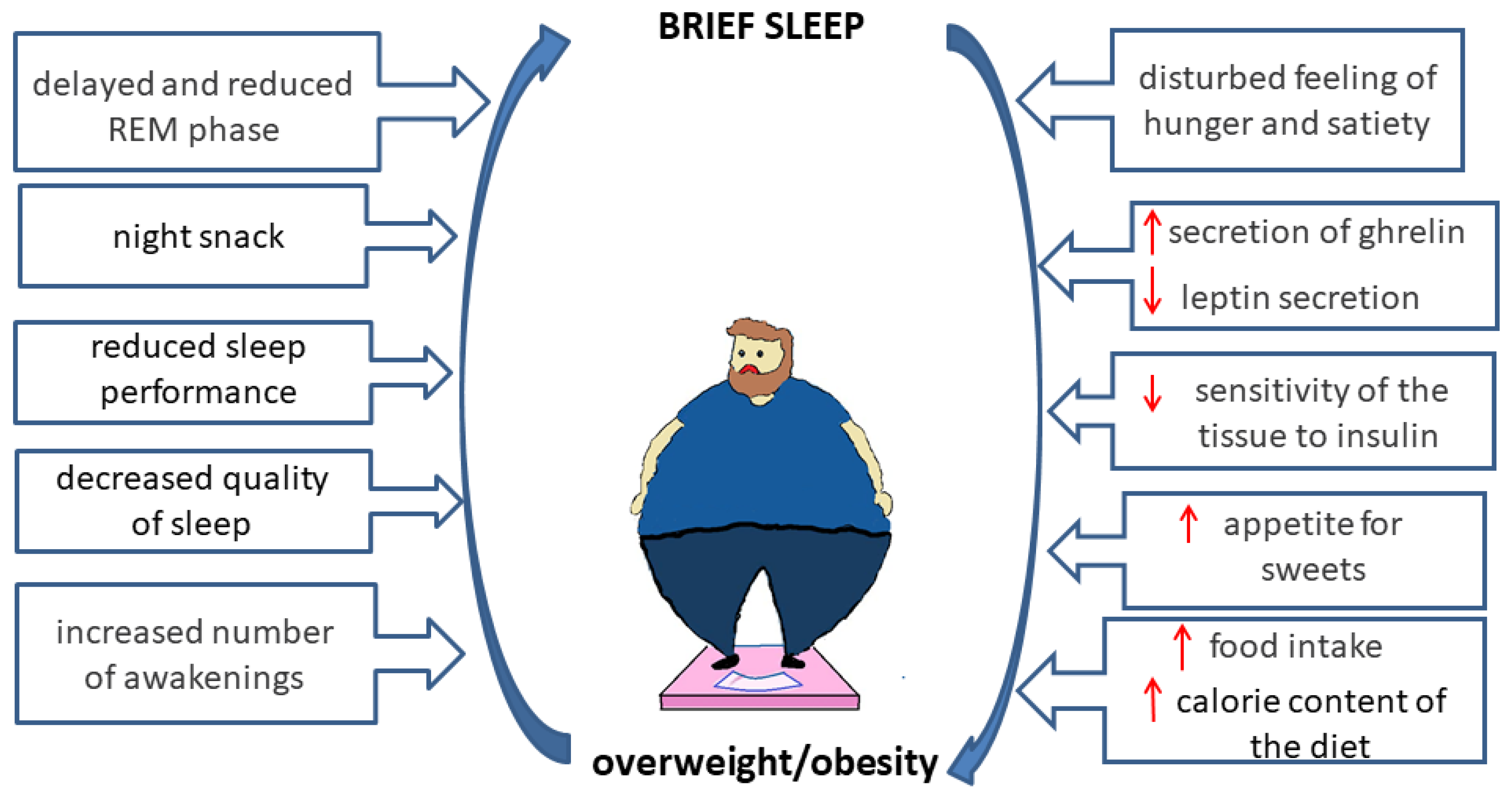
3.1.1. Sleep and Energy Intake
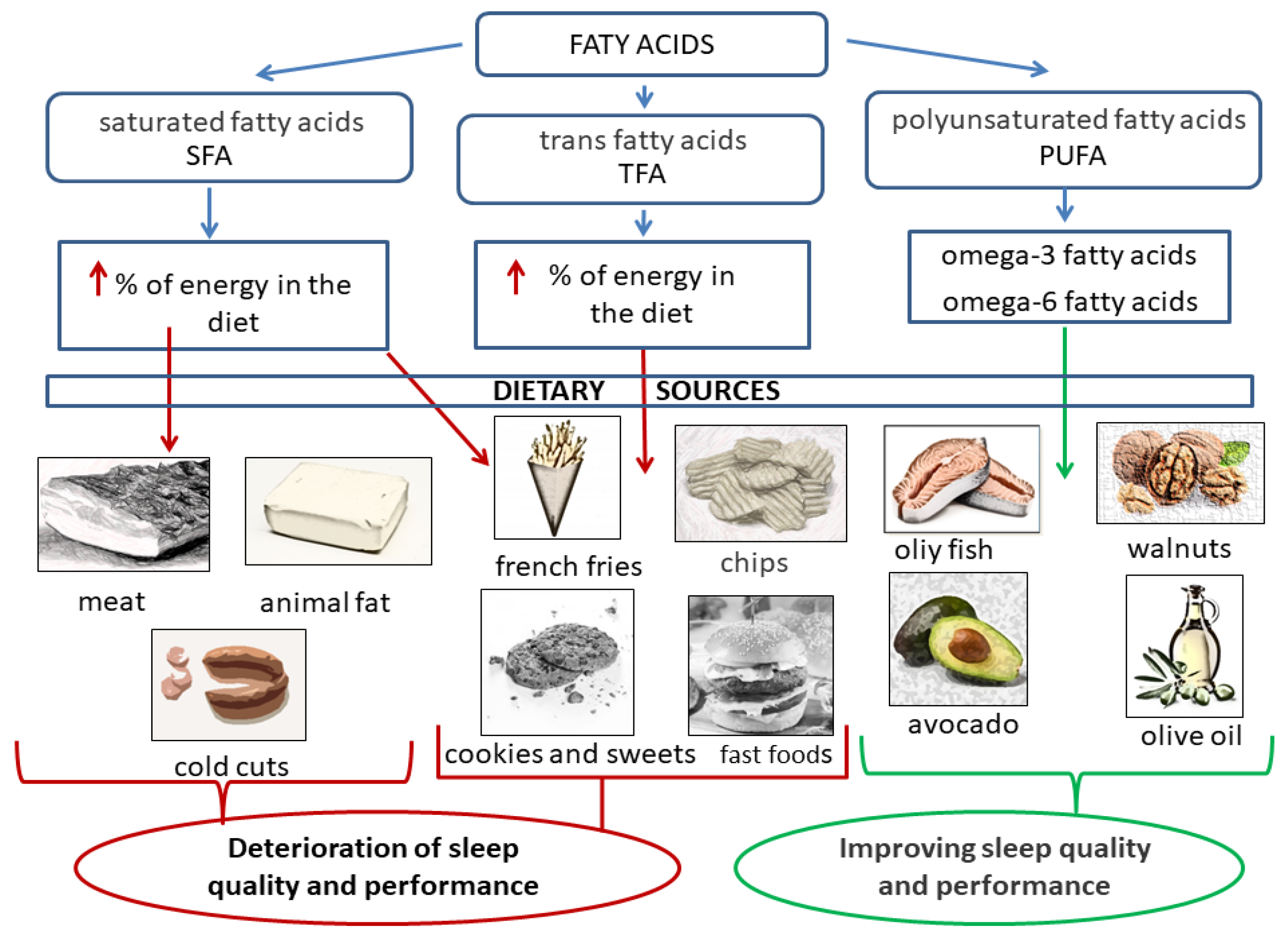
3.1.2. Dietary Fat and Sleep Quality
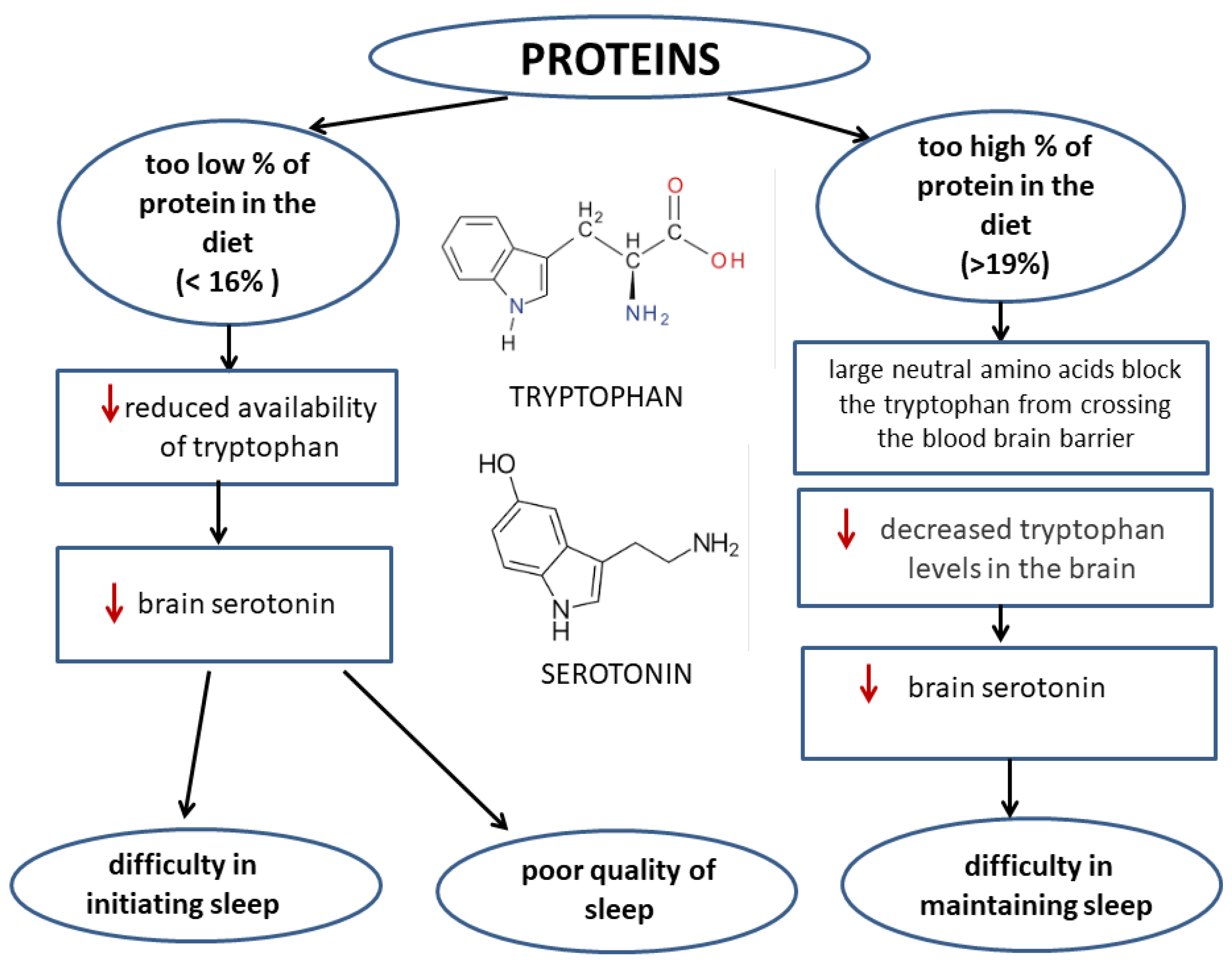
3.1.3. Dietary Protein and Sleep Quality
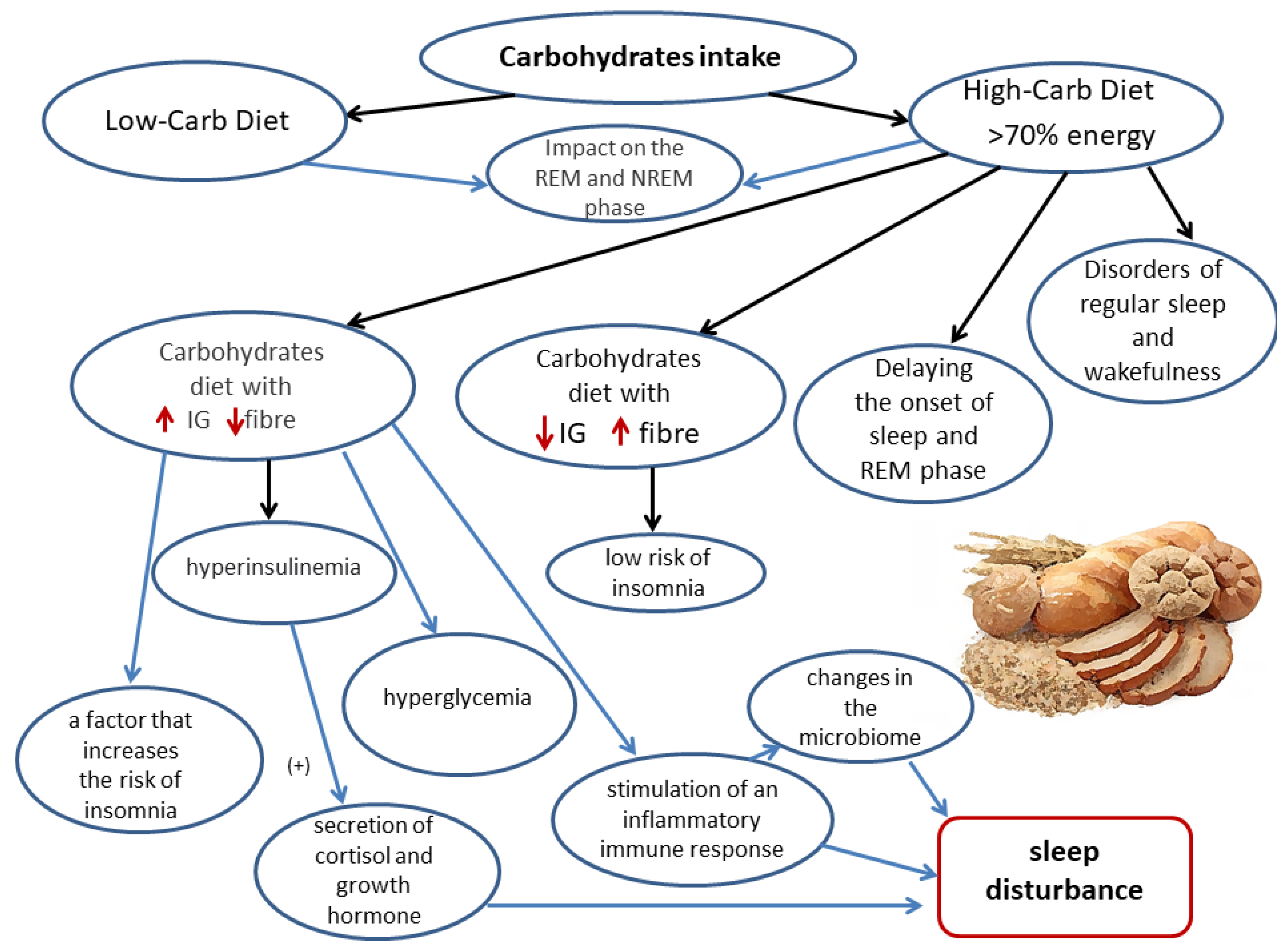
3.1.4. Dietary Carbohydrates and Sleep Quality
3.1.5. Caffeine
3.1.6. Vitamin D
3.1.7. Tryptophan, Serotonin, and Melatonin
3.1.8. Gamma Aminobutyric Acid
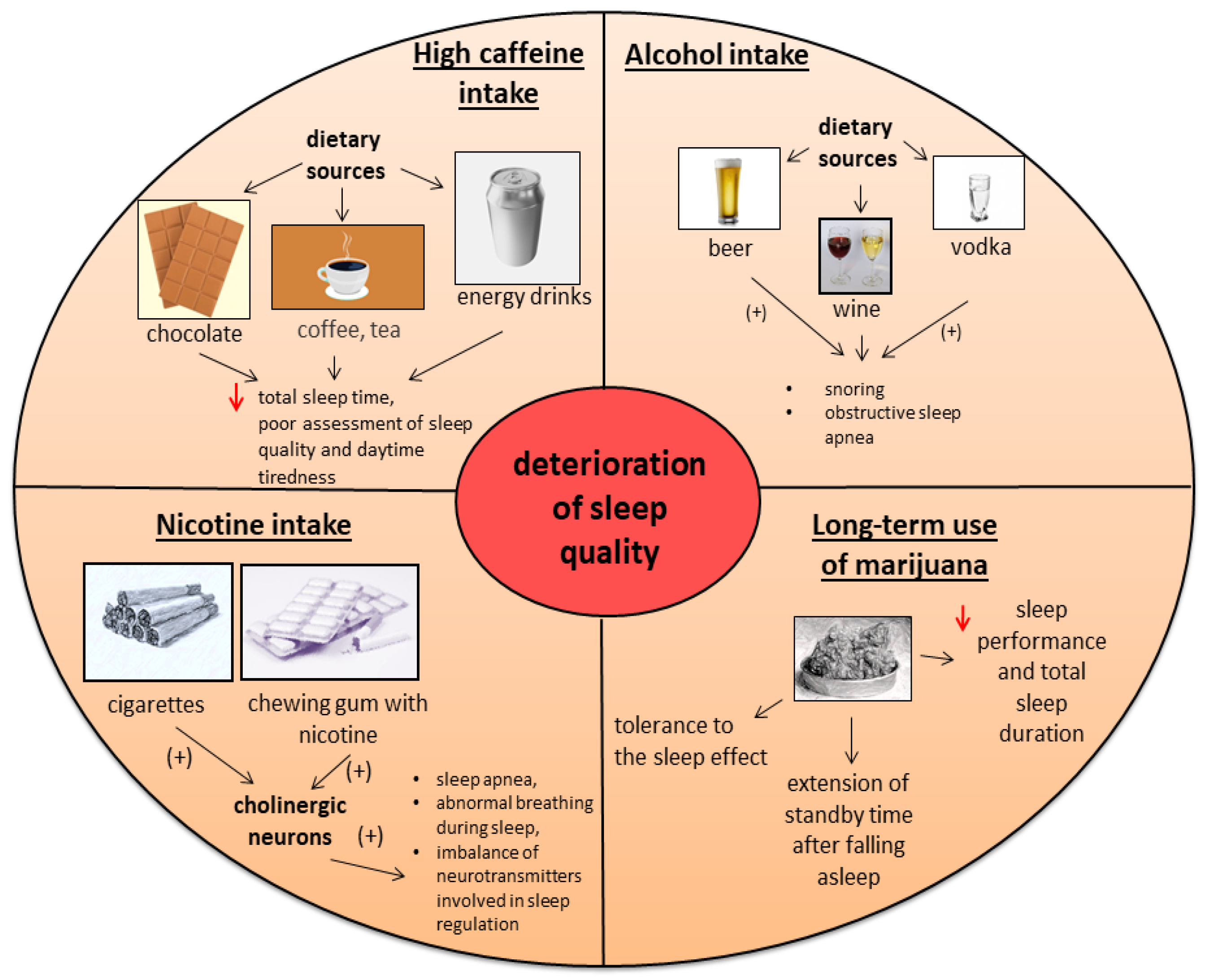
3.2. Stimulants and Drugs That Affect Sleep Quality
3.2.1. Alcohol
3.2.2. Nicotine
3.2.3. Cannabis
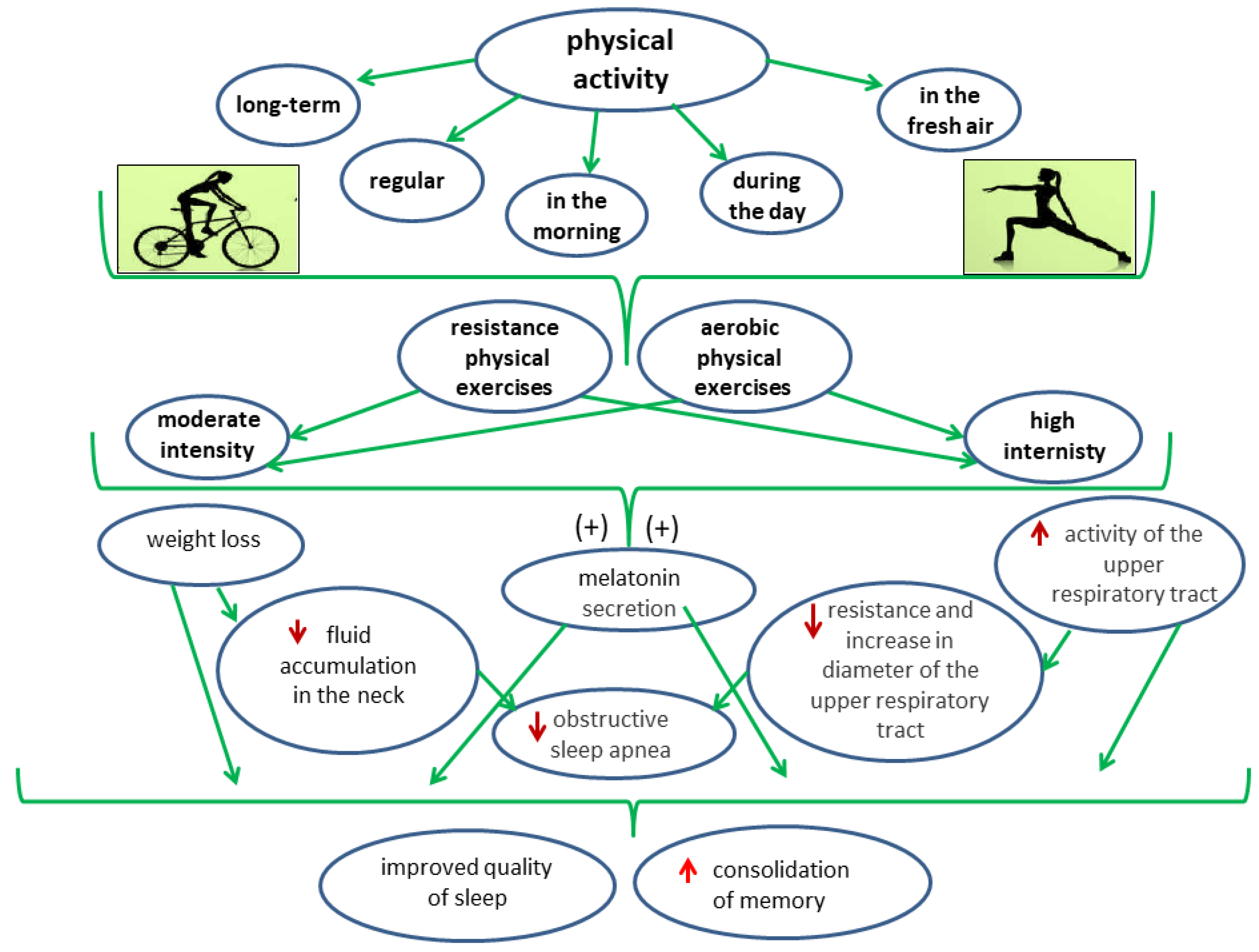
3.3. The Impact of Physical Activity on the Quality of Sleep
3.3.1. The Effect of Recreational Physical Activity on Sleep Quality
3.3.2. The Effect of Physical Exercise on the Quality of Sleep in People with Insomnia
3.3.3. The Impact of Physical Activity on the Quality of Sleep of Children and Adolescents
3.3.4. The Effect of Physical Activity on Sleep Quality in Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krueger, J.M.; Frank, M.G.; Wisor, J.P.; Roy, S. Sleep function: Toward elucidating an enigma. Sleep Med. Rev. 2016, 28, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, M.R. Why Sleep is important for health: A psychoneuroimmunology perspective. Annu. Rev. Psychol. 2016, 66, 143–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saidi, O.; Rochette, E.; Doré, É.; Maso, F.; Raoux, J.; Andrieux, F.; Fantini, M.L.; Merlin, E.; Pereira, B.; Walrand, S.; et al. Randomized double-blind controlled trial on the effect of proteins with different tryptophan/large neutral amino acid ratios on sleep in adolescents: The protmorpheus study. Nutrients 2020, 12, 1885. [Google Scholar] [CrossRef] [PubMed]
- Murawski, B.; Plotnikoff, R.C.; Rayward, A.T.; Vandelanotte, C.; Brown, W.J.; Duncan, M.J. Randomised controlled trial using a theory-based m-health intervention to improve physical activity and sleep health in adults: The Synergy Study protocol. BMJ Open 2018, 8, e018997. [Google Scholar] [CrossRef]
- Dashti, H.S.; Jones, S.E.; Wood, A.R.; Lane, J.M.; van Hees, V.T.; Wang, H.; Rhodes, J.A.; Song, Y.; Patel, K.; Anderson, S.G.; et al. Genome-wide association study identifies genetic loci for self-reported habitual sleep duration supported by accelerometer-derived estimates. Nat. Commun. 2019, 10, 1100. [Google Scholar] [CrossRef] [Green Version]
- Morsing, J.A.; Smith, M.G.; Ögren, M.; Thorsson, P.; Pedersen, E.; Forssén, J.; Waye, K.P. Wind turbine noise and sleep: Pilot studies on the influence of noise characteristics. Int. J. Environ. Res. Public Health 2018, 15, 2573. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Cheng, L.Y.; Chiu, M.H.; Paller, K.A. Promoting memory consolidation during sleep: A meta-analysis of targeted memory reactivation. Psychol. Bull. 2020, 146, 218–244. [Google Scholar] [CrossRef]
- Rakowska, M.; Abdellahi, M.E.; Bagrowska, P.; Navarrete, M.; Lewis, P.A. Long term effects of cueing procedural memory reactivation during NREM sleep. NeuroImage 2021, 244, 118573. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Rawtaer, I.; Fam, J.; Jiang, M.-J.; Feng, L.; Kua, E.H.; Mahendran, R. Sleep correlates of depression and anxiety in an elderly Asian population. Psychogeriatrics 2016, 16, 191–195. [Google Scholar] [CrossRef]
- Kwok, C.S.; Kontopantelis, E.; Kuligowski, G.; Gray, M.; Muhyaldeen, A.; Gale, C.P.; Peat, G.M.; Cleator, J.; Chew-Graham, C.; Loke, Y.K.; et al. Self-reported sleep duration and quality and cardiovascular disease and mortality: A dose-response meta-analysis. J. Am. Heart Assoc. 2018, 7, e008552. [Google Scholar] [CrossRef] [Green Version]
- Zhai, L.; Zhang, H.; Zhang, D. Sleep duration and depression among adults: A meta-analysis of prospective studies. Depress. Anxiety 2015, 32, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Prather, A.A.; Janicki-Deverts, D.; Hall, M.H.; Cohen, S. Behaviorally assessed sleep and susceptibility to the common cold. Sleep 2015, 38, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Aouad, R. The effects of insomnia and sleep loss on cardiovascular disease. Sleep Med. Clin. 2017, 12, 167–177. [Google Scholar] [CrossRef]
- Gobbi, G.; Comai, S. Differential function of melatonin MT1 and MT2 receptors in REM and NREM sleep. Front. Endocrinol. 2019, 10, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, M.R. Sleep and inflammation: Partners in sickness and in health. Nat. Rev. Immunol. 2019, 19, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Valko, P.O.; Hunziker, S.; Graf, K.; Werth, E.; Baumann, C.R. Sleep-wake misperception. A comprehensive analysis of a large sleep lab cohort. Sleep Med. 2021, 88, 96–103. [Google Scholar] [CrossRef]
- Brown, R.E.; Basheer, R.; McKenna, J.T.; Strecker, R.E.; McCarley, R.W. Control of sleep and wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef] [Green Version]
- Abbasi, S.F.; Jamil, H.; Chen, W. EEG-based neonatal sleep stage classification using ensemble learning. Comput. Mater. Contin. 2022, 70, 4619–4633. [Google Scholar] [CrossRef]
- Watson, N.F.; Buchwald, D.; Vitiello, M.; Noonan, C.; Goldberg, J. A twin study of sleep duration and body mass Index. J. Clin. Sleep Med. 2010, 6, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Watson, N.F.; Safwan Badr, M.; Belenky, G.; Bliwise, G.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended amount of sleep for a healthy adult: A joint consensus statement of the american academy of sleep medicine and sleep research society. Sleep 2015, 38, 843–844. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National sleep foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J. Insomnia. JAMA 2013, 309, 706–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bollu, P.C.; Kaur, H. Sleep medicine: Insomnia and sleep. Mo. Med. 2019, 116, 68–75. [Google Scholar] [PubMed]
- Reed, D.L.; Sacco, W.P. Measuring sleep efficiency: What should the denominator be? J. Clin. Sleep Med. 2016, 12, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Klingelhoefer, L.; Bhattacharya, K.; Reichmann, H. Restless legs syndrome. Clin. Med. 2016, 16, 379–382. [Google Scholar] [CrossRef]
- de Zambotti, M.; Goldstone, A.; Colrain, I.M.; Baker, F. Insomnia disorder in adolescence: Diagnosis, impact, and treatment. Sleep Med. Rev. 2018, 39, 12–24. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflügers Arch. Eur. J. Physiol. 2012, 463, 121–137. [Google Scholar] [CrossRef] [Green Version]
- Scammell, T.E.; Arrigoni, E.; Lipton, J.O. Neural circuitry of wakefulness and sleep. Neuron 2017, 93, 747–765. [Google Scholar] [CrossRef] [Green Version]
- Jessen, N.A.; Munk, A.S.F.; Lundgaard, I.; Nedergaard, M. The glymphatic system: A beginner’s guide. Neurochem. Res. 2015, 40, 2583–2599. [Google Scholar] [CrossRef] [Green Version]
- Adam, K. Sleep as a restorative process and a theory to explain why. Prog. Brain Res. 1980, 53, 289–305. [Google Scholar] [CrossRef]
- Rasmussen, M.K.; Mestre, H.; Nedergaard, M. The glymphatic pathway in neurological disorders. Lancet Neurol. 2018, 17, 1016–1024. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Tan, F.; Wei, L.; Li, X.; Lyu, Z.; Feng, X.; Wen, Y.; Guo, L.; He, J.; Dai, M.; et al. Sleep duration and the risk of cancer: A systematic review and meta-analysis including dose–response relationship. BMC Cancer 2018, 18, 1149. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Mikic, A.; Pietrolungo, C.E. Effects of diet on sleep quality. Adv. Nutr. Int. Rev. J. 2016, 7, 938–949. [Google Scholar] [CrossRef]
- Binks, H.; Vincent, G.E.; Gupta, C.; Irwin, C.; Khalesi, S. Effects of diet on sleep: A narrative review. Nutrients 2020, 12, 936. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Rodríguez, A.; Rubio-Arias, J.; Ramos-Campo, D.J.; Reche-García, C.; Leyva-Vela, B.; Nadal-Nicolás, Y. Psychological and sleep effects of tryptophan and magnesium-enriched mediterranean diet in women with fibromyalgia. Int. J. Environ. Res. Public Health 2020, 17, 2227. [Google Scholar] [CrossRef] [Green Version]
- O’Callaghan, F.; Muurlink, O.; Reid, N. Effects of caffeine on sleep quality and daytime functioning. Risk Manag. Health Policy 2018, 11, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Shilo, L.; Sabbah, H.; Hadari, R.; Kovatz, S.; Weinberg, U.; Dolev, S.; Dagan, Y.; Shenkman, L. The effects of coffee consumption on sleep and melatonin secretion. Sleep Med. 2002, 3, 271–273. [Google Scholar] [CrossRef]
- He, S.; Hasler, B.P.; Chakravorty, S. Alcohol and sleep-related problems. Curr. Opin. Psychol. 2019, 30, 117–122. [Google Scholar] [CrossRef]
- Gérard, C.; Vidal, H. Impact of gut microbiota on host glycemic control. Front. Endocrinol. 2019, 10, 29. [Google Scholar] [CrossRef]
- Zhao, M.; Tuo, H.; Wang, S.; Zhao, L. The effects of dietary nutrition on sleep and sleep disorders. Mediat. Inflamm. 2020, 2020, 3142874. [Google Scholar] [CrossRef] [PubMed]
- Doherty, R.; Madigan, S.; Warrington, G.; Ellis, J. Sleep and nutrition interactions: Implications for athletes. Nutrients 2019, 11, 822. [Google Scholar] [CrossRef] [Green Version]
- Ogilvie, R.P.; Patel, S. The epidemiology of sleep and obesity. Sleep Health 2018, 3, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Basch, C.E.; Basch, C.H.; Ruggles, K.V.; Rajan, S. Prevalence of sleep duration on an average school night among 4 nationally representative successive samples of american high school students, 2007–2013. Prev. Chronic Dis. 2014, 11, E216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matricciani, L.; Olds, T.; Petkov, J. In search of lost sleep: Secular trends in the sleep time of school-aged children and adolescents. Sleep Med. Rev. 2012, 16, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Cunningham, T.J.; Croft, J.B. Trends in self-reported sleep duration among US adults from 1985 to 2012. Sleep 2015, 38, 829–832. [Google Scholar] [CrossRef] [PubMed]
- Gohil, A.; Hannon, T.S. Poor sleep and obesity: Concurrent epidemics in adolescent youth. Front. Endocrinol. 2018, 9, 364. [Google Scholar] [CrossRef]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004, 1, e62. [Google Scholar] [CrossRef]
- Liu, X.; Forbes, E.; Ryan, N.D.; Rofey, D.; Hannon, T.S.; Dahl, R.E. Rapid eye movement sleep in relation to overweight in children and adolescents. Arch. Gen. Psychiatry 2008, 65, 924–932. [Google Scholar] [CrossRef] [Green Version]
- Ding, C.; Lim, L.L.; Xu, L.; Kong, A.P.S. Sleep and obesity. J. Obes. Metab. Syndr. 2018, 27, 4–24. [Google Scholar] [CrossRef] [Green Version]
- Grandner, M.A.; Kripke, D.F.; Naidoo, N.; Langer, R.D. Relationships among dietary nutrients and subjective sleep, objective sleep, and napping in women. Sleep Med. 2010, 11, 180–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeke, S.C.E.; Storfer-Isser, A.; Redline, S.; Taveras, E.M. Childhood sleep duration and quality in relation to leptin concentration in two cohort studies. Sleep 2014, 37, 613–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, M.A.; Holscher, H.D. Microbiome-mediated effects of the mediterranean diet on inflammation. Adv. Nutr. 2018, 9, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Al-Rashed, F.; Sindhu, S.; Al Madhoun, A.; Alghaith, A.; Azim, R.; Al-Mulla, F.; Ahmad, R. Short sleep duration and its association with obesity and other metabolic risk factors in kuwaiti urban adults. Nat. Sci. Sleep 2021, 13, 1225–1241. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Colacicco, A.M.; D’Introno, A.; Capurso, C.; Torres, F.; Rizzo, C.; Capurso, A.; Panza, F. Dietary intake of unsaturated fatty acids and age-related cognitive decline: A 8.5-year follow-up of the Italian longitudinal study on aging. Neurobiol. Aging 2006, 27, 1694–1704. [Google Scholar] [CrossRef] [PubMed]
- de Souza, R.; Mente, A.; Maroleanu, A.; Cozma, A.I.; Ha, V.; Kishibe, T.; Uleryk, E.; Budylowski, P.; Schünemann, H.; Beyene, J.; et al. Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: Systematic review and meta-analysis of observational studies. BMJ 2015, 351, h3978. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.L.; Dahl, L.; Olson, G.; Thornton, D.; Graff, I.E.; Frøyland, L.; Thayer, J.F.; Pallesen, S. Fish consumption, sleep, daily functioning, and heart rate variability. J. Clin. Sleep Med. 2014, 10, 567–575. [Google Scholar] [CrossRef] [Green Version]
- Lavialle, M.; Champeil-Potokar, G.; Alessandri, J.M.; Balasse, L.; Guesnet, P.; Papillon, C.; Pévet, P.; Vancassel, S.; Vivien-Roels, B.; Denis, I. An (n-3) polyunsaturated fatty acid–deficient diet disturbs daily locomotor activity, melatonin rhythm, and striatal dopamine in syrian hamsters. J. Nutr. 2008, 138, 1719–1724. [Google Scholar] [CrossRef] [Green Version]
- St-Onge, M.-P.; Roberts, A.; Shechter, A.; Choudhury, A.R. Fiber and saturated fat are associated with sleep arousals and slow wave sleep. J. Clin. Sleep Med. 2016, 12, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Sacks, F.M.; Lichtenstein, A.H.; Wu, J.H.Y.; Appel, L.J.; Creager, M.A.; Kris-Etherton, P.M.; Miller, M.; Rimm, E.B.; Rudel, L.L.; Robinson, J.G.; et al. Dietary fats and cardiovascular disease: A presidential advisory from the american heart association. Circulation 2017, 136, e1–e23. [Google Scholar] [CrossRef]
- Surani, S.; Brito, V.; Surani, A.; Ghamande, S. Effect of diabetes mellitus on sleep quality. World J. Diabetes. 2015, 6, 868–873. [Google Scholar] [CrossRef]
- Urade, Y.; Hayaishi, O. Prostaglandin D2 and sleep/wake regulation. Sleep Med. Rev. 2011, 15, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Fang Zhang, F.; Bhupathiraju, S.N. Trends in dietary carbohydrate, protein, and fat intake and diet quality among US adults, 1999–2016. JAMA J. Am. Med. Assoc. 2019, 322, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Brandhorst, S.; Longo, V.S.D. Protein quantity and source, fasting-mimicking diets, and longevity. Adv. Nutr. Int. Rev. J. 2019, 10, S340–S350. [Google Scholar] [CrossRef]
- Tanaka, E.; Yatsuya, H.; Uemura, M.; Murata, C.; Otsuka, R.; Toyoshima, H.; Tamakoshi, K.; Sasaki, S.; Kawaguchi, L.; Aoyama, A. Associations of protein, fat, and carbohydrate intakes with insomnia symptoms among middle-aged Japanese workers. J. Epidemiol. 2013, 23, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Sutanto, C.N.; Loh, W.W.; Toh, D.W.K.; Lee, D.P.S.; Kim, J.E. Association between dietary protein intake and sleep quality in middle-aged and older adults in Singapore. Front. Nutr. 2022, 9, 832341. [Google Scholar] [CrossRef] [PubMed]
- Trommelen, J.; Van Loon, L.J.C. Pre-sleep protein ingestion to improve the skeletal muscle adaptive response to exercise training. Nutrients 2016, 8, 763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daneshzad, E.; Keshavarz, S.A.; Qorbani, M.; Larijani, B.; Azadbakht, L. Association between a low-carbohydrate diet and sleep status, depression, anxiety, and stress score. J. Sci. Food Agric. 2020, 100, 2946–2952. [Google Scholar] [CrossRef]
- Afaghi, A.; O’Connor, H.; Chow, C.M. High-glycemic-index carbohydrate meals shorten sleep onset. Am. J. Clin. Nutr. 2007, 85, 426–430. [Google Scholar] [CrossRef]
- Gangwisch, J.; Hale, L.; St-Onge, M.-P.; Choi, L.; LeBlanc, E.S.; Malaspina, D.; Opler, M.G.; Shadyab, A.H.; Shikany, J.M.; Snetselaar, L.; et al. High glycemic index and glycemic load diets as risk factors for insomnia: Analyses from the women’s health initiative. Am. J. Clin. Nutr. 2020, 111, 429–439. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Jenkins, A.L. Dietary fiber and the glycemic response. Proc. Soc. Exp. Biol. Med. 1985, 180, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Wurtman, R.J.; Wurtman, J.J.; Regan, M.M.; McDermott, J.M.; Tsay, R.H.; Breu, J.J. Effects of normal meals rich in carbohydrates or proteins on plasma tryptophan and tyrosine ratios. Am. J. Clin. Nutr. 2003, 77, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Chen, J.; Wirth, M.D.; Shivappa, N.; Hebert, J.R. Lower dietary inflammatory index scores are associated with lower glycemic index scores among college students. Nutrients 2018, 10, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kräuchi, K.; Cajochen, C.; Werth, E.; Wirz-Justice, A. Alteration of internal circadian phase relationships after morning versus evening carbohydrate-rich meals in humans. J. Biol. Rhythm. 2002, 17, 364–376. [Google Scholar] [CrossRef]
- Haghighatdoost, F.; Karimi, G.; Esmaillzadeh, A.; Azadbakht, L. Sleep deprivation is associated with lower diet quality indices and higher rate of general and central obesity among young female students in Iran. Nutrition 2012, 28, 1146–1150. [Google Scholar] [CrossRef]
- Nishiura, C.; Noguchi, J.; Hashimoto, H. Dietary patterns only partially explain the effect of short sleep duration on the incidence of obesity. Sleep 2010, 33, 753–757. [Google Scholar] [CrossRef] [Green Version]
- Watson, E.J.; Coates, A.M.; Kohler, M.; Banks, S. Caffeine consumption and sleep quality in Australian adults. Nutrients 2016, 8, 479. [Google Scholar] [CrossRef]
- Hindmarch, I.; Rigney, U.; Stanley, N.; Quinlan, P.; Rycroft, J.; Lane, J. A naturalistic investigation of the effects of day-long consumption of tea, coffee and water on alertness, sleep onset and sleep quality. Psychopharmacology 2000, 149, 203–216. [Google Scholar] [CrossRef]
- Van Dongen, H.P.; Price, N.J.; Mullington, J.M.; Szuba, M.P.; Kapoor, S.C.; Dinges, D.F. Caffeine eliminates psychomotor vigilance deficits from sleep inertia. Sleep 2001, 24, 813–819. [Google Scholar] [CrossRef]
- Landolt, H.-P.; Werth, E.; Borbély, A.A.; Dijk, D.-J. Caffeine intake (200 mg) in the morning affects human sleep and EEG power spectra at night. Brain Res. 1995, 675, 67–74. [Google Scholar] [CrossRef]
- Ward, A.L.; Jospe, M.; Morrison, S.; Reynolds, A.N.; Kuroko, S.; Fangupo, L.J.; Smith, C.; Galland, B.C.; Taylor, R.W. Bidirectional associations between sleep quality or quantity, and dietary intakes or eating behaviors in children 6–12 years old: A systematic review with evidence mapping. Nutr. Rev. 2021, 79, 1079–1099. [Google Scholar] [CrossRef] [PubMed]
- Garcion, E.; Wion-Barbot, N.; Montero-Menei, C.N.; Berger, F.; Wion, D. New clues about vitamin D functions in the nervous system. Trends Endocrinol. Metab. 2002, 13, 100–105. [Google Scholar] [CrossRef]
- Lagunova, Z.; Porojnicu, A.; Aksnes, L.; Holick, M.; Iani, V.; Bruland, O.S.; Moan, J. Effect of vitamin D supplementation and ultraviolet B exposure on serum 25-hydroxyvitamin D concentrations in healthy volunteers: A randomized, crossover clinical trial. Br. J. Dermatol. 2013, 169, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Vaes, A.; Brouwer-Brolsma, E.; van der Zwaluw, N.; van Wijngaarden, J.; Berendsen, A.; van Schoor, N.; van der Velde, N.; Uitterlinden, A.; Lips, P.; Dhonukshe-Rutten, R.; et al. Food sources of vitamin D and their association with 25-hydroxyvitamin D status in Dutch older adults. J. Steroid Biochem. Mol. Biol. 2017, 173, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Chae, C.H.; Kim, Y.O.; Son, J.S.; Kim, C.W.; Park, H.O.; Lee, J.H.; Shin, Y.H.; Kwak, H.S. The relationship between serum vitamin D levels and sleep quality in fixed day indoor field workers in the electronics manufacturing industry in Korea. Ann. Occup. Environ. Med. 2017, 29, 25. [Google Scholar] [CrossRef]
- Musiol, I.M.; Stumpf, W.E.; Bidmon, H.-J.; Heiss, C.; Mayerhofer, A.; Bartke, A. Vitamin d nuclear binding to neurons of the septal, substriatal and amygdaloid area in the siberian hamster (phodopus sungorus) brain. Neuroscience 1992, 48, 841–848. [Google Scholar] [CrossRef]
- Eyles, D.W. Vitamin D: Brain and behavior. JBMR Plus 2021, 5, e10419. [Google Scholar] [CrossRef]
- Watson, E.J.; Banks, S.; Coates, A.M.; Kohler, M.J. The relationship between caffeine, sleep, and behavior in children. J. Clin. Sleep Med. 2017, 13, 533–543. [Google Scholar] [CrossRef] [Green Version]
- Majid, M.S.; Ahmad, H.S.; Bizhan, H.; Hosein, H.Z.M.; Mohammad, A. The effect of vitamin D supplement on the score and quality of sleep in 20–50 year-old people with sleep disorders compared with control group. Nutr. Neurosci. 2018, 21, 511–519. [Google Scholar] [CrossRef]
- Watford, M.; Wu, G. Protein. Adv. Nutr. Int. Rev. J. 2018, 9, 651–653. [Google Scholar] [CrossRef] [Green Version]
- He, W.; Wu, G. Metabolism of amino acids in the brain and their roles in regulating food intake. Adv. Exp. Med. Biol. 2020, 1265, 167–185. [Google Scholar] [CrossRef] [PubMed]
- Bravo, R.; Matito, S.; Cubero, J.; Paredes, S.D.; Franco, L.; Rivero, M.; Rodríguez, A.B.; Barriga, C. Tryptophan-enriched cereal intake improves nocturnal sleep, melatonin, serotonin, and total antioxidant capacity levels and mood in elderly humans. AGE 2012, 35, 1277–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, D.; Yu, Y.; Shen, Y.; Liu, Q.; Zhao, Z.; Sharma, R.; Reiter, R.J. Melatonin synthesis and function: Evolutionary history in animals and plants. Front. Endocrinol. 2019, 10, 249. [Google Scholar] [CrossRef] [PubMed]
- Howatson, G.; Bell, P.G.; Tallent, J.; Middleton, B.; McHugh, M.P.; Ellis, J. Effect of tart cherry juice (Prunus cerasus) on melatonin levels and enhanced sleep quality. Eur. J. Nutr. 2012, 51, 909–916. [Google Scholar] [CrossRef]
- Diana, M.; Quílez, J.; Rafecas, M. Gamma-aminobutyric acid as a bioactive compound in foods: A review. J. Funct. Foods 2014, 10, 407–420. [Google Scholar] [CrossRef]
- Briguglio, M.; Dell’Osso, B.; Panzica, G.; Malgaroli, A.; Banfi, G.; Dina, C.Z.; Galentino, R.; Porta, M. Dietary neurotransmitters: A narrative review on current knowledge. Nutrients 2018, 10, 591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byun, J.-I.; Shin, Y.Y.; Chung, S.-E.; Shin, W.C. Safety and efficacy of gamma-aminobutyric acid from fermented rice germ in patients with insomnia symptoms: A randomized, double-blind trial. J. Clin. Neurol. 2018, 14, 291–295. [Google Scholar] [CrossRef]
- Yamatsu, A.; Yamashita, Y.; Maru, I.; Yang, J.; Tatsuzaki, J.; Kim, M. The improvement of sleep by oral intake of GABA and apocynum venetum leaf extract. J. Nutr. Sci. Vitaminol. 2015, 61, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Luppi, P.-H.; Peyron, C.; Fort, P. Not a single but multiple populations of GABAergic neurons control sleep. Sleep Med. Rev. 2017, 32, 85–94. [Google Scholar] [CrossRef]
- Irish, L.A.; Kline, C.E.; Gunn, H.E.; Buysse, D.J.; Hall, M.H. The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Med. Rev. 2015, 22, 23–36. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.H.; Kuo, H.Y.; Chueh, K.H. Sleep hygiene education efficacy on sleep quality in working women. J. Nurs. Res. 2010, 18, 283–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hershner, S.; O’Brien, L.M. The impact of a randomized sleep education intervention for college students. J. Clin. Sleep Med. 2018, 14, 337–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zengin, L.; Aylaz, R. The effects of sleep hygiene education and reflexology on sleep quality and fatigue in patients receiving chemotherapy. Eur. J. Cancer Care 2019, 28, e13020. [Google Scholar] [CrossRef]
- Stein, M.D.; Friedmann, P.D. Disturbed sleep and its relationship to alcohol use. Subst. Abus. 2006, 26, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Drummond, S.P.; Gillin, J.C.; Smith, T.L.; DeModena, A. The sleep of abstinent pure primary alcoholic patients: Natural course and relationship to relapse. Alcohol. Clin. Exp. Res. 1998, 22, 1796–1802. [Google Scholar] [CrossRef]
- Costa e Silva, J.A.; Chase, M.; Sartorius, N.; Roth, T. Special report from a symposium held by the world health organization and the world federation of sleep research societies: An overview of insomnias and related disorders-recognition, epidemiology, and rational management. Sleep 1996, 19, 412–416. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Tomasi, D.; Manza, P.; Shokri-Kojori, E.; Demiral, S.B.; Feldman, D.E.; Kroll, D.S.; Biesecker, C.L.; McPherson, K.L.; Wang, G.-J.; et al. Sleep disturbances are associated with cortical and subcortical atrophy in alcohol use disorder. Transl. Psychiatry 2021, 11, 428. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, M.S.; Shipley, J.E. Alcohol use and periodic limb movements of sleep. Alcohol. Clin. Exp. Res. 1993, 17, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Nigri, D.H.; Addor, G.; De Barros Franco, C.A.; Martins, R.C.; Gomes, M.P.V.F.; Strollo, P.J. Alcohol induced apnea. J. Clin. Sleep. Med. 2005, 1, 424–426. [Google Scholar] [CrossRef] [Green Version]
- Purani, H.; Friedrichsen, S.; Allen, A.M. Sleep quality in cigarette smokers: Associations with smoking-related outcomes and exercise. Addict. Behav. 2018, 90, 71–76. [Google Scholar] [CrossRef]
- AlRyalat, S.A.; Kussad, S.; El Khatib, O.; Hamad, I.; Al-Tanjy, A.; Alshnneikat, M.; AbuMahfouz, B. Assessing the effect of nicotine dose in cigarette smoking on sleep quality. Sleep Breath. 2021, 25, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Wetter, D.W.; Fiore, M.C.; Baker, T.B.; Young, T.B. Tobacco withdrawal and nicotine replacement influence objective measures of sleep. J. Consult. Clin. Psychol. 1995, 63, 658–667. [Google Scholar] [CrossRef]
- Kesner, A.J.; Lovinger, D.M. Cannabinoids, endocannabinoids and sleep. Front. Mol. Neurosci. 2020, 13, 125. [Google Scholar] [CrossRef] [PubMed]
- Short, N.A.; Zvolensky, M.J.; Schmidt, N.B. A pilot randomized clinical trial of brief behavioral treatment for insomnia to reduce problematic cannabis use among trauma-exposed young adults. J. Subst. Abus. Treat. 2021, 131, 108537. [Google Scholar] [CrossRef] [PubMed]
- Chakravorty, S.; Vandrey, R.G.; He, S.; Stein, M.D. Sleep management among patients with substance use disorders. Med. Clin. N. Am. 2018, 102, 733–743. [Google Scholar] [CrossRef]
- Kaul, M.; Zee, P.C.; Sahni, A.S. Effects of cannabinoids on sleep and their therapeutic potential for sleep disorders. Neurotherapeutics 2021, 18, 217–227. [Google Scholar] [CrossRef]
- Piper, B.J.; DeKeuster, R.M.; Beals, M.L.; Cobb, C.M.; Burchman, C.A.; Perkinson, L.; Lynn, S.T.; Nichols, S.D.; Abess, A.T. Substitution of medical cannabis for pharmaceutical agents for pain, anxiety, and sleep. J. Psychopharmacol. 2017, 31, 569–575. [Google Scholar] [CrossRef]
- Angarita, G.A.; Emadi, N.; Hodges, S.; Morgan, P.T. Sleep abnormalities associated with alcohol, cannabis, cocaine, and opiate use: A comprehensive review. Addict. Sci. Clin. Pract. 2016, 11, 9. [Google Scholar] [CrossRef] [Green Version]
- Conroy, D.A.; Kurth, M.E.; Strong, D.R.; Brower, K.J.; Stein, M.D. Marijuana use patterns and sleep among community-based young adults. J. Addict. Dis. 2016, 35, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Haney, M.; Ward, A.S.; Comer, S.D.; Foltin, R.W.; Fischman, M.W. Abstinence symptoms following oral THC administration to humans. Psychopharmacology 1999, 141, 385–394. [Google Scholar] [CrossRef]
- Diaz, K.M.; Shimbo, D. Physical activity and the prevention of hypertension. Curr. Hypertens. Rep. 2013, 15, 659–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilckens, K.A.; Erickson, K.I.; Wheeler, M.E. Physical Activity and Cognition: A Mediating Role of Efficient Sleep. Behav. Sleep Med. 2018, 16, 569–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christie, A.D.; Seery, E.; Kent, J.A. Physical activity, sleep quality, and self-reported fatigue across the adult lifespan. Exp. Gerontol. 2016, 77, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Murray, K.; Godbole, S.; Natarajan, L.; Full, K.; Hipp, J.A.; Glanz, K.; Mitchell, J.; Laden, F.; James, P.; Quante, M.; et al. The relations between sleep, time of physical activity, and time outdoors among adult women. PLoS ONE 2017, 12, e0182013. [Google Scholar] [CrossRef]
- Tsunoda, K.; Kitano, N.; Kai, Y.; Uchida, K.; Kuchiki, T.; Okura, T.; Nagamatsu, T. Prospective study of physical activity and sleep in middle-aged and older adults. Am. J. Prev. Med. 2015, 48, 662–673. [Google Scholar] [CrossRef] [PubMed]
- Bisson, A.N.S.; Robinson, S.; Lachman, M.E. Walk to a better night of sleep: Testing the relationship between physical activity and sleep. Sleep Health 2019, 5, 487–494. [Google Scholar] [CrossRef]
- Buxton, O.M.; L’Hemite-Balériaux, M.; Hirschfeld, U.; Cauter, E. Acute and delayed effects of exercise on human melatonin secretion. J. Biol. Rhythm. 1997, 12, 568–574. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Passos, G.S.; Poyares, D.; Santana, M.G.; Garbuio, S.A.; Tufik, S.; de Mello, M.T. Effect of acute physical exercise on patients with chronic primary insomnia. J. Clin. Sleep Med. 2010, 6, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.-J.; Fox, K.R.; Ku, P.-W.; Chang, Y.-W. Effects of aquatic exercise on sleep in older adults with mild sleep impairment: A randomized controlled trial. Int. J. Behav. Med. 2015, 23, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.A.; Torre, A.L.; Banfi, G.; Bonato, M. Acute sleep hygiene strategy improves objective sleep latency following a late-evening soccer-specific training session: A randomized controlled trial. J. Sports Sci. 2019, 37, 2711–2719. [Google Scholar] [CrossRef] [PubMed]
- Focht, B.C.; Koltyn, K.F. Influence of resistance exercise of different intensities on state anxiety and blood pressure. Med. Sci. Sports Exerc. 1999, 31, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Dias de Andrade, F.M.; Pinto Pedrosa, R. The role of physical exercise in obstructive sleep apnea. J. Bras. Pneumol. 2016, 42, 457–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham, L.V.; Schwartz, A.R. The pathogenesis of obstructive sleep apnea. J. Thorac. Dis. 2015, 7, 1358–1372. [Google Scholar]
- Mendelson, M.; Lyons, O.; Yadollahi, A.; Inami, T.; Oh, P.; Bradley, T.D. Effects of exercise training on sleep apnoea in patients with coronary artery disease: A randomised trial. Eur. Respir. J. 2016, 48, 142–150. [Google Scholar] [CrossRef]
- McSharry, D.G.; Saboisky, J.P.; DeYoung, P.; Matteis, P.; Jordan, A.S.; Trinder, J.; Smales, E.; Hess, L.; Guo, M.; Malhotra, A. A Mechanism for upper airway stability during slow wave sleep. Sleep 2013, 36, 555–563. [Google Scholar] [CrossRef] [Green Version]
- Iftikhar, I.H.; Kline, C.E.; Youngstedt, S.D. Effects of exercise training on sleep apnea: A meta-analysis. Lung 2014, 192, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Janssen, X.; Martin, A.; Hughes, A.R.; Hill, C.M.; Kotronoulas, G.; Hesketh, K.R. Associations of screen time, sedentary time and physical activity with sleep in under 5 s: A systematic review and meta-analysis. Sleep Med. Rev. 2020, 49, 101226. [Google Scholar] [CrossRef]
- Ji, M.; Tang, A.; Zhang, Y.; Zou, J.; Zhou, G.; Deng, J.; Yang, L.; Li, M.; Chen, J.; Qin, H.; et al. The relationship between obesity, sleep and physical activity in Chinese preschool children. Int. J. Environ. Res. Public Health 2018, 15, 527. [Google Scholar] [CrossRef] [Green Version]
- Calhoun, S.L.; Fernandez-Mendoza, J.; Vgontzas, A.N.; Liao, D.; Bixler, E.O. Prevalence of insomnia symptoms in a general population sample of young children and preadolescents: Gender effects. Sleep Med. 2014, 15, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Yoong, S.L.; Grady, A.; Stacey, F.; Polimeni, M.; Clayton, O.; Jones, J.; Nathan, N.; Wyse, R.; Wolfenden, L. A pilot randomized controlled trial examining the impact of a sleep intervention targeting home routines on young children’s (3–6 years) physical activity. Pediatr. Obes. 2019, 14, e12481. [Google Scholar] [CrossRef] [PubMed]
- Collier, S.; Fairbrother, K.; Cartner, B.; Alley, J.R.; Curry, C.D.; Dickinson, D.L.; Morris, D.M. Effects of exercise timing on sleep architecture and nocturnal blood pressure in prehypertensives. Vasc. Health Risk Manag. 2014, 10, 691–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Štefan, L.; Vrgoč, G.; Rupčić, T.; Sporiš, G.; Sekulić, D. Sleep duration and sleep quality are associated with physical activity in elderly people living in nursing homes. Int. J. Environ. Res. Public Health 2018, 15, 2512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartescu, I.; Morgan, K.; Stevinson, C.D. Increased physical activity improves sleep and mood outcomes in inactive people with insomnia: A randomized controlled trial. J. Sleep Res. 2015, 24, 526–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, P.-Y.; Ho, K.-H.; Chen, H.-C.; Chien, M.-Y. Exercise training improves sleep quality in middle-aged and older adults with sleep problems: A systematic review. J. Physiother. 2012, 58, 157–163. [Google Scholar] [CrossRef] [Green Version]
- WHO. A Technical Package for Increasing Physical Activity. Available online: https://apps.who.int/iris/bitstream/handle/10665/275415/9789241514804-eng.pdf?sequence=1&isAllowed=y. (accessed on 1 March 2022).
- Reid, K.J.; Baron, K.G.; Lu, B.; Naylor, E.; Wolfe, L.; Zee, P.C. Aerobic exercise improves self-reported sleep and quality of life in older adults with insomnia. Sleep Med. 2010, 11, 934–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sejbuk, M.; Mirończuk-Chodakowska, I.; Witkowska, A.M. Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients 2022, 14, 1912. https://doi.org/10.3390/nu14091912
Sejbuk M, Mirończuk-Chodakowska I, Witkowska AM. Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients. 2022; 14(9):1912. https://doi.org/10.3390/nu14091912
Chicago/Turabian StyleSejbuk, Monika, Iwona Mirończuk-Chodakowska, and Anna Maria Witkowska. 2022. "Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors" Nutrients 14, no. 9: 1912. https://doi.org/10.3390/nu14091912
APA StyleSejbuk, M., Mirończuk-Chodakowska, I., & Witkowska, A. M. (2022). Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients, 14(9), 1912. https://doi.org/10.3390/nu14091912