
Vitamin D Deficiency in Chronic Childhood Disorders: Importance of Screening and Prevention


Abstract
:1. Introduction
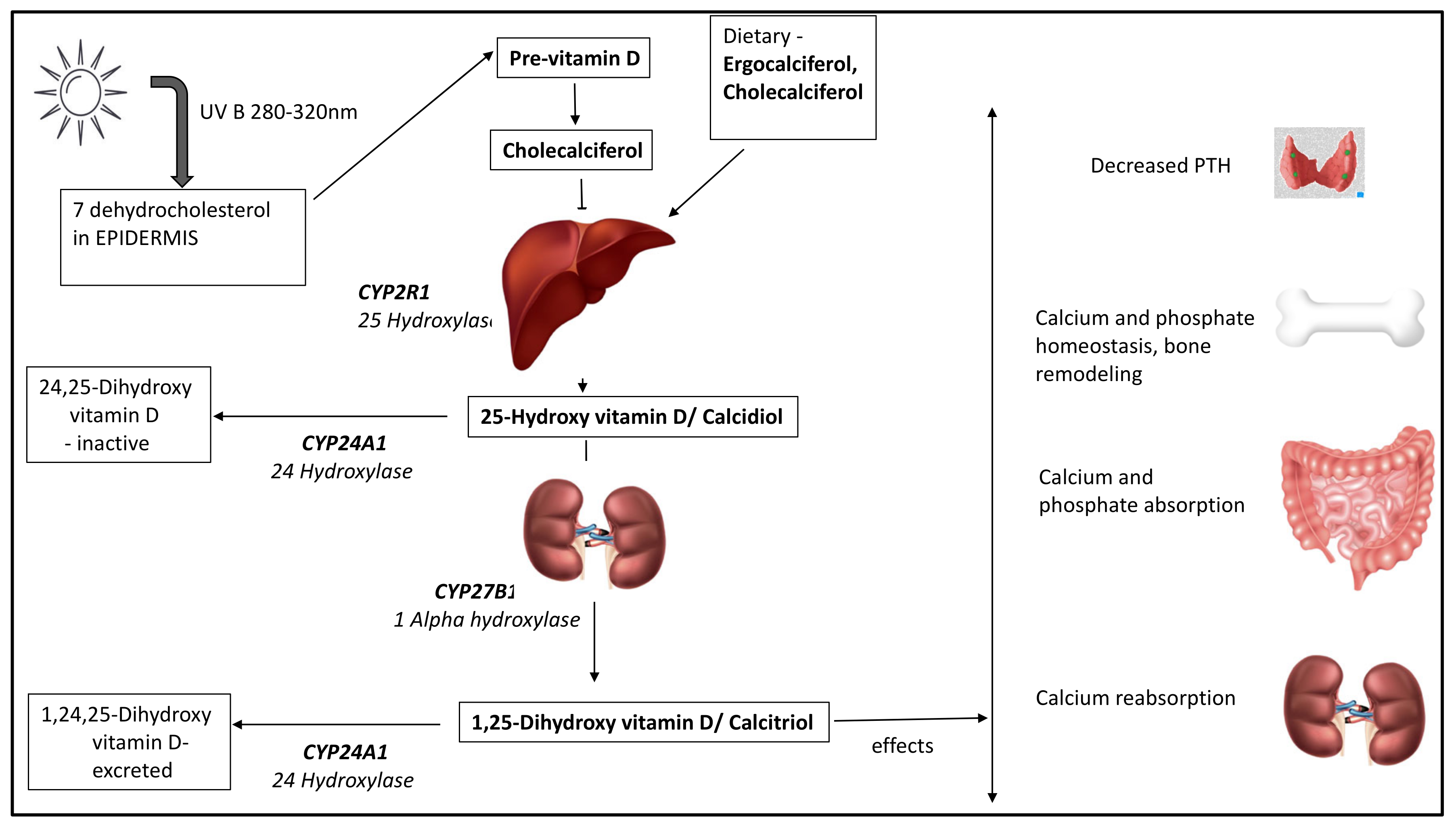
2. Vitamin D Metabolism
Sources of Vitamin D
3. Vitamin D Deficiency
3.1. Identifying the High-Risk Population
3.2. Biochemical Definition of Vitamin D Deficiency
- vitamin D sufficiency > 50 nmol/L (20 ng/mL);
- vitamin D insufficiency: 30–50 nmol/L (12–20 ng/mL);
- vitamin D deficiency < 30 nmol/L (12 ng/mL).
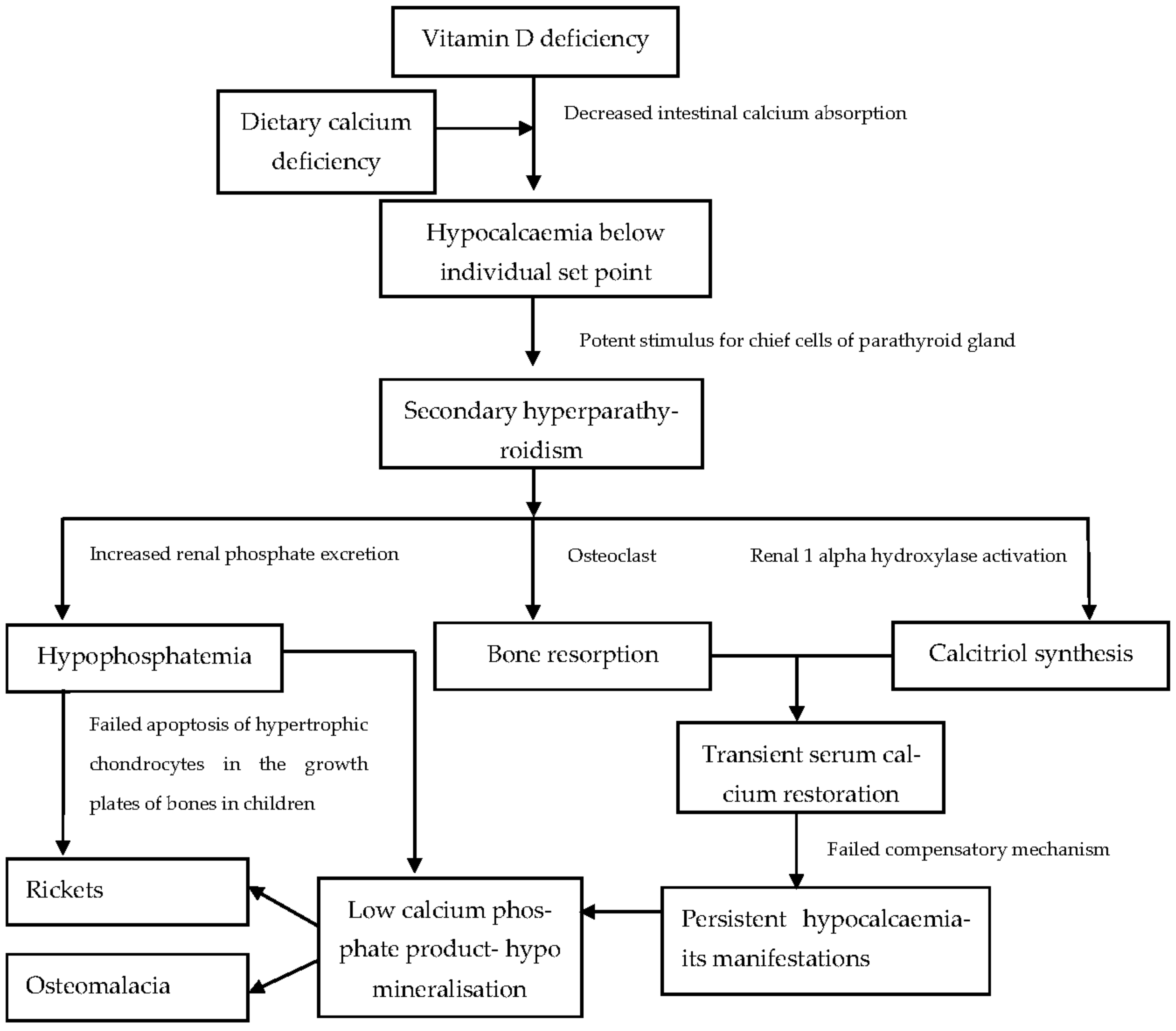
3.3. Pathophysiology of Vitamin-D-Deficient State
- Hypocalcaemia
- Secondary Hyperparathyroidism
- High Alkaline Phosphatase (ALP) or Hyperphosphatasaemia
- Hypophosphataemia
- Skeletal Hypomineralisation
3.4. Clinical Syndrome of VDD
4. Vitamin D and Chronic Liver Disease
4.1. Pathophysiologic Mechanisms Involved in HO
- Liver disease: Depending on the aetiopathogenesis of hepatic disease, the mechanism by which bone health is affected may vary. However, the final target is the bone remodelling unit (the site where remodelling occurs), resulting in an imbalance between bone formation and resorption [43]. Advanced liver disease has been associated with increased levels of sclerostin (secreted by osteocytes), which blocks the molecular signalling pathways necessary for osteoblast differentiation [44]. Autoimmune hepatitis and hepatitis C result in the release of cytokines and inflammatory factors (Interleukin 6, Interleukin 1b, Tumour necrosis factor alpha) having bone-resorptive action and, more importantly, via secretion of RANKL (receptor activator of nuclear factor kappa beta) by activated T-lymphocytes and fibroblasts, which activates osteoclasts [41,45]. Infiltrative and cholestatic diseases also negatively impact osteoblast differentiation and proliferation [46].
- Vitamin D deficiency: VDD is a key player in the development of HO. A higher prevalence of VDD in children and adults with chronic hepatic disease has been reported in the literature [47,48,49]. In a large cohort of patients with CLD (n = 118), Lee et al. observed that cirrhosis, African American race and female gender were independent risk determinants for severe VDD (25OHD < 17.5 nmol/L or 7 ng/mL) [49]. Decreased 25-hydroxylase activity, the malabsorption of fat-soluble vitamins, relatively insufficient vitamin D supplementation, malnutrition, low albumin and DBP, and poor sunlight exposure are some of the factors contributing to VDD in long-standing liver disease [50,51,52,53].
- Other factors: Associated growth failure and pubertal delay [54] may contribute to adverse bone health due to the absence of an anabolic effect of Insulin-like growth factor 1 (IGF-1) and sex hormones on bones [55]. Sarcopenia or low muscle mass and strength, due to impaired protein synthesis in CLD, contributes to low bone mass [53]. Steroid therapy for hepatic disease negatively impacts bone mass by enhancing the lifespan of existing osteoclasts, increasing the apoptosis of osteocytes and osteoblasts [56], supressing the formation of osteoblasts in the bone marrow and promoting loss of calcium through the kidneys and gut [57].
4.2. Biochemical and Clinical Manifestations
4.3. Recommendations for Monitoring and Treatment of VDD in CLD
5. Vitamin D Deficiency in Chronic Kidney Disease
5.1. Pathophysiology of Renal Osteodystrophy
5.2. Biochemical and Clinical Manifestations
5.3. Recommendations for Monitoring and Treatment of VDD in CKD
6. Vitamin D and Chronic Malabsorptive Disorders
6.1. Pathophysiology of VDD in Chronic GI Disorders
- Insufficient dietary intake of calcium and vitamin D along with higher requirements.
- Disrupted enterohepatic circulation [85].
- Limited outdoor activities and sunlight exposure due to the chronic debilitating nature of the condition.
6.2. Biochemical and Clinical Manifestations
6.3. Recommendations for Prevention and Treatment of VDD in Chronic GI Disorders
7. Vitamin D in Overweight and Obesity
7.1. Pathophysiology of VDD in Childhood Obesity
- Sequestration and volumetric dilution effect: Increased deposition of vitamin D in adipose tissue makes it less bioavailable in obese individuals [99]. In simple terms, as compared to lean individuals, in obese individuals, vitamin D gets distributed in a larger volume of fat tissue, resulting in lower serum levels [100].
- Insufficient routine supplementation: The requirement of vitamin D in obese individuals is higher and often routine doses of supplementation or treatment may not ensure adequacy [105].
7.2. Clinical Manifestations
7.3. Recommendations for Prevention and Treatment of VDD in Childhood Obesity
8. Vitamin D and Chronic Neurologic and Myopathic Illnesses
9. Vitamin D and Chronic Skin Diseases
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, G. 100 Years of vitamin D: Historical aspects of vitamin D. Endocr. Connect. 2022, 11, e210594. [Google Scholar] [CrossRef] [PubMed]
- Wolf, G. The discovery of vitamin D: The contribution of Adolf Windaus. J. Nutr. 2004, 134, 1299–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, G.; Strugnell, S.A.; DeLuca, H.F. Current Understanding of the Molecular Actions of Vitamin D. Physiol. Rev. 1998, 78, 1193–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCollum, E.V.; Pitz, W.; Simmonds, N.; Becker, J.E.; Shipley, P.G.; Bunting, R.W. The effect of additions of fluorine to the diet of the rat on the quality of the teeth. 1925. Studies on experimental rickets. XXI. An experimental demonstration of the existence of a vitamin which promotes calcium deposition. 1922. The effect of additions of fluorine to the diet of the rat on the quality of the teeth. 1925. J. Biol. Chem. 2002, 277, E8. [Google Scholar] [PubMed]
- Jones, G. The discovery and synthesis of the nutritional factor vitamin D. Int. J. Paleopathol. 2018, 23, 96–99. [Google Scholar] [CrossRef]
- Lawson, D.E.M.; Wilson, P.W.; Kodicek, E. Metabolism of vitamin D. A new cholecalciferol metabolite, involving loss of hydrogen at C-1, in chick intestinal nuclei. Biochem. J. 1969, 115, 269–277. [Google Scholar] [CrossRef] [Green Version]
- DeLuca, H.F.; Zierold, C. Mechanisms and functions of vitamin D. Nutr. Rev. 1998, 56, S4–S10, discussion S54–S75. [Google Scholar] [CrossRef]
- DeLuca, H.F.; Holick, M.F.; Schnoes, H.K.; Suda, T.; Cousins, R.J. Isolation and identification of 1,25-dihydroxycholecalciferol. A metabolite of vitamin D active in intestine. Biochemistry 1971, 10, 2799–2804. [Google Scholar] [CrossRef]
- Inouye, K.; Sakaki, T. Enzymatic studies on the key enzymes of vitamin D metabolism; 1 alpha-hydroxylase (CYP27B1) and 24-hydroxylase (CYP24). Biotechnol. Annu. Rev. 2001, 7, 179–194. [Google Scholar]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Fletcher, J.; Bishop, E.L.; Harrison, S.R.; Swift, A.; Cooper, S.C.; Dimeloe, S.K.; Raza, K.; Hewison, M. Autoimmune disease and interconnections with vitamin D. Endocr. Connect. 2022, 11, e210554. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.H.; Fang, T.C. The pleiotropic effect of vitamin D. ISRN Nephrol. 2013, 2013, 898125. [Google Scholar] [CrossRef] [PubMed]
- Ultraviolet Radiation, Vitamin D and Health Report of the Independent Advisory Group on Non-Ionising Radiation. 2017. Available online: https://www.gov.uk/government/publications/ultraviolet-radiation-and-vitamin-d-the-effects-on-health (accessed on 15 May 2023).
- Uday, S.; Högler, W. Nutritional rickets & osteomalacia: A practical approach to management. Indian J. Med. Res. 2020, 152, 356–367. [Google Scholar] [PubMed]
- Al-Daghri, N.M.; Yakout, S.; Sabico, S.; Wani, K.; Hussain, S.D.; Aljohani, N.; Uday, S.; Högler, W. Establishing the Prevalence of Osteomalacia in Arab Adolescents Using Biochemical Markers of Bone Health. Nutrients 2022, 14, 5354. [Google Scholar] [CrossRef] [PubMed]
- Kift, R.; Berry, J.L.; Vail, A.; Durkin, M.T.; Rhodes, L.E.; Webb, A.R. Lifestyle factors including less cutaneous sun exposure contribute to starkly lower vitamin D levels in U.K. South Asians compared with the white population. Br. J. Dermatol. 2013, 169, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Uday, S.; Högler, W. Prevention of rickets and osteomalacia in the UK: Political action overdue. Arch. Dis. Child. 2018, 103, 901–906. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. Horm. Res. Paediatr. 2016, 85, 83–106. [Google Scholar] [CrossRef] [Green Version]
- Arundel, P.; Shaw, N. Vitamin D and Bone Health: A Practical Clinical Guideline for Patient Management in Children and Young People Camerton, Somerset, England, 2018. Available online: https://theros.org.uk/media/54vpzzaa/ros-vitamin-d-and-bone-health-in-children-november-2018.pdf (accessed on 7 May 2023).
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Dabas, A.; Seth, A.; Bhatia, V.L.; Khadgawat, R.; Kumar, P.; Balasubramanian, S.; Khadilkar, V.; Mallikarjuna, H.B.; Godbole, T.; et al. Indian Academy of Pediatrics Revised (2021) Guidelines on Prevention and Treatment of Vitamin D Deficiency and Rickets. Indian Pediatr. 2022, 59, 142–158. [Google Scholar] [CrossRef]
- Holick, M.F.; MacLaughlin, J.A.; Clark, M.B.; Holick, S.A.; Potts, J.T., Jr.; Anderson, R.R.; Blank, I.H.; Parrish, J.A.; Elias, P. Photosynthesis of previtamin D3 in human skin and the physiologic consequences. Science 1980, 210, 203–205. [Google Scholar] [CrossRef]
- Boyle, I.T.; Gray, R.W.; DeLuca, H.F. Regulation by calcium of in vivo synthesis of 1,25-dihydroxycholecalciferol and 21,25-dihydroxycholecalciferol. Proc. Natl. Acad. Sci. USA 1971, 68, 2131–2134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atapattu, N.; Shaw, N.; Högler, W. Relationship between serum 25-hydroxyvitamin D and parathyroid hormone in the search for a biochemical definition of vitamin D deficiency in children. Pediatr. Res. 2013, 74, 552–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakos, S.; Dhawan, P.; Porta, A.; Mady, L.J.; Seth, T. Vitamin D and intestinal calcium absorption. Mol. Cell. Endocrinol. 2011, 347, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikle, D.D. Vitamin D metabolism, mechanism of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.H.; May, B.K.; Morris, H.A. Vitamin D metabolism: New concepts and clinical implications. Clin. Biochem. Rev. 2003, 24, 13–26. [Google Scholar]
- Nadar, R.; Uday, S. A clinician’s guide to vitamin D and bone health in children. Paediatr. Child. Health 2021, 31, 364–370. [Google Scholar] [CrossRef]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Haffner, D.; Leifheit-Nestler, M.; Grund, A.; Schnabel, D. Rickets guidance: Part I-diagnostic workup. Pediatr. Nephrol. 2022, 37, 2013–2036. [Google Scholar] [CrossRef]
- Egbuna, O.I.; Brown, E.M. Hypercalcaemic and hypocalcaemic conditions due to calcium-sensing receptor mutations. Best. Pract. Res. Clin. Rheumatol. 2008, 22, 129–148. [Google Scholar] [CrossRef] [Green Version]
- Cannalire, G.; Pilloni, S.; Esposito, S.; Biasucci, G.; Di Franco, A.; Street, M.E. Alkaline phosphatase in clinical practice in childhood: Focus on rickets. Front. Endocrinol. 2023, 14, 1111445. [Google Scholar] [CrossRef]
- Goretti Penido, M.; Alon, U.S. Phosphate homeostasis and its role in bone health. Pediatr. Nephrol. 2012, 27, 2039–2048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, W.L.; Arsenault, A.L.; Hodsman, A.B. Rearrangement of the metaphyseal vasculature of the rat growth plate in rickets and rachitic reversal: A model of vascular arrest and angiogenesis renewed. Anat. Rec. 1991, 229, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Uday, S.; Högler, W. Spot the silent sufferers: A call for clinical diagnostic criteria for solar and nutritional osteomalacia. J. Steroid Biochem. Mol. Biol. 2019, 188, 141–146. [Google Scholar] [CrossRef]
- Ladhani, S.; Srinivasan, L.; Buchanan, C.; Allgrove, J. Presentation of vitamin D deficiency. Arch. Dis. Child. 2004, 89, 781–784. [Google Scholar] [CrossRef] [Green Version]
- Narchi, H.; El Jamil, M.; Kulaylat, N. Symptomatic rickets in adolescence. Arch. Dis. Child. 2001, 84, 501–503. [Google Scholar] [CrossRef] [Green Version]
- Julies, P.; Lynn, R.M.; Pall, K.; Leoni, M.; Calder, A.; Mughal, Z.; Shaw, N.; McDonnell, C.; McDevitt, H.; Blair, M. Nutritional rickets under 16 years: UK surveillance results. Arch. Dis. Child. 2020, 105, 587–592. [Google Scholar] [CrossRef]
- López-Larramona, G.; Lucendo, A.J.; González-Castillo, S.; Tenias, J.M. Hepatic osteodystrophy: An important matter for consideration in chronic liver disease. World J. Hepatol. 2011, 3, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Wesseling-Perry, K.; Pereira, R.C.; Tseng, C.H.; Elashoff, R.; Zaritsky, J.J.; Yadin, O.; Sahney, S.; Gales, B.; Jüppner, H.; Salusky, I.B. Early skeletal and biochemical alterations in pediatric chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2012, 7, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Collier, J. Bone disorders in chronic liver disease. Hepatology 2007, 46, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Therneau, T.M.; Jorgensen, A.; DeSotel, C.K.; Egan, K.S.; Dickson, E.R.; Hay, J.E.; Lindor, K.D. Bone disease in patients with primary sclerosing cholangitis: Prevalence, severity and prediction of progression. J. Hepatol. 1998, 29, 729–735. [Google Scholar] [CrossRef]
- Jeong, H.M.; Kim, D.J. Bone Diseases in Patients with Chronic Liver Disease. Int. J. Mol. Sci. 2019, 20, 4270. [Google Scholar] [CrossRef] [Green Version]
- Rhee, Y.; Kim, W.J.; Han, K.J.; Lim, S.K.; Kim, S.H. Effect of liver dysfunction on circulating sclerostin. J. Bone Miner. Metab. 2014, 32, 545–549. [Google Scholar] [CrossRef]
- Handzlik-Orlik, G.; Holecki, M.; Wilczyński, K.; Duława, J. Osteoporosis in liver disease: Pathogenesis and management. Ther. Adv. Endocrinol. Metab. 2016, 7, 128–135. [Google Scholar] [CrossRef] [Green Version]
- Valenti, L.; Varenna, M.; Fracanzani, A.L.; Rossi, V.; Fargion, S.; Sinigaglia, L. Association between iron overload and osteoporosis in patients with hereditary hemochromatosis. Osteoporos. Int. 2009, 20, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Arteh, J.; Narra, S.; Nair, S. Prevalence of vitamin D deficiency in chronic liver disease. Dig. Dis. Sci. 2010, 55, 2624–2628. [Google Scholar] [CrossRef] [PubMed]
- Stokes, C.S.; Volmer, D.A.; Grünhage, F.; Lammert, F. Vitamin D in chronic liver disease. Liver Int. 2013, 33, 338–352. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Jalaludin, M.Y.; Wong, S.Y.; Ong, S.Y.; Foo, H.W.; Ng, R.T. Vitamin D non-sufficiency is prevalent in children with chronic liver disease in a tropical country. Pediatr. Neonatol. 2019, 60, 12–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández, N.F.; Linares Torres, P.; Joáo Matias, D.; Jorquera Plaza, F.; Olcoz Goñi, J.L. Vitamin D deficiency in chronic liver disease, clinical-epidemiological analysis and report after vitamin d supplementation. Gastroenterol. Hepatol. 2016, 39, 305–310. [Google Scholar] [CrossRef]
- Venu, M.; Martin, E.; Saeian, K.; Gawrieh, S. High prevalence of vitamin A deficiency and vitamin D deficiency in patients evaluated for liver transplantation. Liver Transpl. 2013, 19, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, C.G.; Götze, O.; Geier, A. Molecular changes in hepatic metabolism and transport in cirrhosis and their functional importance. World J. Gastroenterol. 2016, 22, 72–88. [Google Scholar] [CrossRef]
- Bering, T.; Diniz, K.G.D.; Coelho, M.P.P.; Vieira, D.A.; Soares, M.M.S.; Kakehasi, A.M.; Correia, M.I.T.D.; Teixeira, R.; Queiroz, D.M.M.; Rocha, G.A.; et al. Association between pre-sarcopenia, sarcopenia, and bone mineral density in patients with chronic hepatitis C. J. Cachexia Sarcopenia Muscle 2018, 9, 255–268. [Google Scholar] [CrossRef] [Green Version]
- Kyrana, E. Impact of Chronic Liver Disease on Nutrition, Growth and Puberty in Adolescence. In Liver Disease in Adolescence; Springer: Berlin/Heidelberg, Germany, 2022; pp. 3–19. Available online: https://link.springer.com/10.1007/978-3-030-98808-1_1 (accessed on 15 May 2023).
- Högler, W.; Baumann, U.; Kelly, D. Growth and bone health in chronic liver disease and following liver transplantation in children. Pediatr. Endocrinol. Rev. 2010, 7, 266–274. [Google Scholar]
- Weinstein, R.S.; Jilka, R.L.; Parfitt, A.M.; Manolagas, S.C. Inhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on bone. J. Clin. Investig. 1998, 102, 274–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, T.J.; Halstead, L.R.; Teitelbaum, S.L.; Hahn, B.H. Altered mineral metabolism in glucocorticoid-induced osteopenia. Effect of 25-hydroxyvitamin D administration. J. Clin. Investig. 1979, 64, 655–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Antiga, L.; Moniz, C.; Buxton-Thomas, M.; Cheeseman, P.; Gray, B.; Abraha, H.; Baker, A.J.; Heaton, N.D.; Rela, M.; Mieli-Vergani, G.; et al. Bone mineral density and height gain in children with chronic cholestatic liver disease undergoing transplantation. Transplantation 2002, 73, 1788–1793. [Google Scholar] [CrossRef]
- Helenius, I.; Remes, V.; Salminen, S.; Valta, H.; Mäkitie, O.; Holmberg, C.; Palmu, P.; Tervahartiala, P.; Sarna, S.; Helenius, M.; et al. Incidence and predictors of fractures in children after solid organ transplantation: A 5-year prospective, population-based study. J. Bone Miner. Res. 2006, 21, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Mouzaki, M.; Bronsky, J.; Gupte, G.; Hojsak, I.; Jahnel, J.; Pai, N.; Quiros-Tejeira, R.E.; Wieman, R.; Sundaram, S. Nutrition Support of Children with Chronic Liver Diseases: A Joint Position Paper of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 498–511. [Google Scholar] [CrossRef] [Green Version]
- Guichelaar, M.M.J.; Schmoll, J.; Malinchoc, M.; Hay, J.E. Fractures and avascular necrosis before and after orthotopic liver transplantation: Long-term follow-up and predictive factors. Hepatology 2007, 46, 1198–1207. [Google Scholar] [CrossRef]
- Mitchell, D.M.; Regan, S.; Cooley, M.R.; Lauter, K.B.; Vrla, M.C.; Becker, C.B.; Burnett-Bowie, S.A.; Mannstadt, M. Long-term follow-up of patients with hypoparathyroidism. J. Clin. Endocrinol. Metab. 2012, 97, 4507–4514. [Google Scholar] [CrossRef] [Green Version]
- Alonso, E.M. Growth and developmental considerations in pediatric liver transplantation. Liver Transpl. 2008, 14, 585–591. [Google Scholar] [CrossRef]
- Feranchak, A.P.; Suchy, F.J.; Sokol, R.J. Liver Disease in Children, 4th ed.; Suchy, F.J., Sokol, R.J., Balistreri, W.F., Eds.; Cambridge University Press: New York, NY, USA, 2007; pp. 111–139. Available online: https://www.cambridge.org/core/product/identifier/9780511547409/type/book (accessed on 15 May 2022).
- Bilezikian, J.P.; Formenti, A.M.; Adler, R.A.; Binkley, N.; Bouillon, R.; Lazaretti-Castro, M.; Marcocci, C.; Napoli, N.; Rizzoli, R.; Giustina, A. Vitamin D: Dosing, levels, form, and route of administration: Does one approach fit all? Rev. Endocr. Metab. Disord. 2021, 22, 1201–1218. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, T.O.; Imel, E.A.; Holm, I.A.; Jan de Beur, S.M.; Insogna, K.L. A clinician’s guide to X-linked hypophosphatemia. J. Bone Miner. Res. 2011, 26, 1381–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esfandiar, N.; Shakiba, M.; Mirzaei, Z. Vitamin D Deficiency in Children with Chronic Kidney Disease. J. Clin. Diagn. Res. 2019, 123, 791–796. [Google Scholar] [CrossRef]
- Dyussenova, S.B.; Gordiyenko, M.Y.; Serikova, G.B.; Turlybekova, S.A.; Issayeva, A.A.; Yerimbetova, N.A.; Goroshko, V.O. Vitamin D Deficiency in Children with Chronic Renal Disease. Open. Access. Maced. J. Med. Sci. 2021, 9, 1751–1757. [Google Scholar] [CrossRef]
- Menon, S.; Valentini, R.P.; Hidalgo, G.; Peschansky, L.; Mattoo, T.K. Vitamin D insufficiency and hyperparathyroidism in children with chronic kidney disease. Pediatr. Nephrol. 2008, 23, 1831–1836. [Google Scholar] [CrossRef]
- Balmukhanova, A.; Kabulbayev, K.; Alpay, H.; Kanatbayeva, A.; Balmukhanova, A. FGF-23 and Phosphate in Children with Chronic Kidney Disease: A Cross-Sectional Study in Kazakhstan. Medicina 2020, 57, 15. [Google Scholar] [CrossRef]
- Shroff, R.; Wan, M.; Nagler, E.V.; Bakkaloglu, S.; Fischer, D.C.; Bishop, N.; Cozzolino, M.; Bacchetta, J.; Edefonti, A.; Stefanidis, C.J.; et al. Clinical practice recommendations for native vitamin D therapy in children with chronic kidney disease Stages 2–5 and on dialysis. Nephrol. Dial. Transplant. 2017, 32, 1098–1113. [Google Scholar] [CrossRef] [Green Version]
- Levin, A.; Bakris, G.L.; Molitch, M.; Smulders, M.; Tian, J.; Williams, L.A.; Andress, D.L. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease. Kidney Int. 2007, 71, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Suh, J.S. Diagnosis and Management of Chronic Kidney Disease-Mineral Bone Disease in Children. Child. Kidney Dis. 2020, 24, 14–18. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef] [Green Version]
- National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am. J. Kidney Dis. 2003, 42, S1–S201. [Google Scholar] [CrossRef]
- Haffner, D.; Leifheit-Nestler, M. Treatment of hyperphosphatemia: The dangers of aiming for normal PTH levels. Pediatr. Nephrol. 2020, 35, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Shroff, R.; Wan, M.; Gullett, A.; Ledermann, S.; Shute, R.; Knott, C.; Wells, D.; Aitkenhead, H.; Manickavasagar, B.; van’t Hoff, W.; et al. Ergocalciferol supplementation in children with CKD delays the onset of secondary hyperparathyroidism: A randomized trial. Clin. J. Am. Soc. Nephrol. 2012, 7, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Jean, G.; Souberbielle, J.C.; Chazot, C. Vitamin D in Chronic Kidney Disease and Dialysis Patients. Nutrients 2017, 9, 328. [Google Scholar] [CrossRef] [Green Version]
- Drube, J.; Wan, M.; Bonthuis, M.; Wühl, E.; Bacchetta, J.; Santos, F.; Grenda, R.; Edefonti, A.; Harambat, J.; Shroff, R.; et al. Clinical practice recommendations for growth hormone treatment in children with chronic kidney disease. Nat. Rev. Nephrol. 2019, 15, 577–589. [Google Scholar] [CrossRef] [Green Version]
- Sylvester, F.A.; Wyzga, N.; Hyams, J.S.; Davis, P.M.; Lerer, T.; Vance, K.; Hawker, G.; Griffiths, A.M. Natural history of bone metabolism and bone mineral density in children with inflammatory bowel disease. Inflamm. Bowel Dis. 2007, 13, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Javorsky, B.R.; Maybee, N.; Padia, S.; Dalkin, A.C. Vitamin D Deficiency in Gastrointestinal Disease. Pract. Gastroenterol. 2006, 30, 52–72. [Google Scholar]
- IBD Working Group of British Society of Paediatric Gastroenterology Hepatology and Nutrition. Vitamin D in Paediatric Inflammatory Bowel Disease. 2019. Available online: https://bspghan.org.uk/wp-content/uploads/2020/11/BSPGHAN-statement-Vitamin-D-in-IBD-December-2019.pdf (accessed on 16 May 2023).
- Akhshayaa, G.; Seth, A.; Kumar, P.; Jain, A. Prevalence and management of vitamin D deficiency in children with newly diagnosed coeliac disease: Cohort study. Paediatr. Int. Child. Health 2021, 41, 247–252. [Google Scholar]
- De Prisco, C.; Levine, S.N. Metabolic bone disease after gastric bypass surgery for obesity. Am. J. Med. Sci. 2005, 329, 57–61. [Google Scholar] [CrossRef]
- Staun, M.; Jarnum, S. Measurement of the 10,000-molecular weight calcium-binding protein in small-intestinal biopsy specimens from patients with malabsorption syndromes. Scand. J. Gastroenterol. 1988, 23, 827–832. [Google Scholar] [CrossRef]
- Scott, E.M. Guidelines for osteoporosis in coeliac disease and inflammatory bowel disease. Gut 2000, 46, i1–i8. [Google Scholar] [CrossRef]
- Crabtree, N.; Hogler, W.; Chapman, D.; Walford, J.; Shaw, N. Vertebral Fractures in children with chronic inflammatory and/or disabling conditions: The SNAP study. Bone Abstr. 2017, 6, OC17. [Google Scholar] [CrossRef]
- Locatelli, V.; Bianchi, V.E. Effect of GH/IGF-1 on Bone Metabolism and Osteoporsosis. Int. J. Endocrinol. 2014, 2014, 235060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pappa, H.; Thayu, M.; Sylvester, F.; Leonard, M.; Zemel, B.; Gordon, C. Skeletal health of children and adolescents with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 11–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, M.; Pacaud, D.; Petryk, A.; Collett-Solberg, P.F.; Kappy, M. Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Vitamin D deficiency in children and its management: Review of current knowledge and recommendations. Pediatrics 2008, 122, 398–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miele, E.; Shamir, R.; Aloi, M.; Assa, A.; Braegger, C.; Bronsky, J.; de Ridder, L.; Escher, J.C.; Hojsak, I.; Kolaček, S.; et al. Nutrition in Pediatric Inflammatory Bowel Disease: A Position Paper on Behalf of the Porto Inflammatory Bowel Disease Group of the European Society of Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 687–708. [Google Scholar] [CrossRef] [Green Version]
- Balachandar, R.; Fabbri, A. Relative Efficacy of Vitamin D2 and Vitamin D3 in Improving Vitamin D Status: Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3328. [Google Scholar] [CrossRef]
- Pappa, H.M.; Mitchell, P.D.; Jiang, H.; Kassiff, S.; Filip-Dhima, R.; Di Fabio, D.; Quinn, N.; Lawton, R.C.; Varvaris, M.; Van Straaten, S.; et al. Treatment of vitamin D insufficiency in children and adolescents with inflammatory bowel disease: A randomized clinical trial comparing three regimens. J. Clin. Endocrinol. Metab. 2012, 97, 2134–2142. [Google Scholar] [CrossRef] [Green Version]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 1289 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Peterson, C. Vitamin D deficiency and childhood obesity: Interactions, implications, and recommendations. Nutr. Diet. Suppl. 2015, 2015, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Fiamenghi, V.I.; de Mello, E.D. Vitamin D deficiency in children and adolescents with obesity: A meta-analysis. J. Pediatr. 2021, 97, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Zhu, L.; He, L.; Duan, Y.; Liang, W.; Nie, Z.; Jin, Y.; Wu, X.; Fang, Y. A meta-analysis of the relationship between vitamin D deficiency and obesity. Int. J. Clin. Exp. Med. 2015, 8, 14977–14984. [Google Scholar] [PubMed]
- Pereira-Santos, M.; Costa, P.R.F.; Assis, A.M.O.; Santos, C.A.S.T.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vranić, L.; Mikolašević, I.; Milić, S. Vitamin D Deficiency: Consequence or Cause of Obesity? Medicina 2019, 55, 541. [Google Scholar] [CrossRef] [Green Version]
- Vajro, P.; Lenta, S.; Socha, P.; Dhawan, A.; McKiernan, P.; Baumann, U.; Durmaz, O.; Lacaille, F.; McLin, V.; Nobili, V. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: Position paper of the ESPGHAN Hepatology Committee. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 700–713. [Google Scholar] [CrossRef]
- Targher, G.; Bertolini, L.; Scala, L.; Cigolini, M.; Zenari, L.; Falezza, G.; Arcaro, G. Associations between serum 25-hydroxyvitamin D3 concentrations and liver histology in patients with non-alcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 517–524. [Google Scholar] [CrossRef]
- Raychaudhuri, M.; Sanyal, D. Childhood obesity: Determinants, evaluation, and prevention. Indian J. Endocrinol. Metab. 2012, 16, S192–S194. [Google Scholar] [CrossRef]
- Walsh, J.S.; Bowles, S.; Evans, A.L. Vitamin D in obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 389–394. [Google Scholar] [CrossRef]
- Lee, P.; Greenfield, J.R.; Seibel, M.J.; Eisman, J.A.; Center, J.R. Adequacy of vitamin D replacement in severe deficiency is dependent on body mass index. Am. J. Med. 2009, 122, 1056–1060. [Google Scholar] [CrossRef]
- Theintz, G.; Buchs, B.; Rizzoli, R.; Slosman, D.; Clavien, H.; Sizonenko, P.C.; Bonjour, J.P. Longitudinal monitoring of bone mass accumulation in healthy adolescents: Evidence for a marked reduction after 16 years of age at the levels of lumbar spine and femoral neck in female subjects. J. Clin. Endocrinol. Metab. 1992, 75, 1060–1065. [Google Scholar] [PubMed]
- Dimitri, P. The Impact of Childhood Obesity on Skeletal Health and Development. J. Obes. Metab. Syndr. 2019, 28, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Ahn, J.; Kim, H.K.; Kim, J.H. Obese children experience more extremity fractures than nonobese children and are significantly more likely to die from traumatic injuries. Acta Paediatr. 2016, 105, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Kessler, J.; Koebnick, C.; Smith, N.; Adams, A. Childhood obesity is associated with increased risk of most lower extremity fractures. Clin. Orthop. Relat. Res. 2013, 471, 1199–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Orthopaedic Surgeons Position Statement. The Impact of Obesity on Bone and Joint Health. 2015. Available online: https://www.aaos.org/contentassets/1cd7f41417ec4dd4b5c4c48532183b96/1184-the-impact-of-obesity-on-bone-and-joint-health1.pdf (accessed on 16 May 2023).
- Montgomery, C.O.; Young, K.L.; Austen, M.; Jo, C.H.; Blasier, R.D.; Ilyas, M. Increased risk of Blount disease in obese children and adolescents with vitamin D deficiency. J. Pediatr. Orthop. 2010, 30, 879–882. [Google Scholar] [CrossRef]
- Rajakumar, K.; Fernstrom, J.D.; Holick, M.F.; Janosky, J.E.; Greenspan, S.L. Vitamin D status and response to Vitamin D(3) in obese vs. non-obese African American children. Obesity 2008, 16, 90–95. [Google Scholar] [CrossRef]
- Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellof, M.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Vitamin D in the healthy European paediatric population. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Isik, G.; Ustundag, B.; Dogan, Y. Vitamin D Insufficiency in Children with Chronic Neurological Diseases: Frequency and Causative Factors. Iran. J. Child. Neurol. 2023, 17, 31–38. [Google Scholar]
- Mughal, M.Z. Fractures in Children with Cerebral Palsy. Curr. Osteoporos. Rep. 2014, 12, 313–318. [Google Scholar] [CrossRef]
- Henderson, R.C.; Lark, R.K.; Gurka, M.J.; Worley, G.; Fung, E.B.; Conaway, M.; Stallings, V.A.; Stevenson, R.D. Bone density and metabolism in children and adolescents with moderate to severe cerebral palsy. Pediatrics 2002, 110, e5. [Google Scholar] [CrossRef] [Green Version]
- Yaşar, E.; Adigüzel, E.; Arslan, M.; Matthews, D.J. Basics of bone metabolism and osteoporosis in common pediatric neuromuscular disabilities. Eur. J. Paediatr. Neurol. 2018, 22, 17–26. [Google Scholar] [CrossRef] [PubMed]
- McNamara, N.A.; Romanowski, E.M.F.; Olson, D.P.; Shellhaas, R.A. Bone Health and Endocrine Comorbidities in Pediatric Epilepsy. Semin. Pediatr. Neurol. 2017, 24, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Romano, C.; van Wynckel, M.; Hulst, J.; Broekaert, I.; Bronsky, J.; Dall’Oglio, L.; Mis, N.F.; Hojsak, I.; Orel, R.; Papadopoulou, A.; et al. European Society for Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for the Evaluation and Treatment of Gastrointestinal and Nutritional Complications in Children with Neurological Impairment. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 242–264. [Google Scholar] [CrossRef] [Green Version]
- Ward, L.M.; Hadjiyannakis, S.; McMillan, H.J.; Noritz, G.; Weber, D.R. Bone Health and Osteoporosis Management of the Patient With Duchenne Muscular Dystrophy. Pediatrics 2018, 142, S34–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-Triviño, F.J.; Arias-Santiago, S.; Gilaberte-Calzada, Y. Vitamin D and the Skin: A Review for Dermatologists. Actas Dermosifiliogr. 2019, 110, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Kechichian, E.; Ezzedine, K. Vitamin D and the Skin: An Update for Dermatologists. Am. J. Clin. Dermatol. 2018, 19, 223–235. [Google Scholar] [CrossRef]
- Saalbach, A.; Kunz, M. Impact of Chronic Inflammation in Psoriasis on Bone Metabolism. Front. Immunol. 2022, 13, 925503. [Google Scholar] [CrossRef]
- Cubillos, S.; Norgauer, J. Low vitamin D-modulated calcium-regulating proteins in psoriasis vulgaris plaques: S100A7 overexpression depends on joint involvement. Int. J. Mol. Med. 2016, 38, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Compston, J. Glucocorticoid-induced osteoporosis: An update. Endocrine 2018, 61, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Blair, H.C.; Peng, Y.; Zaidi, N.; Adebanjo, O.A.; Wu, X.B.; Wu, X.Y.; Iqbal, J.; Epstein, S.; Abe, E.; et al. Calcineurin regulates bone formation by the osteoblast. Proc. Natl. Acad. Sci. USA 2005, 102, 17130–17135. [Google Scholar] [CrossRef] [Green Version]
- Uehara, R.; Suzuki, Y.; Ichikawa, Y. Methotrexate (MTX) inhibits osteoblastic differentiation in vitro: Possible mechanism of MTX osteopathy. J. Rheumatol. 2001, 28, 251–256. [Google Scholar] [PubMed]
- O’Regan, S.; Melhorn, D.K.; Newman, A.J. Methotrexate-induced bone pain in childhood leukemia. Am. J. Dis. Child. 1973, 126, 489–490. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Risk Group | Key Factors Responsible for Increased Risk of Vitamin D Deficiency | |
|---|---|---|
|  | Lack and/or insufficiency of UV-B exposure and/or penetration |
|  | Periods of increased physiologic demand |
| Reduced vitamin D synthesis | |
| Chronic illnesses | ||
| Decreased calcitriol synthesis | |
| Malabsorption, decreased calcitriol synthesis | |
| Malabsorption | |
|  | Poor UV-B exposure |
| Obesity | Reduced availability of vitamin D due to sequestration in fatty tissue | |
| Medications | ||
| Induces catabolism of vitamin D | |
| ||
|
| Age (Years) | Daily Supplementation (Oral D2/D3 IU) | Treatment of VDD 12 Weeks (Oral D2/D3 IU) | I.M. 1 Single Dose (D2 IU) |
|---|---|---|---|
| 0–1 | 2000 | 6000 | 50,000 |
| >1–10 | 3000–4000 | 6000–10,000 | 150,000 |
| 11–18 | 4000–6000 | 10,000–12,000 | 300,000 |
| Stage of CKD | GFR (Cr-cl) mL/min | FGF-23 | Calcium | Phosphate | Calcitriol | PTH |
|---|---|---|---|---|---|---|
| 1 | >90 | N | N | N | N | N |
| 2 | 60–89 | ↑ | N | N | ↓ | N/↑ |
| 3 | 30–59 | ↑↑ | N/↓ | N/↑ | ↓↓ | ↑ |
| 4 | 15–29 | ↑↑ | ↓ | ↑↑ | ↓↓ | ↑↑ |
| 5 | <15 | ↑↑ | ↓ | ↑↑ | ↓↓ | ↑↑↑ |
| Stage of VDD in CKD | Treatment (Daily Dose Regimen) D2/D3 | Treatment (Alternative Regimen) D2/D3 | Follow-Up Supplementation D2/D3 |
|---|---|---|---|
| Severe deficiency (<12 nmol/L or 5 ng/mL) | 8000 IU for 1 month, then 4000 IU for 2 months | 50,000 IU weekly for 1 month then 50,000 IU fortnightly for 2 months | After treatment- daily dose |
| Mild deficiency (12 to 50 nmol/L or 5–20 ng/mL) | 4000 IU for 3 months | 50,000 IU fortnightly for 3 months | 0–1 year 400 IU 1–18 years 600 IU |
| Insufficiency (50 to 75 nmol/L or 20–30 ng/mL) | 2000 IU for 3 months | 50,000 IU once a month for 3 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joshi, M.; Uday, S. Vitamin D Deficiency in Chronic Childhood Disorders: Importance of Screening and Prevention. Nutrients 2023, 15, 2805. https://doi.org/10.3390/nu15122805
Joshi M, Uday S. Vitamin D Deficiency in Chronic Childhood Disorders: Importance of Screening and Prevention. Nutrients. 2023; 15(12):2805. https://doi.org/10.3390/nu15122805
Chicago/Turabian StyleJoshi, Madhura, and Suma Uday. 2023. "Vitamin D Deficiency in Chronic Childhood Disorders: Importance of Screening and Prevention" Nutrients 15, no. 12: 2805. https://doi.org/10.3390/nu15122805
APA StyleJoshi, M., & Uday, S. (2023). Vitamin D Deficiency in Chronic Childhood Disorders: Importance of Screening and Prevention. Nutrients, 15(12), 2805. https://doi.org/10.3390/nu15122805