
Association between Dietary Inflammatory Index and Gastric Adenocarcinoma: A Multicenter Case-Control Study in Brazil
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
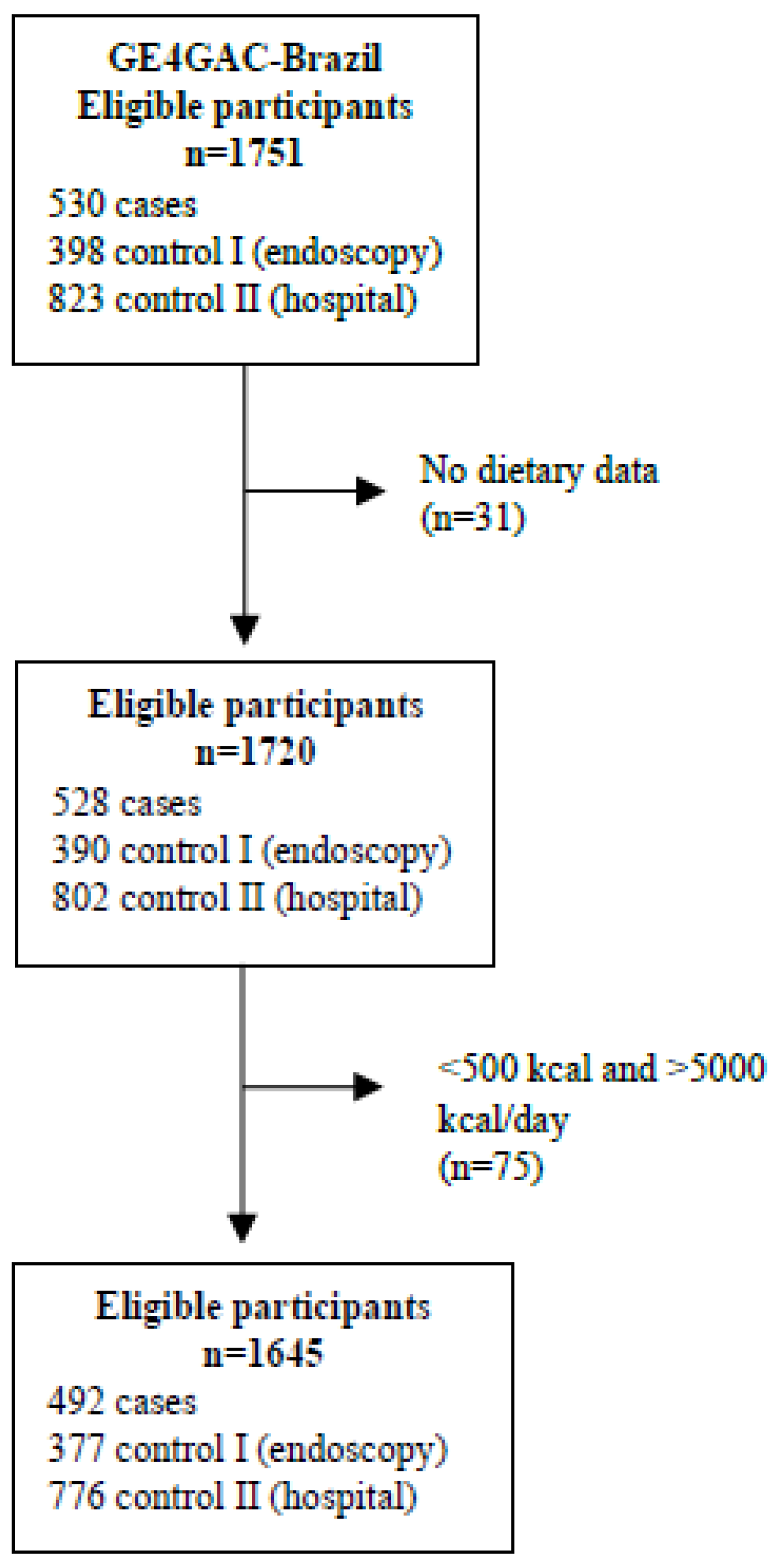
2.1. Study Population and Design
2.2. Data Collection
2.3. Dietary Assessment
2.4. Assessing Dietary Inflammatory Potential
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Brazilian National Cancer Institute Cancer Statistics in Brazil 2023–2025. Available online: https://www.gov.br/inca/pt-br/assuntos/cancer/numeros (accessed on 12 December 2022).
- Ilic, M.; Ilic, I. Epidemiology of Stomach Cancer. World J. Gastroenterol. 2022, 28, 1187–1203. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.P.; Wenker, T.N.; El-Serag, H.B. Global Burden of Gastric Cancer: Epidemiological Trends, Risk Factors, Screening and Prevention. Nat. Rev. Clin. Oncol. 2023, 20, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Piazuelo, M.B.; Carneiro, F.; Camargo, M.C. Considerations in Comparing Intestinal- and Diffuse-type Gastric Adenocarcinomas. Helicobacter 2023, 28, e12975. [Google Scholar] [CrossRef]
- Toh, J.W.T.; Wilson, R.B. Pathways of Gastric Carcinogenesis, Helicobacter Pylori Virulence and Interactions with Antioxidant Systems, Vitamin C and Phytochemicals. Int. J. Mol. Sci. 2020, 21, 6451. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and Developing a Literature-Derived, Population-Based Dietary Inflammatory Index. Public. Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Liang, Z.; Feng, Y.; Shivappa, N.; Hebert, J.R.; Xu, X. Dietary Inflammatory Index and Mortality from All Causes, Cardiovascular Disease, and Cancer: A Prospective Study. Cancers 2022, 14, 4609. [Google Scholar] [CrossRef]
- Marx, W.; Veronese, N.; Kelly, J.T.; Smith, L.; Hockey, M.; Collins, S.; Trakman, G.L.; Hoare, E.; Teasdale, S.B.; Wade, A.; et al. The Dietary Inflammatory Index and Human Health: An Umbrella Review of Meta-Analyses of Observational Studies. Adv. Nutr. 2021, 12, 1681–1690. [Google Scholar] [CrossRef]
- US Department of Agriculture. US Department of Health and Human Services Dietary Guidelines for Americans 2020–2025. Available online: https://www.dietaryguidelines.gov/resources/2020-2025-dietary-guidelines-online-materials (accessed on 19 February 2023).
- Lee, S.; Lee, J.; Choi, I.J.; Kim, Y.-W.; Ryu, K.W.; Kim, Y.-I.; Oh, J.-K.; Tran, B.T.; Kim, J. Dietary Inflammatory Index and the Risk of Gastric Cancer in a Korean Population. Oncotarget 2017, 8, 85452–85462. [Google Scholar] [CrossRef] [Green Version]
- Du, S.; Li, Y.; Su, Z.; Shi, X.; Johnson, N.L.; Li, P.; Zhang, Y.; Zhang, Q.; Wen, L.; Li, K.; et al. Index-Based Dietary Patterns in Relation to Gastric Cancer Risk: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2020, 123, 964–974. [Google Scholar] [CrossRef]
- Liang, Y.; Jiao, H.; Qu, L.; Liu, H. Positive Association between Dietary Inflammatory Index and Gastric Cancer Risk: A Systematic Review and Meta-Analysis. Nutr. Cancer 2020, 72, 1290–1296. [Google Scholar] [CrossRef]
- Lozano-Lorca, M.; Salcedo-Bellido, I.; Olmedo-Requena, R.; Castaño-Vinyals, G.; Amiano, P.; Shivappa, N.; Hébert, J.R.; Pérez-Gómez, B.; Gracia-Lavedan, E.; Gómez-Acebo, I.; et al. Dietary Inflammatory Index and Prostate Cancer Risk: MCC-Spain Study. Prostate Cancer Prostatic Dis. 2022, 25, 568–575. [Google Scholar] [CrossRef]
- Hayati, Z.; Montazeri, V.; Shivappa, N.; Hebert, J.R.; Pirouzpanah, S. The Association between the Inflammatory Potential of Diet and the Risk of Histopathological and Molecular Subtypes of Breast Cancer in Northwestern Iran: Results from the Breast Cancer Risk and Lifestyle Study. Cancer 2022, 128, 2298–2312. [Google Scholar] [CrossRef]
- Aminianfar, A.; Vahid, F.; Shayanfar, M.; Davoodi, S.H.; Mohammad-Shirazi, M.; Shivappa, N.; Sharifi, G.; Hebert, J.R.; Surkan, P.J.; Faghfoori, Z.; et al. The Association between the Dietary Inflammatory Index and Glioma: A Case-Control Study. Clin. Nutr. 2020, 39, 433–439. [Google Scholar] [CrossRef]
- Bartelli, T.F.; Senda de Abrantes, L.L.; Freitas, H.C.; Thomas, A.M.; Silva, J.M.; Albuquerque, G.E.; Araújo, L.F.; Branco, G.P.; de Amorim, M.G.; Serpa, M.S.; et al. Genomics and Epidemiology for Gastric Adenocarcinomas (GE4GAC): A Brazilian Initiative to Study Gastric Cancer. Appl. Cancer Res. 2019, 39, 12. [Google Scholar] [CrossRef] [Green Version]
- Boffetta, P.; Garfinkel, L. Alcohol Drinking and Mortality among Men Enrolled in an American Cancer Society Prospective Study. Epidemiology 1990, 1, 342–348. [Google Scholar] [CrossRef]
- Paragomi, P.; Dabo, B.; Pelucchi, C.; Bonzi, R.; Bako, A.T.; Sanusi, N.M.; Nguyen, Q.H.; Zhang, Z.-F.; Palli, D.; Ferraroni, M.; et al. The Association between Peptic Ulcer Disease and Gastric Cancer: Results from the Stomach Cancer Pooling (StoP) Project Consortium. Cancers 2022, 14, 4905. [Google Scholar] [CrossRef]
- Lolio, C.A.; Souza, J.M.P.; Santo, A.H.; Buchalla, C.M. Prevalence of Smoking in a City of Southeasthern Brazil. Rev. Saude Publica 1993, 27, 262–265. [Google Scholar] [CrossRef]
- Tseng, C.-H. The Relationship between Diabetes Mellitus and Gastric Cancer and the Potential Benefits of Metformin: An Extensive Review of the Literature. Biomolecules 2021, 11, 1022. [Google Scholar] [CrossRef]
- Bae, J.-M. Diabetes History and Gastric Cancer Risk: Different Results by Types of Follow-Up Studies. Asian Pac. J. Cancer Prev. 2022, 23, 1523–1528. [Google Scholar] [CrossRef]
- Huang, X.-Z.; Chen, Y.; Wu, J.; Zhang, X.; Wu, C.-C.; Zhang, C.-Y.; Sun, S.-S.; Chen, W.-J. Aspirin and Non-Steroidal Anti-Inflammatory Drugs Use Reduce Gastric Cancer Risk: A Dose-Response Meta-Analysis. Oncotarget 2017, 8, 4781–4795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poly, T.N.; Lin, M.-C.; Syed-Abdul, S.; Huang, C.-W.; Yang, H.-C.; Li, Y.-C. Proton Pump Inhibitor Use and Risk of Gastric Cancer: Current Evidence from Epidemiological Studies and Critical Appraisal. Cancers 2022, 14, 3052. [Google Scholar] [CrossRef] [PubMed]
- Segna, D.; Brusselaers, N.; Glaus, D.; Krupka, N.; Misselwitz, B. Association between Proton-Pump Inhibitors and the Risk of Gastric Cancer: A Systematic Review with Meta-Analysis. Therap Adv. Gastroenterol. 2021, 14, 175628482110514. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Pan American Health Organization. Multicenter Survey Aging, Health and Wellbeing in Latin America and the Caribbean (SABE): Preliminary Report. In Proceedings of the XXXVI Reunion del Comite Asesor de Investigaciones en Salud, Washington, DC, USA, 9–11 June 2001; OPAS: Kingston, Jamaica, 2001; p. 19. [Google Scholar]
- Laurén, P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and so-Called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Lameza, M.M.S. Validation of the Food Frequency Questionnaire for Previously Treated Colorectal Cancer Patients. Dissertação de Mestrado, Fundação Antônio Prudente, São Paulo, Brazil, 2010. [Google Scholar]
- Peres, S.V.; Silva, D.R.M.; Coimbra, F.J.F.; Fagundes, M.A.; Auzier, J.J.N.; Pelosof, A.G.; Araujo, M.S.; Assumpção, P.P.; Curado, M.P. Consumption of Processed and Ultra-Processed Foods by Patients with Stomach Adenocarcinoma: A Multicentric Case–Control Study in the Amazon and Southeast Regions of Brazil. Cancer Causes Control. 2022, 33, 889–898. [Google Scholar] [CrossRef]
- University of São Paulo; Food Research Center. Brazilian Food Composition Table (TBCA) Version 7.2. Available online: http://www.fcf.usp.br/tbca (accessed on 2 January 2023).
- Harmon, B.E.; Wirth, M.D.; Boushey, C.J.; Wilkens, L.R.; Draluck, E.; Shivappa, N.; Steck, S.E.; Hofseth, L.; Haiman, C.A.; Le Marchand, L.; et al. The Dietary Inflammatory Index Is Associated with Colorectal Cancer Risk in the Multiethnic Cohort. J. Nutr. 2017, 147, 430–438. [Google Scholar] [CrossRef] [Green Version]
- Hébert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII)—Lessons Learned, Improvements Made, and Future Directions. Adv. Nutr. 2019, 10, 185–195. [Google Scholar] [CrossRef]
- Shivappa, N.; Hébert, J.R.; Ferraroni, M.; La Vecchia, C.; Rossi, M. Association between Dietary Inflammatory Index and Gastric Cancer Risk in an Italian Case-Control Study. Nutr. Cancer 2016, 68, 1262–1268. [Google Scholar] [CrossRef] [Green Version]
- Vahid, F.; Shivappa, N.; Faghfoori, Z.; Khodabakhshi, A.; Zayeri, F.; Hebert, J.R.; Davoodi, S.H. Validation of a Dietary Inflammatory Index (DII) and Association with Risk of Gastric Cancer: A Case-Control Study. Asian Pac. J. Cancer Prev. 2018, 19, 1471–1477. [Google Scholar] [CrossRef]
- Bodén, S.; Myte, R.; Wennberg, M.; Harlid, S.; Johansson, I.; Shivappa, N.; Hébert, J.R.; Van Guelpen, B.; Nilsson, L.M. The Inflammatory Potential of Diet in Determining Cancer Risk; A Prospective Investigation of Two Dietary Pattern Scores. PLoS ONE 2019, 14, e0214551. [Google Scholar] [CrossRef]
- Acuna, N.; Park, S.-Y.; Le Marchand, L.; Hébert, J.R.; Boushey, C.; Wilkens, L.R.; Wu, A.H.; Setiawan, V.W. Diet Quality and Risk of Gastric Adenocarcinoma: The Multiethnic Cohort. Am. J. Clin. Nutr. 2023, 117, 46–54. [Google Scholar] [CrossRef]
- Vitelli-Storelli, F.; Rubín-García, M.; Pelucchi, C.; Benavente, Y.; Bonzi, R.; Rota, M.; Palli, D.; Ferraroni, M.; Lunet, N.; Morais, S.; et al. Family History and Gastric Cancer Risk: A Pooled Investigation in the Stomach Cancer Pooling (STOP) Project Consortium. Cancers 2021, 13, 3844. [Google Scholar] [CrossRef]
- Assumpção, P.P.; Barra, W.F.; Ishak, G.; Coelho, L.G.V.; Coimbra, F.J.F.; Freitas, H.C.; Dias-Neto, E.; Camargo, M.C.; Szklo, M. The Diffuse-Type Gastric Cancer Epidemiology Enigma. BMC Gastroenterol. 2020, 20, 223. [Google Scholar] [CrossRef]
- Huang, R.J.; Laszkowska, M.; In, H.; Hwang, J.H.; Epplein, M. Controlling Gastric Cancer in a World of Heterogeneous Risk. Gastroenterology 2023, 164, 736–751. [Google Scholar] [CrossRef]
- Curado, M.P.; de Oliveira, M.M.; de Araújo Fagundes, M. Prevalence of Helicobacter Pylori Infection in Latin America and the Caribbean Populations: A Systematic Review and Meta-Analysis. Cancer Epidemiol. 2019, 60, 141–148. [Google Scholar] [CrossRef]
- Correa, P.; Piazuelo, M.B. The Gastric Precancerous Cascade. J. Dig. Dis. 2012, 13, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Hui, Y.; Tu, C.; Liu, D.; Zhang, H.; Gong, X. Risk Factors for Gastric Cancer: A Comprehensive Analysis of Observational Studies. Front. Public. Health 2023, 10, 892468. [Google Scholar] [CrossRef]
- Dalmartello, M.; Turati, F.; Zhang, Z.F.; Lunet, N.; Rota, M.; Bonzi, R.; Galeone, C.; Martimianaki, G.; Palli, D.; Ferraroni, M.; et al. Allium Vegetables Intake and the Risk of Gastric Cancer in the Stomach Cancer Pooling (StoP) Project. Br. J. Cancer 2022, 126, 1755–1764. [Google Scholar] [CrossRef]
- Su, X.-Q.; Yin, Z.-Y.; Jin, Q.-Y.; Liu, Z.-C.; Han, X.; Hu, Z.-Q.; Zhang, L.; Ma, J.-L.; Li, Z.-X.; Zhang, Y.; et al. Allium Vegetable Intake Associated with the Risk of Incident Gastric Cancer: A Continuous Follow-up Study of a Randomized Intervention Trial. Am. J. Clin. Nutr. 2023, 117, 22–32. [Google Scholar] [CrossRef]
- Li, W.-Q.; Zhang, J.-Y.; Ma, J.-L.; Li, Z.-X.; Zhang, L.; Zhang, Y.; Guo, Y.; Zhou, T.; Li, J.-Y.; Shen, L.; et al. Effects of Helicobacter Pylori Treatment and Vitamin and Garlic Supplementation on Gastric Cancer Incidence and Mortality: Follow-up of a Randomized Intervention Trial. BMJ 2019, 366, l5016. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, J.C.; Wang, Q.; Lin, P.-H.; Shrubsole, M.J.; Epplein, M. Supplement Use and Gastric Cancer Risk in the Southern Community Cohort Study. Cancer Causes Control 2023. [Google Scholar] [CrossRef]
- Guo, Y.; Li, Z.-X.; Zhang, J.-Y.; Ma, J.-L.; Zhang, L.; Zhang, Y.; Zhou, T.; Liu, W.-D.; Han, Z.-X.; Li, W.-Q.; et al. Association Between Lifestyle Factors, Vitamin and Garlic Supplementation, and Gastric Cancer Outcomes. JAMA Netw. Open 2020, 3, e206628. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Cook, N.R.; Albert, C.; Zaharris, E.; Gaziano, J.M.; Van Denburgh, M.; Buring, J.E.; Manson, J.E. Vitamins C and E and Beta Carotene Supplementation and Cancer Risk: A Randomized Controlled Trial. JNCI J. Natl. Cancer Inst. 2009, 101, 14–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damiani, T.F.; Pereira, L.P.; Ferreira, M.G. Consumption of Fruit, Greens and Vegetables in the Midwest Region of Brazil: Prevalence and Associated Factors. Cien Saude Colet. 2017, 22, 369–382. [Google Scholar] [CrossRef] [Green Version]
- Nardoto, G.B.; da Silva, R.J.; Schor, T.; Garavello, M.E.P.E.; Silva, M.R.F.; Rodrigues, L.P.F.; Murrieta, R.S.S.; Camilo, E.A.; Reinaldo, E.D.F.; Aquino, F.C.; et al. Mapping Carbon and Nitrogen Isotopic Composition of Fingernails to Demonstrate a Rural–Urban Nutrition Transition in the Center-West, Northeast, and Amazon Regions of Brazil. Am. J. Phys. Anthropol. 2020, 172, 650–663. [Google Scholar] [CrossRef]
- Noblat, A.K.M.; Melo, E.M.S.; Silva, W.A.; Silvério, M.L.; Correia, J.M. Impact of Pesticides on Food: A Literature Review. Res. Soc. Dev. 2021, 10, e36110614504. [Google Scholar] [CrossRef]
- Levy, R.B.; Andrade, G.C.; Cruz, G.L.; Rauber, F.; Louzada, M.L.C.; Claro, R.M.; Monteiro, C.A. Três Décadas Da Disponibilidade Domiciliar de Alimentos Segundo a NOVA—Brasil, 1987–2018. Rev. Saude Publica 2022, 56, 75. [Google Scholar] [CrossRef]
- Costa, C.S.; Sattamini, I.F.; Steele, E.M.; Louzada, M.L.C.; Claro, R.M.; Monteiro, C.A. Consumo de Alimentos Ultraprocessados e Associação Com Fatores Sociodemográficos Na População Adulta Das 27 Capitais Brasileiras (2019). Rev. Saude Publica 2021, 55, 47. [Google Scholar] [CrossRef]
- Mignogna, C.; Costanzo, S.; Di Castelnuovo, A.; Ruggiero, E.; Shivappa, N.; Hebert, J.R.; Esposito, S.; De Curtis, A.; Persichillo, M.; Cerletti, C.; et al. The Inflammatory Potential of the Diet as a Link between Food Processing and Low-Grade Inflammation: An Analysis on 21,315 Participants to the Moli-Sani Study. Clin. Nutr. 2022, 41, 2226–2234. [Google Scholar] [CrossRef]
- Lin, X.-J.; Wang, C.-P.; Liu, X.-D.; Yan, K.-K.; Li, S.; Bao, H.-H.; Zhao, L.-Y.; Liu, X. Body Mass Index and Risk of Gastric Cancer: A Meta-Analysis. Jpn. J. Clin. Oncol. 2014, 44, 783–791. [Google Scholar] [CrossRef] [Green Version]
- Pan American Health Organization. Updated PAHO Regional Sodium Reduction Targets. Available online: https://iris.paho.org/handle/10665.2/54971 (accessed on 3 February 2023).
- Jachimowicz-Rogowska, K.; Winiarska-Mieczan, A. Initiatives to Reduce the Content of Sodium in Food Products and Meals and Improve the Population’s Health. Nutrients 2023, 15, 2393. [Google Scholar] [CrossRef]


{kind=link}
| Variables | GE4GAC-Brazil (n = 1645) | p-Value 1 | ||
|---|---|---|---|---|
| Cases (n = 492) | Control I (n = 377) | Control II (n = 776) | ||
| Median (P25, P75) or n (%) | ||||
| Sex | 0.002 | |||
| Female | 199 (40.4) | 182 (48.3) | 398 (51.3) | |
| Male | 293 (59.6) | 195 (51.7) | 378 (48.7) | |
| Age (years) | 58 (49, 65) a | 57 (44, 64) b | 55 (44, 64) b | 0.001 |
| Self-reported ethnicity | ||||
| White | 181 (36.8) | 180 (47.7) | 287 (37.0) | <0.001 |
| Brown | 249 (50.6) | 134 (35.5) | 320 (41.3) | |
| Black | 44 (8.9) | 43 (11.4) | 110 (14.2) | |
| Others | 18 (3.7) | 20 (5.3) | 58 (7.5) | |
| Schooling (years) † | <0.001 | |||
| ≤8 | 232 (47.2) | 96 (25.5) | 172 (22.2) | |
| 9–12 | 159 (32.3) | 163 (43.2) | 412 (53.1) | |
| ≥13 | 101 (20.5) | 118 (31.3) | 192 (24.7) | |
| Marital status | 0.13 | |||
| Married | 353 (71.7) | 247 (65.5) | 523 (67.4) | |
| Single | 71 (14.4) | 66 (17.5) | 147 (18.9) | |
| Others | 68 (13.8) | 64 (17.0) | 106 (13.7) | |
| Family history of cancer in first-degree relatives | <0.001 | |||
| No | 188 (38.4) | 159 (42.3) | 391 (50.5) | |
| Yes | 302 (61.6) | 217 (57.7) | 383 (49.5) | |
| Tobacco smoking § | <0.001 | |||
| No | 198 (40.5) | 227 (60.5) | 495 (64.1) | |
| Low | 80 (16.4) | 67 (17.9) | 106 (13.7) | |
| Intermediate/High | 211 (43.1) | 81 (21.6) | 171 (22.2) | |
| Alcohol consumption ¥ | <0.001 | |||
| No | 230 (47.2) | 180 (48.5) | 508 (66.7) | |
| Low | 75 (15.4) | 55 (14.8) | 64 (8.4) | |
| Intermediate/High | 182 (37.4) | 136 (36.7) | 190 (24.9) | |
| Diabetes | 0.003 | |||
| No | 447 (90.9) | 327 (86.7) | 721 (92.9) | |
| Yes | 45 (9.1) | 50 (13.3) | 55 (7.1) | |
| Peptic ulcer | 0.04 | |||
| No | 451 (91.7) | 359 (95.2) | - | |
| Yes | 41 (8.3) | 18 (4.3) | - | |
| H. pylori status * | 0.04 | |||
| Negative | 230 (77.4) | 226 (70.0) | - | |
| Positive | 67 (22.6) | 97 (30.0) | - | |
| PPIs/H2RAs | <0.001 | |||
| No | 265 (54.2) | 215 (57.2) | 681 (88.0) | |
| Yes | 224 (45.8) | 161 (42.8) | 93 (12.0) | |
| Antacids | <0.001 | |||
| No | 418 (85.1) | 329 (87.5) | 755 (97.4) | |
| Yes | 73 (14.9) | 47 (12.5) | 20 (2.6) | |
| Aspirin | 0.33 | |||
| No | 462 (94.1) | 351 (93.4) | 739 (95.4) | |
| Yes | 29 (5.9) | 25 (6.6) | 36 (4.6) | |
| Other NSAIDs | <0.001 | |||
| No | 435 (88.6) | 331 (88.0) | 736 (95.0) | |
| Yes | 56 (11.4) | 45 (12.0) | 39 (5.0) | |
| BMI (categories) | <0.001 | |||
| Normal weight | 208 (42.3) | 148 (39.4) | 322 (41.5) | |
| Underweight/Malnutrition | 138 (28.0) | 24 (6.4) | 88 (11.4) | |
| Overweight | 78 (15.9) | 118 (31.4) | 222 (28.6) | |
| Obesity | 68 (13.8) | 86 (22.9) | 143 (18.5) | |
| Energy intake (kcal/day) | 2193 (1664, 2824) a | 2087 (1503, 2653) a | 1792 (1352, 2391) b | <0.001 |
| Sodium intake (g/day) | 2.2 (1.7, 5.5) a | 1.7 (1.5, 2.0) c | 1.8 (1.5, 2.5) b | <0.001 |
| Nutritional supplement | 0.07 | |||
| No | 408 (83.1) | 308 (81.7) | 671 (86.5) | |
| Yes | 83 (16.9) | 69 (18.3) | 105 (13.5) | |
| Anatomical location | - | |||
| Cardia | 101 (22.3) | - | - | |
| Non-cardia | 352 (77.7) | - | - | |
| Histological subtype | - | |||
| Diffuse | 203 (50.1) | - | - | |
| Intestinal | 174 (43.0) | - | - | |
| Mixed | 28 (6.9) | - | - | |
| E-DII score | −0.45 (−1.46, 0.53) b | −0.73 (−2.00, 0.56) a | −0.83 (−2.03, 0.25) a | <0.001 |
| Components | Cases (n = 492) | Control I (n = 377) | Control II (n = 776) | p-Value 1 | E-DII Quartiles § | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control I | Control II | |||||||||||||
| Q1 n = 94 (−5.55, −2.01) | Q2 n = 94 (−2.00, −0.74) | Q3 n = 95 (−0.73, 0.56) | Q4 n = 94 (>0.56) | p-Value 1 ‡ | Q1 n = 194 (−5.09, −2.04) | Q2 n = 194 (−2.03, −0.83) | Q3 n = 194 (−0.82, 0.25) | Q4 n = 194 (>0.25) | p-Value 1 ‡ | |||||
| Median (P25, P75) | Median (P25, P75) | Median (P25, P75) | ||||||||||||
| Pro-inflammatory | ||||||||||||||
| Carbohydrates (g/day) | 119.7 (104.8, 133.4) | 122.1 (107.8, 136.5) | 121.5 (106.5, 136.4) | 0.23 | 131.8 (118.4, 147.3) bc | 122.8, 113.6, 135.7) e | 118.2 (105.8, 134.0) | 112.7 (97.0, 126.1) | <0.001 | 130.4 (115.6, 147.2) bc | 126.0 (112.7, 141.1) de | 115.5 (101.7, 130.0) | 111.7 (96.0, 125.4) | <0.001 |
| Proteins (g/day) | 43.7 (38.9, 49.5) a | 41.5 (37.5, 47.1) b | 43.0 (37.5, 48.7) a | <0.001 | 40.7 (36.3, 45.5) | 42.0 (36.2, 46.8) | 40.2 (36.7, 46.6) | 43.0 (36.4, 49.5) | 0.45 | 42.6 (36.7, 43.4) bc | 41.7 (36.1, 46.9) de | 44.0 (39.1, 51.1) | 44.1 (38.1, 51.1) | <0.001 |
| Total fats (g/day) | 39.9 (35.1, 44.4) | 40.4 (35.4, 44.8) | 39.8 (34.7, 44.5) | 0.54 | 36.9 (32.6, 43.5) c | 39.4 (35.3, 43.2) e | 41.4 (36.7, 45.0) | 42.7 (39.3, 46.8) | <0.001 | 38.5 (33.4, 43.3) c | 38.6 (33.6, 43.0) e | 40.6 (35.3, 44.8) | 41.5 (38.0, 46.3) | <0.001 |
| SFAs (g/day) | 12.7 (11.0, 14.2) a | 12.2 (10.3, 14.3) ab | 12.2 (10.5, 14.2) bc | 0.03 | 10.8 (9.0, 12.6) bc | 11.6 (9.9, 13.4) e | 12.6 (10.8, 14.3) f | 14.3 (12.5, 15.3) | <0.001 | 10.9 (9.7, 12.7) bc | 11.7 (10.1, 13.5) de | 12.7 (10.9, 14.4) f | 13.8 (11.7, 15.3) | <0.001 |
| TFAs (g/day) | 0.9 (0.7, 1.1) ab | 0.9 (0.7, 1.2) ab | 0.8 (0.6, 1.1) c | 0.001 | 0.6 (0.5, 0.9) bc | 0.9 (0.6, 1.1) e | 1.0 (0.8, 1.2) f | 1.2 (0.9, 1.4) | <0.001 | 0.7 (0.5, 0.9) bc | 0.8 (0.6, 0.9) de | 0.9 (0.7, 1.1) | 1.0 (0.8, 1.2) | <0.001 |
| Cholesterol (mg/day) | 153.2 (119.6, 196.8) a | 131.1 (102.0, 166.0) c | 144.5 (110.2, 187.0) b | <0.001 | 115.4 (96.0, 163.5) c | 128.2 (96.4, 155.5) | 135.6 (108.4, 161.0) | 143.6 (118.0, 178.3) | 0.01 | 128.6 (99.0, 175.0) bc | 130.6 (102.2, 170.7) de | 152.6 (115.6, 198.0) | 159.2 (125.0, 199.7) | <0.001 |
| Iron (mg/day) | 6.2 (5.6, 7.0) b | 6.5 (5.7, 7.4) a | 6.4 (5.6, 7.2) ab | 0.03 | 6.5 (5.8, 7.3) | 6.7 (5.8, 7.5) e | 6.9 (6.0, 7.6) f | 6.1 (5.6, 6.7) | 0.001 | 7.0 (5.9, 7.8) abc | 6.4 (5.6, 7.3) e | 6.3 (5.6, 6.9) | 6.0 (5.3, 6.7) | <0.001 |
| Vitamin B12 (mg/day) | 1.9 (1.5, 2.3) a | 1.7 (1.3, 2.0) c | 1.8 (1.4, 2.3) b | <0.001 | 1.5 (1.2, 1.9) c | 1.7 (1.2, 1.9) e | 1.7 (1.4, 2.1) | 1.8 (1.5, 2.4) | <0.001 | 1.6 (1.2, 2.0) bc | 1.7 (1.3, 2.1) de | 1.8 (1.5, 2.3) | 2.0 (1.6, 2.5) | <0.001 |
| Anti-inflammatory | ||||||||||||||
| Omega-3 (g/day) | 1.2 (1.1, 1.5) | 1.2 (1.0, 1.5) | 1.3 (1.1, 1.5) | 0.14 | 1.4 (1.1, 1.6) bc | 1.2 (1.1, 1.4) | 1.2 (1.0, 1.4) f | 1.1 (0.9, 1.3) | <0.001 | 1.3 (1.1, 1.6) bc | 1.2 (1.1, 1.5) | 1.2 (1.0, 1.4) | 1.2 (1.0, 1.4) | 0.001 |
| Omega-6 (g/day) | 7.8 (6.6, 9.1) b | 8.1 (7.0, 9.5) a | 8.0 (6.8, 9.5) b | 0.01 | 8.2 (7.0, 9.5) | 8.2 (7.0, 9.3) | 8.1 (7.1, 9.4) | 8.0 (6.4, 9.6) | 0.76 | 8.4 (6.9, 9.9) | 8.0 (6.8, 9.6) | 8.0 (6.7, 9.3) | 7.8 (6.5, 9.1) | 0.076 |
| MUFAs (g/day) | 13.4 (11.6, 15.1) | 13.7 (11.6, 15.8) | 13.5 (11.4, 15.4) | 0.21 | 12.7 (10.7, 16.2) c | 13.3 (11.4, 15.0) e | 13.7 (11.7, 15.4) | 14.6 (13.1, 16.4) | 0.003 | 13.4 (11.2, 15.3) | 13.1 (11.0, 14.8) e | 13.6 (11.5, 15.4) | 14.3 (12.2, 15.8) | 0.008 |
| Vitamin A (RE/day) | 258.1 (195.7, 348.5) c | 322.4 (234.1, 432.1) a | 280.1 (209.8, 387.0) b | <0.001 | 374.4 (272.3, 577.3) c | 336.3 (231.1, 502.7) e | 327.2 (258.3, 418.0) f | 245.1 (190.6, 348.6) | <0.001 | 384.7 (294.9, 560.7) abc | 284.0 (211.7, 373.1) de | 246.0 (186.0, 340.2) | 238.2 (180.1, 318.6) | <0.001 |
| β-carotene (µg/day) | 982.7 (610.2, 1476.3) b | 1257.6 (809.7, 1833.0) a | 1144.3 (700.5, 1786.6) a | <0.001 | 2005.6 (1581, 2820.0) abc | 1437.2 (1011.3, 1931.0) de | 1082.5 (817.7, 1454.1) f | 714.8 (489.0, 1038.6) | <0.001 | 2205.6 (1578.3, 3041.6) abc | 1245.8 (862.7, 1646.5) de | 922.0 (567.6, 1251.1) | 745.4 (544.3, 1093.6) | <0.001 |
| Vitamin B1 (mg/day) | 0.7 (0.6, 0.8) b | 0.8 (0.7, 0.9) a | 0.7 (0.6, 0.8) ab | 0.003 | 0.8 (0.7, 0.9) bc | 0.8 (0.7, 0.9) e | 0.8 (0.7, 0.8) f | 0.7 (0.6, 0.8) | <0.001 | 0.8 (0.7, 0.9) abc | 0.8 (0.7, 0.9) de | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.8) | <0.001 |
| Vitamin B2 (mg/day) | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.8) | 0.38 | 0.8 (0.7, 0.9) bc | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.8) | <0.001 | 0.8 (0.7, 0.9) abc | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.8) | 0.7 (0.6, 0.8) | <0.001 |
| Niacin (mg/day) | 10.0 (8.6, 11.4) | 9.8 (8.3, 11.2) | 9.8 (8.4, 11.4) | 0.13 | 9.6 (8.2, 11.2) | 9.8 (8.3, 11.4) | 9.3 (8.3, 11.1) | 10.0 (8.6, 11.7) | 0.39 | 9.5 (7.9, 10.6) bc | 9.4 (7.9, 10.6) de | 10.4 (9.1, 12.1) | 10.3 (8.5, 11.9) | <0.001 |
| Vitamin B6 (mg/day) | 1.0 (0.9, 1.2) a | 1.0 (0.8, 1.2) b | 1.0 (0.9, 1.2) a | 0.002 | 1.1 (1.0, 1.3) abc | 1.0 (0.9, 1.1) | 0.9 (0.8, 1.1) | 0.9 (0.7, 1.0) | <0.001 | 1.1 (1.0, 1.2) abc | 1.0 (0.9, 1.2) | 1.0 (0.9, 1.2) | 1.0 (0.9, 1.1) | <0.001 |
| PUFAs (g/day) | 9.3 (8.2, 11.0) | 9.8 (8.3, 11.4) | 9.7 (8.2, 11.3) | 0.06 | 9.8 (8.3, 11.5) | 9.8 (8.4, 11.2) | 9.8 (8.4, 11.1) | 9.6 (7.9, 11.2) | 0.67 | 10.2 (8.4, 11.9) | 9.7 (8.3, 11.5) | 9.6 (8.1, 11.0) | 9.5 (8.1, 10.8) | 0.090 |
| Folic acid (µg/day) | 214.5 (184.8, 256.3) c | 235.7 (202.0, 274.5) a | 227.0 (190.5, 266.2) b | <0.001 | 267.5 (224.8, 306.7) bc | 247.5 (219.0, 285.7) e | 236.7 (209.7, 267.3) f | 196.0 (172.7, 223.8) | <0.001 | 256.2 (229.1, 302.5) abc | 239.8 (208.6, 279.2) de | 216.3 (186.1, 249.0) f | 193.8 (169.8, 224.8) | <0.001 |
| Vitamin C (mg/day) | 57.3 (33.6, 83.5) | 54.8 (34.0, 94.4) | 59.0 (36.7, 93.1) | 0.11 | 111.1 (87.8, 150.0) abc | 69.0 (51.3, 95.7) de | 45.6 (30.7. 58.5) f | 32.1 (23.2, 42.2) | <0.001 | 106.5 (74.4, 145.3) abc | 70.7 (49.6, 99.9) de | 46.4 (31.5, 62.8) | 38.2 (25.7, 53.4) | <0.001 |
| Vitamin D (µg/day) | 3.0 (2.0, 4.3) a | 2.0 (1.4, 2.9) c | 2.6 (1.7, 3.8) b | <0.001 | 2.6 (1.8, 3.3) bc | 2.1 (1.4, 3.0) | 1.8 (1.3, 2.7) | 1.8 (1.4, 2.3) | <0.001 | 2.8 (1.8, 3.8) | 2.4 (1.6, 3.4) | 2.6 (1.5, 3.7) | 2.6 (1.8, 4.2) | 0.092 |
| Vitamin E (mg/day) | 3.2 (2.8, 3.7) b | 3.6 (3.1, 4.3) a | 3.5 (2.9, 4.2) a | <0.001 | 4.6 (4.0, 5.2) abc | 3.6 (3.3, 4.3) de | 3.3 (3.0, 3.7) f | 3.0 (2.6, 3.5) | <0.001 | 4.3 (3.9, 5.0) abc | 3.6 (3.1, 4.3) de | 3.1 (2.8, 3.6) | 3.0 (2.6, 3.4) | <0.001 |
| Fibers (g/day) | 10.5 (8.3, 13.3) b | 11.8 (9.4, 14.8) a | 11.4 (8.6, 14.5) a | <0.001 | 16.0 (14.2, 19.1) abc | 13.1 (11.5, 15.2) de | 10.8 (9.5, 12.7) f | 8.3 (7.1, 9.7) | <0.001 | 16.1 (13.3, 20.3) abc | 12.8 (10.9, 15.0) de | 10.1 (8.2, 11.6) f | 8.2 (7.0, 10.0) | <0.001 |
| Magnesium (g/day) | 133.7 (119.8, 156.6) c | 139.5 (121.0, 163.3) abc | 141.0 (122.4, 165.5) ab | 0.01 | 175.8 (157.0, 200.2) abc | 146.4 (133.2, 163.3) de | 131.5 (122.8, 143.3) f | 114.4 (102.7, 123.3) | <0.001 | 175.7 (152.9, 218.4) abc | 152.8 (133.1, 167.2) de | 129.8 (118.1, 141.8) | 121.0 (109.6, 134.2) | <0.001 |
| Selenium (g/day) | 62.1 (54.2, 75.0) a | 58.8 (51.4, 71.2) c | 61.8 (52.8, 75.2) ab | 0.003 | 59.0 (50.8, 75.4) | 58.4 (51.5, 68.0) | 58.3 (52.4, 72.4) | 60.3 (51.3, 70.2) | 0.79 | 66.2 (54.1, 78.9) c | 59.8 (50.5, 73.0) | 62.6 (53.7, 72.7) | 61.1 (53.1, 71.1) | 0.018 |
| Zinc (mg/day) | 6.5 (5.7, 7.4) a | 6.3 (5.4, 7.2) ab | 6.3 (5.5, 7.2) b | 0.03 | 6.0 (5.3, 6.9) | 6.5 (5.4, 7.3) | 6.5 (5.8, 7.2) | 6.4 (5.7, 7.5) | 0.13 | 6.2 (5.3, 6.8) bc | 6.1 (5.3, 7.3) e | 6.5 (5.8, 7.4) | 6.6 (5.7, 7.4) | 0.001 |
| Caffeine (mg/day) | 0.6 (0.1, 2.7) b | 2.0 (0.4, 23.0) a | 0.6 (0.9, 3.3) b | <0.001 | 0.4 (0.0, 1.6) abc | 1.5 (0.2, 22.8) e | 7.8 (0.8, 28.0) | 14.5 (1.4, 31.0) | <0.001 | 0.5 (0.5, 1.7) | 0.7 (0.2, 2.9) | 0.6 (0.1, 4.9) | 0.8 (0.0, 5.3) | 0.470 |
| Onion (g/day) | 2.5 (0.0, 6.1) c | 3.9 (1.6, 8.4) a | 3.5 (0.6, 6.5) b | <0.001 | 5.7 (2.1, 12.0) c | 4.5 (1.2, 9.3) | 4.0 (1.8, 8.4) | 2.9 (1.2, 5.1) | 0.001 | 5.1 (2.1, 9.4) bc | 4.0 (1.8, 6.4) de | 2.7 (0.0, 5.6) | 2.2 (0.0, 5.0) | <0.001 |
| Pepper (g/day) | 0.0 (0.0, 0.8) | 0.0 (0.0, 0.4) | 0.0 (0.0, 0.7) | 0.21 | 0.0 (0.0, 0.0) | 0.0 (0.0, 0.5) | 0.0 (0.0, 0.8) | 0.0 (0.0, 0.5) | 0.15 | 0.0 (0.0, 0.6) | 0.0 (0.0, 0.2) d | 0.0 (0.0, 0.8) | 0.0 (0.0, 0.9) | 0.016 |
| E−DII Quartiles | p−Trend ‡ | |||||
|---|---|---|---|---|---|---|
| Q1 (−5.55, −2.01) | Q2 (−2.00, −0.74) | Q3 (−0.73, 0.56) | Q4 (>0.56) | Per 1-Point Increment in the E-DII Score | ||
| OR | OR (95% CI) | OR (95% CI) | OR (95% CI) | |||
| All 1 | ||||||
| Cases/Controls | 68/94 | 134/94 | 169/95 | 121/94 | 492/377 | |
| Crude | 1.00 | 1.97 (1.31–2.96) | 2.46 (1.65–3.67) | 1.78 (1.18–2.68) | 1.15 (1.05–1.26) | 0.003 |
| Model 1 | 1.00 | 1.62 (0.97–2.70) | 1.94 (1.14–3.30) | 1.70 (0.88–3.27) | 1.17 (1.02–1.35) | 0.02 |
| Model 2 a | 1.00 | 1.51 (0.81–2.81) | 2.10 (1.06–3.98) | 2.60 (1.16–5.70) | 1.24 (1.05–1.46) | 0.01 |
| Anatomical location 2 | ||||||
| Cardia | ||||||
| Cases/Controls | 13/94 | 32/94 | 30/95 | 26/94 | 101/377 | |
| Crude | 1.00 | 2.46 (1.22–4.98) | 2.28 (1.12–4.65) | 2.00 (0.96–4.13) | 1.19 (1.03–1.38) | 0.02 |
| Model 1 | 1.00 | 1.90 (0.85–4.20) | 2.02 (0.87–4.64) | 1.81 (0.69–4.73) | 1.26 (1.03–1.54) | 0.03 |
| Model 2 | 1.00 | 1.22 (0.50–2.97) | 1.49 (0.58–3.83) | 1.49 (0.49–4.53) | 1.19 (0.95–1.50) | 0.13 |
| Non-cardia | ||||||
| Cases/Controls | 49/94 | 93/94 | 126/95 | 84/94 | 352/377 | |
| Crude | 1.00 | 1.90 (1.21–2.97) | 2.54 (1.65–3.94) | 1.71 (1.09–2.70) | 1.13 (1.03–1.25) | 0.01 |
| Model 1 | 1.00 | 1.60 (0.89–2.88) | 2.28 (1.24–4.19) | 1.82 (0.86–3.88) | 1.19 (1.02–1.40) | 0.03 |
| Model 2 | 1.00 | 1.75 (0.86–3.60) | 2.54 (1.19–5.41) | 3.93 (1.59–9.70) | 1.28 (1.07–1.55) | 0.01 |
| Histological subtype 2 | ||||||
| Diffuse | ||||||
| Cases/Controls | 29/94 | 55/94 | 76/95 | 43/94 | 203/377 | |
| Crude | 1.00 | 1.90 (1.11–3.23) | 2.59 (1.55–4.34) | 1.48 (0.86–2.57) | 1.12 (0.99–1.25) | 0.06 |
| Model 1 | 1.00 | 1.68 (0.87–3.17) | 2.43 (1.26–4.68) | 2.30 (1.00–5.23) | 1.23 (1.07–1.51) | 0.01 |
| Model 2 | 1.00 | 1.45 (0.67–3.13) | 2.36 (1.06–5.23) | 2.90 (1.06–7.82) | 1.30 (1.06–1.60) | 0.01 |
| Intestinal | ||||||
| Cases/Controls | 25/94 | 48/94 | 62/95 | 39/94 | 174/377 | |
| Crude | 1.00 | 1.92 (1.10–3.37) | 2.45 (1.42–4.23) | 1.56 (0.87–2.78) | 1.13 (0.99–1.23) | 0.06 |
| Model 1 | 1.00 | 1.93 (0.98–3.84) | 2.34 (1.15–4.77) | 1.53 (0.63–3.70) | 1.20 (1.00–1.44) | 0.05 |
| Model 2 | 1.00 | 1.75 (0.75–4.10) | 2.16 (0.88–5.30) | 2.58 (0.89–7.44) | 1.26 (1.00–1.57) | 0.04 |
| E-DII Quartiles | Per 1-Point Increment in theE-DII Score | |||||
|---|---|---|---|---|---|---|
| Q1 (−5.09, −2.04) | Q2 (−2.03, −0.83) | Q3 (−0.82, 0.25) | Q4 (>0.25) | p-Trend ‡ | ||
| OR | OR (95% CI) | OR (95% CI) | OR (95% CI) | |||
| All 1 | ||||||
| Cases/Controls | 65/194 | 119/194 | 156/194 | 152/195 | 492/777 | |
| Crude | 1.00 | 1.83 (1.28–2.65) | 2.41 (1.69–3.44) | 2.35 (1.65–3.36) | 1.20 (1.11–1.29) | <0.001 |
| Model 1 a | 1.00 | 1.42 (0.91–2.22) | 2.27 (1.44–3.58) | 2.70 (1.60–4.54) | 1.27 (1.13–1.43) | <0.001 |
| Anatomical location 2 | ||||||
| Cardia | ||||||
| Cases/Controls | 11/194 | 30/194 | 24/194 | 36/195 | 101/777 | |
| Crude | 1.00 | 2.72 (1.33–5.60) | 2.18 (1.04–4.58) | 3.27 (1.62–6.62) | 1.24 (1.08–1.43) | 0.002 |
| Model 1 | 1.00 | 1.87 (0.84–4.15) | 2.18 (0.95–5.04) | 3.31 (1.32–8.24) | 1.31 (1.08–1.60) | 0.007 |
| Non-cardia | ||||||
| Cases/Controls | 48/194 | 84/194 | 118/194 | 103/195 | 352/777 | |
| Crude | 1.00 | 1.75 (1.17–2.63) | 2.46 (1.66–3.63) | 2.15 (1.44–3.19) | 1.18 (1.08–1.28) | <0.001 |
| Model 1 | 1.00 | 1.44 (0.86–2.39) | 2.43 (1.44–4.09) | 2.97 (1.64–5.39) | 1.30 (1.14–1.50) | <0.001 |
| Histological subtype 2 | ||||||
| Diffuse | ||||||
| Cases/Controls | 28/194 | 48/194 | 71/194 | 56/195 | 203/777 | |
| Crude | 1.00 | 1.71 (1.03–2.85) | 2.53 (1.56–4.10) | 2.00 (1.21–3.26) | 1.16 (1.05–1.29) | 0.005 |
| Model 1 | 1.00 | 1.33 (0.73–2.43) | 2.80 (1.54–5.10) | 2.48 (1.23–5.00) | 1.26 (1.08–1.48) | 0.003 |
| Intestinal | ||||||
| Cases/Controls | 23/194 | 46/194 | 54/194 | 51/195 | 174/777 | |
| Crude | 1.00 | 2.00 (1.17–3.43) | 2.35 (1.38–3.98) | 2.21 (1.30–3.75) | 1.17 (1.05–1.31) | 0.006 |
| Model 1 | 1.00 | 1.66 (0.89–3.06) | 2.52 (1.34–4.74) | 2.82 (1.38–5.74) | 1.30 (1.10–1.51) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, A.R.C.; Guandalini, V.R.; Pereira, T.S.S.; Zhao, L.; Wirth, M.D.; Hébert, J.R.; Fernandes, G.A.; de Assumpção, P.P.; Barbosa, M.S.; Curado, M.P. Association between Dietary Inflammatory Index and Gastric Adenocarcinoma: A Multicenter Case-Control Study in Brazil. Nutrients 2023, 15, 2867. https://doi.org/10.3390/nu15132867
Silva ARC, Guandalini VR, Pereira TSS, Zhao L, Wirth MD, Hébert JR, Fernandes GA, de Assumpção PP, Barbosa MS, Curado MP. Association between Dietary Inflammatory Index and Gastric Adenocarcinoma: A Multicenter Case-Control Study in Brazil. Nutrients. 2023; 15(13):2867. https://doi.org/10.3390/nu15132867
Chicago/Turabian StyleSilva, Alex Richard Costa, Valdete Regina Guandalini, Taísa Sabrina Silva Pereira, Longgang Zhao, Michael D. Wirth, James R. Hébert, Gisele Aparecida Fernandes, Paulo Pimentel de Assumpção, Mônica Santiago Barbosa, and Maria Paula Curado. 2023. "Association between Dietary Inflammatory Index and Gastric Adenocarcinoma: A Multicenter Case-Control Study in Brazil" Nutrients 15, no. 13: 2867. https://doi.org/10.3390/nu15132867
APA StyleSilva, A. R. C., Guandalini, V. R., Pereira, T. S. S., Zhao, L., Wirth, M. D., Hébert, J. R., Fernandes, G. A., de Assumpção, P. P., Barbosa, M. S., & Curado, M. P. (2023). Association between Dietary Inflammatory Index and Gastric Adenocarcinoma: A Multicenter Case-Control Study in Brazil. Nutrients, 15(13), 2867. https://doi.org/10.3390/nu15132867