
Astaxanthin Supplemented with High-Intensity Functional Training Decreases Adipokines Levels and Cardiovascular Risk Factors in Men with Obesity

 , , , , ,
, , , , , 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Body Composition and Cardio-Respiratory Fitness Assessments
2.3. Training Protocols
2.4. Supplementation of Astaxanthin and Placebo
2.5. Nutrient Intake and Dietary Analysis
2.6. Assessment of Blood Markers
2.7. Statistical Analysis
3. Results
3.1. Anthropometric Characteristics and Cardio-Respiratory Parameters
3.2. Lipid Profiles
3.3. Metabolic Factors
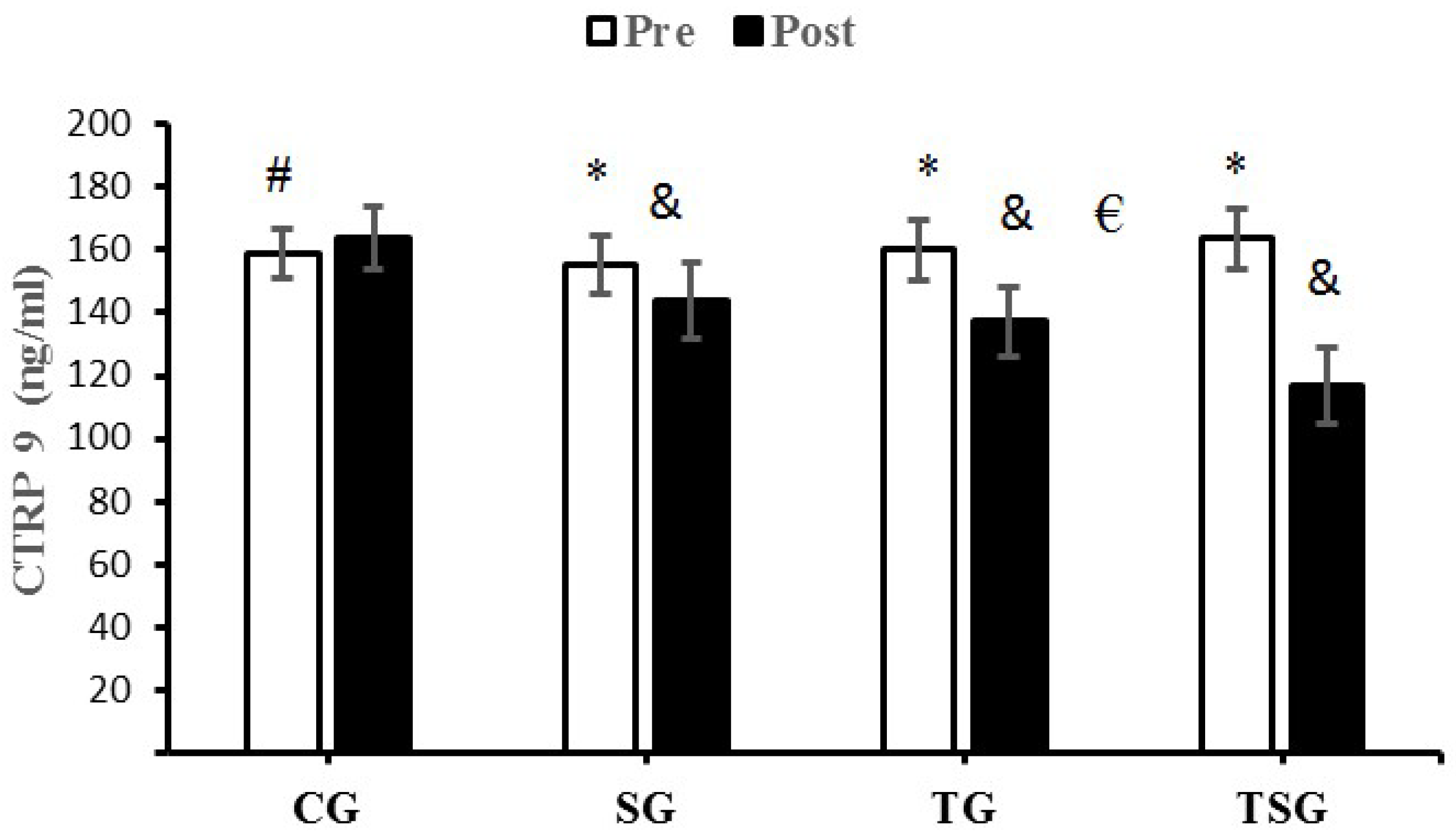
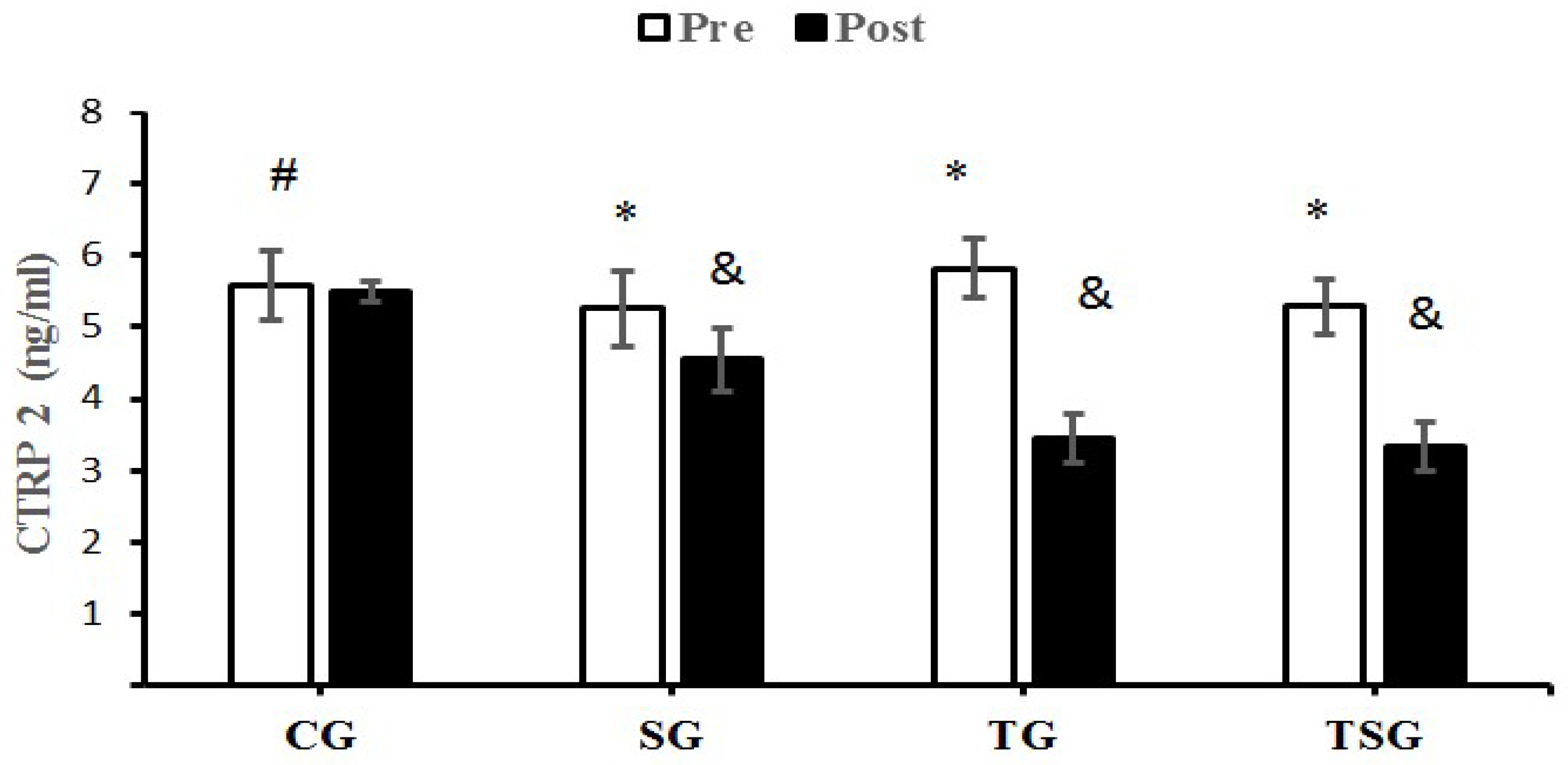
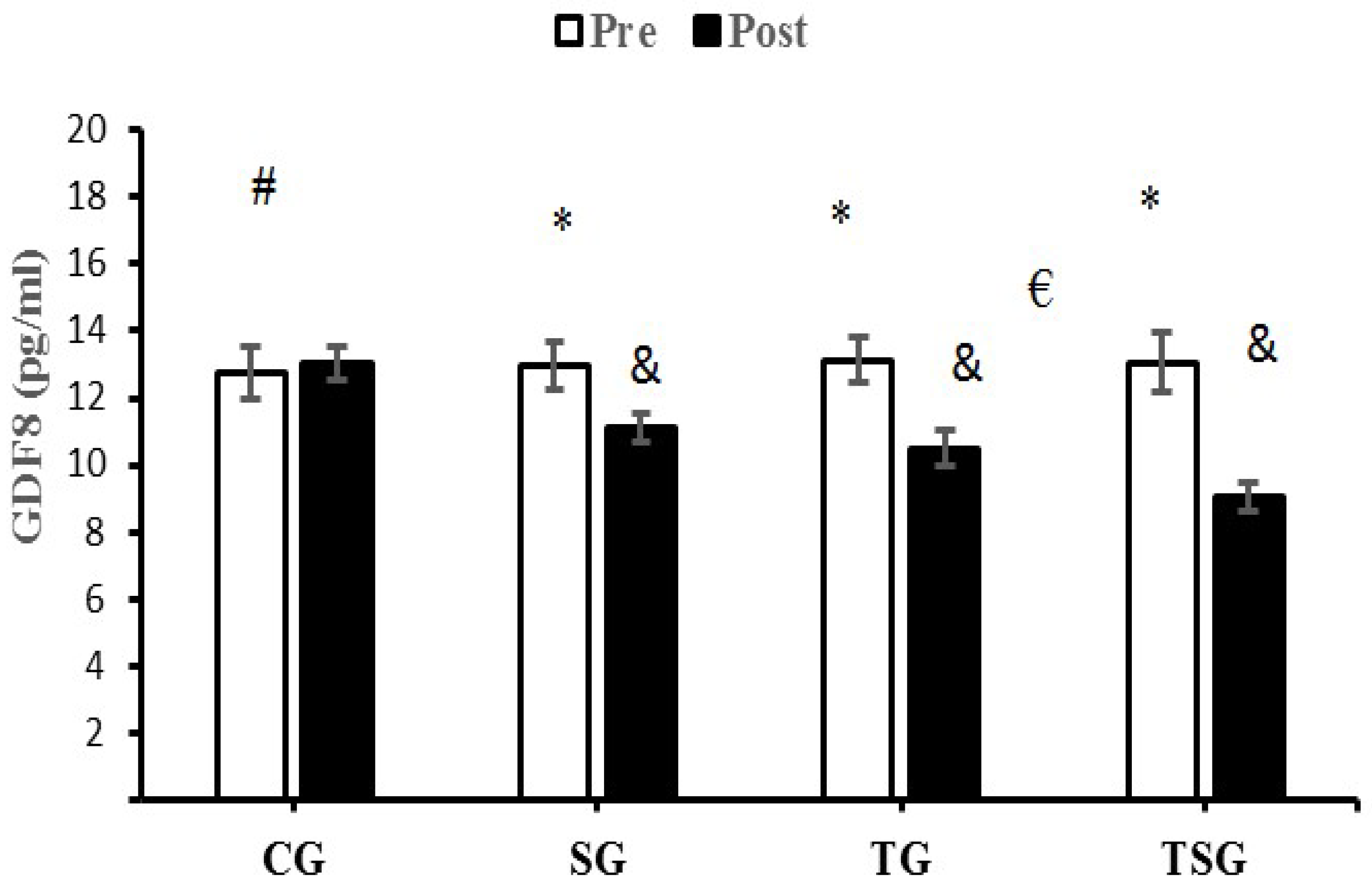
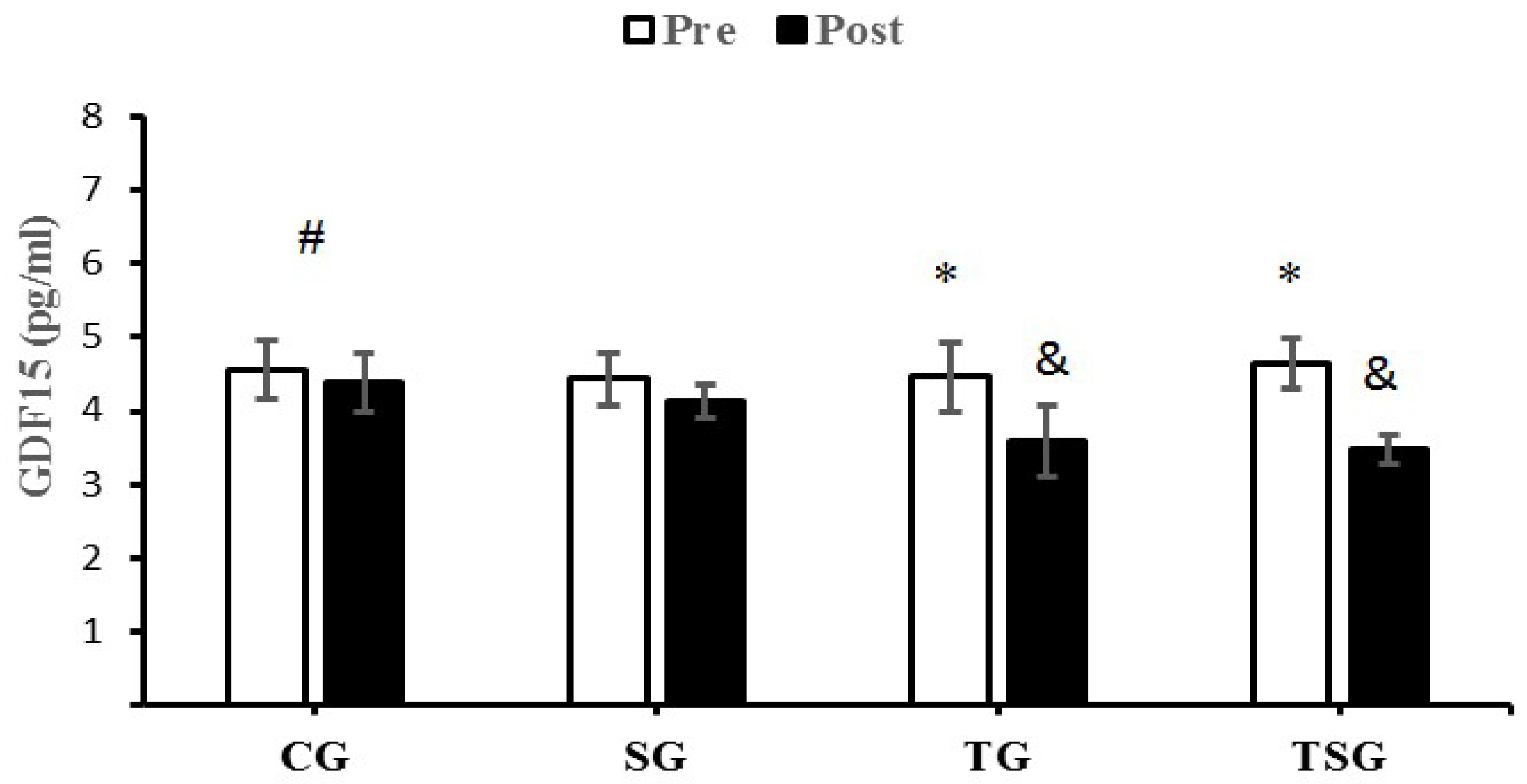
3.4. Adipokines and Growth Differentiation Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeidi, A.; Tayebi, S.M.; Khosravi, A.; Razi, O.; Sellami, M.; Abderrahman, A.B.; Zouhal, H. Obesity, Fat Mass, Osteopontin and Exercise Training. Int. J. Appl. Exerc. Physiol. 2019, 8, 177–179. [Google Scholar]
- Haslam, D.W.; James, W.P. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2017, 114, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Shoelson, S.E.; Herrero, L.; Naaz, A. Obesity, inflammation, and insulin resistance. Gastroenterology 2007, 132, 2169–2180. [Google Scholar] [CrossRef] [PubMed]
- Lumeng, C.N.; Saltiel, A.R. Inflammatory links between obesity and metabolic disease. J. Clin. Investig. 2011, 121, 2111–2117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, J.M.; Wei, Z.; Seldin, M.M.; Byerly, M.S.; Aja, S.; Wong, G.W. CTRP9 transgenic mice are protected from diet-induced obesity and metabolic dysfunction. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 305, R522–R533. [Google Scholar] [CrossRef] [Green Version]
- Jerobin, J.; Ramanjaneya, M.; Bettahi, I.; Parammal, R.; Siveen, K.S.; Alkasem, M.; Aye, M.; Sathyapalan, T.; Skarulis, M.; Atkin, S.L. Regulation of circulating CTRP-2/CTRP-9 and GDF-8/GDF-15 by intralipids and insulin in healthy control and polycystic ovary syndrome women following chronic exercise training. Lipids Health Dis. 2021, 20, 1–11. [Google Scholar] [CrossRef]
- Seldin, M.M.; Tan, S.Y.; Wong, G.W. Metabolic function of the CTRP family of hormones. Rev. Endocr. Metab. Disord. 2014, 15, 111–123. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.W.; Krawczyk, S.A.; Kitidis-Mitrokostas, C.; Revett, T.; Gimeno, R.; Lodish, H.F. Molecular, biochemical and functional characterizations of C1q/TNF family members: Adipose-tissue-selective expression patterns, regulation by PPAR-γ agonist, cysteine-mediated oligomerizations, combinatorial associations and metabolic functions. Biochem. J. 2008, 416, 161–177. [Google Scholar] [CrossRef] [Green Version]
- Wolf, R.M.; Steele, K.E.; Peterson, L.A.; Zeng, X.; Jaffe, A.E.; Schweitzer, M.A.; Magnuson, T.H.; Wong, G.W. C1q/TNF-related protein-9 (CTRP9) levels are associated with obesity and decrease following weight loss surgery. J. Clin. Endocrinol. Metab. 2016, 101, 2211–2217. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.M.; Seldin, M.M.; Tan, S.Y.; Wong, G.W. CTRP2 overexpression improves insulin and lipid tolerance in diet-induced obese mice. PLoS ONE 2014, 9, e88535. [Google Scholar] [CrossRef] [PubMed]
- Hanna, A.; Frangogiannis, N.G. The role of the TGF-β superfamily in myocardial infarction. Front. Cardiovasc. Med. 2019, 6, 140. [Google Scholar] [CrossRef]
- Guo, T.; Jou, W.; Chanturiya, T.; Portas, J.; Gavrilova, O.; McPherron, A.C. Myostatin inhibition in muscle, but not adipose tissue, decreases fat mass and improves insulin sensitivity. PLoS ONE 2009, 4, e4937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, Q.; Mracek, T.; Gonzalez-Muniesa, P.; Kos, K.; Wilding, J.; Trayhurn, P.; Bing, C. Identification of macrophage inhibitory cytokine-1 in adipose tissue and its secretion as an adipokine by human adipocytes. Endocrinology 2009, 150, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.; Yang, J.; Gardner, J.; Xiong, Y. GDF15 deficiency promotes high fat diet-induced obesity in mice. PLoS ONE 2018, 13, e0201584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hale, C.; Véniant, M.M. Growth differentiation factor 15 as a potential therapeutic for treating obesity. Mol. Metab. 2021, 46, 101117. [Google Scholar] [CrossRef]
- Lu, J.F.; Zhu, M.Q.; Xie, B.C.; Shi, X.C.; Liu, H.; Zhang, R.X.; Xia, B.; Wu, J.W. Camptothecin effectively treats obesity in mice through GDF15 induction. PLoS Biol. 2022, 20, e3001517. [Google Scholar] [CrossRef]
- Pervin, S.; Reddy, S.T.; Singh, R. Novel Roles of Follistatin/Myostatin in Transforming Growth Factor-β Signaling and Adipose Browning: Potential for Therapeutic Intervention in Obesity Related Metabolic Disorders. Front. Endocrinol. 2021, 12, 339. [Google Scholar] [CrossRef]
- Koncarevic, A.; Kajimura, S.; Cornwall-Brady, M.; Andreucci, A.; Pullen, A.; Sako, D.; Kumar, R.; Grinberg, A.V.; Liharska, K.; Ucran, J.A. A novel therapeutic approach to treating obesity through modulation of TGFβ signaling. Endocrinology 2012, 153, 3133–3146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolnes, K.J.; Petersen, M.H.; Lien-Iversen, T.; Højlund, K.; Jensen, J. Effect of Exercise Training on Fat Loss—Energetic Perspectives and the Role of Improved Adipose Tissue Function and Body Fat Distribution. Front. Physiol. 2021, 1634. [Google Scholar] [CrossRef]
- Durkalec-Michalski, K.; Nowaczyk, P.M.; Siedzik, K. Effect of a four-week ketogenic diet on exercise metabolism in CrossFit-trained athletes. J. Int. Soc. Sport. Nutr. 2019, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Kliszczewicz, B.; Quindry, C.J.; Blessing, L.D.; Oliver, D.G.; Esco, R.M.; Taylor, J.K. Acute exercise and oxidative stress: CrossFit™ vs. treadmill bout. J. Hum. Kinet. 2015, 47, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feito, Y.; Heinrich, K.M.; Butcher, S.J.; Poston, W.S.C. High-intensity functional training (HIFT): Definition and research implications for improved fitness. Sports 2018, 6, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibana, R.A.; De Almeida, L.M.; de Sousa, N.M.F.; Dda, C.N.; Neto, I.; De Almeida, J.A.; De Souza, V.C.; Mde, F.L.; Ode, T.N.; Vieira, D. Two consecutive days of crossfit training affects pro and anti-inflammatory cytokines and osteoprotegerin without impairments in muscle power. Front. Physiol. 2016, 7, 260. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, P. CrossFit® training strategies from the perspective of concurrent training: A systematic review. J. Sport. Sci. Med. 2020, 19, 670. [Google Scholar]
- Xia, W.; Tang, N.; Kord-Varkaneh, H.; Low, T.Y.; Tan, S.C.; Wu, X.; Zhu, Y. The effects of astaxanthin supplementation on obesity, blood pressure, CRP, glycemic biomarkers, and lipid profile: A meta-analysis of randomized controlled trials. Pharmacol. Res. 2020, 161, 105113. [Google Scholar] [CrossRef]
- Fakhri, S.; Abbaszadeh, F.; Dargahi, L.; Jorjani, M. Astaxanthin: A mechanistic review on its biological activities and health benefits. Pharmacol. Res. 2018, 136, 1–20. [Google Scholar] [CrossRef]
- Aoi, W.; Naito, Y.; Takanami, Y.; Ishii, T.; Kawai, Y.; Akagiri, S.; Kato, Y.; Osawa, T.; Yoshikawa, T. Astaxanthin improves muscle lipid metabolism in exercise via inhibitory effect of oxidative CPT I modification. Biochem. Biophys. Res. Commun. 2008, 366, 892–897. [Google Scholar] [CrossRef]
- Thomas, S.; Reading, J.; Shephard, R.J. Revision of the physical activity readiness questionnaire (PAR-Q). Can. J. Sport Sci. 1992, 17, 338–445. [Google Scholar]
- Nathanson, V. Revising the Declaration of Helsinki; BMJ Publishing Group Ltd.: London, UK, 2013; Volume 346. [Google Scholar]
- Ghroubi, S.; Elleuch, H.; Chikh, T.; Kaffel, N.; Abid, M.; Elleuch, M. Physical training combined with dietary measures in the treatment of adult obesity. A comparison of two protocols. Ann. Phys. Rehabil. Med. 2009, 52, 394–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, G.R.; Byrne, N.M.; Sirikul, B.; Fernández, J.R.; Zuckerman, P.A.; Darnell, B.E.; Gower, B.A. Resistance training conserves fat-free mass and resting energy expenditure following weight loss. Obesity 2008, 16, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094. [Google Scholar] [CrossRef] [PubMed]
- Perciavalle, V.; Marchetta, N.S.; Giustiniani, S.; Borbone, C.; Perciavalle, V.; Petralia, M.C.; Buscemi, A.; Coco, M. Attentive processes, blood lactate and CrossFit®. Physician Sportsmed. 2016, 44, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Timón, R.; Olcina, G.; Camacho-Cardeñosa, M.; Camacho-Cardenosa, A.; Martinez-Guardado, I.; Marcos-Serrano, M. 48-hour recovery of biochemical parameters and physical performance after two modalities of CrossFit workouts. Biol. Sport 2019, 36, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Mangine, G.T.; Van Dusseldorp, T.A.; Feito, Y.; Holmes, A.J.; Serafini, P.R.; Box, A.G.; Gonzalez, A.M. Testosterone and cortisol responses to five high-intensity functional training competition workouts in recreationally active adults. Sports 2018, 6, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glassman, G. A theoretical template for crossfit’s programming. CrossFit J. 2003, 6, 1–5. [Google Scholar]
- Heinrich, K.M.; Patel, P.M.; O’Neal, J.L.; Heinrich, B.S. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014, 14, 789. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and athletic performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef]
- Hsing, A.W.; Gao, Y.-T.; Chua, S.; Deng, J.; Stanczyk, F.Z. Insulin resistance and prostate cancer risk. J. Natl. Cancer Inst. 2003, 95, 67–71. [Google Scholar] [CrossRef] [Green Version]
- Serra, D.; Mera, P.; Malandrino, M.I.; Mir, J.F.; Herrero, L. Mitochondrial fatty acid oxidation in obesity. Antioxid. Redox Signal. 2013, 19, 269–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha-Rodrigues, S.; Rodríguez, A.; Gouveia, A.M.; Gonçalves, I.O.; Becerril, S.; Ramírez, B.; Beleza, J.; Frühbeck, G.; Ascensão, A.; Magalhães, J. Effects of physical exercise on myokines expression and brown adipose-like phenotype modulation in rats fed a high-fat diet. Life Sci. 2016, 165, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Cheema, S.K.; Clandinin, M.T. Diet fat alters expression of genes for enzymes of lipogenesis in lean and obese mice. Biochim. Biophys. Acta (BBA) Lipids Lipid Metab. 1996, 1299, 284–288. [Google Scholar] [CrossRef]
- Itani, S.I.; Ruderman, N.B.; Schmieder, F.; Boden, G. Lipid-induced insulin resistance in human muscle is associated with changes in diacylglycerol, protein kinase C, and IκB-α. Diabetes 2002, 51, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Coppack, S.; Evans, R.; Fisher, R.; Frayn, K.; Gibbons, G.; Humphreys, S.; Kirk, M.; Potts, J.; Hockaday, T. Adipose tissue metabolism in obesity: Lipase action in vivo before and after a mixed meal. Metabolism 1992, 41, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.L.; Goldfine, I.D.; Maddux, B.A.; Grodsky, G.M. Oxidative stress and stress-activated signaling pathways: A unifying hypothesis of type 2 diabetes. Endocr. Rev. 2002, 23, 599–622. [Google Scholar] [CrossRef] [Green Version]
- Murano, I.; Barbatelli, G.; Parisani, V.; Latini, C.; Muzzonigro, G.; Castellucci, M.; Cinti, S. Dead adipocytes, detected as crown-like structures, are prevalent in visceral fat depots of genetically obese mice. J. Lipid Res. 2008, 49, 1562–1568. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, S.; Manabe, I.; Nagasaki, M.; Eto, K.; Yamashita, H.; Ohsugi, M.; Otsu, M.; Hara, K.; Ueki, K.; Sugiura, S. CD8+ effector T cells contribute to macrophage recruitment and adipose tissue inflammation in obesity. Nat. Med. 2009, 15, 914–920. [Google Scholar] [CrossRef]
- Tsuda, T.; Horio, F.; Uchida, K.; Aoki, H.; Osawa, T. Dietary cyanidin 3-O-β-D-glucoside-rich purple corn color prevents obesity and ameliorates hyperglycemia in mice. J. Nutr. 2003, 133, 2125–2130. [Google Scholar] [CrossRef] [Green Version]
- Wolfram, S.; Wang, Y.; Thielecke, F. Anti-obesity effects of green tea: From bedside to bench. Mol. Nutr. Food Res. 2006, 50, 176–187. [Google Scholar] [CrossRef]
- Kobayashi, M. In vivo antioxidant role of astaxanthin under oxidative stress in the green alga Haematococcus pluvialis. Appl. Microbiol. Biotechnol. 2000, 54, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Bennedsen, M.; Wang, X.; Willén, R.; Wadström, T.; Andersen, L.P. Treatment of H. pylori infected mice with antioxidant astaxanthin reduces gastric inflammation, bacterial load and modulates cytokine release by splenocytes. Immunol. Lett. 2000, 70, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.D.; Kim, J.H.; Chang, M.J.; Kyu-Youn, Y.; Shin, W.G. Effects of astaxanthin on oxidative stress in overweight and obese adults. Phytother. Res. 2011, 25, 1813–1818. [Google Scholar] [CrossRef]
- Speranza, L.; Pesce, M.; Patruno, A.; Franceschelli, S.; De Lutiis, M.A.; Grilli, A.; Felaco, M. Astaxanthin treatment reduced oxidative induced pro-inflammatory cytokines secretion in U937: SHP-1 as a novel biological target. Mar. Drugs 2012, 10, 890–899. [Google Scholar] [CrossRef]
- Nawaz, A.; Nishida, Y.; Takikawa, A.; Fujisaka, S.; Kado, T.; Aminuddin, A.; Bilal, M.; Jeelani, I.; Aslam, M.R.; Nishimura, A. Astaxanthin, a Marine Carotenoid, Maintains the Tolerance and Integrity of Adipose Tissue and Contributes to Its Healthy Functions. Nutrients 2021, 13, 4374. [Google Scholar] [CrossRef]
- Lee, S.J.; Bai, S.K.; Lee, K.S.; Namkoong, S.; Na, H.J.; Ha, K.S.; Han, J.A.; Yim, S.V.; Chang, K.; Kwon, Y.G.; et al. Astaxanthin Inhibits Nitric Oxide Production and Inflammatory Gene Expression by Suppressing I (kappa) B Kinase-dependent NF-(kappa) B Activation. Mol. Cells 2003, 16, 97–105. [Google Scholar]
- Ikeuchi, M.; Koyama, T.; Takahashi, J.; Yazawa, K. Effects of astaxanthin supplementation on exercise-induced fatigue in mice. Biol. Pharm. Bull. 2006, 29, 2106–2110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feito, Y.; Hoffstetter, W.; Serafini, P.; Mangine, G. Changes in body composition, bone metabolism, strength, and skill-specific performance resulting from 16-weeks of HIFT. PLoS ONE 2018, 13, e0198324. [Google Scholar] [CrossRef]
- Murawska-Cialowicz, E.; Wojna, J.; Zuwala-Jagiello, J. Crossfit training changes brain-derived neurotrophic factor and irisin levels at rest, after wingate and progressive tests, and improves aerobic capacity and body composition of young physically active men and women. J. Physiol. Pharmacol. 2015, 66, 811–821. [Google Scholar]
- Cocks, M.; Shaw, C.S.; Shepherd, S.O.; Fisher, J.P.; Ranasinghe, A.M.; Barker, T.A.; Tipton, K.D.; Wagenmakers, A.J. Sprint interval and endurance training are equally effective in increasing muscle microvascular density and eNOS content in sedentary males. J. Physiol. 2013, 591, 641–656. [Google Scholar] [CrossRef]
- Shepherd, S.O.; Cocks, M.; Tipton, K.; Ranasinghe, A.M.; Barker, T.A.; Burniston, J.G.; Wagenmakers, A.J.; Shaw, C.S. Sprint interval and traditional endurance training increase net intramuscular triglyceride breakdown and expression of perilipin 2 and 5. J. Physiol. 2013, 591, 657–675. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Seo, J.M.; Nguyen, A.; Pham, T.X.; Park, H.J.; Park, Y.; Kim, B.; Bruno, R.S.; Lee, J. Astaxanthin-rich extract from the green alga Haematococcus pluvialis lowers plasma lipid concentrations and enhances antioxidant defense in apolipoprotein E knockout mice. J. Nutr. 2011, 141, 1611–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishimoto, Y.; Yoshida, H.; Kondo, K. Potential anti-atherosclerotic properties of astaxanthin. Mar. Drugs 2016, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.Y.; Park, J.W.; Lee, N.; Hwang, S.Y.; Cho, G.J.; Hong, H.C.; Yoo, H.J.; Hwang, T.G.; Kim, S.M.; Baik, S.H. Effects of a combined aerobic and resistance exercise program on C1q/TNF-related protein-3 (CTRP-3) and CTRP-5 levels. Diabetes Care 2013, 36, 3321–3327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPherron, A.C.; Lawler, A.M.; Lee, S.-J. Regulation of skeletal muscle mass in mice by a new TGF-p superfamily member. Nature 1997, 387, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Schuelke, M.; Wagner, K.R.; Stolz, L.E.; Hübner, C.; Riebel, T.; Kömen, W.; Braun, T.; Tobin, J.F.; Lee, S.-J. Myostatin mutation associated with gross muscle hypertrophy in a child. N. Engl. J. Med. 2004, 350, 2682–2688. [Google Scholar] [CrossRef]
- Keipert, S.; Ost, M. Stress-induced FGF21 and GDF15 in obesity and obesity resistance. Trends Endocrinol. Metab. 2021, 32, 904–915. [Google Scholar] [CrossRef]
- Sarkar, S.; Legere, S.; Haidl, I.; Marshall, J.; MacLeod, J.B.; Aguiar, C.; Lutchmedial, S.; Hassan, A.; Brunt, K.R.; Kienesberger, P. Serum GDF15, a promising biomarker in obese patients undergoing heart surgery. Front. Cardiovasc. Med. 2020, 7, 103. [Google Scholar] [CrossRef]
- Kempf, T.; Guba-Quint, A.; Torgerson, J.; Magnone, M.C.; Haefliger, C.; Bobadilla, M.; Wollert, K.C. Growth differentiation factor 15 predicts future insulin resistance and impaired glucose control in obese nondiabetic individuals: Results from the XENDOS trial. Eur. J. Endocrinol. 2012, 167, 671. [Google Scholar] [CrossRef] [Green Version]
- Vila, G.; Riedl, M.; Anderwald, C.; Resl, M.; Handisurya, A.; Clodi, M.; Prager, G.; Ludvik, B.; Krebs, M.; Luger, A. The relationship between insulin resistance and the cardiovascular biomarker growth differentiation factor-15 in obese patients. Clin. Chem. 2011, 57, 309–316. [Google Scholar] [CrossRef] [Green Version]
- Cai, L.; Li, C.; Wang, Y.; Mo, Y.; Yin, J.; Ma, X. Increased serum GDF15 related to improvement in metabolism by lifestyle intervention among young overweight and obese adults. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 1195. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Fealy, C.E.; Kirwan, J.P. Exercise training promotes a GDF15-associated reduction in fat mass in older adults with obesity. Am. J. Physiol. Endocrinol. Metab. 2019, 316, E829–E836. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.B.; Nicolaisen, T.S.; Ørtenblad, N.; Gejl, K.D.; Jensen, R.; Fritzen, A.M.; Larsen, E.L.; Karstoft, K.; Poulsen, H.E.; Morville, T. Pharmacological but not physiological GDF15 suppresses feeding and the motivation to exercise. Nat. Commun. 2021, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Laurens, C.; Parmar, A.; Murphy, E.; Carper, D.; Lair, B.; Maes, P.; Vion, J.; Boulet, N.; Fontaine, C.; Marquès, M. Growth and differentiation factor 15 is secreted by skeletal muscle during exercise and promotes lipolysis in humans. JCI Insight 2020, 5, e131870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinert, M.; Clemmensen, C.; Sjøberg, K.A.; Carl, C.S.; Jeppesen, J.F.; Wojtaszewski, J.F.; Kiens, B.; Richter, E.A. Exercise increases circulating GDF15 in humans. Mol. Metab. 2018, 9, 187–191. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, M.C.; Gerosa-Neto, J.; Zanchi, N.E.; Lira, F.S.; Rossi, F.E. Role of metabolic stress for enhancing muscle adaptations: Practical applications. World J. Methodol. 2017, 7, 46. [Google Scholar] [CrossRef]
- Kaspar, F.; Jelinek, H.F.; Perkins, S.; Al-Aubaidy, H.A.; Dejong, B.; Butkowski, E. Acute-phase inflammatory response to single-bout HIIT and endurance training: A comparative study. Mediat. Inflamm. 2016, 2016, 5474837. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Walker, K.; Min, X.; Hale, C.; Tran, T.; Komorowski, R.; Yang, J.; Davda, J.; Nuanmanee, N.; Kemp, D. Long-acting MIC-1/GDF15 molecules to treat obesity: Evidence from mice to monkeys. Sci. Transl. Med. 2017, 9, eaan8732. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CG | SG | TG | TSG | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Energy (kcal/day) | 2260 ± 47 | 2269 ± 56 | 2278 ± 101 | 2149 ± 100 | 2269 ± 117 | 2141 ± 117 | 2273 ± 157 | 2129 ± 126 |
| CHO (g/day) | 281 ± 31.4 | 283 ± 33.3 | 279.4 ± 27.1 | 261 ± 27.5 | 289 ± 48.6 | 261 ± 39.2 | 288 ± 38.6 | 259 ± 29.1 |
| Fat (g/day) | 82.2 ± 11.0 | 81 ± 9.8 | 86.5 ± 10.7 | 75 ± 11.2 | 83.4 ± 12.4 | 73.1 ± 11.2 | 80.8 ± 13.87 | 70.2 ± 11.3 |
| Protein (g/day) | 104 ± 12.0 | 106 ± 11.3 | 101 ± 13.5 | 93 ± 12.6 | 103 ± 14.8 | 94 ± 11.7 | 102 ± 14.5 | 90 ± 13.5 |
| CG | SG | TG | TSG | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Height (cm) | 167.5 ± 2.7 | - | 168.2 ± 3.5 | - | 167.5 ± 4.1 | - | 167.7 ± 3.1 | - |
| Weight (kg) | 95.3 ± 1.8 | 92.1 ± 2.1 | 94.2 ± 2.6 | 90.1 ± 2.3 a | 94.3 ± 0.9 | 90.1 ± 2.3 a,b | 95.1 ± 1.9 | 88.2 ± 2.3 a,b,ab |
| Fat percentage (%) | 31.1 ± 1.5 | 31.8 ± 2.1 a | 31.1 ± 1.5 | 29.0 ± 0.7 a,b | 31.3 ± 1.4 | 27.8 ± 0.9 a,b | 32.1 ± 1.3 | 27.6 ± 1.2 a,b,ab |
| BMI (kg/m2) | 34.1 ± 2.5 | 33.7 ± 1.4 | 33.2 ± 1.4 | 32.4 ± 1.6 a,b | 33.5 ± 1.7 | 32.1 ± 1.5 a,b | 33.8 ± 1.2 | 31.8 ± 0.6 a,b,ab |
| FFM (kg) | 26.6 ± 1.2 | 25.5 ± 2.2 | 26.1 ± 1.8 | 28.5 ± 0.8 a,b | 25.7 ± 1.2 | 28.4 ± 1.6 a,b | 26.1 ± 1.7 | 29.3 ± 1.2 a,b,ab |
| VO2peak (mL·kg−1·min−1) | 26.2 ± 2.4 | 25.9 ± 2.2 | 26.1 ± 2.8 | 26.5 ± 2.9 a | 26.3 ± 2.3 | 28.9 ± 1.9 a,b | 26.0 ± 2.1 | 29.1 ± 2.2 a,b,ab |
| HDL (mg·dL−1) | 38.3 ± 1.2 | 37.4 ± 1.30 | 37.8 ± 1.23 | 39.8 ± 1.2 a | 37.6 ± 1.6 | 43.5 ± 1.3 a,b | 37.5 ± 1.4 | 44.2 ± 1.1 a,b,ab |
| LDL (mg·dL−1) | 127.2 ± 4.4 | 127.0 ± 4.7 | 127.5 ± 5.4 | 123.4 ± 5.2 a,b | 128.7 ± 4.3 | 113.2 ± 2.9 a,b | 129.1 ± 3.6 | 112.5 ± 2.5 a,b,ab |
| TC (mg·dL−1) | 228.7 ± 5.2 | 228.8 ± 5.2 | 229.4 ± 5.4 | 224.0 ± 5.1 a,b | 232.1 ± 1.6 | 211.4 ± 2.6 a,b | 231.5 ± 5.1 | 207.2 ± 2.1 a,b.ab |
| TG (mg·dL−1) | 244.1 ± 4.3 | 244.8 ± 3.8 | 247.8 ± 5.9 | 244.1 ± 5.4 a | 246.5 ± 7.4 | 217.0 ± 5.4 a,b | 244.9 ± 5.9 | 214.8 ± 4.6 a,b,ab |
| Insulin (ng·mL)−1 | 19.1 ± 0.6 | 19.4 ± 0.5 | 19.1 ± 0.7 | 17.9 ± 0.5 a,b | 19.1 ± 0.4 | 16.4 ± 0.4 | 19.4 ± 0.4 | 15.8 ± 0.5 a,b,ab |
| Glucose (mg·dL−1) | 100.4 ± 13.1 | 94.7 ± 6.4 | 102.9 ± 10.7 | 88.7 ± 4.5 a,b | 103.2 ± 5.7 | 78.0 ± 5.4 | 105.6 ± 7.1 | 75.5 ± 7.7 a,b,ab |
| HOMA-IR | 4.7 ± 0.7 | 4.5 ± 0.3 | 4.8 ± 0.4 | 3.9 ± 0.2 a | 4.8 ± 0.2 | 3.1 ± 0.2 | 5.0 ± 0.3 | 2.9 ± 0.3 a,b,ab |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeidi, A.; Nouri-Habashi, A.; Razi, O.; Ataeinosrat, A.; Rahmani, H.; Mollabashi, S.S.; Bagherzadeh-Rahmani, B.; Aghdam, S.M.; Khalajzadeh, L.; Al Kiyumi, M.H.; et al. Astaxanthin Supplemented with High-Intensity Functional Training Decreases Adipokines Levels and Cardiovascular Risk Factors in Men with Obesity. Nutrients 2023, 15, 286. https://doi.org/10.3390/nu15020286
Saeidi A, Nouri-Habashi A, Razi O, Ataeinosrat A, Rahmani H, Mollabashi SS, Bagherzadeh-Rahmani B, Aghdam SM, Khalajzadeh L, Al Kiyumi MH, et al. Astaxanthin Supplemented with High-Intensity Functional Training Decreases Adipokines Levels and Cardiovascular Risk Factors in Men with Obesity. Nutrients. 2023; 15(2):286. https://doi.org/10.3390/nu15020286
Chicago/Turabian StyleSaeidi, Ayoub, Akbar Nouri-Habashi, Omid Razi, Ali Ataeinosrat, Hiwa Rahmani, Shirin Shirzad Mollabashi, Behnam Bagherzadeh-Rahmani, Shahin Mahmoudi Aghdam, Leila Khalajzadeh, Maisa Hamed Al Kiyumi, and et al. 2023. "Astaxanthin Supplemented with High-Intensity Functional Training Decreases Adipokines Levels and Cardiovascular Risk Factors in Men with Obesity" Nutrients 15, no. 2: 286. https://doi.org/10.3390/nu15020286
APA StyleSaeidi, A., Nouri-Habashi, A., Razi, O., Ataeinosrat, A., Rahmani, H., Mollabashi, S. S., Bagherzadeh-Rahmani, B., Aghdam, S. M., Khalajzadeh, L., Al Kiyumi, M. H., Hackney, A. C., Laher, I., Heinrich, K. M., & Zouhal, H. (2023). Astaxanthin Supplemented with High-Intensity Functional Training Decreases Adipokines Levels and Cardiovascular Risk Factors in Men with Obesity. Nutrients, 15(2), 286. https://doi.org/10.3390/nu15020286