
Rectus Femoris Cross-Sectional Area and Phase Angle asPredictors of 12-Month Mortality in Idiopathic Pulmonary Fibrosis Patients
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting Study
2.2. Anthropometric and Body Composition Parameters
2.3. Abdominal and Muscle Nutritional Ultrasound
2.4. Assessment of Nutritional Status
2.5. Assessment of Respiratory Status
2.6. Statistical Analysis
3. Results
3.1. General Characterization of the Population Study
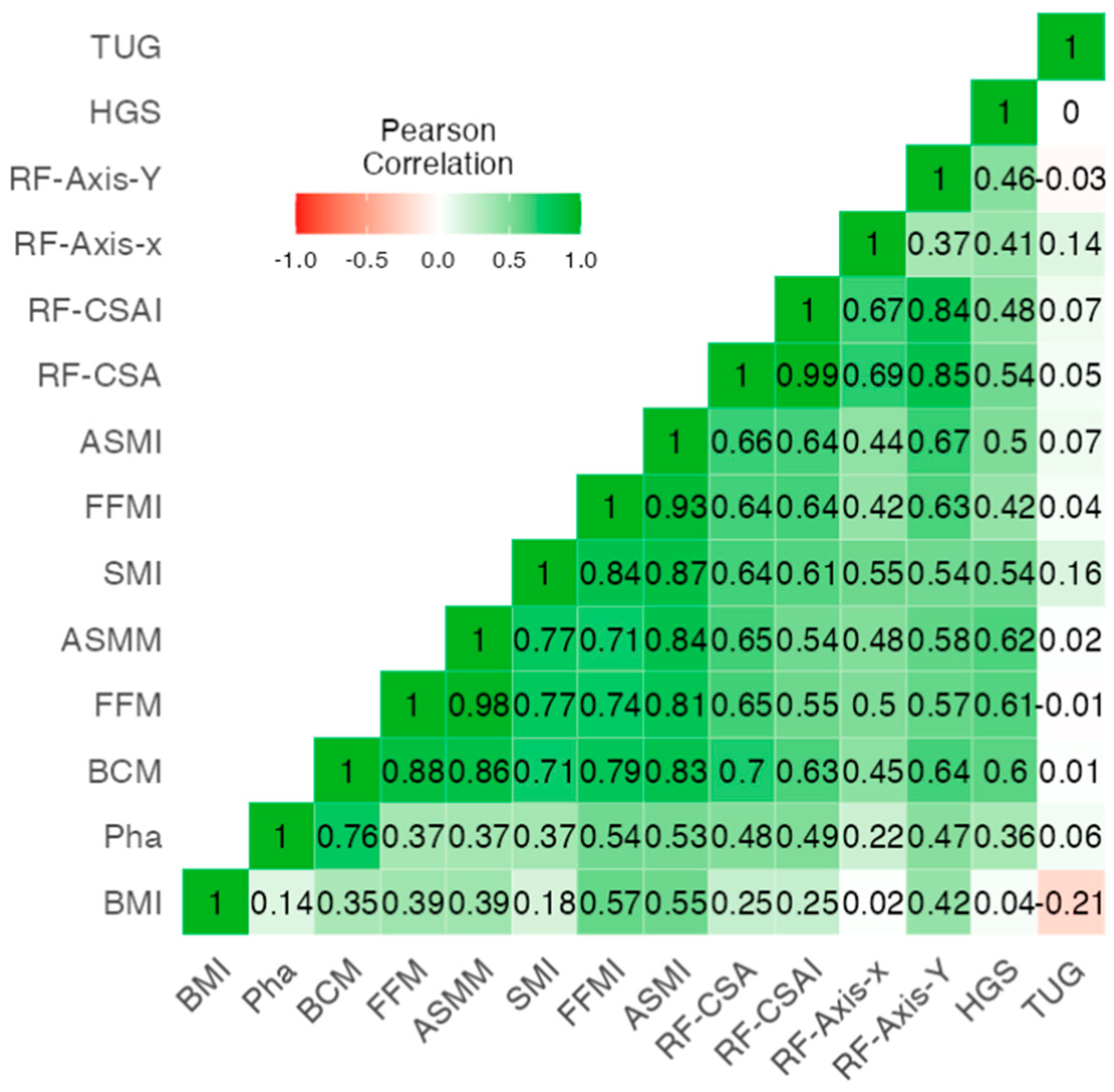
3.2. Correlation Analysis between BIA Muscle Measures, Muscular Ultrasound, HGS with 12-Month Mortality
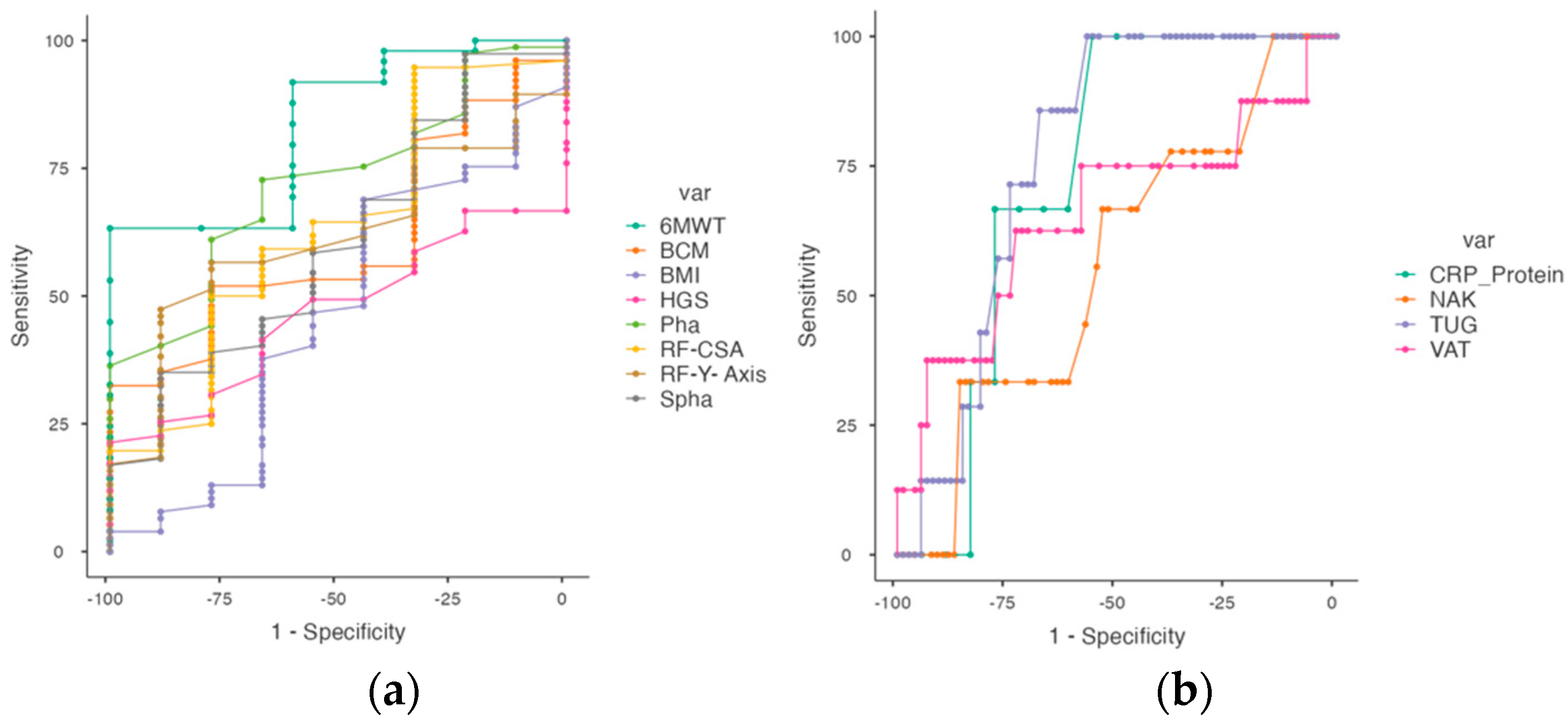
3.3. Cut-Off Point for 12-Month Mortality in IPF Patients
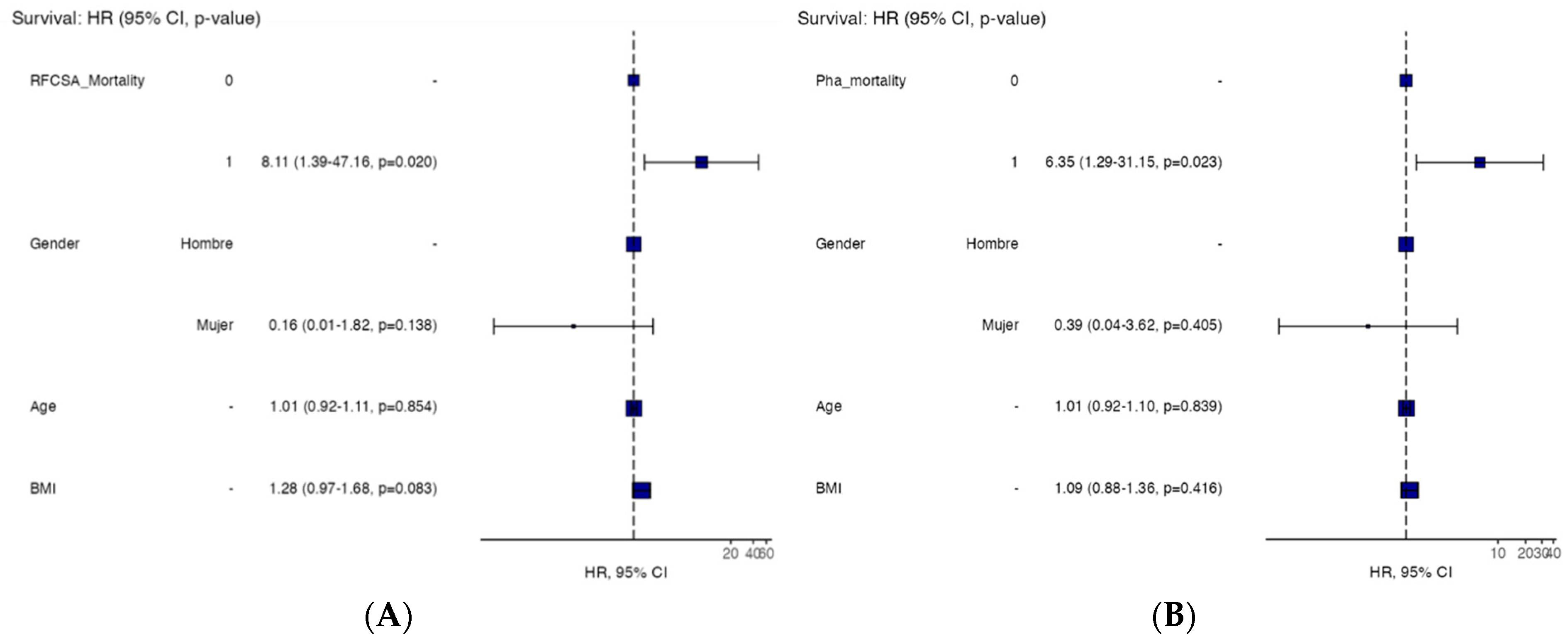
3.4. 12-Month Mortality Risk for IPF Patients
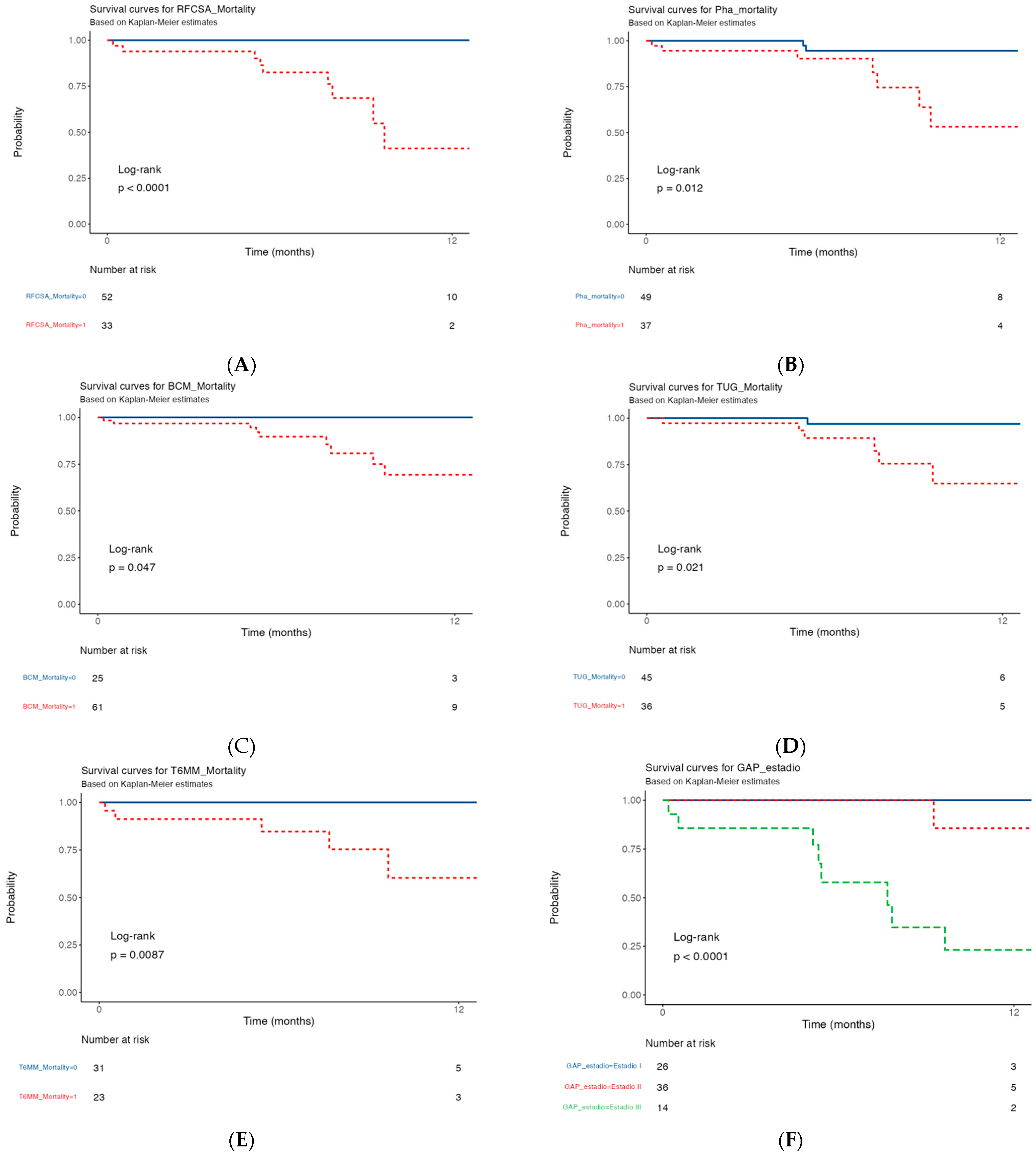
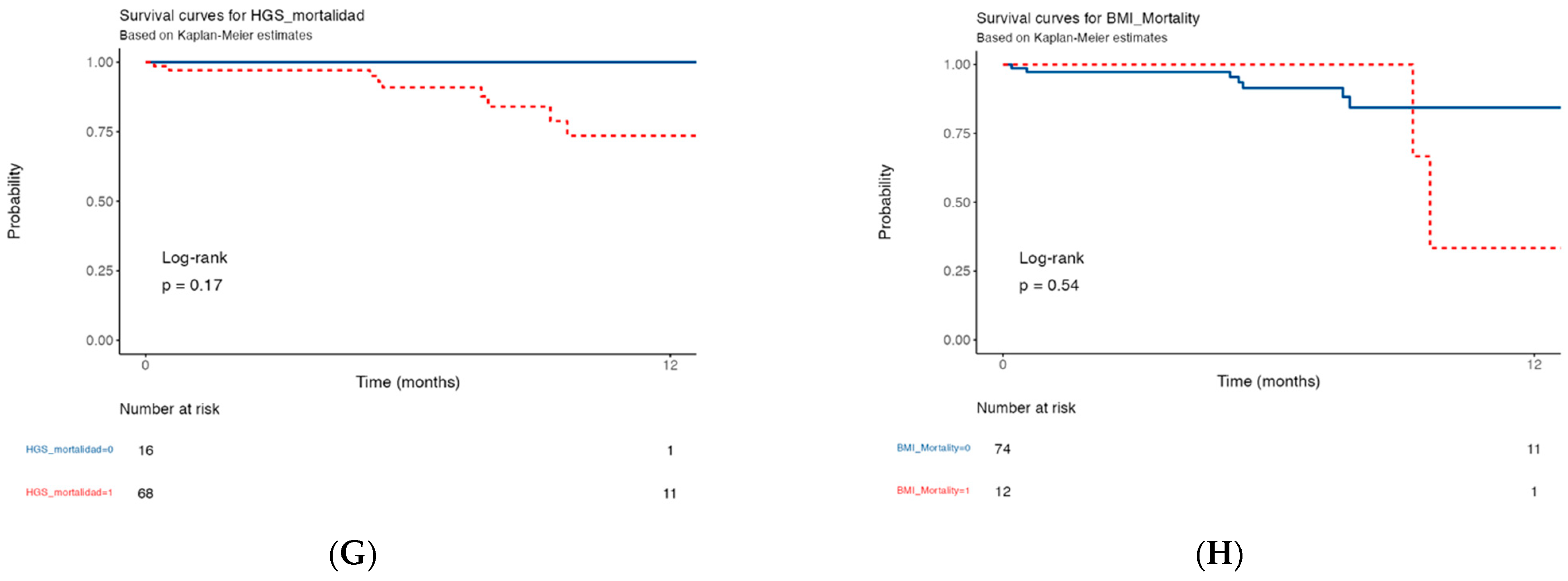
3.5. Kaplan–Meier Survival Curve of 12-Month Mortality in IPF Patients with Morphofunctional Assessment Techniques
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed]
- Kreuter, M.; Ehlers-Tenenbaum, S.; Palmowski, K.; Bruhwyler, J.; Oltmanns, U.; Muley, T.; Heussel, C.P.; Warth, A.; Kolb, M.; Herth, F.J.F. Impact of Comorbidities on Mortality in Patients with Idiopathic Pulmonary Fibrosis. PLoS ONE 2016, 11, e0151425. [Google Scholar] [CrossRef] [PubMed]
- Nakatsuka, Y.; Handa, T.; Kokosi, M.; Tanizawa, K.; Puglisi, S.; Jacob, J.; Sokai, A.; Ikezoe, K.; Kanatani, K.T.; Kubo, T.; et al. The Clinical Significance of Body Weight Loss in Idiopathic Pulmonary Fibrosis Patients. Respiration 2018, 96, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.M.; Thomas, A.; Crinion, S.J.; Kent, B.D.; Tambuwala, M.M.; Fabre, A.; Pepin, J.-L.; Roche, H.M.; Arnaud, C.; Ryan, S. Intermittent hypoxia in obstructive sleep apnoea mediates insulin resistance through adipose tissue inflammation. Eur. Respir. J. 2017, 49, 1601731. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Cox, I.A.; Campbell, J.A.; Xia, Q.; Otahal, P.; de Graaff, B.; Corte, T.J.; Teoh, A.K.Y.; Walters, E.H.; Palmer, A.J. Mortality and survival in idiopathic pulmonary fibrosis: A systematic review and meta-analysis. ERJ Open Res. 2022, 8, 00591–02021. [Google Scholar] [CrossRef]
- Faverio, P.; Bocchino, M.; Caminati, A.; Fumagalli, A.; Gasbarra, M.; Iovino, P.; Petruzzi, A.; Scalfi, L.; Sebastiani, A.; Stanziola, A.A.; et al. Nutrition in Patients with Idiopathic Pulmonary Fibrosis: Critical Issues Analysis and Future Research Directions. Nutrients 2020, 12, 1131. [Google Scholar] [CrossRef] [PubMed]
- Schwebel, C.; Pin, I.; Barnoud, D.; Devouassoux, G.; Brichon, P.Y.; Chaffanjon, P.; Chavanon, O. Prevalence and consequences of nutritional depletion in lung transplant candidates. Eur. Respir. J. 2000, 16, 1050–1055. [Google Scholar] [CrossRef]
- Lee, J.H.; Jang, J.H.; Jang, H.J.; Kim, S.Y.; Chung, M.P.; Yoo, H.; Jeong, S.H.; Song, J.W. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front. Med. 2023, 10, 1052129. [Google Scholar] [CrossRef] [PubMed]
- García Almeida, J.M.; García García, C.; Vegas Aguilar, I.M.; Bellido Castañeda, V.; Bellido Guerrero, D. Morphofunctional assessment of patient’s nutritional status: A global approach. Nutr. Hosp. 2021, 38, 592–600. [Google Scholar] [PubMed]
- Garlini, L.M.; Alves, F.D.; Ceretta, L.B.; Perry, I.S.; Souza, G.C.; Clausell, N.O. Phase angle and mortality: A systematic review. Eur. J. Clin. Nutr. 2019, 73, 495–508. [Google Scholar] [CrossRef]
- De Benedetto, F.; Marinari, S.; De Blasio, F. Phase angle in assessment and monitoring treatment of individuals with respiratory disease. Rev. Endocr. Metab. Disord. 2023, 24, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; García-Almeida, J.M.; Bellido-Guerrero, D.; Talluri, A.; Lukaski, H.; Tinahones, F.J. Phase angle and standardized phase angle from bioelectrical impedance measurements as a prognostic factor for mortality at 90 days in patients with COVID-19: A longitudinal cohort study. Clin. Nutr. 2021, 41, 3106–3114. [Google Scholar] [CrossRef] [PubMed]
- Vegas-Aguilar, I.M.; Guirado-Peláez, P.; Fernández-Jiménez, R.; Boughanem, H.; Tinahones, F.J.; Garcia-Almeida, J.M. Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer. Cancers 2023, 15, 847. [Google Scholar] [CrossRef]
- García-Almeida, J.M.; García-García, C.; Vegas-Aguilar, I.M.; Ballesteros Pomar, M.D.; Cornejo-Pareja, I.M.; Medina, B.F.; de Luis Roman, D.A. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinol. Diabetes Nutr. 2023, 70, 74–84. [Google Scholar] [CrossRef]
- García-García, C.; Vegas-Aguilar, I.M.; Rioja-Vázquez, R.; Cornejo-Pareja, I.; Tinahones, F.J.; García-Almeida, J.M. Rectus Femoris Muscle and Phase Angle as Prognostic Factor for 12-Month Mortality in a Longitudinal Cohort of Patients with Cancer (AnyVida Trial). Nutrients 2023, 15, 522. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Torralvo, F.J.; Porras, N.; Ruiz-García, I.; Maldonado-Araque, C.; García-Olivares, M.; Girón, M.V.; Gonzalo-Marín, M.; Olveira, C.; Olveira, G. Usefulness of Muscle Ultrasonography in the Nutritional Assessment of Adult Patients with Cystic Fibrosis. Nutrients 2022, 14, 3377. [Google Scholar] [CrossRef]
- Mesquita, R.; Wilke, S.; Smid, D.E.; Janssen, D.J.; Franssen, F.M.; Probst, V.S.; Wouters, E.F.; Muris, J.W.; Pitta, F.; A Spruit, M. Measurement properties of the Timed Up & Go test in patients with COPD. Chronic Respir. Dis. 2016, 13, 344–352. [Google Scholar]
- Hendriks, S.; Huisman, M.G.; Ghignone, F.; Vigano, A.; de Liguori Carino, N.; Farinella, E.; Girocchi, R.; Audisio, R.A.; van Munster, B.; de Bock, G.H.; et al. Timed up and go test and long-term survival in older adults after oncologic surgery. BMC Geriatr. 2022, 22, 934. [Google Scholar] [CrossRef]
- Piccoli, A.; Nigrelli, S.; Caberlotto, A.; Bottazzo, S.; Rossi, B.; Pillon, L.; Maggiore, Q. Bivariate normal values of the bioelectrical impedance vector in adult and elderly populations. Am. J. Clin. Nutr. 1995, 61, 269–270. [Google Scholar] [CrossRef]
- Piccoli, A.; Rossi, B.; Pillon, L.; Bucciante, G. A new method for monitoring body fluid variation by bioimpedance analysis: The RXc graph. Kidney Int. 1994, 46, 534–539. [Google Scholar] [CrossRef]
- Cardinal, T.R.; Wazlawik, E.; Bastos, J.L.; Nakazora, L.M.; Scheunemann, L. Standardized phase angle indicates nutritional status in hospitalized preoperative patients. Nutr. Res. 2010, 30, 594–600. [Google Scholar] [CrossRef]
- De Palo, T.; Messina, G.; Edefonti, A.; Perfumo, F.; Pisanello, L.; Peruzzi, L.; Di Iorio, B.; Mignozzi, M.; Vienna, A.; Conti, G.; et al. Normal values of the bioelectrical impedance vector in childhood and puberty. Nutrition 2000, 16, 417–424. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Hamagawa, K.; Matsumura, Y.; Kubo, T.; Hayato, K.; Okawa, M.; Tanioka, K.; Yamasaki, N.; Kitaoka, H.; Yabe, T.; Nishinaga, M.; et al. Abdominal visceral fat thickness measured by ultrasonography predicts the presence and severity of coronary artery disease. Ultrasound Med. Biol. 2010, 36, 1769–1775. [Google Scholar] [CrossRef] [PubMed]
- Torrisi, S.E.; Ley, B.; Kreuter, M.; Wijsenbeek, M.; Vittinghoff, E.; Collard, H.R.; Vancheri, C. The added value of comorbidities in predicting survival in idiopathic pulmonary fibrosis: A multicentre observational study. Eur. Respir. J. 2019, 53, 1801587. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xu, P.; Wang, Y.; Wang, M.; Li, H.; Lin, S.; Mao, C.; Wang, B.; Song, X.; Lv, C. Astaxanthin prevents pulmonary fibrosis by promoting myofibroblast apoptosis dependent on Drp1-mediated mitochondrial fission. J. Cell. Mol. Med. 2015, 19, 2215–2231. [Google Scholar] [CrossRef] [PubMed]
- Ley, B.; Ryerson, C.J.; Vittinghoff, E.; Ryu, J.H.; Tomassetti, S.; Lee, J.S.; Poletti, V.; Buccioli, M.; Elicker, B.M.; Jones, K.D.; et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann. Intern. Med. 2012, 156, 684–691. [Google Scholar] [CrossRef]
- Lacedonia, D.; De Pace, C.C.; Rea, G.; Capitelli, L.; Gallo, C.; Scioscia, G.; Tondo, P.; Bocchino, M. Machine Learning and BMI Improve the Prognostic Value of GAP Index in Treated IPF Patients. Bioengineering 2023, 10, 251. [Google Scholar] [CrossRef]
- Nathan, S.D.; du Bois, R.M.; Albera, C.; Bradford, W.Z.; Costabel, U.; Kartashov, A.; Noble, P.W.; Sahn, S.A.; Valeyre, D.; Weycker, D.; et al. Validation of test performance characteristics and minimal clinically important difference of the 6-minute walk test in patients with idiopathic pulmonary fibrosis. Respir. Med. 2015, 109, 914–922. [Google Scholar] [CrossRef]
- Alakhras, M.; Decker, P.A.; Nadrous, H.F.; Collazo-Clavell, M.; Ryu, J.H. Body mass index and mortality in patients with idiopathic pulmonary fibrosis. Chest 2007, 131, 1448–1453. [Google Scholar] [CrossRef]
- Vestbo, J.; Prescott, E.; Almdal, T.; Dahl, M.; Nordestgaard, B.G.; Andersen, T.; Sørensen, T.I.A. Body mass, fat-free body mass, and prognosis in patients with chronic obstructive pulmonary disease from a random population sample: Findings from the Copenhagen City Heart Study. Am. J. Respir. Crit. Care Med. 2006, 173, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Jouneau, S.; Rousseau, C.; Lederlin, M.; Lescoat, A.; Kerjouan, M.; Chauvin, P.; Luque-Paz, D.; Guillot, S.; Oger, E.; Vernhet, L.; et al. Malnutrition and decreased food intake at diagnosis are associated with hospitalization and mortality of idiopathic pulmonary fibrosis patients. Clin. Nutr. 2022, 41, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Martínez, M.; Rodríguez-García, W.; González-Islas, D.; Orea-Tejeda, A.; Keirns-Davis, C.; Salgado-Fernández, F.; Hernandez-Lopez, S. Impact of Body Composition and Sarcopenia on Mortality in Chronic Obstructive Pulmonary Disease Patients. J. Clin. Med. 2023, 12, 1321. [Google Scholar] [CrossRef]
- Machado, F.V.C.; Bloem, A.E.M.; Schneeberger, T.; Jarosch, I.; Gloeckl, R.; Winterkamp, S.; Franssen, F.M.E.; Koczulla, A.R.; Pitta, F.; Spruit, M.A.; et al. Relationship between body composition, exercise capacity and health-related quality of life in idiopathic pulmonary fibrosis. BMJ Open Respir. Res. 2021, 8, e001039. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Talluri, A. Phase angle as an index of physiological status: Validating bioelectrical assessments of hydration and cell mass in health and disease. Rev. Endocr. Metab. Disord. 2022, 24, 371–379. [Google Scholar] [CrossRef]
- da Silva, B.R.; Orsso, C.E.; Gonzalez, M.C.; Sicchieri, J.M.F.; Mialich, M.S.; Jordao, A.A.; Prado, C.M. Phase angle and cellular health: Inflammation and oxidative damage. Rev. Endocr. Metab. Disord. 2022, 24, 543–562. [Google Scholar] [CrossRef]
- García-Almeida, J.M.; García-García, C.; Ballesteros-Pomar, M.D.; Olveira, G.; Lopez-Gomez, J.J.; Bellido, V.; Lesmes, I.B.; Burgos, R.; Sanz-Paris, A.; Matia-Martin, P.; et al. Expert Consensus on Morphofunctional Assessment in Disease-Related Malnutrition. Grade Review and Delphi Study. Nutrients 2023, 15, 612. [Google Scholar] [CrossRef]
- Wu, W.; Li, C.; Zhu, X.; Liu, X.; Li, P.; Wan, R.; Wu, X.; Chen, S. Genetic association of telomere length, obesity and tobacoo smoking with idiopathic pulmonary fibrosis risk. BMC Public Health 2023, 23, 868. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Yoshimura, K.; Enomoto, Y.; Yasui, H.; Hozumi, H.; Karayama, M.; Furuhashi, K.; Enomoto, N.; Fujisawa, T.; Nakamura, Y.; et al. Distinct profile and prognostic impact of body composition changes in idiopathic pulmonary fibrosis and idiopathic pleuroparenchymal fibroelastosis. Sci. Rep. 2018, 8, 14074. [Google Scholar] [CrossRef]
- de Paula, W.D.; Rodrigues, M.P.; Ferreira, N.M.C.; Passini, V.V.; Melo-Silva, C.A. Noninvasive assessment of peripheral skeletal muscle weakness in idiopathic pulmonary fibrosis: A pilot study with multiparametric MRI of the rectus femoris muscle. Multidiscip. Respir. Med. 2020, 15, 707. [Google Scholar]
- Zhi, J.; Shan, Q.; Liang, L.; Liu, H.; Huang, H. Low skeletal muscle area as a prognostic marker for chronic obstructive pulmonary disease in elderly patients admitted to ICU. Sci. Rep. 2019, 9, 19117. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.A.; Ross, D.W.; Pivert, K.A.; Lang, V.J.; Sozio, S.M.; O’Neill, W.C. Point-of-Care Ultrasound Training during Nephrology Fellowship: A National Survey of Fellows and Program Directors. Clin. J. Am. Soc. Nephrol. 2022, 17, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Hashim, A.; Tahir, M.J.; Ullah, I.; Asghar, M.S.; Siddiqi, H.; Yousaf, Z. The utility of point of care ultrasonography (POCUS). Ann. Med. Surg. 2021, 71, 102982. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Survival | Non-Survival | p-Value | |
|---|---|---|---|---|
| N = 86 | N = 77 | N = 9 | ||
| Demographic variables | ||||
| Age (years) | 71.0 (7.26) | 71.0 (7.37) | 71.0 (6.65) | 0.949 |
| Weight (kg) | 78.30 (12.1) | 77.7 (11.7) | 83.9 (14.6) | 0.144 |
| Weight loss (%) | 6.41 (6.78) | 6.26 (6.66) | 7.71 (8.12) | 0.696 |
| BMI (kg/m2) | 27.40 (3.44) | 27.3 (3.46) | 28.0 (3.41) | 0.612 |
| BIA | ||||
| PhA (°) | 4.78 (0.77) | 4.85 (0.76) | 4.27 (0.65) | 0.033 |
| SPhA | −1.03 (1.01) | −0.98 (0.99) | −1.41 (1.06) | 0.23 |
| Hydration (%) | 74.60(2.31) | 74.6 (2.36) | 75.1 (1.87) | 0.165 |
| NaK | 1.18 (0.18) | 1.17 (0.18) | 1.21 (0.16) | 0.548 |
| BCM (kg) | 25.5 (5.17) | 25.7 (5.28) | 23.8 (3.89) | 0.287 |
| FFM (kg) | 54.5 (7.48) | 54.47 (7.61) | 54.98 (6.49) | 0.868 |
| ASMM (kg) | 20.2 (3.29) | 20.17 (3.36) | 20.38 (2.77) | 0.383 |
| SMI (cm2/m2) | 8.81 (1.20) | 8.85 (1.22) | 8.41(1.06) | 0.299 |
| FFMI (%) | 19.0 (1.74) | 19.1 (1.74) | 18.4 (1.70) | 0.219 |
| FM (kg) | 23.8 (7.91) | 23.2 (7.37) | 29.0 (10.8) | 0.038 |
| Echography exploration | ||||
| RF-CSA (cm2) | 3.38 (0.98) | 3.43 (0.99) | 2.96 (0.84) | 0.196 |
| RF-CIR (cm) | 8.15 (1.11) | 8.19 (1.10) | 7.81 (1.23) | 0.333 |
| RF-X-axis (cm) | 3.43 (0.50) | 3.45 (0.50) | 3.32 (0.49) | 0.466 |
| RF-Y-axis (cm) | 1.11 (0.27) | 1.12 (0.28) | 1.02 (0.16) | 0.291 |
| L-SAT (cm) | 0.78 (0.52) | 0.78 (0.53) | 0.78 (0.44) | 0.563 |
| T-SAT (cm2) | 1.67 (0.71) | 1.66 (0.71) | 1.73 (0.77) | 0.779 |
| S-SAT (cm2) | 0.72 (0.30) | 0.71 (0.29) | 0.79 (0.35) | 0.544 |
| VAT (cm2) | 0.65 (0.30) | 0.62 (0.25) | 0.89 (0.56) | 0.146 |
| Functional measurement | ||||
| HGS max (kg) | 34.5 (10.4) | 34.4 (10.8) | 36.0 (5.61) | 0.655 |
| HGS mean (kg) | 33.0 (10.1) | 32.9 (10.5) | 34.0 (5.61) | 0.761 |
| TUG (s) | 8.29 (5.24) | 8.21 (5.45) | 9.14 (1.93) | 0.019 |
| 6MW (m) | 405.0 (76.2) | 416 (61.6) | 301 (128) | <0.001 |
| Biochemical variables | ||||
| Glucose (mg/dL) | 110 (38.3) | 111 (27.5) | 105 (80.1) | 0.038 |
| Urea (mg/dL) | 43.5 (14.8) | 42.6 (14.0) | 47.0 (18.7) | 0.567 |
| Creatinine (mg/dL) | 1.05 (0.25) | 1.08 (0.26) | 0.90 (0.10) | 0.165 |
| Total cholesterol (mg/dL) | 198 (58.8) | 198 (56.3) | 199 (85.0) | 0.985 |
| Triglycerides (mg/dL) | 142 (90.5) | 131 (89.5) | 195 (91.9) | 0.274 |
| FCV (%) | 67.9 (15.9) | 68.5 (16.5) | 62.1 (9.49) | 0.265 |
| FEV1 (%) | 77.9 (19.4) | 78.8 (20.5) | 10.0 (5.40) | 0.233 |
| DLCO (%) | 47.3 (18.2) | 50.02 (17.1) | 25.25 (10.7) | <0.001 |
| Clinicopathological variables | ||||
| Diagnostic (month) | 15.5 (19.2) | 16.2 (19.8) | 10.1 (11.8) | 0.436 |
| GAP Stage: | <0.001 | |||
| I | 26 (34.2%) | 26.0 (34.2%) | 0.0 (0.00%) | |
| II | 36 (47.4%) | 35.0 (46.1%) | 1.0 (1.30%) | |
| III | 14 (18.4%) | 6.0 (7.9%) | 8.0 (10.5%) | |
| SGA | 0.396 | |||
| A | 15.0 (17.4%) | 15.0 (17.4%) | 0.0 (0.0%) | |
| B | 52.0 (60.5%) | 45.0 (52.3%) | 7.0 (8.1%) | |
| C | 19.0 (22.1%) | 17.0 (19.8%) | 2.0 (2.3%) | |
| RF-CSA | RF-CSAI | RF-X-Axis | RF-Y-Axis | HGS | TUG | |
|---|---|---|---|---|---|---|
| BMI (kg/m2) | ||||||
| r= 0.25 | r = −0.25 | r = −0.02 | r = 0.42 | r = 0.04 | r = −0.21 | |
| p < 0.05 | p = 0.056 | p = 0.885 | p < 0.001 | p = 0.844 | p < 0.211 | |
| PhA (°) | r = 0.48 | r = 0.49 | r = 0.22 | r = 0.47 | r = 0.348 | r = −0.06 |
| p < 0.001 | p < 0.001 | p = 0.096 | p < 0.001 | p < 0.001 | p = 0.620 | |
| BCM(kg) | r= 0.70 | r = 0.63 | r= 0.45 | r = 0.64 | r = 0.60 | r = 0.01 |
| p < 0.001 | p = <0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p = 912 | |
| FFM(kg) | r = 0.65 | r = 0.55 | r = 0.50 | r = 0.57 | r = 0.61 | r = −0.01 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p = 920 | |
| ASMM (kg) | r = 0.65 | r = 0.54 | r = 0.48 | r = 0.58 | r = 0.62 | r = 0.02 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p = 850 | |
| SMI (kg/m) | r = 0.64 | r = 0.61 | r = 0.55 | r = 0.54 | r = 0.54 | r = 0.16 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p = 0.161 | |
| FFMI(Kg/m) | r = 0.64 | r = 0.64 | r = 0.42 | r = 0.63 | r = 0.42 | r = 0.04 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.739 | |
| ASMI (Kg/m) | r = 0.66 | r = 0.64 | r = 0.44 | r = 0.67 | r = 0.50 | r = 0.07 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.800 | |
| Handgrip strength (kg) | r = 0.54 | r = 0.54 | r = 0.41 | r = 0.46 | -- | r = −0.358 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||
| TUG | r = 0.05 | r = 0.07 | r = 0.14 | r = −0.03 | r = −0.358 | -- |
| p < 0.651 | p < 0.555 | p < 0.633 | p < 0.800 | p < 0.001 |
| AUC | Cut-Off ▴ | Sensitivity | Specificity | |
|---|---|---|---|---|
| Rectus Femoris | ||||
| RF-CSA | 0.857 | 3.00 | 64.41% | 100.0% |
| RF-CIR | 0.577 | 8.79 | 35.53% | 88.89% |
| RF-X-axis | 0.567 | 3.88 | 22.37% | 100.0% |
| RF-Y-axis | 0.615 | 1.10 | 47.37% | 88.89% |
| L-SAT | 0.440 | 0.65 | 42.67% | 66.67% |
| Abdominal | ||||
| T-SAT | 0.474 | 0.83 | 94,94% | 22.22% |
| S-SAT | 0.437 | 0.30 | 97.37% | 11.11% |
| VAT | 0.658 | 0.75 | 62.50% | 72.97% |
| BIA | ||||
| SPhA | 0.618 | −0.44 | 35.0% | 88.9% |
| PhA | 0.722 | 4.5 | 72.7% | 66.6% |
| BCM | 0.609 | 28.8 | 32.47% | 100.0% |
| NaK | 0.562 | 1.17 | 66.67% | 53.25% |
| Functional test | ||||
| HGS | 0.468 | 44.0 | 21.33% | 100.0% |
| TUG | 0.771 | 7.20 | 100.0% | 56.76% |
| 6MM | 0.830 | 420.0 | 63.27% | 100.0% |
| Blood test | ||||
| CRP protein | 0.731 | 7 | 100% | 55.56% |
| Dependent: Survival (My Time, My Outcome) | All | HR (Univariable) | HR (Multivariable) | |
|---|---|---|---|---|
| PhA–mortality | Survival | 49 (57.0) | - | - |
| Non-survival | 37 (43.0) | 5.92 (1.23–28.55, p = 0.027) | 6.35 (1.29–31.15, p = 0.023) | |
| Gender | Male | 71 (82.6) | - | - |
| Female | 15 (17.4) | 0.67 (0.08–5.38, p = 0.706) | 0.39 (0.04–3.62, p = 0.405) | |
| Age | Mean (SD) | 71.0 (7.3) | 1.02 (0.93–1.12, p = 0.669) | 1.01 (0.88–1.36, p = 0.416) |
| BMI | Mean (SD) | 27.4 (3.4) | 1.06 (0.87–1.28, p = 0.579) | 1.09 (0.88–1.36, p = 0.416) |
| Dependent: Survival (My Time, My Outcome) | All | HR (Univariable) | HR (Multivariable) | |
|---|---|---|---|---|
| RF-CSA–mortality | Survival | 40 (47.1) | - | - |
| Non-survival | 45 (52.9) | 3.92 (0.81–18.97, p = 0.089) | 8.11 (1.39–47.16, p = 0.020) | |
| Gender | Male | 70 (82.4) | - | - |
| Female | 15 (17.6) | 0.66 (0.08–5.34, p = 0.700) | 0.16 (0.01–1.82, p = 0.138) | |
| Age | Mean (SD) | 70.9 (7.3) | 1.02 (0.93–1.12, p = 0.655) | 1.01 (0.92–1.11, p = 0.854) |
| BMI | Mean (SD) | 27.3 (3.2) | 1.07 (0.87–1.31, p = 0.521) | 1.28 (0.97–1.68, p = 0.083) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Jiménez, R.; Cabrera Cesar, E.; Sánchez García, A.; Espíldora Hernández, F.; Vegas-Aguilar, I.M.; Amaya-Campos, M.d.M.; Cornejo-Pareja, I.; Guirado-Peláez, P.; Simón-Frapolli, V.; Murri, M.; et al. Rectus Femoris Cross-Sectional Area and Phase Angle asPredictors of 12-Month Mortality in Idiopathic Pulmonary Fibrosis Patients. Nutrients 2023, 15, 4473. https://doi.org/10.3390/nu15204473
Fernández-Jiménez R, Cabrera Cesar E, Sánchez García A, Espíldora Hernández F, Vegas-Aguilar IM, Amaya-Campos MdM, Cornejo-Pareja I, Guirado-Peláez P, Simón-Frapolli V, Murri M, et al. Rectus Femoris Cross-Sectional Area and Phase Angle asPredictors of 12-Month Mortality in Idiopathic Pulmonary Fibrosis Patients. Nutrients. 2023; 15(20):4473. https://doi.org/10.3390/nu15204473
Chicago/Turabian StyleFernández-Jiménez, Rocío, Eva Cabrera Cesar, Ana Sánchez García, Francisco Espíldora Hernández, Isabel M. Vegas-Aguilar, Maria del Mar Amaya-Campos, Isabel Cornejo-Pareja, Patricia Guirado-Peláez, Victor Simón-Frapolli, Mora Murri, and et al. 2023. "Rectus Femoris Cross-Sectional Area and Phase Angle asPredictors of 12-Month Mortality in Idiopathic Pulmonary Fibrosis Patients" Nutrients 15, no. 20: 4473. https://doi.org/10.3390/nu15204473
APA StyleFernández-Jiménez, R., Cabrera Cesar, E., Sánchez García, A., Espíldora Hernández, F., Vegas-Aguilar, I. M., Amaya-Campos, M. d. M., Cornejo-Pareja, I., Guirado-Peláez, P., Simón-Frapolli, V., Murri, M., Garrido-Sánchez, L., Martínez Mesa, A., Piñel-Jimenez, L., Benítez-Cano Gamonoso, M., Dalla-Rovere, L., García Olivares, M., Velasco-Garrido, J. L., Tinahones-Madueño, F., & García-Almeida, J. M. (2023). Rectus Femoris Cross-Sectional Area and Phase Angle asPredictors of 12-Month Mortality in Idiopathic Pulmonary Fibrosis Patients. Nutrients, 15(20), 4473. https://doi.org/10.3390/nu15204473