
Trends in Beef Intake in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2018



Abstract
:1. Introduction
2. Materials and Methods
2.1. Dietary Intake Assessment
2.2. Analytical Sample—Beef Intake Trends
2.3. Analytical Sample—Usual Intake of Beef, per Capita and per Consumer
2.4. Calculation of Beef-Related Variables
2.5. Comparison of Usual Intake of Beef to “Meats, Poultry, Eggs” Modeled in HDP
2.6. Statistical Analysis
3. Results
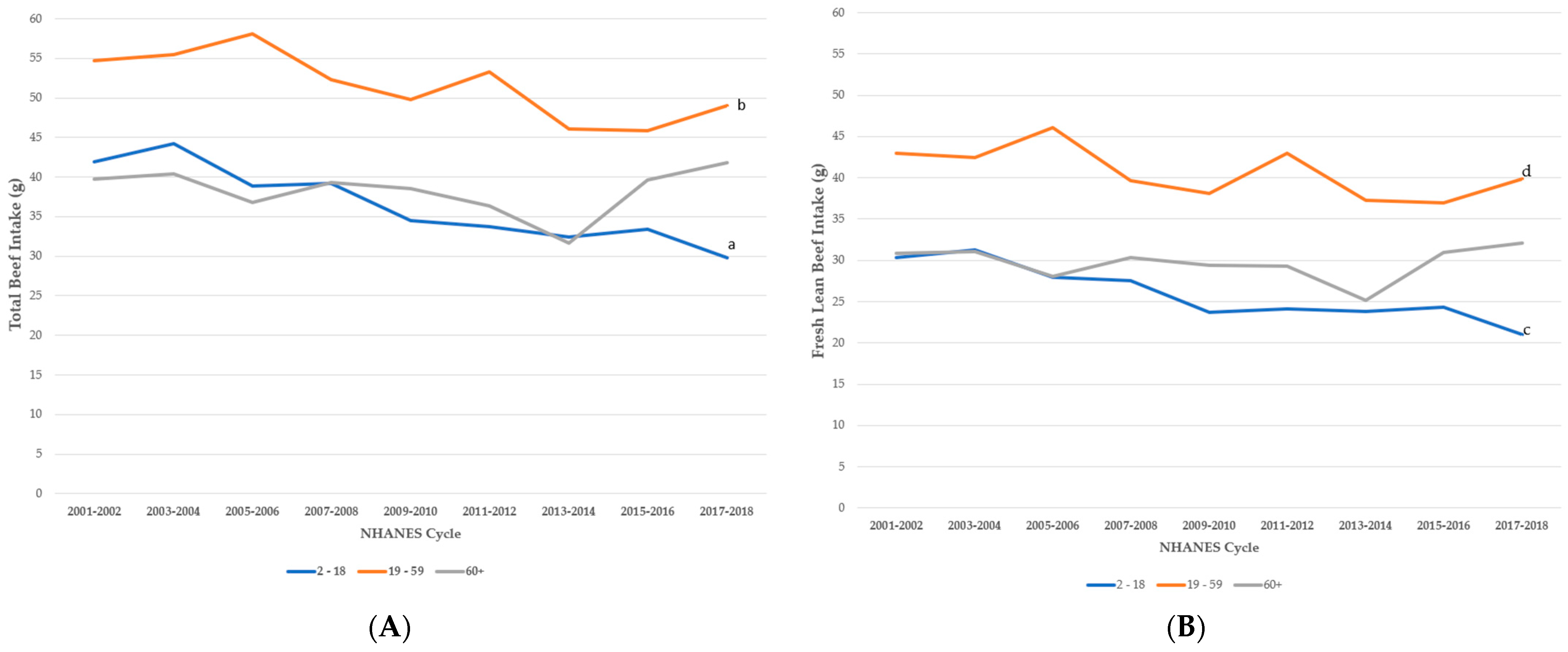
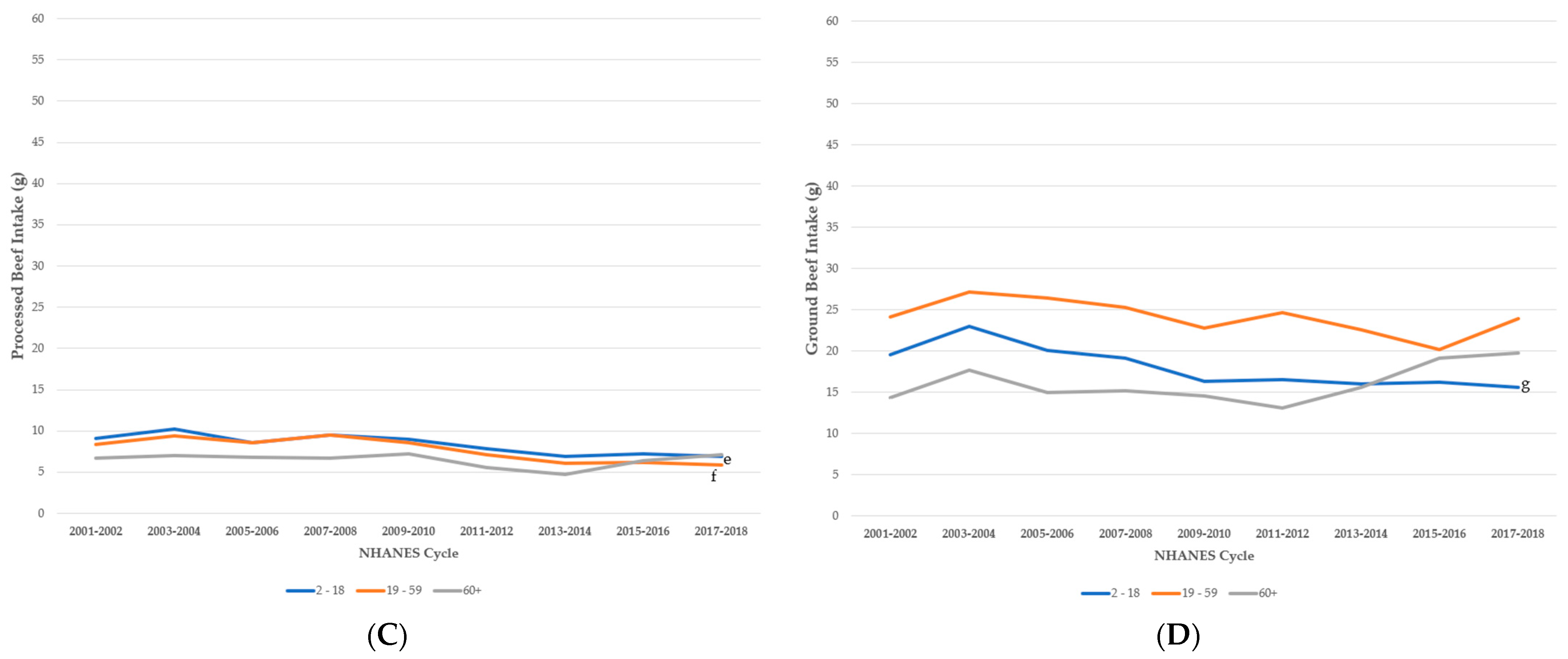
3.1. Trends in Intake of Beef by Age Group, NHANES 2001–2018
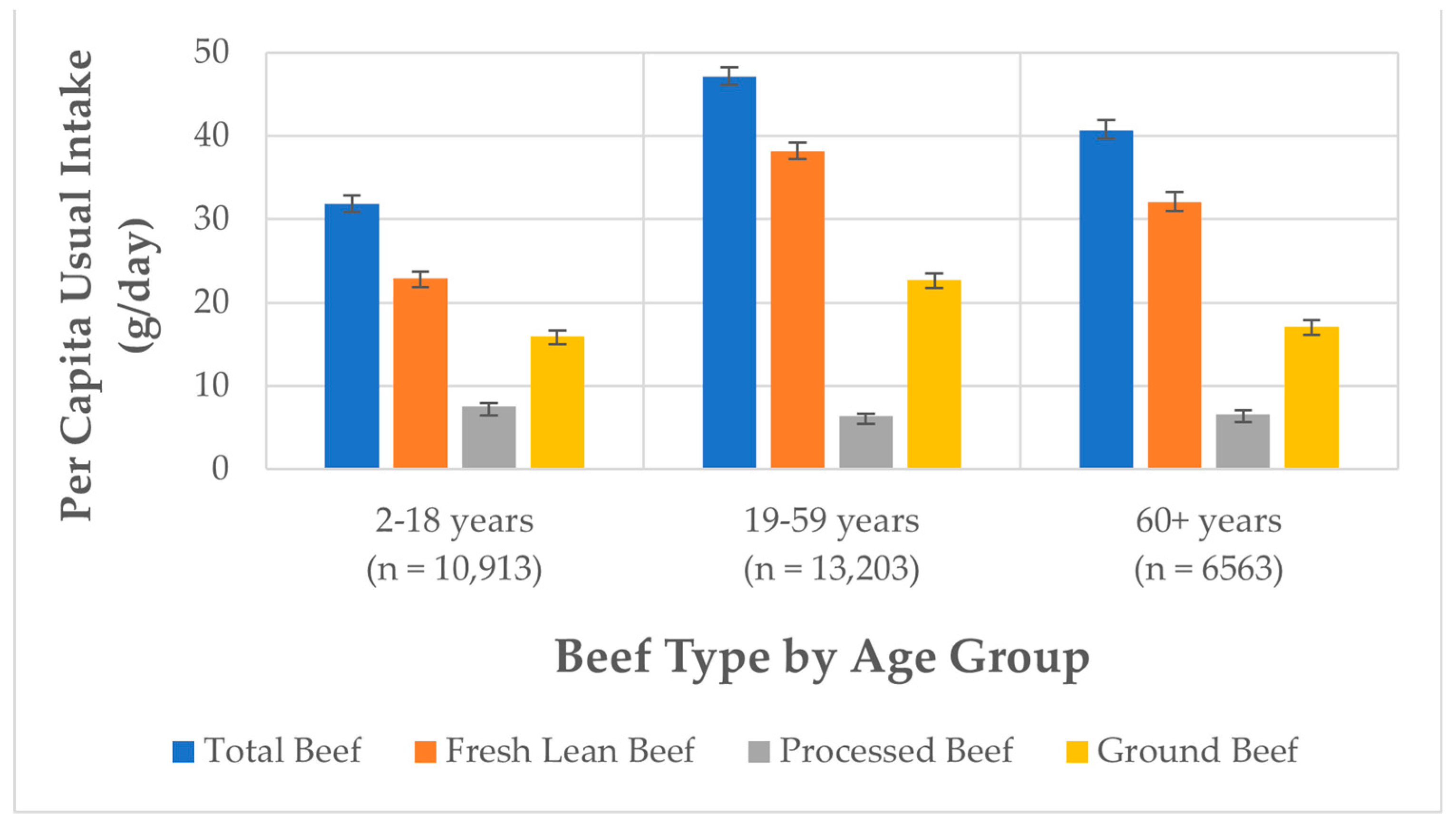
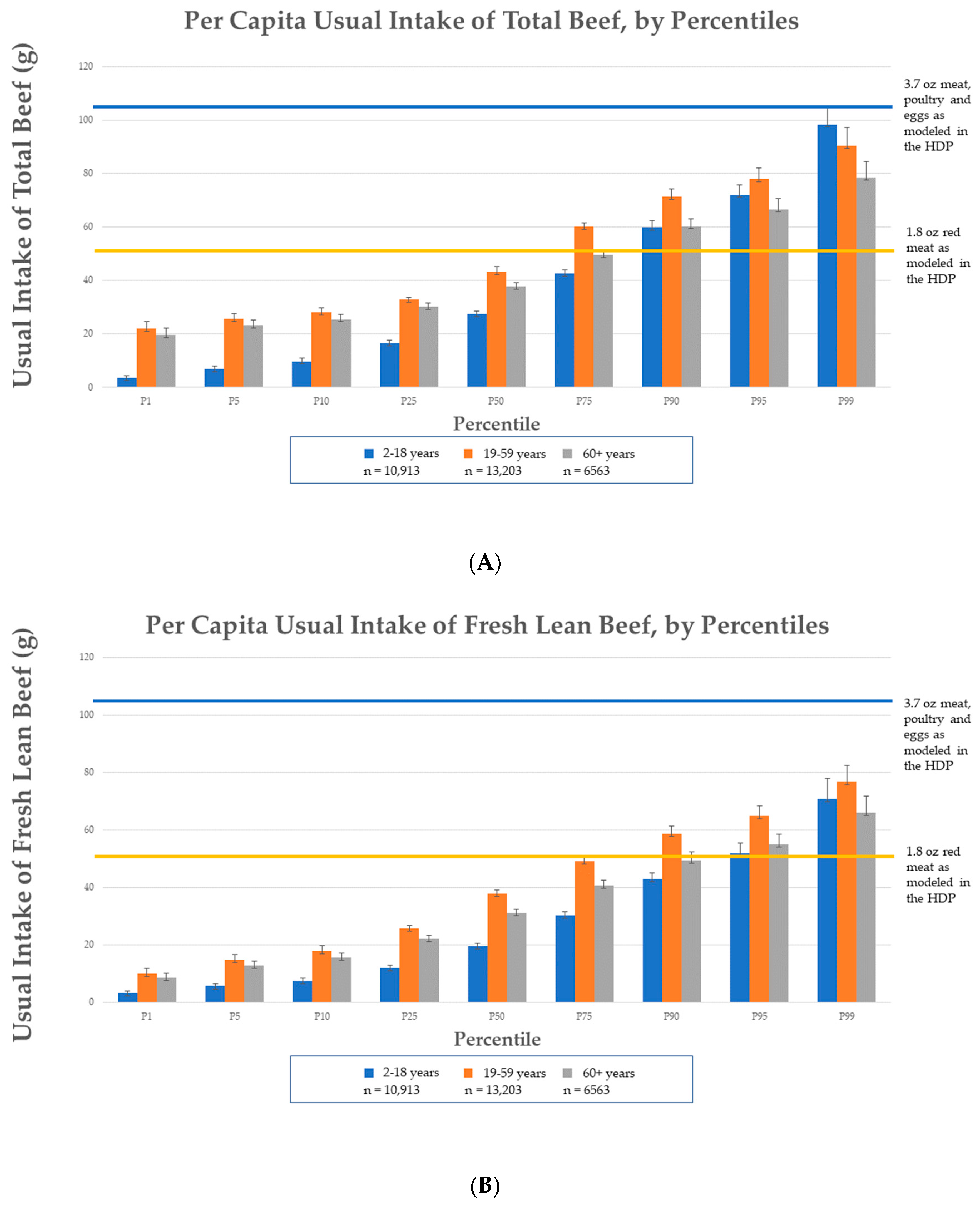
3.2. Per Capita Usual Intake of Beef, NHANES 2011–2018
3.3. Comparison of Per Capita Usual Intake of Beef to HDP Modeling
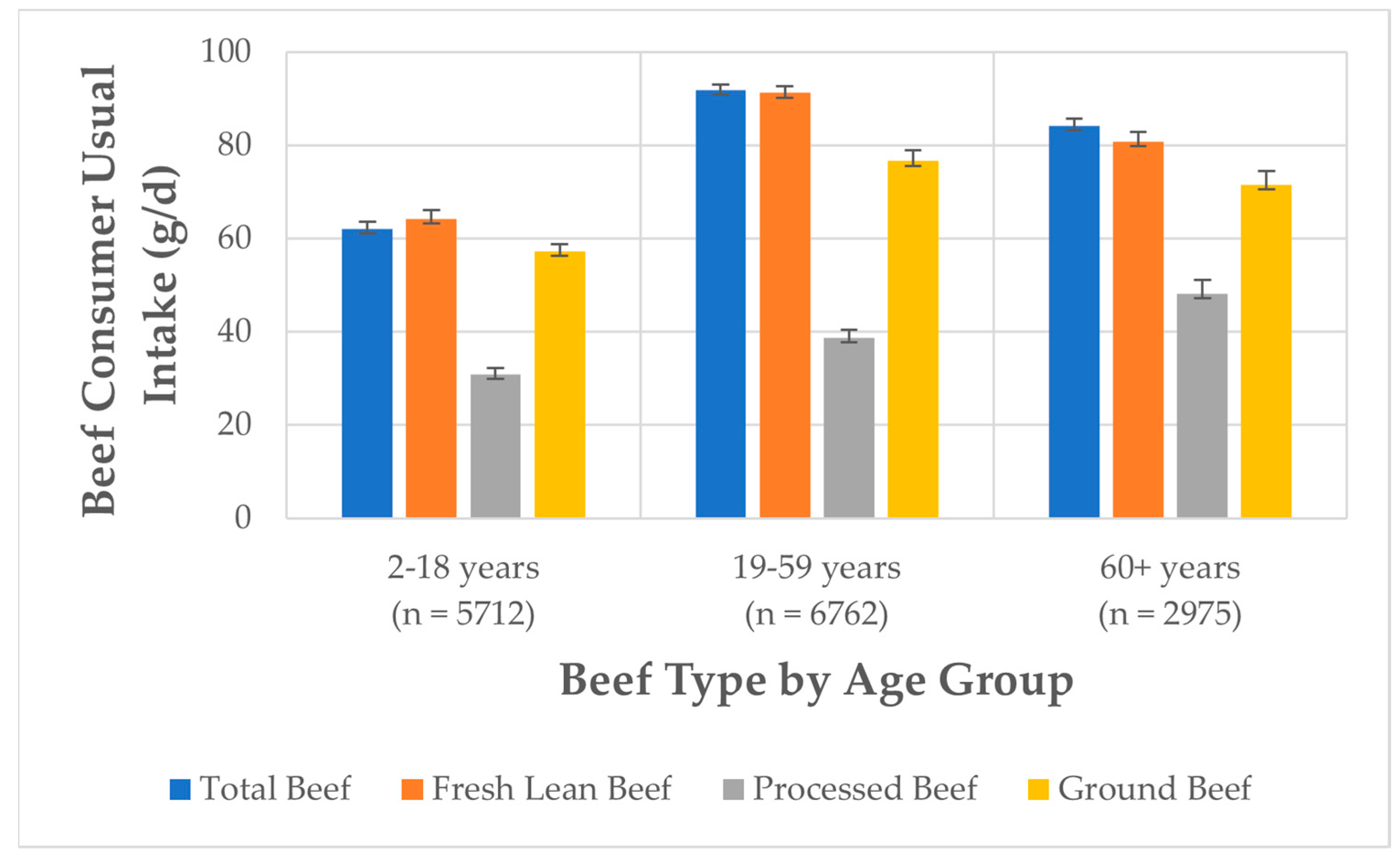
3.4. Beef Consumer Usual Intake of Beef, NHANES 2011–2018
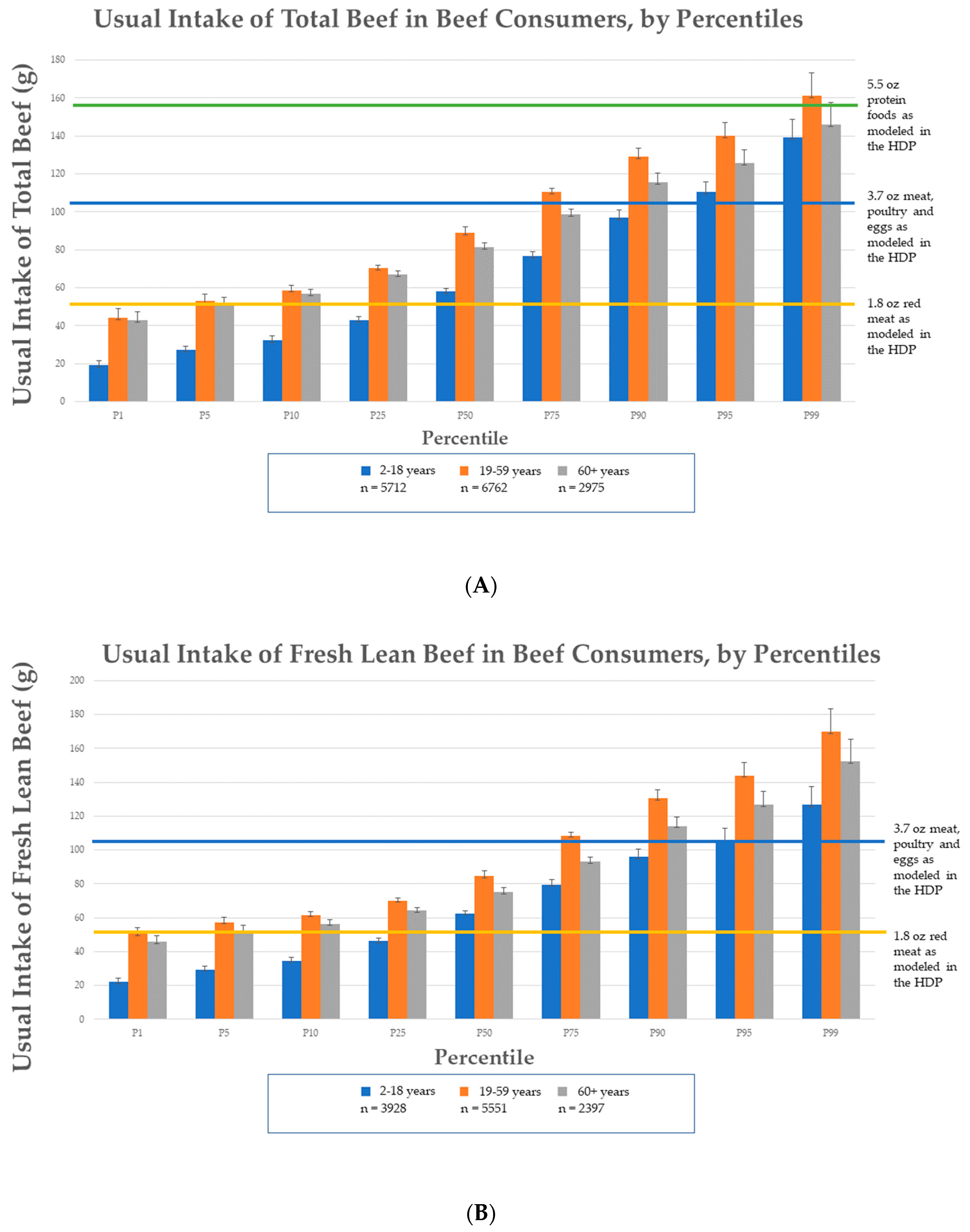
3.5. Comparison of Beef Consumer Usual Intakes to HDP Modeling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zanovec, M.; O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L., 3rd; Nicklas, T.A. Lean beef contributes significant amounts of key nutrients to the diets of US adults: National Health and Nutrition Examination Survey 1999–2004. Nutr. Res. 2010, 30, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. The Nutrient Rich Foods Index helps to identify healthy, affordable foods. Am. J. Clin. Nutr. 2010, 91, 1095S–1101S. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.A.; Clemens, J.C.; Friday, J.E.; Moshfegh, A.J. Food Patterns Equivalents Database 2017–2018: Methodology and User Guide. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 4 April 2023).
- Gifford, C.L.; O’Connor, L.E.; Campbell, W.W.; Woerner, D.R.; Belk, K.E. Broad and Inconsistent Muscle Food Classification Is Problematic for Dietary Guidance in the U.S. Nutrients 2017, 9, 1027. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.E.; Gifford, C.L.; Woerner, D.R.; Sharp, J.L.; Belk, K.E.; Campbell, W.W. Dietary Meat Categories and Descriptions in Chronic Disease Research Are Substantively Different within and between Experimental and Observational Studies: A Systematic Review and Landscape Analysis. Adv. Nutr. 2020, 11, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; Van Horn, L.; Wylie-Rosett, J. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025. Available online: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (accessed on 4 April 2023).
- O’Connor, L.E.; Campbell, W.W. Red Meat and Health: Getting to the Heart of the Matter. Nutr. Today 2017, 52, 167–173. [Google Scholar] [CrossRef]
- Carroll, A.E.; Doherty, T.S. Meat Consumption and Health: Food for Thought. Ann. Intern. Med. 2019, 171, 767–768. [Google Scholar] [CrossRef]
- Zeng, L.; Ruan, M.; Liu, J.; Wilde, P.; Naumova, E.N.; Mozaffarian, D.; Zhang, F.F. Trends in Processed Meat, Unprocessed Red Meat, Poultry, and Fish Consumption in the United States, 1999–2016. J. Acad. Nutr. Diet. 2019, 119, 1085–1098. [Google Scholar] [CrossRef]
- Ahluwalia, N.; Dwyer, J.; Terry, A.; Moshfegh, A.; Johnson, C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical Considerations, and Uses to Inform Public Policy. Adv. Nutr. 2016, 7, 121–134. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Zanovec, M.; Keast, D.R.; Fulgoni, V.L., 3rd; Nicklas, T.A. Nutrient contribution of total and lean beef in diets of US children and adolescents: National Health and Nutrition Examination Survey 1999–2004. Meat Sci. 2011, 87, 250–256. [Google Scholar] [CrossRef]
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef]
- O’Connor, L.E.; Herrick, K.A.; Parsons, R.; Reedy, J. Heterogeneity in Meat Food Groups Can Meaningfully Alter Population-Level Intake Estimates of Red Meat and Poultry. Front. Nutr. 2021, 8, 778369. [Google Scholar] [CrossRef]
- 2020 Dietary Guidelines Advisory Committee and Food Pattern Modeling Team. Food Pattern Modeling: Ages 2 Years and Older. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-07/FoodPatternModeling_Report_2YearsandOlder.pdf (accessed on 4 April 2023).
- Murphy, M.M.; Barraj, L.M.; Higgins, K.A. Healthy U.S.-style dietary patterns can be modified to provide increased energy from protein. Nutr. J. 2022, 21, 39. [Google Scholar] [CrossRef]
- Herrick, K.A.; Rossen, L.M.; Parsons, R.; Dodd, K.W. Estimating Usual Dietary in Take from National Health and Nutrition Examination Survey Data Using the National Cancer Institute Method. Available online: https://www.cdc.gov/nchs/data/series/sr_02/sr02_178.pdf (accessed on 4 April 2023).
- Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services. Available online: https://www.dietaryguidelines.gov/2020-advisory-committee-report (accessed on 4 April 2023).
- Kim, H.; Caulfield, L.E.; Rebholz, C.M.; Ramsing, R.; Nachman, K.E. Trends in types of protein in US adolescents and children: Results from the National Health and Nutrition Examination Survey 1999–2010. PLoS ONE 2020, 15, e0230686. [Google Scholar] [CrossRef]
- Frank, S.M.; Jaacks, L.M.; Batis, C.; Vanderlee, L.; Taillie, L.S. Patterns of Red and Processed Meat Consumption across North America: A Nationally Representative Cross-Sectional Comparison of Dietary Recalls from Canada, Mexico, and the United States. Int. J. Environ. Res. Public Health 2021, 18, 357. [Google Scholar] [CrossRef]
- Neff, R.A.; Edwards, D.; Palmer, A.; Ramsing, R.; Righter, A.; Wolfson, J. Reducing meat consumption in the USA: A nationally representative survey of attitudes and behaviours. Public Health Nutr. 2018, 21, 1835–1844. [Google Scholar] [CrossRef]
- Klurfeld, D.M. The whole food beef matrix is more than the sum of its parts. Crit. Rev. Food Sci. Nutr. 2022, 1–9. [Google Scholar] [CrossRef]
- Al-Shaar, L.; Satija, A.; Wang, D.D.; Rimm, E.B.; Smith-Warner, S.A.; Stampfer, M.J.; Hu, F.B.; Willett, W.C. Red meat intake and risk of coronary heart disease among US men: Prospective cohort study. BMJ 2020, 371, m4141. [Google Scholar] [CrossRef]
- Papier, K.; Fensom, G.K.; Knuppel, A.; Appleby, P.N.; Tong, T.Y.N.; Schmidt, J.A.; Travis, R.C.; Key, T.J.; Perez-Cornago, A. Meat consumption and risk of 25 common conditions: Outcome-wide analyses in 475,000 men and women in the UK Biobank study. BMC Med. 2021, 19, 53. [Google Scholar] [CrossRef]
- Hill, E.R.; O’Connor, L.E.; Wang, Y.; Clark, C.M.; McGowan, B.S.; Forman, M.R.; Campbell, W.W. Red and processed meat intakes and cardiovascular disease and type 2 diabetes mellitus: An umbrella systematic review and assessment of causal relations using Bradford Hill’s criteria. Crit. Rev. Food Sci. Nutr. 2022, 1–18. [Google Scholar] [CrossRef]
- Zeraatkar, D.; Han, M.A.; Guyatt, G.H.; Vernooij, R.W.M.; El Dib, R.; Cheung, K.; Milio, K.; Zworth, M.; Bartoszko, J.J.; Valli, C.; et al. Red and Processed Meat Consumption and Risk for All-Cause Mortality and Cardiometabolic Outcomes: A Systematic Review and Meta-analysis of Cohort Studies. Ann. Intern. Med. 2019, 171, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Lescinsky, H.; Afshin, A.; Ashbaugh, C.; Bisignano, C.; Brauer, M.; Ferrara, G.; Hay, S.I.; He, J.; Iannucci, V.; Marczak, L.B.; et al. Health effects associated with consumption of unprocessed red meat: A Burden of Proof study. Nat. Med. 2022, 28, 2075–2082. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.M.; Taillie, L.S.; Jaacks, L.M. How Americans eat red and processed meat: An analysis of the contribution of thirteen different food groups. Public Health Nutr. 2022, 25, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Harnack, L.; Mork, S.; Valluri, S.; Weber, C.; Schmitz, K.; Stevenson, J.; Pettit, J. Nutrient Composition of a Selection of Plant-Based Ground Beef Alternative Products Available in the United States. J. Acad. Nutr. Diet. 2021, 121, 2401–2408.e12. [Google Scholar] [CrossRef] [PubMed]
- Berryman, C.E.; Lieberman, H.R.; Fulgoni, V.L., 3rd; Pasiakos, S.M. Protein intake trends and conformity with the Dietary Reference Intakes in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2014. Am. J. Clin. Nutr. 2018, 108, 405–413. [Google Scholar] [CrossRef]
- Wolfe, R.R.; Cifelli, A.M.; Kostas, G.; Kim, I.Y. Optimizing Protein Intake in Adults: Interpretation and Application of the Recommended Dietary Allowance Compared with the Acceptable Macronutrient Distribution Range. Adv. Nutr. 2017, 8, 266–275. [Google Scholar] [CrossRef]
- Sayer, R.D.; Speaker, K.J.; Pan, Z.; Peters, J.C.; Wyatt, H.R.; Hill, J.O. Equivalent reductions in body weight during the Beef WISE Study: Beef’s role in weight improvement, satisfaction and energy. Obes. Sci. Pract. 2017, 3, 298–310. [Google Scholar] [CrossRef]
- Porter Starr, K.N.; Pieper, C.F.; Orenduff, M.C.; McDonald, S.R.; McClure, L.B.; Zhou, R.; Payne, M.E.; Bales, C.W. Improved Function With Enhanced Protein Intake per Meal: A Pilot Study of Weight Reduction in Frail, Obese Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1369–1375. [Google Scholar] [CrossRef]
- Porter Starr, K.N.; Connelly, M.A.; Orenduff, M.C.; McDonald, S.R.; Sloane, R.; Huffman, K.M.; Kraus, W.E.; Bales, C.W. Impact on cardiometabolic risk of a weight loss intervention with higher protein from lean red meat: Combined results of 2 randomized controlled trials in obese middle-aged and older adults. J. Clin. Lipidol. 2019, 13, 920–931. [Google Scholar] [CrossRef]
- Paddon-Jones, D.; Campbell, W.W.; Jacques, P.F.; Kritchevsky, S.B.; Moore, L.L.; Rodriguez, N.R.; van Loon, L.J. Protein and healthy aging. Am. J. Clin. Nutr. 2015, 101, 1339S–1345S. [Google Scholar] [CrossRef]
- Phillips, S.M.; Fulgoni, V.L., 3rd; Heaney, R.P.; Nicklas, T.A.; Slavin, J.L.; Weaver, C.M. Commonly consumed protein foods contribute to nutrient intake, diet quality, and nutrient adequacy. Am. J. Clin. Nutr. 2015, 101, 1346S–1352S. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Fulgoni, V.L., 3rd. Contribution of beef to key nutrient intakes in American adults: An updated analysis with NHANES 2011–2018. Nutr. Res. 2022, 105, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef]
- An, R.; Nickols-Richardson, S.M.; Alston, R.J.; Shen, S. Fresh and Fresh Lean Beef Intake in Relation to Functional Limitations among US Older Adults, 2005–2016. Am. J. Health Behav. 2019, 43, 729–738. [Google Scholar] [CrossRef]
- Hawley, A.L.; Liang, X.; Børsheim, E.; Wolfe, R.R.; Salisbury, L.; Hendy, E.; Wu, H.; Walker, S.; Tacinelli, A.M.; Baum, J.I. The potential role of beef and nutrients found in beef on outcomes of wellbeing in healthy adults 50 years of age and older: A systematic review of randomized controlled trials. Meat Sci. 2022, 189, 108830. [Google Scholar] [CrossRef]
- You, W.; Henneberg, R.; Saniotis, A.; Ge, Y.; Henneberg, M. Total Meat Intake is Associated with Life Expectancy: A Cross-Sectional Data Analysis of 175 Contemporary Populations. Int. J. Gen. Med. 2022, 15, 1833–1851. [Google Scholar] [CrossRef]
- An, R.; Nickols-Richardson, S.; Alston, R.; Shen, S.; Clarke, C. Total, Fresh, Lean, and Fresh Lean Beef Consumption in Relation to Nutrient Intakes and Diet Quality among U.S. Adults, 2005–2016. Nutrients 2019, 11, 563. [Google Scholar] [CrossRef]
- Nicklas, T.A.; O’Neil, C.E.; Zanovec, M.; Keast, D.R.; Fulgoni, V.L., 3rd. Contribution of beef consumption to nutrient intake, diet quality, and food patterns in the diets of the US population. Meat Sci. 2012, 90, 152–158. [Google Scholar] [CrossRef]
- O’Connor, L.E.; Wambogo, E.A.; Herrick, K.A.; Parsons, R.; Reedy, J. A Standardized Assessment of Processed Red Meat and Processed Poultry Intake in the US Population Aged ≥2 Years Using NHANES. J. Nutr. 2022, 152, 190–199. [Google Scholar] [CrossRef]
- Taylor, E.V.; Holt, K.G.; Mahon, B.E.; Ayers, T.; Norton, D.; Gould, L.H. Ground beef consumption patterns in the United States, FoodNet, 2006 through 2007. J. Food Prot. 2012, 75, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Fehrenbach, K.S.; Righter, A.C.; Santo, R.E. A critical examination of the available data sources for estimating meat and protein consumption in the USA. Public Health Nutr. 2016, 19, 1358–1367. [Google Scholar] [CrossRef] [PubMed]
- Leroy, F.; Cofnas, N. Should dietary guidelines recommend low red meat intake? Crit. Rev. Food Sci. Nutr. 2020, 60, 2763–2772. [Google Scholar] [CrossRef] [PubMed]
- Leme, A.C.; Baranowski, T.; Thompson, D.; Philippi, S.; O’Neil, C.E.; Fulgoni, V.L., 3rd; Nicklas, T.A. Food Sources of Shortfall Nutrients Among US Adolescents: National Health and Nutrition Examination Survey (NHANES) 2011–2014. Fam. Community Health 2020, 43, 59–73. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Beef Variable | Related FPID Variables | Calculation |
|---|---|---|
| Total Beef | pf_meat 1; pf_cured meat 2 | Descriptions examined to determine the percentage of each variable assumed to be beef. Percentage of beef applied. Total includes solid fat in beef in excess of 2.63 g per ounce (9.28%) [i.e., discretionary fat] and lean beef portion. |
| Processed Beef | pf_cured meat | Cured meat includes frankfurters, sausages, corned beef, and luncheon meat. Descriptions examined to determine the percentage of each variable assumed to be beef. Percentage of beef applied. Total includes solid fat in beef in excess of 2.63 g per ounce (9.28%) [i.e., discretionary fat] and lean beef portion. |
| Fresh lean beef | pf_meat | Solid fat in excess of 2.63 g per ounce (9.28%) is subtracted, fresh lean portion remains |
| Ground beef | pf_meat; the descriptions of ingredients in FPID helped delineate ground beef products (i.e., ground beef or similar term used in food ingredient description) | Total includes solid fat in beef in excess of 2.63 g per ounce (9.28%) [i.e., discretionary fat] and lean beef portion. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, C.S.; Fulgoni, V.L., III; Van Elswyk, M.E.; McNeill, S.H. Trends in Beef Intake in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2018. Nutrients 2023, 15, 2475. https://doi.org/10.3390/nu15112475
Lau CS, Fulgoni VL III, Van Elswyk ME, McNeill SH. Trends in Beef Intake in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2018. Nutrients. 2023; 15(11):2475. https://doi.org/10.3390/nu15112475
Chicago/Turabian StyleLau, Clara S., Victor L. Fulgoni, III, Mary E. Van Elswyk, and Shalene H. McNeill. 2023. "Trends in Beef Intake in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2018" Nutrients 15, no. 11: 2475. https://doi.org/10.3390/nu15112475
APA StyleLau, C. S., Fulgoni, V. L., III, Van Elswyk, M. E., & McNeill, S. H. (2023). Trends in Beef Intake in the United States: Analysis of the National Health and Nutrition Examination Survey, 2001–2018. Nutrients, 15(11), 2475. https://doi.org/10.3390/nu15112475